
Health Risks, Preventive Behaviours and Respiratory Illnesses at the 2019 Arbaeen: Implications for COVID-19 and Other Pandemics

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview of the Study
2.2. The Survey
2.3. Survey Administration
2.4. Interviewers
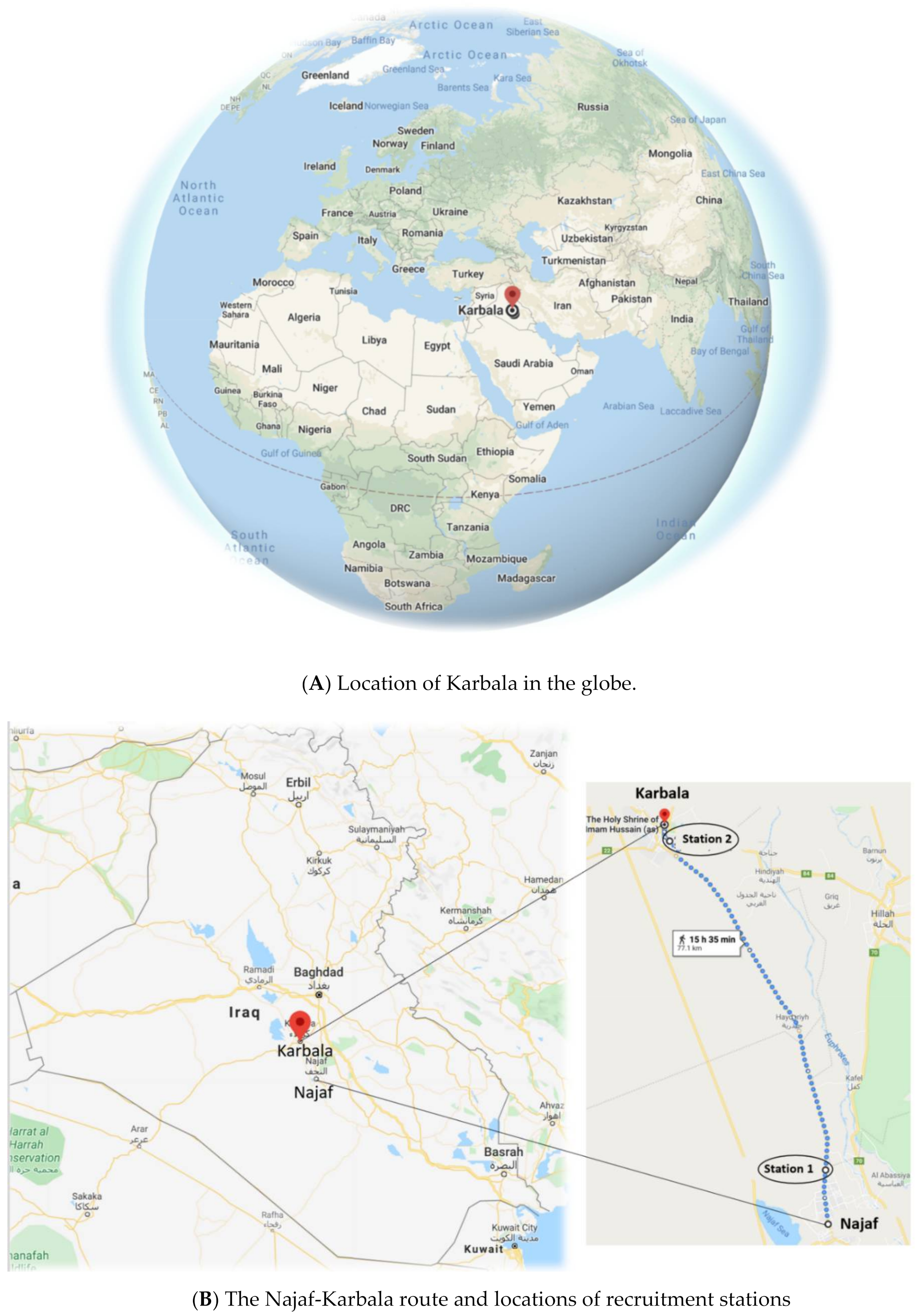
2.5. Recruitment
2.6. Analysis
2.7. Ethics
3. Results
3.1. Demographics
3.2. Reported Symptoms
3.3. Preventive Measures/Risk Factors and Association with Infectious Disease Symptoms
3.4. Pre-Existing Conditions
3.5. Toilet Facilities
3.6. Multivariate Predictors of the Development of Cough and at Least One of Cough, Breathlessness, or Fever
4. Discussion
4.1. Results Discussion
4.2. Limitations
4.3. Implications of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. English Version of the 2019 Arbaeen Full Survey

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Before approaching participant, research assistant to:
|
- ☐
- Do you give consent to take part in this survey?
- -
- Estimated broad age group
- ☐
- less than 35
- ☐
- 35–60
- ☐
- More than 60
- ☐
- unknown
- -
- Reason for refusal (stated or observed):
- ☐
- Language barrier
- ☐
- Cultural reasons
- ☐
- Too tired
- ☐
- No time
- ☐
- Suspicious about the survey
- ☐
- No reason given or observed
- ☐
- Other
- ☐
- IraqIf Iraq: Town/region of residence________________ (select from dropdown list)
- ☐
- Anbar
- ☐
- Arbil
- ☐
- Babel
- ☐
- Baghdad
- ☐
- Basra
- ☐
- Dahuk
- ☐
- Dhi Qar
- ☐
- Diyala
- ☐
- Karbala
- ☐
- Kirkuk
- ☐
- Maysan
- ☐
- Muthanna
- ☐
- Najaf
- ☐
- Ninawa
- ☐
- Qadisiyyah
- ☐
- Salah ad-Din
- ☐
- Sulaymaniyyah
- ☐
- Wasit
- ☐
- Other (please specify) ___________
Then skip to Q4- ☐
- Iran
- ☐
- Afghanistan
- ☐
- Algeria
- ☐
- Australia
- ☐
- Austria
- ☐
- Azerbaijan
- ☐
- Bahrain
- ☐
- Bangladesh
- ☐
- Belgium
- ☐
- Canada
- ☐
- China
- ☐
- Denmark
- ☐
- Egypt
- ☐
- France
- ☐
- Germany
- ☐
- Greece
- ☐
- India
- ☐
- Indonesia
- ☐
- Ireland
- ☐
- Italy
- ☐
- Japan
- ☐
- Jordon
- ☐
- Kenya
- ☐
- Kuwait
- ☐
- Lebanon
- ☐
- Malaysia
- ☐
- Morrocco
- ☐
- Neatherlands
- ☐
- New Zealand
- ☐
- Nigeria
- ☐
- Norway
- ☐
- Oman
- ☐
- Pakistan
- ☐
- Qatar
- ☐
- Saudi Arabia
- ☐
- Singapore
- ☐
- South Africa
- ☐
- Spain
- ☐
- Sudan
- ☐
- Sweden
- ☐
- Switzerland
- ☐
- Syria
- ☐
- Tunesia
- ☐
- Turkey
- ☐
- UAE
- ☐
- UK
- ☐
- USA
- ☐
- Yemen
- ☐
- Other
- ☐
- Home
- ☐
- Shrine of Imam Ali
- ☐
- Outskirts of Najaf
- ☐
- Stick number ……….
- ☐
- ☐ Other
- ☐
- Hotel
- ☐
- Private House
- ☐
- Mawkib (tent/outside)
- ☐
- Permanent Mawkib (built structure)
- ☐
- Mosque/Hussayniya
- ☐
- Other
- ☐
- Restaurant
- ☐
- Street food (sold)
- ☐
- Street food (donated)
- ☐
- Home food
- ☐
- Mawkib (outside cooking)
- ☐
- Mawkib (kitchen facility)
- ☐
- Other
- ☐
- Accommodation
- ☐
- Food
- ☐
- Neither
- ☐
- Hotel
- ☐
- Private house
- ☐
- Mawkib (tent/outside)
- ☐
- Permanent mawkib (building structure)
- ☐
- Mosque/hussayniya
- ☐
- Own home
- ☐
- Other
- ☐
- a hose
- ☐
- a bucket of water
- ☐
- running water for hand washing
- ☐
- soap or detergent for handwashing
- ☐
- a shared towel for drying hands
- ☐
- none of the above
- ☐
- Restaurant
- ☐
- Street food (sold)
- ☐
- Street food (donated)
- ☐
- Home food
- ☐
- Mawkib (outside cooking)
- ☐
- Mawkib (kitchen facility)
- ☐
- Other
- ☐
- Disposable cup
- ☐
- Reuseable cup (given to you by others)
- ☐
- Reuseable cup (your own)
- ☐
- No street food (sold)
- ☐
- No street food (donated)
- ☐
- Only bottled water (Note: translations into the other languages had this response option as ‘bottled or packaged water’)
- ☐
- No ice
- ☐
- Avoiding fresh fruits or salads
- ☐
- Carrying antibiotics
- ☐
- Carrying medicine to stop diarrhoea
- ☐
- Hand washing
- ☐
- Face mask
- ☐
- Other
- ☐
- Inhaler, like Ventolin (salbutamol)
- ☐
- Heart tablet (like nitroglycerin)
- ☐
- Antibiotics
- ☐
- Other
- ☐
- No, nothing makes it better
- ☐
- Chest pain
- ☐
- Heart problem
- ☐
- Diabetes
- ☐
- Neurological condition (e.g., stroke)
- ☐
- Other
- ☐
- Chest pain
- ☐
- Heart problem
- ☐
- Diabetes
- ☐
- Neurological condition (e.g., stroke)
- ☐
- Other
- ☐
- Nothing
- ☐
- Antibiotics
- ☐
- Pain killer
- ☐
- Other medicine(s)
- ☐
- Oxygen
- ☐
- Hospitalisation
- ☐
- Surgery
- ☐
- Other
- ☐
- No
- ☐
- Heart problems
- ☐
- Lung problems, including asthma
- ☐
- Diabetes
- ☐
- Kidney disease
- ☐
- Bowel disease
- ☐
- Neurological conditions (eg. stroke)
- ☐
- Hypertension
- ☐
- Other
References
- Zepeda-Lopez, H.M.; Perea-Araujo, L.; Miliar-García, A.; Dominguez-López, A.; Xoconostle-Cázarez, B.; Lara-Padilla, E.; Hernandez, J.A.R.; Sevilla-Reyes, E.; Orozco, M.E.; Ahued-Ortega, A.; et al. In-side the outbreak of the 2009 influenza A (H1N1) v virus in Mexico. PLoS ONE 2010, 5, e13256. [Google Scholar] [CrossRef]
- Ebrahim, S.H.; Memish, Z.A. COVID-19—The role of mass gatherings. Travel Med. Infect. Dis. 2020, 34, 101617. [Google Scholar] [CrossRef]
- Rudan, I. A cascade of causes that led to the COVID-19 tragedy in Italy and in other European Union countries. J. Glob. Health 2020, 10, 010335. [Google Scholar] [CrossRef]
- Badshah, S.L.; Ullah, A.; Badshah, S.H.; Ahmad, I. Spread of Novel Coronavirus by Returning Pilgrims from Iran to Pakistan. J. Travel Med. 2020, 27, taaa044. [Google Scholar] [CrossRef]
- Mat, N.F.C.; Edinur, H.A.; Razab, M.K.A.A.; Safuan, S. A single mass gathering resulted in massive transmission of COVID-19 infec-tions in Malaysia with further international spread. J. Travel Med. 2020, 27, taaa059. [Google Scholar] [CrossRef]
- Shim, E.; Tariq, A.; Choi, W.; Lee, Y.; Chowell, G. Transmission potential and severity of COVID-19 in South Korea. Int. J. Infect. Dis. 2020, 93, 339–344. [Google Scholar] [CrossRef]
- Sims, A. Millions of Muslims Take Part in Mass Pilgrimage of Arbaeen—In Spite of Isis. Independent. 2016. Available online: https://www.independent.co.uk/news/world/middle-east/20-million-muslims-march-against-isis-arbaeen-pilgrimage-iraq-karbala-a7436561.html (accessed on 6 February 2021).
- BBC Reporter. Shia Pilgrims Flock to Karbala for Arbaeen Climax. BBC. 2014. Available online: https://www.bbc.com/news/world-middle-east-30462820 (accessed on 1 March 2020).
- Press TV. Arba’een Walk 2019: World’s Largest Gathering in Numbers PRESS TV. 2019. Available online: https://www.presstv.com/Detail/2019/10/21/609183/Arbaeen-walk-2019-numbers-records (accessed on 1 February 2020).
- Al-Ansari, F.; Al Ansari, M.; Hill-Cawthorne, G.A.; Abdulzahra, M.S.; Al-Ansari, M.B.; Al-Ansari, B.; Rashid, H.; Negin, J.; Conigrave, K.M. Arbaeen public health concerns: A pilot cross-sectional survey. Travel Med. Infect. Dis. 2020, 35, 101546. [Google Scholar] [CrossRef]
- Karampourian, A.; Ghomian, Z.; Khorasani-Zavareh, D. Exploring challenges of health system preparedness for communicable diseases in Arbaeen mass gathering: A qualitative study. F1000Research 2018, 7, 1448. [Google Scholar] [CrossRef] [Green Version]
- Al-Ashqar, M. Report of Number of 1442 Hijri (2020 AD) Arbaeen Pilgrims Counted Electronically by Recording Walkers through Entries to Karbala (in Arabic); The Holy Shrine of Al-Abbas, Office of the Secretary General, Shiite Endown-ment Diwan, Republic of Iraq: Karbala, Iraq, 2020. [Google Scholar]
- Hantoosh, H.; Lami, F.; Saber, B. Disease Burden on Health Facilities in Governorates South of Karbala during the Arbaeenia Mass Gathering in Iraq in 2014: Cross-Sectional Study. JMIR Public Health Surveill. 2019, 5, e10917. [Google Scholar] [CrossRef]
- Lami, F.; Hameed, I.; Jewad, A.W.; Khader, Y.; Amiri, M. Real-Time Surveillance of Infectious Diseases and Other Health Conditions during Iraq’s Arbaeenia Mass Gathering: Cross-Sectional Study. JMIR Public Health Surveill. 2019, 5, e14510. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- The World Bank. World Bank Country and Lending Groups. World Bank Group, 2020. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 5 July 2020).
- Lami, F.; Asi, W.; Khistawi, A.; Jawad, I. Syndromic Surveillance of Communicable Diseases in Mobile Clinics during the Arba-eenia Mass Gathering in Wassit Governorate, Iraq, in 2014: Cross-Sectional Study. JMIR Public Health Surveill. 2019, 5, e10920. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, J.; Jafari, F. Prevalence of Diseases in Pilgrims Referring to Iranian Clinics in Iraq. Int. J. Travel Med. Glob. Health 2016, 4, 31–33. [Google Scholar] [CrossRef]
- Gautret, P.; Benkouiten, S.; Griffiths, K.; Sridhar, S. The inevitable Hajj cough: Surveillance data in French pilgrims, 2012–2014. Travel Med. Infect. Dis. 2015, 13, 485–489. [Google Scholar] [CrossRef]
- Memish, Z.A.; Zumla, A.; Alhakeem, R.F.; Assiri, A.; Turkestani, A.; Al Harby, K.D.; Alyemni, M.; Dhafar, K.; Gautret, P.; Barbeschi, M.; et al. Hajj: Infectious disease surveillance and control. Lancet 2014, 383, 2073–2082. [Google Scholar] [CrossRef]
- Abubakar, I.; Gautret, P.; Brunette, G.W.; Blumberg, L.; Johnson, D.; Poumerol, G.; Memish, Z.A.; Barbeschi, M.; Khan, A.S. Global perspectives for prevention of infec-tious diseases associated with mass gatherings. Lancet 2012, 12, 66–74. [Google Scholar] [CrossRef]
- Ahmed, Q.A.; Arabi, Y.M.; Memish, Z.A. Health risks at the Hajj. Lancet 2006, 367, 1008–1015. [Google Scholar] [CrossRef]
- Dzaraly, N.D.; Rahman, N.I.A.; Simbak, N.B.; Ab Wahab, S.; Osman, O.; Ismail, S.; Haque, M. Patterns of communicable and non-communicable diseases in Pilgrims during Hajj. Res. J. Pharm. Technol. 2014, 7, 12. [Google Scholar]
- Hoang, V.-T.; Gautret, P. Infectious Diseases and Mass Gatherings. Curr. Infect. Dis. Rep. 2018, 20, 44. [Google Scholar] [CrossRef]
- Hashim, S.; Ayub, Z.N.; Mohamed, Z.; Hasan, H.; Harun, A.; Ismail, N.; Rahman, Z.A.; Suraiya, S.; Naing, N.N.; Aziz, A.A. The prevalence and preventive measures of the respiratory illness among Malaysian pilgrims in 2013 hajj season. J. Travel Med. 2016, 23, tav019. [Google Scholar] [CrossRef] [Green Version]
- Alborzi, A.; Aelami, M.H.; Ziyaeyan, M.; Jamalidoust, M.; Moeini, M.; Pourabbas, B.; Abbasian, A. Viral etiology of acute respiratory infec-tions among Iranian Hajj pilgrims, 2006. J. Travel Med. 2009, 16, 239–242. [Google Scholar] [CrossRef] [Green Version]
- Simon, A.K.; Hollander, G.A.; McMichael, A.J. Evolution of the immune system in humans from infancy to old age. Proc. R. Soc. B Boil. Sci. 2015, 282, 20143085. [Google Scholar] [CrossRef]
- Liao, J.; Fan, S.; Chen, J.; Wu, J.; Xu, S.; Guo, Y.; Li, C.; Zhang, X.; Wu, C.; Mou, H.; et al. Epidemiological and Clinical Characteristics of COVID-19 in Adolescents and Young Adults. Innovation 2020, 1, 100001. [Google Scholar] [CrossRef]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; El-harakeh, A.; Bognanni, A.; Lotfi, T.; Loeb, M.; et al. Physical distancing, face masks, and eye protection to pre-vent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Algarni, H.; Memish, Z.A.; Assiri, A.M. Health conditions for travellers to Saudi Arabia for the pilgrimage to Mecca (Hajj)—2015. J. Epidemiol. Glob. Health 2015, 6, 7–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benkouiten, S.; Brouqui, P.; Gautret, P. Non-pharmaceutical interventions for the prevention of respiratory tract infections dur-ing Hajj pilgrimage. Travel Med. Infect. Dis. 2014, 12, 429–442. [Google Scholar] [CrossRef]
- Barasheed, O.; Alfelali, M.; Mushta, S.; Bokhary, H.; Alshehri, J.; Attar, A.A.; Booy, R.; Rashid, H. Uptake and effectiveness of facemask against res-piratory infections at mass gatherings: A systematic review. Int. J. Infect. Dis. 2016, 47, 105–111. [Google Scholar] [CrossRef] [Green Version]
- Memish, Z.A.; Assiri, A.M.; AlShehri, M.; Hussain, R.; AlOmar, I. The prevalance of respiratory viruses among healthcare workers serving pilgrims in Makkah during the 2009 influenza A (H1N1) pandemic. Travel Med. Infect. Dis. 2012, 10, 18–24. [Google Scholar] [CrossRef]
- Al-Asmary, S.; Al-Shehri, A.-S.; Abou-Zeid, A.; Abdel-Fattah, M.; Hifnawy, T.; El-Said, T. Acute respiratory tract infections among Hajj medical mission personnel, Saudi Arabia. Int. J. Infect. Dis. 2007, 11, 268–272. [Google Scholar] [CrossRef] [Green Version]
- Hoang, V.-T.; Ali-Salem, S.; Belhouchat, K.; Meftah, M.; Sow, D.; Dao, T.-L.; Ly, T.D.A.; Drali, T.; Ninove, L.; Yezli, S.; et al. Respiratory tract infections among French Hajj pilgrims from 2014 to 2017. Sci. Rep. 2019, 9, 17771. [Google Scholar] [CrossRef] [PubMed]
- Simmerman, J.M.; Suntarattiwong, P.; Levy, J.; Jarman, R.G.; Kaewchana, S.; Gibbons, R.V.; Cowling, B.J.; Sanasuttipun, W.; Maloney, S.A.; Uyeki, T.M.; et al. Findings from a household ran-domized controlled trial of hand washing and face masks to reduce influenza transmission in Bangkok, Thailand. Influenza Other Respir. Viruses 2011, 5, 256–267. [Google Scholar] [CrossRef]
- Isaacs, D.; Britton, P.; Howard-Jones, A.; Kesson, A.; Khatami, A.; Marais, B.; Nayda, C.; Outhred, A. Do facemasks protect against COVID-19? J. Paediatr. Child Health 2020, 56, 976–977. [Google Scholar] [CrossRef]
- Benkouiten, S.; Charrel, R.; Belhouchat, K.; Drali, T.; Salez, N.; Nougairede, A.; Zandotti, C.; Memish, Z.A.; Al Masri, M.; Gaillard, C.; et al. Circulation of respiratory viruses among pil-grims during the 2012 Hajj pilgrimage. Clin. Infect. Dis. 2013, 57, 992–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatrad, A.R.; Shafi, S.; Memish, Z.; Sheikh, A. Hajj and the risk of influenza. BMJ 2006, 333, 1182–1183. [Google Scholar] [CrossRef]
- Goldman, E. Exaggerated risk of transmission of COVID-19 by fomites. Lancet Infect. Dis. 2020, 20, 892–893. [Google Scholar] [CrossRef]
- Geller, C.; Varbanov, M.; Duval, R.E. Human coronaviruses: Insights into environmental resistance and its influence on the de-velopment of new antiseptic strategies. Viruses 2012, 4, 3044–3068. [Google Scholar] [CrossRef] [Green Version]
- Dong, J.H.X.-P. Stability of SARS coronavirus in human specimens and environment and its sensitivity to heating and UV irra-diation. Biomed. Environ. Sci. 2003, 16, 246–255. [Google Scholar]
- Abdul, A.; Chaudhry, J. Health related experiences among international pilgrims departing through King Abdul Aziz interna-tional airport, Jeddah, Saudi Arabia, Hajj 1431 H (2010). Saudi Epidemiol. Bull. 2010, 18, 42–44. [Google Scholar]
- Deris, Z.Z.; Hasan, H.; Sulaiman, S.A.; Wahab, M.S.A.; Naing, N.N.; Othman, N.H. The prevalence of acute respiratory symptoms and role of protective measures among Malaysian hajj pilgrims. J. Travel Med. 2010, 17, 82–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mustafa, A.N.; Gessner, B.D.; Ismail, R.; Yusoff, A.F.; Abdullah, N.; Ishak, I.; Abdullah, N.; Merican, M.I. A case-control study of influenza vaccine effec-tiveness among Malaysian pilgrims attending the Haj in Saudi Arabia. Int. J. Infect Dis. 2003, 7, 210–214. [Google Scholar] [CrossRef] [Green Version]
- Memish, Z.A.; Assiri, A.M.; Hussain, R.; AlOmar, I.; Stephens, G. Detection of Respiratory Viruses among Pilgrims in Saudi Arabia during the Time of a Declared Influenza A(H1N1) Pandemic. J. Travel Med. 2011, 19, 15–21. [Google Scholar] [CrossRef] [Green Version]
- Salamati, P.; Razavi, S.M.; Saeednejad, M. Vaccination in Hajj: An overview of the recent findings. Int. J. Prev. Med. 2016, 7, 129. [Google Scholar] [CrossRef] [PubMed]
- Saeed, K.M.I.; Mofleh, J.; Rasooly, M.H.; Aman, M.I. Occurrence of acute respiratory infection, diarrhea and jaundice among Afghan pilgrims, 2010. J. Epidemiol. Glob. Health 2012, 2, 215–220. [Google Scholar] [CrossRef] [Green Version]
- Jin, J.-M.; Bai, P.; He, W.; Wu, F.; Liu, X.-F.; Han, D.-M.; Liu, S.; Yang, J.-K. Gender Differences in Patients with COVID-19: Focus on Severity and Mortality. Front. Public Health 2020, 8, 152. [Google Scholar] [CrossRef] [PubMed]
- Arcavi, L.; Benowitz, N.L. Cigarette Smoking and Infection. Arch. Intern. Med. 2004, 164, 2206–2216. [Google Scholar] [CrossRef]
- World Health Organisation. Smoking and COVID-19. 2020. Available online: https://www.who.int/news-room/commentaries/detail/smoking-and-covid-19 (accessed on 7 September 2020).
- Taher, A.; Abo-ghniem, T.N.; Albujeer, A.N.; Almahafdha, A.; Khoshnevisan, M.H. Oral Hygiene and Mass Gathering of Iraqi and Non-Iraqi Visitors in Arbaeen; A Random Sample Survey for 3500 Visitor. Res. Rev. J. Dent. Sci. 2017, 5, 92–95. [Google Scholar]
- World Health Organisation. Considerations for mass gatherings in the context of COVID-19. In Annex: Considerations in Adjusting Public Health and Social Measures in the Context of COVID-19; World Health Organisation: Geneva, Switzerland, 2020. [Google Scholar]




| Male n = 1163 | Female n = 675 | p-Value | Total n = 1838 a | ||||
|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | na | (%) | ||
| Age (years) | <0.001 | ||||||
| 16–24 | 309 | (26.6) | 128 | (19.0) | 438 | (24.1) | |
| 25–44 | 556 | (47.8) | 283 | (41.9) | 841 | (46.2) | |
| 45–64 | 247 | (21.2) | 239 | (35.4) | 487 | (26.7) | |
| 65+ | 41 | (3.5) | 13 | (1.9) | 54 | (3.0) | |
| Country of origin | <0.001 | ||||||
| Iraq | 426 | (36.6) | 356 | (52.8) | 782 | (42.6) | |
| Iran | 667 | (57.4) | 267 | (39.6) | 933 | (50.8) | |
| Low to lower middle income | 30 | (2.6) | 13 | (1.9) | 43 | (2.3) | |
| Other upper middle income | 3 | (0.3) | 12 | (1.8) | 15 | (0.8) | |
| High income | 24 | (2.1) | 13 | (1.9) | 37 | (2.0) | |
| Unknown (non-recorded) | 13 | (1.1) | 14 | (2.1) | 27 | (1.5) | |
| Language survey completed with | <0.001 | ||||||
| Arabic | 490 | (42.1) | 396 | (58.8) | 886 | (48.3) | |
| Persian | 645 | (55.5) | 264 | (39.1) | 908 | (49.5) | |
| English | 19 | (1.6) | 6 | (0.9) | 25 | (1.4) | |
| Urdu | 9 | (0.8) | 8 | (1.2) | 17 | (0.9) | |
| Number of days walked so far b | |||||||
| 1 day | 185 | (19.3) | 112 | (22.3) | 297 | (20.3) | |
| 2–3 days | 518 | (54.1) | 302 | (60.0) | 820 | (56.2) | |
| 4–7 days | 195 | (20.4) | 75 | (14.9) | 270 | (18.5) | |
| 8+ days | 59 | (6.2) | 14 | (2.8) | 73 | (5.0) | |
| Type of accommodation c | |||||||
| Mawkib (tent/outside) | 584 | (50.2) | 187 | (27.7) | <0.001 | 770 | (41.9) |
| Private house | 370 | (31.8) | 182 | (27.0) | 0.029 | 552 | (30.0) |
| Mosque/hussayniya | 276 | (23.7) | 254 | (37.7) | <0.001 | 530 | (28.9) |
| Permanent mawkib (built structure) | 242 | (20.8) | 165 | (24.5) | 0.07 | 407 | (22.2) |
| Hotel | 39 | (3.4) | 18 | (2.7) | 0.413 | 57 | (3.1) |
| Other | 90 | (7.7) | 62 | (9.2) | 0.278 | 152 | (8.3) |
| Source of food c | |||||||
| Mawkib (outside cooking) | 742 | (63.8) | 368 | (54.6) | <0.001 | 1110 | (60.4) |
| Mawkib (kitchen facility) | 508 | (43.7) | 435 | (64.5) | <0.001 | 943 | (51.3) |
| Private home food | 137 | (11.8) | 94 | (13.9) | 0.181 | 231 | (12.6) |
| Street food—donated | 496 | (42.6) | 327 | (48.4) | 0.016 | 822 | (44.7) |
| Street food—sold | 42 | (3.6) | 57 | (8.5) | <0.001 | 99 | (5.4) |
| Restaurant | 22 | (1.9) | 14 | (2.1) | 0.786 | 36 | (2.0) |
| Other | 10 | (0.9) | 7 | (1.0) | 0.702 | 17 | (0.9) |
| Male | Female | p-Value | Total | ||||
|---|---|---|---|---|---|---|---|
| Symptom | n | (%) | n | (%) | na | (%) | |
| Fever | 101 | (8.8) | 47 | (7.1) | 0.202 | 148 | (8.2) |
| Respiratory symptoms | |||||||
| Cough | 312 | (27.3) | 149 | (22.6) | 0.029 | 461 | (25.6) |
| DURATION (DAYS) | 0.098 | ||||||
| 0–2 | 222 | (19.1) | 80 | (11.9) | 302 | (16.4) | |
| 3–7 | 68 | (5.8) | 47 | (7.0) | 115 | (6.2) | |
| 8–14 | 2 | (0.2) | 4 | (0.6) | 6 | (0.33) | |
| 15–30 | 2 | (0.2) | 1 | (0.1) | 3 | (0.15) | |
| 31+ | 3 | (0.3) | 7 | (1.0) | 10 | (0.54) | |
| Sputum | 0.012 | ||||||
| YES | 155 | (13.3) | 55 | (8.5) | 210 | (11.4) | |
| NO | 157 | (13.5) | 93 | (14.4) | 250 | (13.6) | |
| Colour of sputum b | |||||||
| WHITE | 110 | (9.5) | 33 | (4.9) | 143 | (7.8) | |
| GREEN | 37 | (3.2) | 17 | (2.5) | 54 | (2.9) | |
| BROWN/BLACK | 8 | (0.7) | 2 | (0.3) | 10 | (0.5) | |
| BLOOD-STAINED | 1 | (0.1) | 1 | (0.1) | 2 | (0.1) | |
| Breathlessness | 130 | (11.4) | 88 | (13.5) | 0.196 | 218 | (12.1) |
| Sore throat | 213 | (18.8) | 109 | (16.6) | 0.231 | 322 | (18.0) |
| Cough+ fever + sore throat | 37 | (3.2) | 21 | (3.1) | 0.210 | 58 | (3.1) |
| Cough | Breathlessness | Fever | Any of These Symptoms | Total | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | (%) a | p-Value | n | (%) a | p-Value | n | (%) a | p-Value | n | (%) a | p-Value | nb | (%) c | |
| Gender (%) | 0.001 | 0.197 | 0.154 | 0.230 | ||||||||||
| Male | 284 | (25.1) | 107 | (9.5) | 97 | (8.5) | 362 | (32.1) | 1163 | (63.3) | ||||
| Female | 121 | (18.6) | 74 | (11.4) | 44 | (6.6) | 191 | (29.4) | 675 | (36.7) | ||||
| Age (years) (%) | <0.001 | <0.001 | 0.296 | 0.002 | ||||||||||
| 16–24 | 136 | (32.1) | 70 | (16.4) | 32 | (7.4) | 165 | (38.9) | 438 | (24.1) | ||||
| 25–44 | 169 | (20.7) | 75 | (9.1) | 68 | (8.2) | 237 | (29.0) | 841 | (46.2) | ||||
| 45–64 | 91 | (19.2) | 26 | (5.6) | 32 | (6.7) | 133 | (28.4) | 487 | (26.7) | ||||
| 65+ | 5 | (9.6) | 9 | (17.0) | 5 | (9.4) | 12 | (23.1) | 54 | (3.0) | ||||
| Recruitment station | <0.001 | 0.001 | 0.768 | <0.001 | ||||||||||
| 1 | 64 | (11.3) | 38 | (6.7) | 44 | (7.6) | 102 | (18.2) | 560 | (30.4) | ||||
| 2 | 340 | (28.5) | 143 | (12.0) | 96 | (8.0) | 449 | (37.7) | 1194 | (64.8) | ||||
| No of days walked so far (%) | <0.001 | <0.001 | 0.001 | <0.001 | ||||||||||
| 5 or fewer | 339 | (20.9) | 149 | (9.2) | 120 | (7.3) | 467 | (29.0) | 1671 | (93.2) | ||||
| 6+ | 66 | (55.9) | 32 | (27.8) | 21 | (17.4) | 86 | (72.9) | 122 | (6.8) | ||||
| Type of country of origin (%) d | 0.029 | 0.133 | 0.110 | 0.288 | ||||||||||
| High income | 2 | (5.4) | 5 | (14.3) | 0 | (0) | 7 | (19.4) | 37 | (2.0) | ||||
| Upper middle income | 390 | (23.1) | 174 | (10.3) | 132 | (7.7) | 530 | (31.5) | 1734 | (94.1) | ||||
| Low to lower middle income | 11 | (28.2) | 0 | (0) | 6 | (14.0) | 11 | (28.2) | 44 | (2.4) | ||||
| Unknown/missing | 2 | (9.1) | 2 | (8.0) | 3 | (12.0) | 5 | (20.8) | 27 | (1.5) | ||||
| Source of food | 0.001 | 0.135 | 0.497 | <0.001 | ||||||||||
| Mawkib (outside cooking) | ||||||||||||||
| Yes | 277 | (25.4) | 120 | (11.0) | 82 | (4.5) | 375 | (34.4) | 1111 | (60.3) | ||||
| No | 128 | (18.4) | 61 | (8.8) | 59 | (3.3) | 178 | (25.8) | 731 | (39.7) | ||||
| Mawkib (kitchen facility) | 0.016 | 0.752 | 0.005 | 0.141 | ||||||||||
| Yes | 189 | (20.4) | 95 | (10.3) | 57 | (6.1) | 273 | (29.5) | 945 | (51.3) | ||||
| No | 216 | (25.1) | 86 | (9.9) | 84 | (9.6) | 280 | (32.7) | 897 | (48.7) | ||||
| Home food | 0.763 | 0.207 | 0.002 | 0.957 | ||||||||||
| Yes | 49 | (21.9) | 17 | (7.7) | 29 | (12.8) | 68 | (30.9) | 231 | (12.5) | ||||
| No | 356 | (22.8) | 164 | (10.5) | 112 | (7.1) | 485 | (31.1) | 1611 | (87.5) | ||||
| Street food—donated | <0.001 | 0.512 | 0.797 | 0.001 | ||||||||||
| Yes | 141 | (17.5) | 86 | (10.6) | 65 | (8.0) | 217 | (27.2) | 824 | (44.7) | ||||
| No | 264 | (26.9) | 95 | (9.7) | 76 | (7.6) | 336 | (34.3) | 1018 | (55.3) | ||||
| Street food—sold | 0.189 | 0.775 | 0.547 | 0.622 | ||||||||||
| Yes | 27 | (28.1) | 9 | (9.3) | 6 | (6.2) | 32 | (33.3) | 99 | (5.4) | ||||
| No | 378 | (22.4) | 172 | (10.2) | 135 | (7.9) | 521 | (30.9) | 1743 | (94.6) | ||||
| Restaurant | 0.439 | 0.041 | 0.001 | 0.198 | ||||||||||
| Yes | 5 | (14.7) | 7 | (20.6) | 8 | (23.5) | 14 | (41.2) | 36 | (2.0) | ||||
| No | 400 | (22.8) | 174 | (9.9) | 133 | (7.5) | 539 | (30.9) | 1806 | |||||
| Other | 17 | (0.9) | ||||||||||||
| Preventive measures | ||||||||||||||
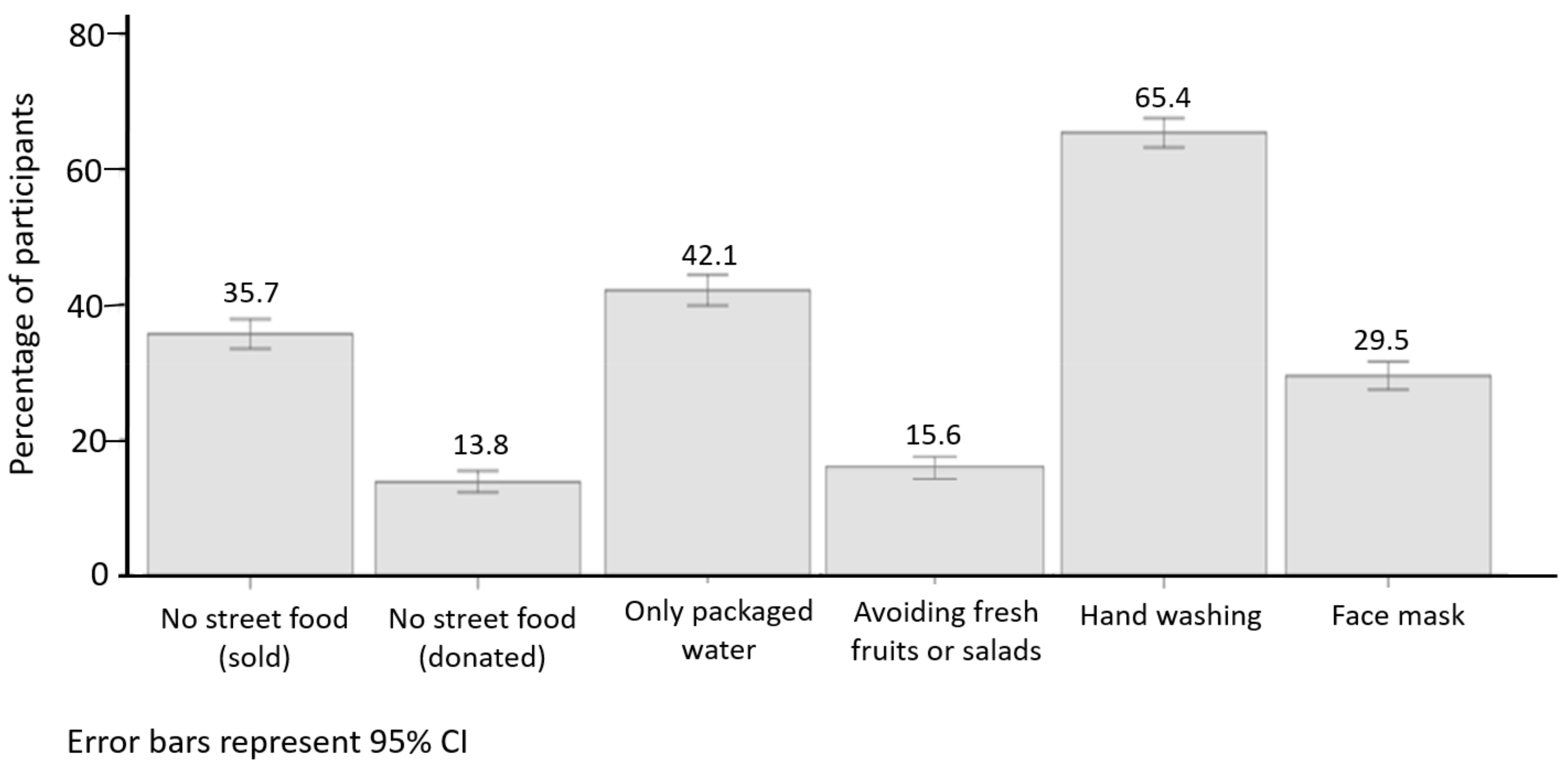
| Avoid street food—sold | 0.816 | 0.002 | <0.001 | <0.001 | ||||||||||
| Yes | 154 | (23.7) | 84 | (13.1) | 74 | (11.3) | 239 | (37.1) | 657 | (35.7) | ||||
| No | 251 | (22.1) | 97 | (8.5) | 67 | (5.8) | 314 | (27.6) | 1185 | (64.3) | ||||
| Avoid street food—donated | 0.237 | 0.615 | <0.001 | <0.001 | ||||||||||
| Yes | 69 | (27.4) | 23 | (9.2) | 38 | (15.0) | 107 | (42.8) | 254 | (13.8) | ||||
| No | 336 | (21.9) | 158 | (10.3) | 103 | (6.6) | 446 | (29.2) | 1588 | (86.2) | ||||
| Only packaged water (bottled or packed cups) | <0.001 | 0.076 | 0.491 | <0.001 | ||||||||||
| Yes | 127 | (16.7) | 66 | (8.7) | 56 | (7.3) | 196 | (25.8) | 776 | (42.1) | ||||
| No | 278 | (27.1) | 115 | (11.2) | 85 | (8.1) | 357 | (35.0) | 1066 | (57.9) | ||||
| Avoid fresh fruits or salads | <0.001 | 0.242 | 0.007 | 0.022 | ||||||||||
| Yes | 41 | (14.5) | 34 | (12.1) | 11 | (3.8) | 71 | (25.3) | 287 | (15.6) | ||||
| No | 364 | (24.2) | 147 | (9.8) | 130 | (8.5) | 482 | (32.2) | 1555 | (84.4) | ||||
| Handwashing | 0.091 | 0.026 | 0.073 | 0.005 | ||||||||||
| Yes | 271 | (22.8) | 133 | (11.3) | 103 | (8.6) | 394 | (33.3) | 1205 | (65.4) | ||||
| No | 134 | (22.4) | 48 | (7.9) | 38 | (6.2) | 159 | (26.7) | 637 | (34.6) | ||||
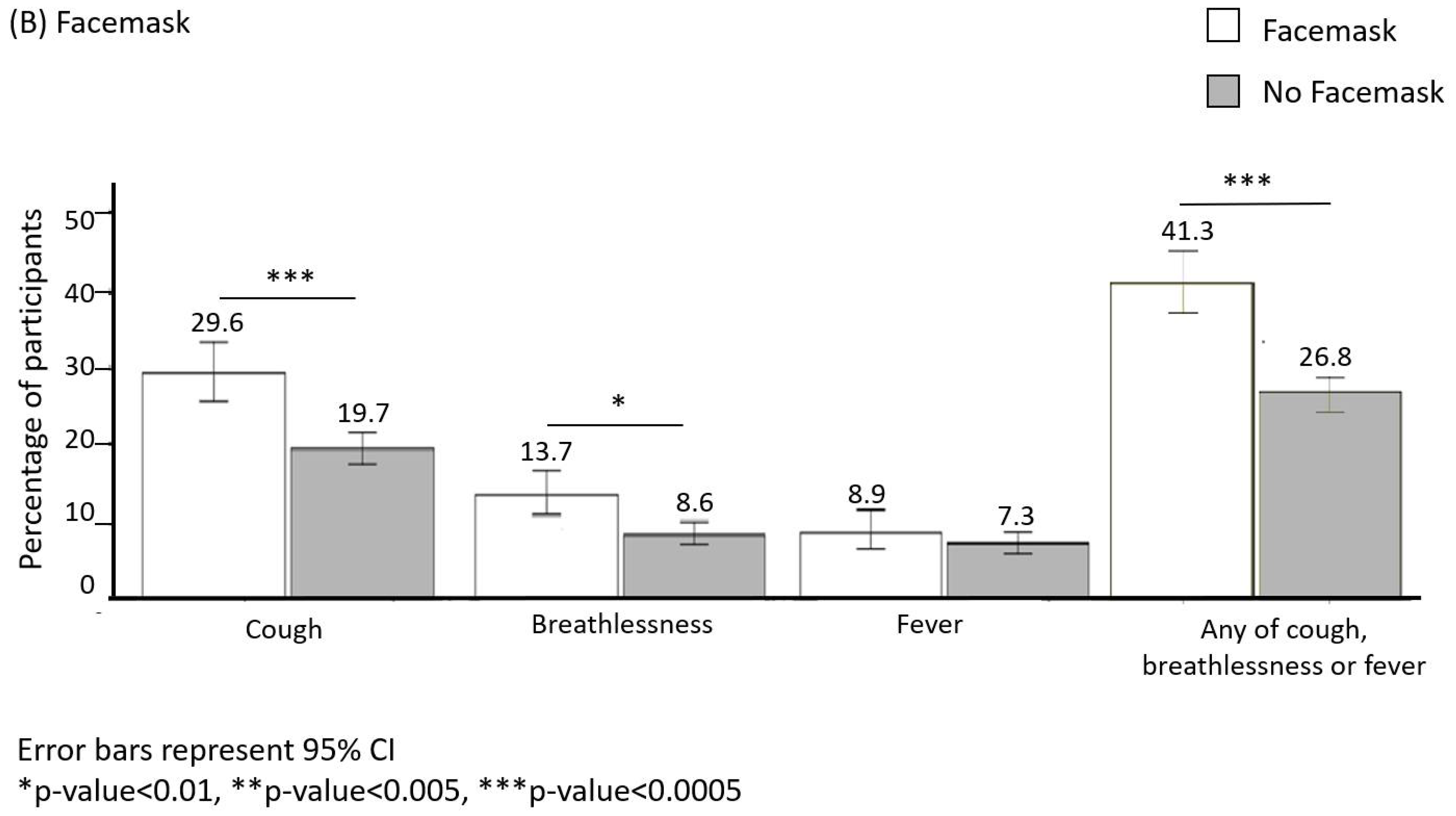
| Facemask | <0.001 | 0.001 | 0.243 | <0.001 | ||||||||||
| Yes | 157 | (29.6) | 73 | (13.7) | 48 | (8.9) | 217 | (41.3) | 543 | (70.5) | ||||
| No | 248 | (19.7) | 108 | (8.6) | 93 | (7.3) | 336 | (26.8) | 1299 | (29.5) | ||||
| Other | ||||||||||||||
| Up to date vaccination | 0.906 | 0.123 | 0.773 | 0.066 | ||||||||||
| Yes | 242 | (22.9) | 109 | (10.3) | 83 | (7.7) | 339 | (32.2) | 1072 | (60.6) | ||||
| No | 123 | (20.6) | 53 | (8.9) | 51 | (8.3) | 161 | (27.0) | 615 | (34.7) | ||||
| Don’t know | 19 | (23.5) | 13 | (16.0) | 5 | (6.2) | 28 | (34.6) | 81 | (4.6) | ||||
| Flu vaccination in the past year (%) | 0.357 | 0.200 | <0.001 | 0.532 | ||||||||||
| Yes | 57 | (20.4) | 36 | (13.0) | 21 | (7.4) | 79 | (28.7) | 279 | (16.0) | ||||
| No | 327 | (22.9) | 140 | (9.8) | 104 | (7.2) | 436 | (30.6) | 1425 | (81.5) | ||||
| Do not know | 4 | (9.1) | 3 | (6.8) | 15 | (34.1) | 21 | (47.7) | 44 | (2.5) | ||||
| Other vaccinations for this trip | 0.705 | 0.032 | <0.001 | 0.294 | ||||||||||
| Yes | 22 | (25.3) | 3 | (3.4) | 19 | (21.8) | 23 | (26.7) | 86 | (5.0) | ||||
| No | 394 | (23.5) | 175 | (10.6) | 117 | (7.0) | 528 | (32.2) | 1644 | (95.0) | ||||
| Missing | 80 | |||||||||||||
| Regular smoking | 0.025 | 0.002 | 0.447 | 0.163 | ||||||||||
| Yes | 86 | (26.3) | 49 | (14.9) | 23 | (6.9) | 111 | (33.9) | 327 | (18.8) | ||||
| No | 302 | (21.2) | 130 | (9.1) | 117 | (8.1) | 425 | (30.0) | 1417 | (81.3) | ||||
| Total (%) | 405 | (22.7) | 181 | (10.1) | 141 | (7.9) | 553 | (31.06) | ||||||
| Dependent Variable | Predictors a | p-Value b Bivariate | OR | 95% CI for OR | p-Value b Multivariate | AOR | 95% CI for AOR | ||
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | Lower | Upper | ||||||
| Cough | |||||||||
| Age | 0.392 | 1.00 | 0.99 | 1.00 | 0.009 | 0.99 | 0.98 | 1.00 | |
| Walked for 6+ days vs. walked for ≤5 days | <0.001 | 4.72 | 3.23 | 6.89 | <0.001 | 4.59 | 3.01 | 7.00 | |
| Use of facemask as a preventive measure vs. not using this measure | <0.001 | 1.86 | 1.49 | 2.32 | <0.001 | 2.71 | 2.08 | 3.53 | |
| Use of packaged water only as a preventive measure vs. not using this measure | <0.001 | 0.57 | 0.46 | 0.72 | <0.001 | 0.60 | 0.45 | 0.78 | |
| Avoiding fresh fruits/salads as a preventive measure vs. not using this measure | <0.001 | 0.54 | 0.39 | 0.76 | 0.007 | 0.58 | 0.39 | 0.86 | |
| Eating mawkib food (indoor kitchen facility) vs. not using this food source | 0.003 | 0.73 | 0.60 | 0.90 | 0.014 | 0.72 | 0.56 | 0.94 | |
| Eating donated street food vs. not using this food source | <0.001 | 0.60 | 0.49 | 0.75 | 0.001 | 0.66 | 0.51 | 0.85 | |
| Any of cough, fever, or breathlessness | |||||||||
| Walked for 6+ days vs. walked for ≤5 days | <0.001 | 6.60 | 4.33 | 10.04 | <0.001 | 7.20 | 4.64 | 11.20 | |
| Eating mawkib food (outside cooking) vs. not using this food source | <0.001 | 1.51 | 1.22 | 1.86 | 0.016 | 1.33 | 1.05 | 1.68 | |
| Use of facemask as a preventive measure vs. not using this measure | <0.001 | 1.92 | 1.55 | 2.38 | <0.001 | 2.47 | 1.95 | 3.13 | |
| Use of packaged water only as a preventive measure vs. not using this measure | <0.001 | 0.65 | 0.53 | 0.80 | <0.001 | 0.64 | 0.50 | 0.81 | |
| Eating donated street food vs. not using this food source | 0.001 | 0.71 | 0.58 | 0.88 | 0.013 | 0.76 | 0.61 | 0.94 | |
| Avoiding sold street food vs. not using this preventive measure | <0.001 | 1.54 | 1.26 | 1.90 | 0.007 | 1.37 | 1.09 | 1.72 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Ansari, F.; Mirzaei, M.; Al-Ansari, B.; Al-Ansari, M.B.; Abdulzahra, M.S.; Rashid, H.; Hill-Cawthorne, G.A.; Al Ansari, M.; Negin, J.; Conigrave, K. Health Risks, Preventive Behaviours and Respiratory Illnesses at the 2019 Arbaeen: Implications for COVID-19 and Other Pandemics. Int. J. Environ. Res. Public Health 2021, 18, 3287. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063287
Al-Ansari F, Mirzaei M, Al-Ansari B, Al-Ansari MB, Abdulzahra MS, Rashid H, Hill-Cawthorne GA, Al Ansari M, Negin J, Conigrave K. Health Risks, Preventive Behaviours and Respiratory Illnesses at the 2019 Arbaeen: Implications for COVID-19 and Other Pandemics. International Journal of Environmental Research and Public Health. 2021; 18(6):3287. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063287
Chicago/Turabian StyleAl-Ansari, Farah, Masoud Mirzaei, Basma Al-Ansari, Mohammad Basim Al-Ansari, Mohammed Saeed Abdulzahra, Harunor Rashid, Grant A. Hill-Cawthorne, Mustafa Al Ansari, Joel Negin, and Katherine Conigrave. 2021. "Health Risks, Preventive Behaviours and Respiratory Illnesses at the 2019 Arbaeen: Implications for COVID-19 and Other Pandemics" International Journal of Environmental Research and Public Health 18, no. 6: 3287. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063287