
Association between Bullying Victimization and Symptoms of Depression among Adolescents: A Moderated Mediation Analysis

Abstract
:1. Introduction
2. Methods
2.1. Study Participants
2.2. Measures
2.2.1. Social Anxiety Scale
2.2.2. Epidemiologic Studies Depression Scale
2.2.3. Bullying Victimization
2.2.4. Sleep Duration
2.3. Statistical Analyses
2.4. Ethics Statement
3. Results
3.1. Sample Characteristics
3.2. Descriptive Analyses
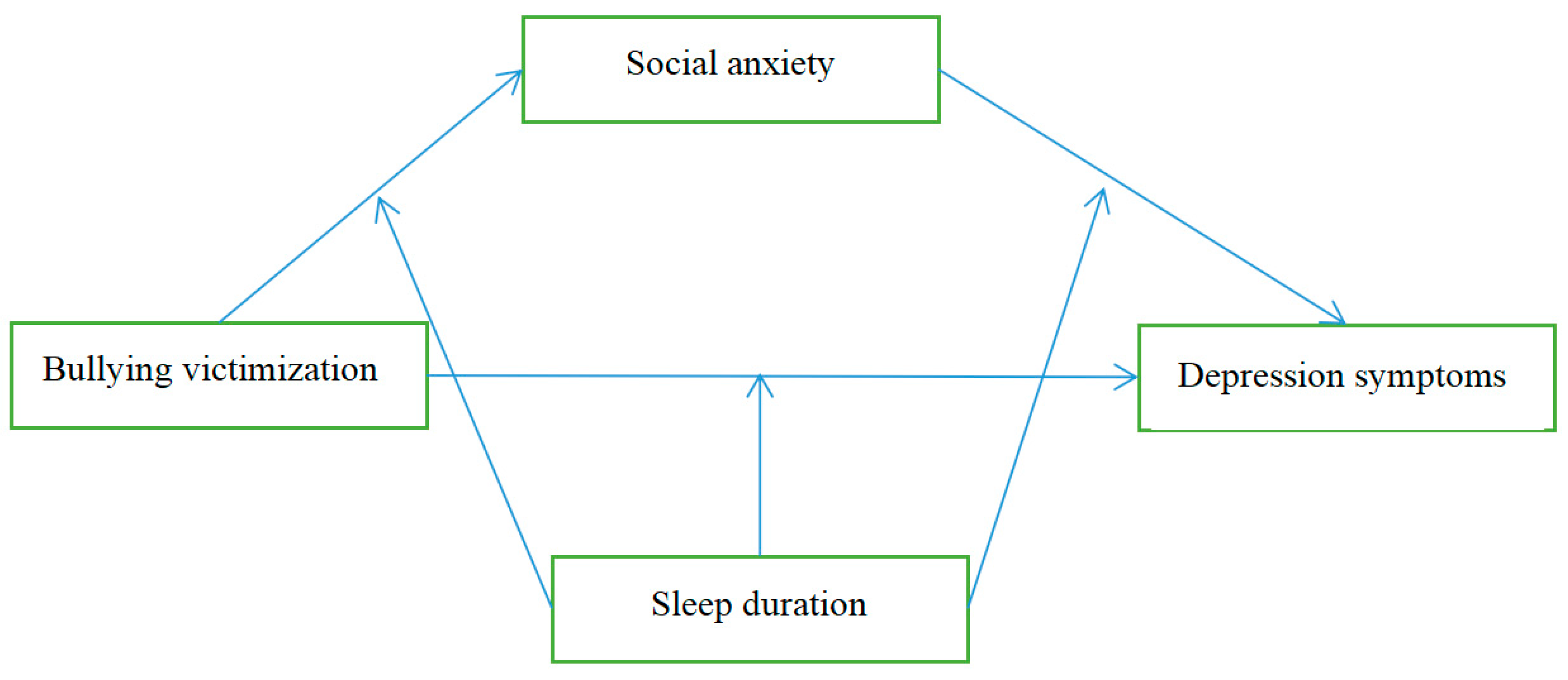
3.3. Testing for the Mediation Effect
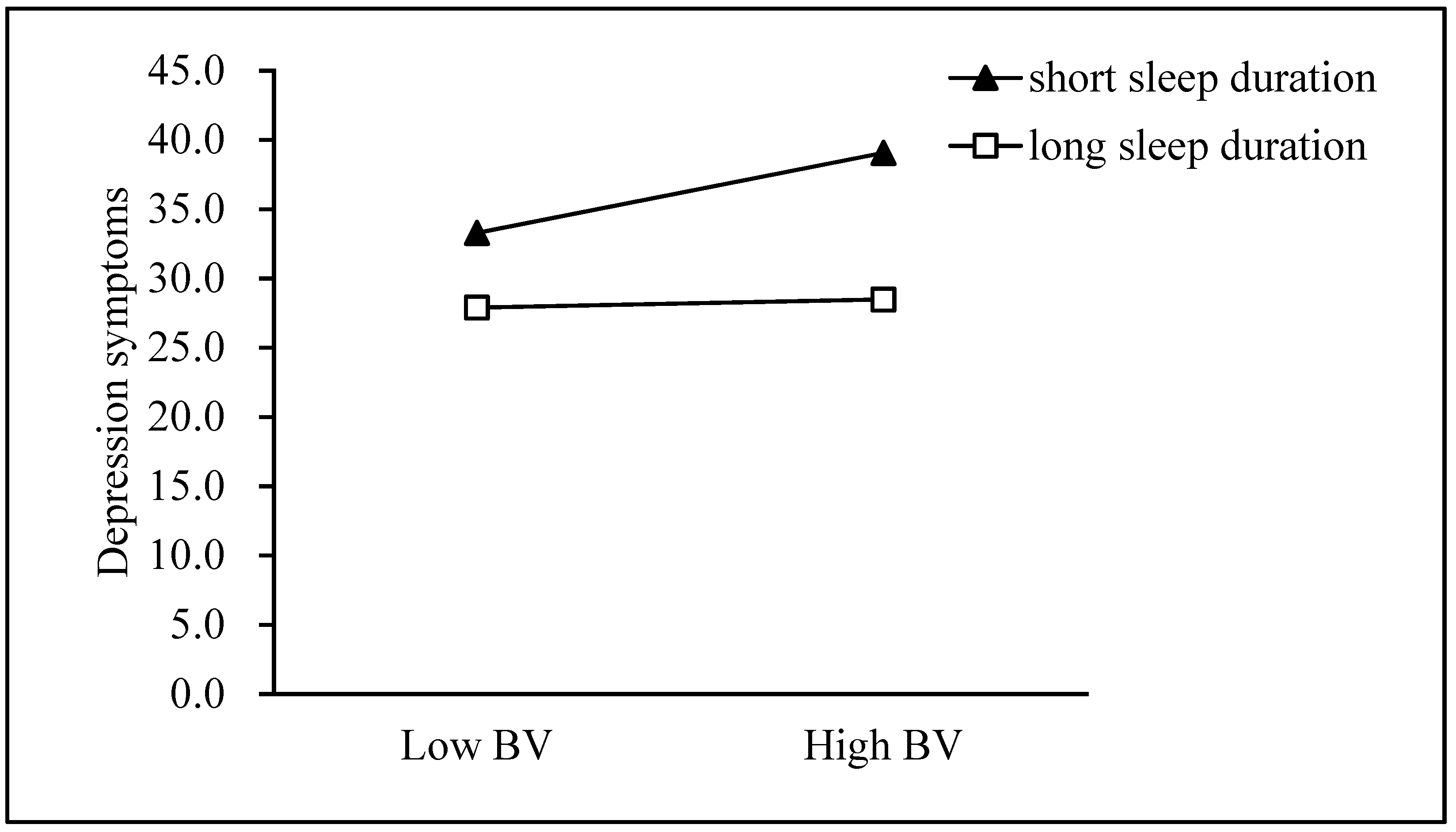
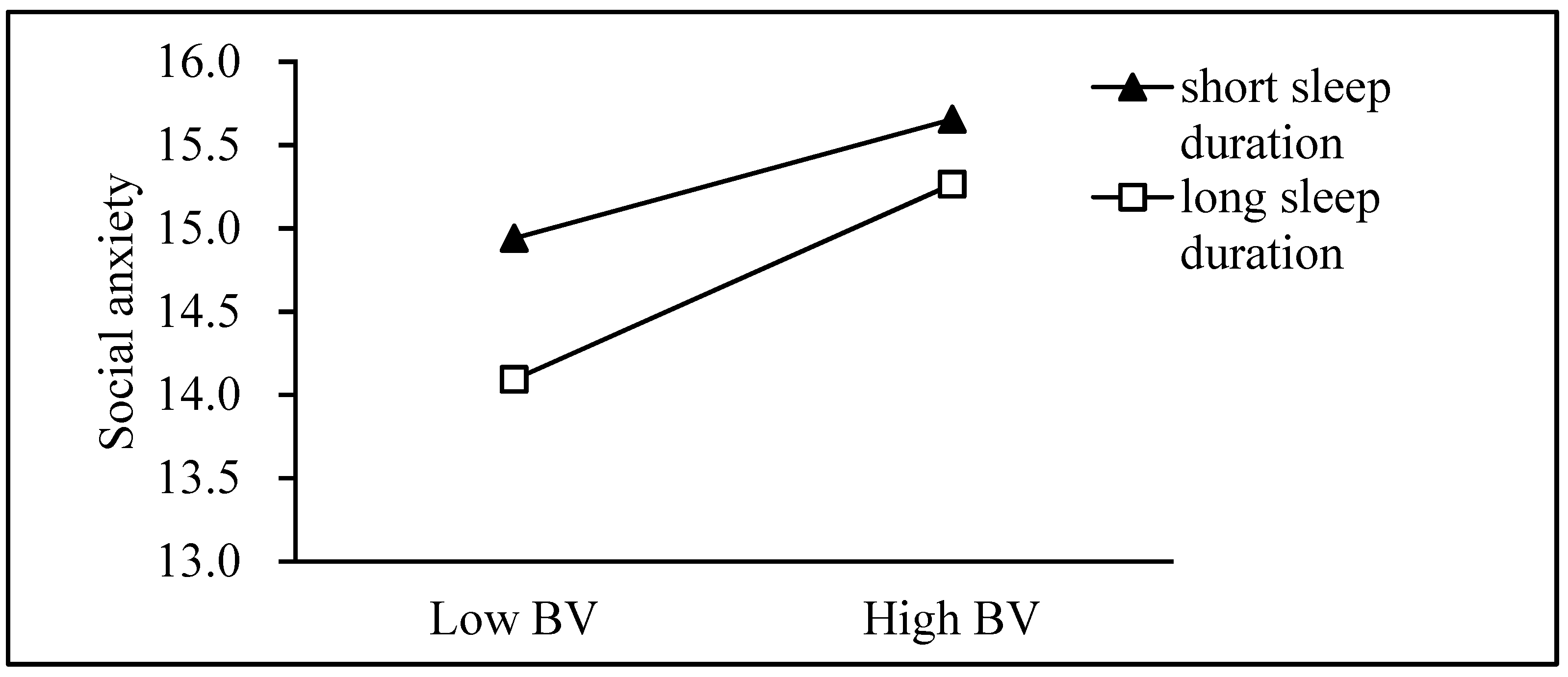
3.4. Testing for the Moderated Mediation Effect
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rao, W.W.; Hu, D.D.; Cao, X.L.; Wen, S.I.; Che, W.; Ng, C.; Ungvari, G. Prevalence of depressive symptoms in children and adolescents in China: A meta-analysis of observational studies. Psychiatry Res. 2019, 272, 790–796. [Google Scholar] [CrossRef]
- Li, J.Y.; Li, J.; Liang, J.H.; Qian, S.; Jia, R.X.; Wang, Y.Q.; Xu, Y. Depressive symptoms among children and adolescents in China: A systematic review and meta-analysis. Med. Sci. Monit. 2019, 25, 7459–7470. [Google Scholar] [CrossRef]
- Hankin, B.L. Future directions in vulnerability to depression among youth: Integrating risk factors and processes across multiple levels of analysis. J. Clin. Child Adolesc. Psychol. 2012, 41, 695–718. [Google Scholar] [CrossRef]
- Kendler, K.S.; Karkowski, L.M.; Prescott, C.A. Causal relationship between stressful life events and the onset of major depression. Am. J. Psychiatry 1999, 156, 837–841. [Google Scholar] [CrossRef]
- Aluede, O.; Adeleke, F.; Omoike, D.; Afen-Akpaida, J. A review of the extent, nature, characteristics and effects of bullying behaviour in schools. J. Instr. Psychol. 2008, 35, 151–158. [Google Scholar]
- Olweus, D. A profile of bullying at school. Educ. Leadersh. 2003, 60, 12–17. [Google Scholar] [CrossRef]
- Langford, R.; Bonnell, C.P.; Jones, E.H.; Pouliou, T.; Murphy, S.M.; Waters, E.; Komro, A.K.; Gibbs, L.F.; Magnus, D.; Campbell, R. The WHO Health Promoting School framework for improving the health and well-being of students and their academic achievement. Cochrane Database Syst. Rev. 2014, 4, CD008958. [Google Scholar] [CrossRef]
- Wei, H.S.; Williams, J.H.; Chen, J.K.; Chang, H.Y. The effects of individual characteristics, teacher practice, and school organizational factors on students’ bullying: A multilevel analysis of public middle schools. Child. Youth Serv. Rev. 2010, 32, 137–143. [Google Scholar] [CrossRef]
- Griffin, R.S.; Gross, A.M. Childhood bullying: Current empirical findings and future directions for research. Aggress. Violent Behav. 2004, 9, 379–400. [Google Scholar] [CrossRef]
- Salmivalli, C. Is there an age decline in victimization by peers at school? Educ. Res. 2002, 44, 269–277. [Google Scholar] [CrossRef]
- Tucker, C.J.; Finkelhor, D.; Turner, H.; Shattuck, A.M. Sibling and peer victimization in childhood and adolescence. Child. Abus. Negl. 2014, 38, 1599–1606. [Google Scholar] [CrossRef]
- Fox, K.R.; Millner, A.J.; Franklin, J.C. Classifying nonsuicidal overdoses: Nonsuicidal self-injury, suicide attempts, or neither? Psychiatry Res. 2016, 244, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Koh, Y.J.; Leventhal, B. School bullying and suicidal risk in korean middle school students. Pediatrics 2005, 115, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.Q.; Chen, M.T.; Zhu, Y.H.; Chan, K.L.; Ip, P. Health correlates, addictive behaviors, and peer victimization among adolescents in China. World J. Pediatr. 2018, 14, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Ford, R.; King, T.; Priest, N.; Kavanagh, A. Bullying and mental health and suicidal behaviour among 14- to 15-year-olds in a representative sample of Australian children. Aust. N. Z. J. Psychiatry 2017, 51, 897–908. [Google Scholar] [CrossRef] [Green Version]
- Moore, S.E.; Norman, R.E.; Sly, P.D.; Whitehouse, A.J.; Zubrick, S.R.; Scott, J. Adolescent peer aggression and its association with mental health and substance use in an Australian cohort. J. Adolesc. 2014, 37, 11–21. [Google Scholar] [CrossRef] [Green Version]
- Wolke, D.; Copeland, W.E.; Angold, A.; Costello, E.J. Impact of bullying in childhood on adult health, wealth, crime, and social outcomes. Psychol. Sci. 2013, 24, 1958–1970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, J.G.; Moore, E.S.; Sly, P.D.; Norman, E.R. Bullying in children and adolescents: A modifiable risk factor for mental illness. Aust. N. Z. J. Psychiatry 2013, 48, 209–212. [Google Scholar] [CrossRef]
- Van der Vermulst, A.; van Rooij, A.J.; Scholte, R.; Van, D.M.D. The bidirectional relationships between online victimization and psychosocial problems in adolescents: A comparison with real-life victimization. J. Youth Adolesc. 2014, 43, 790–802. [Google Scholar] [CrossRef] [Green Version]
- Chu, X.W.; Fan, C.Y.; Chai, H.Y.; Song, K. Victimization and social anxiety: The mediating role of social self-efficacy. Chin. J. Clin. Psychol. 2016, 24, 1051–1054. [Google Scholar]
- Staring, A.B.P.; Ter Huurne, M.A.B.; Mark, V.D.G. Cognitive Behavioral Therapy for negative symptoms (CBT-n) in psychotic disorders: A pilot study. J. Behav. Ther. Exp. Psychiatry 2013, 44, 300–306. [Google Scholar] [CrossRef]
- Rapee, R.M.; Spence, S.H. The etiology of social phobia: Empirical evidence and an initial model. Clin. Psychol. Rev. 2004, 24, 737–767. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, R.S. Bully-victims: An analysis of subtypes and risk characteristics. J. Interpers. Violence 2018, 886260517741213. [Google Scholar] [CrossRef] [PubMed]
- Storch, E.A.; Masia-Warner, S.C. The relationship of peer victimization to social anxiety and loneliness in adolescent females. J. Adolesc. 2004, 27, 351–362. [Google Scholar] [CrossRef]
- Pabian, S.; Vandebosch, H. An investigation of short-term longitudinal associations between social anxiety and victimization and perpetration of traditional bullying and cyberbullying. J. Youth Adolesc. 2015, 45, 328–339. [Google Scholar] [CrossRef] [PubMed]
- Storch, E.A.; Brassard, M.R.; Masia-Warner, C.L. The relationship of peer victimization to social anxiety and loneliness in adolescence. Child Study J. 2003, 33, 1–18. [Google Scholar]
- Starr, L.R.; Davila, J. Temporal patterns of anxious and depressed mood in generalized anxiety disorder: A daily diary study. Behav. Res. Ther. 2012, 50, 131–141. [Google Scholar] [CrossRef] [Green Version]
- Beesdo, K.; Bittner, A.; Pine, D.S.; Stein, M.B.; Höfler, M.; Lieb, R.; Wittchen, H.-U. Incidence of social anxiety disorder and the consistent risk for secondary depression in the first three decades of life. Arch. Gen. Psychiatry 2007, 64, 903–912. [Google Scholar] [CrossRef] [Green Version]
- Nordahl, H.; Nordahl, H.M.; Vogel, P.A.; Wells, A. Explaining depression symptoms in patients with social anxiety disorder: Do maladaptive metacognitive beliefs play a role? Clin. Psychol. Psychother. 2018, 25, 457–464. [Google Scholar] [CrossRef]
- Xiao-Wei, W.U.; Huang, L.; Xiao-Qin, H.E.; Tang, H.B.; Wei-Dan, P.U.; Clinic, P. Social anxiety, aggression and depression: The mediating of regulatory emotional self-efficacy. Chin. J. Clin. Psychol. 2015, 23, 804–807. [Google Scholar]
- Rudolph, K.D.; Flynn, M.; Abaied, J.L. A developmental perspective on interpersonal theories of youth depression. In Handbook of Depression in Children and Adolescents; Springer: New York, NY, USA, 2008; pp. 79–102. [Google Scholar]
- Rubin, K.H.; Coplan, R.J.; Bowker, J.C. Social withdrawal in childhood. Annu. Rev. Psychol. 2009, 60, 141–171. [Google Scholar] [CrossRef] [Green Version]
- Nock, M.K.; Favazza, A.R. Nonsuicidal Self-Injury: Definition and Classification. In Understanding Nonsuicidal Self-Injury: Origins, Assessment, and Treatment; American Psychological Association (APA): Washington, DC, USA, 2009; pp. 9–18. [Google Scholar] [CrossRef]
- Baglioni, C.; Spiegelhalder, K.; Lombardo, C.; Riemann, D. Sleep and emotions: A focus on insomnia. Sleep Med. Rev. 2010, 14, 227–238. [Google Scholar] [CrossRef]
- Zuculo, G.M.; Knap, C.C.F.; Pinato, L. Correlation between sleep and quality of life in cerebral palsy. CoDAS 2014, 26, 447–456. [Google Scholar] [CrossRef]
- Barnes, C.M.; Schaubroeck, J.; Huth, M.; Ghumman, S. Lack of sleep and unethical conduct. Organ. Behav. Hum. Decis. Process. 2011, 115, 169–180. [Google Scholar] [CrossRef]
- Baumeister, R.F.; Vohs, K.D. Self-regulation, ego depletion, and motivation. Soc. Personal. Psychol. Compass. 2007, 1, 115–128. [Google Scholar] [CrossRef]
- Hamilton, N.A.; Nelson, C.A.; Stevens, N.; Kitzman, H. Sleep and psychological well-being. Soc. Indic. Res. 2007, 82, 147–163. [Google Scholar] [CrossRef]
- Kanyinga, S.H.; Chaput, J.P.; Hamilton, H.A.; Colman, I. Bullying involvement, psychological distress, and short sleep duration among adolescents. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 1371–1380. [Google Scholar] [CrossRef]
- Hysing, M.; Askeland, K.G.; La Greca, A.M.; Solberg, M.E.; Breivik, K.; Sivertsen, B. Bullying involvement in adolescence: Implications for sleep, mental health, and academic outcomes. J. Interpers. Violence 2019, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dov, Z.; Orna, T.; Rachel, E.; Peretz, L. The effects of sleep loss on medical residents’ emotional reactions to work events: A cognitive-energy model. Sleep 2005, 28, 47–54. [Google Scholar] [CrossRef] [Green Version]
- Muto, V.; Jaspar, M.; Meyer, C.; Kussé, C.; Chellappa, S.L.; Degueldre, C.; Balteau, E.; Bourdiec, A.S.L.; Luxen, A.; Middleton, B.; et al. Local modulation of human brain responses by circadian rhythmicity and sleep debt. Science 2016, 353, 687–690. [Google Scholar] [CrossRef] [PubMed]
- Richardson, C.; Oar, E.; Fardouly, J.; Magson, N.; Johnco, C.; Forbes, M.; Rapee, R. The moderating role of sleep in the relationship between social isolation and internalising problems in early adolescence. Child. Psychiatry Hum. Dev. 2019, 50, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Blake, M.J.; Trinder, J.A.; Allen, N.B. Mechanisms underlying the association between insomnia, anxiety, and depression in adolescence: Implications for behavioral sleep interventions. Clin. Psychol. Rev. 2018, 63, 25–40. [Google Scholar] [CrossRef] [PubMed]
- Fenigstein, A.; Scheier, M.F.; Buss, A.H. Public and private self-consciousness: Assessment and theory. J. Consult. Clin. Psychol. 1975, 43, 522–527. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Zhou, Z.; Fan, C.; Sun, X. Other-oriented variables affect adolescents loneliness and social anxiety: Interpersonal competence as a mediator. Psychol. Dev. Educ. 2012, 28, 413–420. [Google Scholar]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Zhang, J. Development of the Chinese age norms of CES-D in urban area. Chin. Ment. Health J. 2010, 24, 139–143. [Google Scholar]
- Solberg, M.E.; Olweus, D. Prevalence estimation of school bullying with the Olweus Bully/Victim Questionnaire. Aggress. Behav. 2003, 29, 239–268. [Google Scholar] [CrossRef]
- Wang, H.; Zhou, X.; Lu, C.; Wu, J.; Deng, X.; Hong, L.; Gao, X.; He, Y. Adolescent bullying involvement and psychosocial aspects of family and school life: A cross-sectional study from Guangdong Province in China. PLoS ONE 2012, 7, e38619. [Google Scholar] [CrossRef] [Green Version]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; The Guilford Press: New York, NY, USA, 2014; Volume 51, pp. 335–337. [Google Scholar]
- Wang, H.; Zhou, X.; Lu, C.; Wu, J.; Deng, X.; Hong, L. Problematic internet use in high school students in Guangdong Province, China. PLoS ONE 2011, 6, e19660. [Google Scholar] [CrossRef]
- Surveillance, I.; English, O. Centers for Disease Control and Prevention World Health Organization. 2013. Available online: https://www.who.int/vaccine_safety/initiative/communication/network/nip/en/ (accessed on 16 October 2020).
- Jong, D.P.J.; Sportel, B.E.; Hullu, D.E.; Nauta, M.H. Co-occurrence of social anxiety and depression symptom in adolescence: Differential links with implicit and explicit self-esteem? Psychol. Med. Lond. 2012, 42, 475–484. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Schatzberg, A.F. Social phobia and depression: Prevalence and comorbidity. J. Psychosom. Res. 2010, 68, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Biggs, B.K.; Nelson, J.M.; Sampilo, M.L. Peer relations in the anxiety-depression link: Test of a mediation model. Anxiety Stress Coping 2010, 23, 431–447. [Google Scholar] [CrossRef] [PubMed]
- Gazelle, H.; Ladd, G.W. Anxious solitude and peer exclusion: A diathesis-stress model of internalizing trajectories in childhood. Child. Dev. 2003, 74, 257–278. [Google Scholar] [CrossRef]
- Prinstein, M.J.; Greca, A.M.L. Peer crowd affiliation and internalizing distress in childhood and adolescence: A longitudinal follow-back study. J. Res. Adolesc. 2002, 12, 325. [Google Scholar] [CrossRef]
- McLaughlin, K.A.; King, K. Developmental trajectories of anxiety and depression in early adolescence. J. Abnorm. Child. Psychol. 2015, 43, 311–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, P.I.; Fua, K.; Huang, Y.; Bonelli, W.; Xiong, H.; Barnes, E.L.; Teachman, A.B. Using mobile sensing to test clinical models of depression, social anxiety, state affect, and social isolation among college students. J. Med. Internet Res. 2017, 19, e62. [Google Scholar] [CrossRef]
- Walker, M.P.; Els, V.D.H. Overnight therapy? The role of sleep in emotional brain processing. Psychol. Bull. 2009, 135, 731–748. [Google Scholar] [CrossRef] [Green Version]
- Donoghue, C.; Meltzer, L. Sleep disturbances in adolescents involved in bullying. Sleep 2017, 40, A361. [Google Scholar] [CrossRef] [Green Version]
- Tu, K.M.; Erath, S.A.; El-Sheikh, M. Peer victimization and adolescent adjustment: The moderating role of sleep. J. Abnorm. Child Psychol. 2015, 43, 1447–1457. [Google Scholar] [CrossRef] [Green Version]
- Baum, K.T.; Desai, A.; Field, J.; Miller, L.E.; Rausch, J.R.; Beebe, D.W. Sleep restriction worsens mood and emotion regulation in adolescents. J. Child. Psychol. Psychiatry 2014, 55, 180–190. [Google Scholar] [CrossRef] [Green Version]
- Vandekerckhove, M.; Wang, Y.L. Emotion, emotion regulation and sleep: An intimate relationship. AIMS Neurosci. 2018, 5, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Colten, H.; Altevogt, B.B.M. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem; Committee on Sleep Medicine and Research, The National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Bei, B.; Wiley, J.F.; Allen, N.B.; Trinder, J.A. Cognitive vulnerability model on sleep and mood in adolescents under naturalistically restricted and extended sleep opportunities. Sleep 2015, 38, 453–461. [Google Scholar] [CrossRef] [Green Version]
- Reiss, S.; McNally, R.J. The expectancy model of fear. Theor. Issues Behav. Ther. 1985, 4, 107–121. [Google Scholar]
- Otto, M.W.; Eastman, A.; Lo, S.; Hearon, B.A.; Bickel, W.K.; Zvolensky, M.; Smits, J.A.; Doan, S.N. Anxiety sensitivity and working memory capacity: Risk factors and targets for health behavior promotion. Clin. Psychol. Rev. 2016, 49, 67–78. [Google Scholar] [CrossRef]
- Babson, K.A.; Trainor, C.D.; Bunaciu, L.; Feldner, M.T. An Examination of anxiety sensitivity as a moderator of the relation between sleep anticipatory anxiety and sleep onset latency. J. Cogn. Psychother. 2008, 22, 258–270. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | n | % |
|---|---|---|
| Age | 13.39 ± 1.03 | - |
| Gender | ||
| male | 1494 | 50.5 |
| female | 1462 | 49.5 |
| Only child | ||
| yes | 1966 | 66.5 |
| no | 990 | 33.5 |
| Residence | ||
| urban | 1459 | 49.4 |
| rural | 1497 | 50.6 |
| Grade | ||
| one | 987 | 33.4 |
| two | 983 | 33.3 |
| three | 986 | 33.3 |
| Residence in school | ||
| yes | 421 | 14.2 |
| no | 2535 | 85.8 |
| Variables | M | SD | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|---|
| Bullying victimization | 6.55 | 1.36 | 1 | |||
| Social anxiety | 14.75 | 5.04 | 0.121 ** | 1 | ||
| Depression | 31.99 | 10.42 | 0.491 ** | 0.276 ** | 1 | |
| Sleep duration | 7.80 | 1.32 | −0.232 ** | −0.081 ** | −0.460 ** | 1 |
| Independent Variables | Model 1 (Depressive Symptoms) | Model 2 (Social Anxiety) | Model 3 (Depressive Symptoms) | |||
|---|---|---|---|---|---|---|
| β | t | β | t | β | t | |
| Bullying victimization | 0.11 | 5.81 ** | 0.44 | 6.53 ** | ||
| Social anxiety | 0.46 | 14.18 ** | ||||
| R2 | 0.110 | 0.143 | 0.299 | |||
| F | 33.73 ** | 41.252 ** | 251.027 ** | |||
| Model effect | Effect | SE | t | |||
| Total effect | 1.85 | 0.12 | 15.23 ** | |||
| Direct effect | 1.62 | 0.12 | 14.01 ** | |||
| Indirect effect | 0.23 | 0.05 | 95% CI (0.14–0.33) | |||
| Independent Variables | Model 1 (Depressive Symptoms) | Model 2 (Social Anxiety) | Model 3 (Depressive Symptoms) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | SE | t | β | SE | t | β | SE | t | |
| Bullying victimization | 0.24 | 0.13 | 14.14 *** | 0.13 | 0.08 | 5.95 *** | 0.22 | 0.13 | 13.29 *** |
| Sleep duration | −0.33 | 0.12 | −22.33 *** | −0.07 | 0.07 | −3.45 *** | −0.32 | 0.11 | −22.40 *** |
| Bullying victimization * sleep duration | −0.29 | 0.06 | −16.95 *** | 0.09 | 0.04 | 2.28 ** | −0.29 | 0.06 | −17.10 *** |
| Social anxiety | 0.21 | 0.03 | 15.20 *** | ||||||
| Social anxiety * sleep duration | −0.08 | 0.02 | −5.84 *** | ||||||
| R2 | 0.427 | 0.141 | 0.477 | ||||||
| F | 734.169 *** | 190.494 *** | 538.474 *** | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mei, S.; Hu, Y.; Sun, M.; Fei, J.; Li, C.; Liang, L.; Hu, Y. Association between Bullying Victimization and Symptoms of Depression among Adolescents: A Moderated Mediation Analysis. Int. J. Environ. Res. Public Health 2021, 18, 3316. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063316
Mei S, Hu Y, Sun M, Fei J, Li C, Liang L, Hu Y. Association between Bullying Victimization and Symptoms of Depression among Adolescents: A Moderated Mediation Analysis. International Journal of Environmental Research and Public Health. 2021; 18(6):3316. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063316
Chicago/Turabian StyleMei, Songli, Yueyang Hu, Mengzi Sun, Junsong Fei, Chuanen Li, Leilei Liang, and Yuanchao Hu. 2021. "Association between Bullying Victimization and Symptoms of Depression among Adolescents: A Moderated Mediation Analysis" International Journal of Environmental Research and Public Health 18, no. 6: 3316. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063316