
Contextualizing Evidence for Action on Diabetes in Low-Resource Settings—Project CEAD Part-II, Strengthening the Health System: A Mixed-Methods Study Protocol

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Goals
- To evaluate the implementation of diabetes care according to the 2017 Clinical Practice Guideline [12] in two health districts in Ecuador.
- To use local knowledge and opinions to understand the observed weaknesses, their impact on health equity and identify how local health systems might be strengthened.
- To assess the feasibility and effectiveness (in the short-medium term) of context-led health systems innovations to improve diabetes care locally.
2.2. Setting
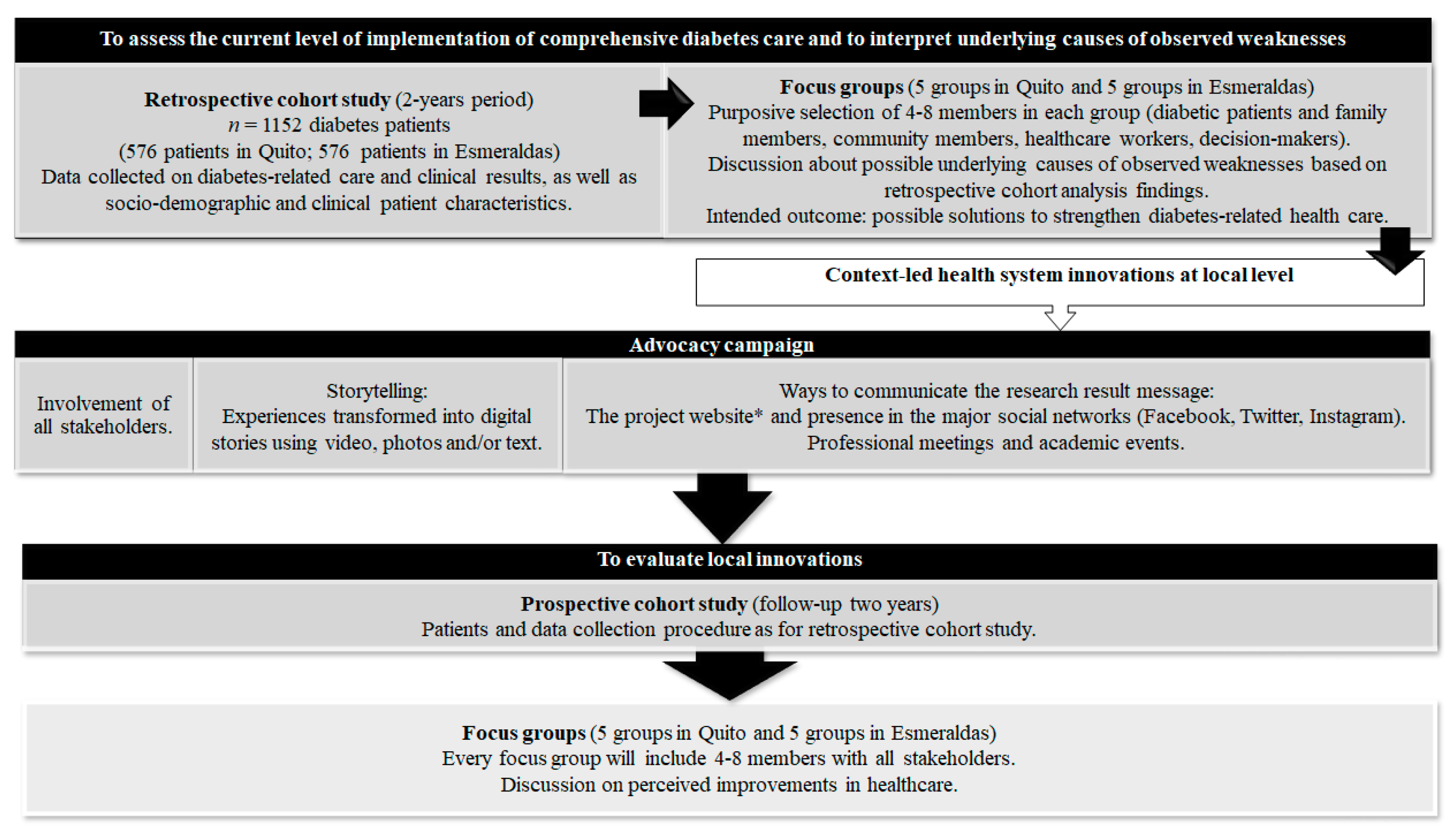
2.3. Study Design
2.3.1. Retrospective Cohort Study
- Study population:
- Data collection procedure:
- Outcomes
- Disease control: Defined in two dimensions. Firstly, biochemical control based on the last laboratory result of glycated hemoglobin or blood glucose, recorded in the year of study. The second dimension will be health-related quality of life, assessed using the DHP-18 questionnaire previously validated in Ecuador.
- Access to healthcare: Care process indicators that represent the proportion of the patients who undergo the care processes recommended by the CPG to manage the disease. We will obtain the care frequency for each patient as a quantitative value and will also categorize those care indicators that are recommended with greater periodicity in the CPG.
- 3.
- Control of complication risk factors: Care result indicators that determine proportion of patients who meet the standards of diabetes care and the clinical objectives during the year of study (January 2019 to December 2020).
- 4.
- Measurements of diabetes-related behaviors/conditions: Access to medication (self-reported) and social support obtained from a standardized questionnaire, and patient information received, self-reported.
- 5.
- Resources used due to decompensation of the disease and/or complications.
- 6.
- Disease complications (as indicators that measure the proportion of patients with complications occurring that could result from insufficient control of the disease).
- Analysis
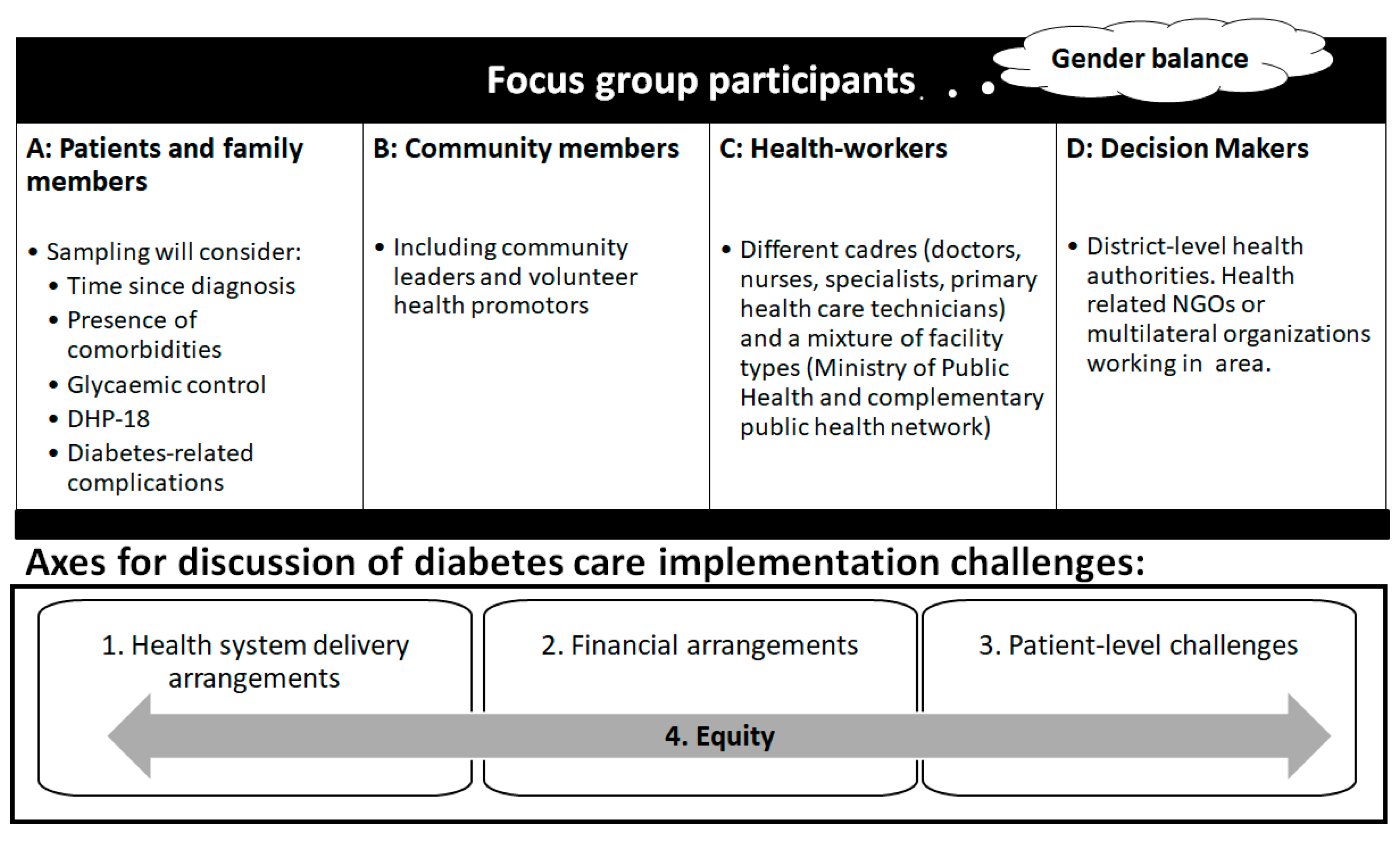
2.3.2. Focus Groups
- Participants
- Procedures
- Analysis
2.3.3. Transforming Findings into Innovations—Advocacy Campaign
- Getting the facts (research and data collection): The study will generate context-specific knowledge on the implementation of diabetes recommendations in participating communities.
- Building support: The participation of stakeholders (patients and family members, community members, healthcare workers and decision-makers) in discussion groups will enable us to influence public policy as well as health services and community attitudes. This will motivate the community-based movements to improve the situation and to implement context-specific policies that prevent morbidity and mortality from diabetes and avoid new cases.
- Developing goals and strategies: The objectives and strategies will emerge from the discussion groups with the participation of stakeholders. Therefore, this strategy will have a higher likelihood of success than externally imposed ones. As we have previously described, we will evaluate the possible improvements through changes in the pre-defined outcomes (Table 2).
- Communicating our message: The project has several ways to reach the largest possible audience (both in the community and in decision-makers) as described below.
- Storytelling:
- Ways to communicate the research results:
2.3.4. Cohort Follow-Up
- Study population:
- Data collection procedure:
- Outcomes:
- Analysis:
2.4. Ethics and Dissemination
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO “Noncommunicable Diseases (NCD)” Global Health Observatory. Available online: http://www.who.int/gho/ncd/en/ (accessed on 13 May 2020).
- Chatterjee, S.; Khunti, K.; Davies, M.J. Type 2 Diabetes. Lancet 2017, 389, 2239–2251. [Google Scholar] [CrossRef]
- Allotey, P.; Davey, T.; Reidpath, D.D. NCDs in Low and Middle-Income Countries—Assessing the Capacity of Health Systems to Respond to Population Needs. BMC Public Health 2014, 14, S1. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases: 2013–2020; WHO: Geneva, Switzerland, 2013; ISBN 978-92-4-150623-6. [Google Scholar]
- International Diabetes Federation. The IDF Diabetes Atlas, 7th ed.; International Diabetes Federation: Brussels, Belgium, 2015; ISBN 78-2-930229-81-2. [Google Scholar]
- Røttingen, J.-A.; Regmi, S.; Eide, M.; Young, A.J.; Viergever, R.F.; Årdal, C.; Guzman, J.; Edwards, D.; Matlin, S.A.; Terry, R.F. Mapping of Available Health Research and Development Data: What’s There, What’s Missing, and What Role Is There for a Global Observatory? Lancet 2013, 382, 1286–1307. [Google Scholar] [CrossRef]
- Manne-Goehler, J.; Geldsetzer, P.; Agoudavi, K.; Andall-Brereton, G.; Aryal, K.K.; Bicaba, B.W.; Bovet, P.; Brian, G.; Dorobantu, M.; Gathecha, G.; et al. Health System Performance for People with Diabetes in 28 Low- and Middle-Income Countries: A Cross-Sectional Study of Nationally Representative Surveys. PLoS Med. 2019, 16, e1002751. [Google Scholar] [CrossRef] [Green Version]
- Roglic. WHO Global report on diabetes: A summary. Int. J. Non-Commun. Dis. 2016, 1, 3–8. [Google Scholar] [CrossRef]
- Steyn, K.; Lombard, C.; Gwebushe, N.; Fourie, J.M.; Everett-Murphy, K.; Zwarenstein, M.; Levitt, N.S. Implementation of National Guidelines, Incorporated within Structured Diabetes and Hypertension Records at Primary Level Care in Cape Town, South Africa: A Randomised Controlled Trial. Glob. Health Action 2013, 6, 20796. [Google Scholar] [CrossRef] [PubMed]
- Kalain, A.; Omole, O.B. Lifestyle Advice, Processes of Care and Glycaemic Control amongst Patients with Type 2 Diabetes in a South African Primary Care Facility. Afr. J. Prim. Health Care Fam. Med. 2020, 12, a2163. [Google Scholar] [CrossRef] [PubMed]
- El Instituto Nacional de Estadística y Censos (INEC). Anuario de Estadísticas Vitales -Nacimientos y Defunciones 2018. Quito, Ecuador. Available online: https://www.ecuadorencifras.gob.ec/nacimientos_y_defunciones/ (accessed on 20 May 2020).
- Ministry of Public Health Ecuador Clinical Practice Guideline for Type 2 Diabetes Mellitus. 1st Edition. Quito, Ecuador. Available online: https://www.salud.gob.ec/wp-content/uploads/downloads/2017/05/Diabetes-mellitus_GPC.pdf (accessed on 15 May 2020).
- National Institute of Health and Care Excellence (NICE). Type 2 Diabetes Management. Clinical Guidance Update (NG28). Available online: https://www.nice.org.uk/guidance/ng28 (accessed on 17 May 2020).
- Ridde, V.; Pérez, D.; Robert, E. Using Implementation Science Theories and Frameworks in Global Health. BMJ Glob. Health 2020, 5, e002269. [Google Scholar] [CrossRef] [PubMed]
- Chilet-Rosell, E.; Piay, N.; Hernández-Aguado, I.; Lumbreras, B.; Barrera-Guarderas, F.; Torres-Castillo, A.L.; Caicedo-Montaño, C.; Montalvo-Villacis, G.; Blasco-Blasco, M.; Rivadeneira, M.F.; et al. Contextualizing Evidence for Action on Diabetes in Low-Resource Settings—Project CEAD Part I: A Mixed-Methods Study Protocol. Int. J. Environ. Res. Public Health 2020, 17, 569. [Google Scholar] [CrossRef] [Green Version]
- Ecuador, M. De Salud Pública Encuesta Nacional de Salud y Nutrición: ENSANUT-ECU 2012; INEC: Quito, Ecuador, 2014; ISBN 978-9942-07-659-5. [Google Scholar]
- Ortiz Parada, M.; Baeza Rivera, M.J. Psychometric Properties of a Scale Designed to Measure Perceived Social Support in Chilean Patients with Type 2 Diabetes. Univ. Psychol. 2011, 10, 189–196. [Google Scholar] [CrossRef]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The Multidimensional Scale of Perceived Social Support. J. Pers. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef] [Green Version]
- Meadows, K.A.; Abrams, C.; Sandbaek, A. Adaptation of the Diabetes Health Profile (DHP-1) for Use with Patients with Type 2 Diabetes Mellitus: Psychometric Evaluation and Cross-Cultural Comparison. Diabet. Med. J. Br. Diabet. Assoc. 2000, 17, 572–580. [Google Scholar] [CrossRef] [PubMed]
- West, B.T.; McCabe, S.E. Alternative Approaches to Assessing Nonresponse Bias in Longitudinal Survey Estimates: An Application to Substance-Use Outcomes Among Young Adults in the United States. Am. J. Epidemiol. 2017, 185, 591–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.J.J.; Bartlett, M.; Ryan, L. On the Impact of Nonresponse in Logistic Regression: Application to the 45 and Up Study. BMC Med. Res. Methodol. 2017, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asociación Latinoamericana de Diabetes (ALAD). Guías ALAD Sobre El Diagnóstico, Control y Tratamiento de La Diabetes Mellitus Tipo 2 Con Medicina Basada En Evidencia. Edición 2019. Available online: http://www.revistaalad.com/guias/5600AX191_guias_alad_2019.pdf (accessed on 25 May 2020).
- Larsson, A.; Palm, M.; Hansson, L.-O.; Axelsson, O. Reference Values for Clinical Chemistry Tests during Normal Pregnancy. BJOG Int. J. Obstet. Gynaecol. 2008, 115, 874–881. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Standards of Medical Care in Diabetes—2014. Diabetes Care 2014, 37, S14–S80. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Pregnancy If You Have Diabetes. NIDDK. 2017. Available online: https://www.niddk.nih.gov/health-information/diabetes/diabetes-pregnancy (accessed on 29 May 2020).
- Smith, M.C.; Moran, P.; Ward, M.K.; Davison, J.M. Assessment of Glomerular Filtration Rate during Pregnancy Using the MDRD Formula. BJOG Int. J. Obstet. Gynaecol. 2008, 115, 109–112. [Google Scholar] [CrossRef]
- ADAPTE collaboration. Guideline Adaptation: A Resource Toolkit. Guideline Adaptation Network. 2010. Available online: https://g-i-n.net/document-store/working-groups-documents/adaptation/resources/adapte-resource-toolkit-guideline-adaptation-2-0.pdf (accessed on 27 May 2020).
- Shiffman, R.N.; Dixon, J.; Brandt, C.; Essaihi, A.; Hsiao, A.; Michel, G.; O’Connell, R. The GuideLine Implementability Appraisal (GLIA): Development of an Instrument to Identify Obstacles to Guideline Implementation. BMC Med. Inform. Decis. Mak. 2005, 5, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Annex 8 Contextualizing the Guidelines—Workbook. In WHO Recommendations: Optimizing Health Worker Roles to Improve Access to Key Maternal and Newborn Health Interventions Through Task Shifting; World Health Organization: Geneva, Switzerland, 2012; ISBN 978-92-4-150484-3. [Google Scholar]
- Torfing, J.; Sørensen, E.; Røiseland, A. Transforming the Public Sector Into an Arena for Co-Creation: Barriers, Drivers, Benefits, and Ways Forward. Adm. Soc. 2019, 51, 795–825. [Google Scholar] [CrossRef]
- von Heimburg, D.; Cluley, V. Advancing Complexity-Informed Health Promotion: A Scoping Review to Link Health Promotion and Co-Creation. Health Promot. Int. 2020. [Google Scholar] [CrossRef]
- Snyder, H.; Iverson, M. Advocating for Change: Understanding How to Impact Health Policy; Center for Healthy Communities. 2006. Available online: https://uniteforreprorights.org/wp-content/uploads/2018/01/AFC_Manual_01.pdf. (accessed on 17 May 2020).
- Njeru, J.W.; Patten, C.A.; Hanza, M.M.K.; Brockman, T.A.; Ridgeway, J.L.; Weis, J.A.; Clark, M.M.; Goodson, M.; Osman, A.; Porraz-Capetillo, G.; et al. Stories for Change: Development of a Diabetes Digital Storytelling Intervention for Refugees and Immigrants to Minnesota Using Qualitative Methods. BMC Public Health 2015, 15, 1311. [Google Scholar] [CrossRef] [Green Version]
- Östlund, U.; Kidd, L.; Wengström, Y.; Rowa-Dewar, N. Combining Qualitative and Quantitative Research within Mixed Method Research Designs: A Methodological Review. Int. J. Nurs. Stud. 2011, 48, 369–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tariq, S.; Woodman, J. Using Mixed Methods in Health Research. JRSM Short Rep. 2013, 4, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Unit Nations Deveolpment Programme Coronavirus Disease COVID-19 Pandemic. Available online: https://www.undp.org/content/undp/en/home/coronavirus.html (accessed on 18 May 2020).
- Hallo, A.; Rojas, A.; Hallo, C. Perspective from Ecuador, the Second Country with More Confirmed Cases of Coronavirus Disease 2019 in South America: A Review. Cureus 2020, 12, e7452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sochas, L.; Channon, A.A.; Nam, S. Counting Indirect Crisis-Related Deaths in the Context of a Low-Resilience Health System: The Case of Maternal and Neonatal Health during the Ebola Epidemic in Sierra Leone. Health Policy Plan. 2017, 32, iii32–iii39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberton, T.; Carter, E.D.; Chou, V.B.; Stegmuller, A.R.; Jackson, B.D.; Tam, Y.; Sawadogo-Lewis, T.; Walker, N. Early Estimates of the Indirect Effects of the COVID-19 Pandemic on Maternal and Child Mortality in Low-Income and Middle-Income Countries: A Modelling Study. Lancet Glob. Health 2020, 8, e901–e908. [Google Scholar] [CrossRef]
- Bambra, C.; Riordan, R.; Ford, J.; Matthews, F. The COVID-19 Pandemic and Health Inequalities. J. Epidemiol. Community Health 2020, 74, 964–968. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Type of Data | Time Point | ||||
|---|---|---|---|---|---|
| Category | Specific Information | Baseline | Retrospective (2 years) | Prospective | |
| Year 1 | Year 2 | ||||
| Demographic data | Date and country of birth | X | |||
| Sex | X | ||||
| Ethnicity | X | ||||
| Marital status | X | X | |||
| Socioeconomic data | Education | X | X | ||
| Employment status | X | X | |||
| Household income | X | X | |||
| Data on access to health services | Primary care consultations | X | X | X | |
| Specialist consultations 1 | X | X | X | ||
| Number of biochemical analysis 2 | X | X | X | ||
| Number of blood pressure records | X | X | X | ||
| Number of BMI records | X | X | X | ||
| Clinical data | Date of diabetes diagnosis | X | |||
| Diabetes-related hospitalizations | X | X | X | ||
| Diabetes-related medical assistance | X | X | X | ||
| Biochemical results 2 | X | X | X | ||
| Results of physical measurement | X | X | X | ||
| Medications 3 | X | X | X | ||
| Diabetes complications 4 | X | X | X | ||
| Access to treatment (self-reported) 5 | X | X | |||
| Perceived social support (MSPSS) 5 | X | X | |||
| Health-related quality of life (DHP-18) 5 | X | X | |||
| Primary Outcomes | Secondary Outcomes | ||
|---|---|---|---|
| Outcome | Definition | Outcome | Definition |
| A. Disease control | C. Control of complication risk factors over the 12-month period | ||
| 1. Biochemist | Proportions of patients with biochemically controlled diabetes 3 | 1. Blood pressure control | Proportion of patients with blood pressure < 140/90 [12] |
| 2. Health-related quality of life | Individual score of the Diabetes Health Profile-18 [19]. | 2. Weight control | Proportion of patients with BMI between 18.5 kg/m2 and 25 kg/m2 or 5% weight loss [12] |
| B. Access to health care of diabetes recommended by the CPG [12] over the 12-month period | 3. Lipemic control | Proportion of patients with LDL cholesterol level < 100 mg/dL [12] | |
| 1. Consultations with a GP 1 | Indicators will expressed as number of measurements per patient and will also be categorized according to compliance with CPG recommendations. | 4. Renal health | Proportion of patients with microalbuminuria level <30 mg/day [12,22] |
| 2. Glycemic testing 1 | D. Diabetes-related behaviours/conditions | ||
| 3. Blood pressure records 1 | 1. Perceived social support | Individual score from the Multidimensional Scale of Perceived Social Support. | |
| 4. BMI determination 1 | 2. Access to treatment | Information self-reporting. | |
| 5. Waist circumference record 1 | E. Resources used due to decompensation of the disease and/or complications over the 12-month period | ||
| 6. HbA1C measurement | Indicators will be expressed as proportion of patients with minimum measurements considered acceptable. | 1. Unscheduled consultations 1 | Number of unscheduled medical appointments required due to diabetes or a diabetes complication. |
| 7. Lipid profile determination | |||
| 8. Creatinine determination | 2. Hospitalizations | Indicator will be reported as proportion of persons requiring hospitalization owing to glycemic decompensation and as total number of hospitalizations. | |
| 9. Diabetic foot exam | |||
| 10. Odontological assessment | F. Complications | ||
| 11. Fundus examination 2 | 1. Renal dysfunction 4 | Proportion of patients with renal dysfunction. According to last glomerular filtration rate and serum creatinine values in pregnant women [23]. | |
| 12. Microalbuminuria determination | |||
| 13. Erectile dysfunction assessment | |||
| 14. Cardiovascular screening | 2. Eye disease | Proportion of patients with retinopathy and/or blindness. | |
| 15. Diabetes-related education | Proportion of patients who have received diabetes education (information self-reporting) | 3. Amputations | Proportion of patients with lower limb amputations. |
| 4. Cardiovascular disease | Proportion of patients with 1 or more cardiovascular events 2. | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernal-Soriano, M.C.; Barrera-Guarderas, F.; Alonso-Jaquete, A.; Chilet-Rosell, E.; Benazizi, I.; Caicedo-Montaño, C.; Márquez-Figueroa, M.; Puig-García, M.; Lumbreras, B.; Hernández-Aguado, I.; et al. Contextualizing Evidence for Action on Diabetes in Low-Resource Settings—Project CEAD Part-II, Strengthening the Health System: A Mixed-Methods Study Protocol. Int. J. Environ. Res. Public Health 2021, 18, 3391. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073391
Bernal-Soriano MC, Barrera-Guarderas F, Alonso-Jaquete A, Chilet-Rosell E, Benazizi I, Caicedo-Montaño C, Márquez-Figueroa M, Puig-García M, Lumbreras B, Hernández-Aguado I, et al. Contextualizing Evidence for Action on Diabetes in Low-Resource Settings—Project CEAD Part-II, Strengthening the Health System: A Mixed-Methods Study Protocol. International Journal of Environmental Research and Public Health. 2021; 18(7):3391. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073391
Chicago/Turabian StyleBernal-Soriano, Mari Carmen, Francisco Barrera-Guarderas, Alfonso Alonso-Jaquete, Elisa Chilet-Rosell, Ikram Benazizi, Cintia Caicedo-Montaño, Mónica Márquez-Figueroa, Marta Puig-García, Blanca Lumbreras, Ildefonso Hernández-Aguado, and et al. 2021. "Contextualizing Evidence for Action on Diabetes in Low-Resource Settings—Project CEAD Part-II, Strengthening the Health System: A Mixed-Methods Study Protocol" International Journal of Environmental Research and Public Health 18, no. 7: 3391. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073391