
Instrument Context Relevance Evaluation, Translation, and Psychometric Testing of the Diabetes Eating Problem Survey-Revised (DEPS-R) among People with Type 1 Diabetes in China

Abstract
:1. Introduction
2. Methods
2.1. Study Design
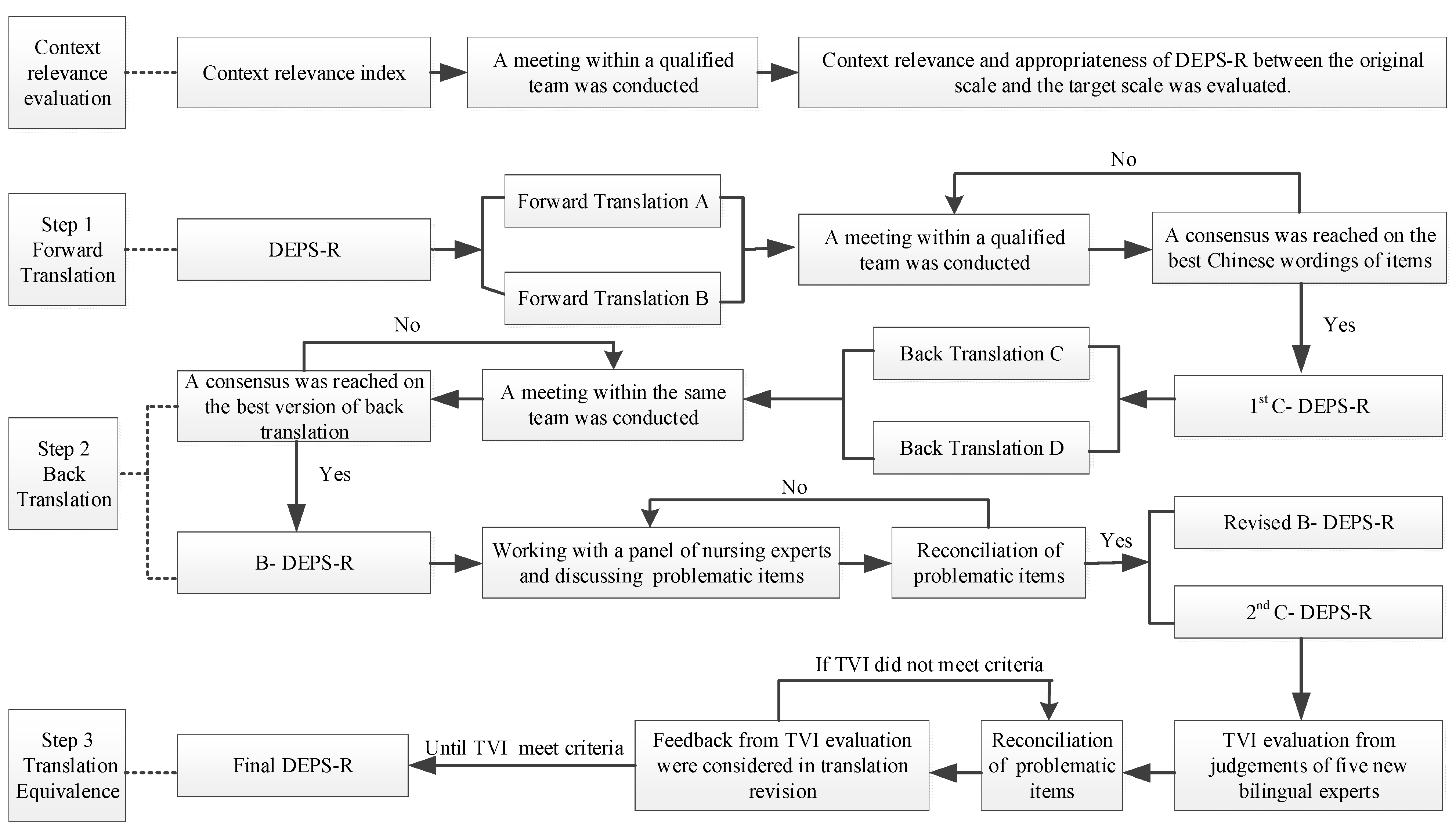
2.2. Phase 1: Context Relevance Evaluation and Instrument Translation
2.3. Testing of the Psychometric Properties
2.4. Setting and Sample
2.5. Recruitment and Data Collection
2.6. Measures
2.7. Reliability and Validity Evaluation
2.8. Data Analyses
3. Results
3.1. Context Relevance and Translation Equivalence Evaluation
3.2. Demographics and T1D-Related Characteristics of Participants
3.3. Test-Retest Reliability
3.4. Internal Consistency Reliability
3.5. Construct Validity
3.5.1. Exploratory Factor Analysis
3.5.2. Inter-Correlations and Distributions of Scores
3.5.3. Convergent Validity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pathak, V.; Pathak, N.M.; O’Neill, C.L.; Guduric-Fuchs, J.; Medina, R.J. Therapies for Type 1 Diabetes: Current Scenario and Future Perspectives. Clin. Med. Insights Endocrinol. Diabetes 2019, 12, 13. [Google Scholar] [CrossRef] [PubMed]
- Tuomilehto, J.; Ogle, G.D.; Lund-Blix, N.A.; Stene, L.C. Update on Worldwide Trends in Occurrence of Childhood Type 1 Diabetes in 2020. Pediatr. Endocrinol. Rev. 2020, 17, 198–209. [Google Scholar] [PubMed]
- Dyson, P.A.; Twenefour, D.; Breen, C.; Duncan, A.; Elvin, E.; Goff, L.; Hill, A.; Kalsi, P.; Marsland, N.; McArdle, P.; et al. Diabetes UK evidence-based nutrition guidelines for the prevention and management of diabetes. Diabet. Med. 2018, 35, 541–547. [Google Scholar] [CrossRef] [PubMed]
- National Clinical Guideline Centre. National Clinical Guideline Centre. National Institute for Health and Care Excellence: Clinical Guidelines. In Type 1 Diabetes in Adults: Diagnosis and Management; National Clinical Guideline Centre: London, UK, 2015. [Google Scholar]
- Mannucci, E.; Rotella, F.; Ricca, V.; Moretti, S.; Placidi, G.F.; Rotella, C.M. Eating disorders in patients with Type 1 diabetes: A meta-analysis. J. Endocrinol. Investig. 2005, 28, 417–419. [Google Scholar] [CrossRef] [PubMed]
- Prodam, F.; Cadario, F.; Bellone, S.; Trovato, L.; Moia, S.; Pozzi, E.; Savastio, S.; Bona, G. Obestatin Levels Are Associated With C-Peptide and Antiinsulin Antibodies at the Onset, Whereas Unacylated and Acylated Ghrelin Levels Are Not Predictive of Long-Term Metabolic Control in Children With Type 1 Diabetes. J. Clin. Endocrinol. Metab. 2014, 99, E599–E607. [Google Scholar] [CrossRef]
- Young, V.; Eiser, C.; Johnson, B.; Brierley, S.; Epton, T.; Elliott, J.; Heller, S. Eating problems in adolescents with Type 1 diabetes: A systematic review with meta-analysis. Diabet. Med. 2013, 30, 189–198. [Google Scholar] [CrossRef]
- Doyle, E.A.; Quinn, S.M.; Ambrosino, J.M.; Weyman, K.; Tamborlane, W.V.; Jastreboff, A.M. Disordered Eating Behaviors in Emerging Adults With Type 1 Diabetes: A Common Problem for Both Men and Women. J. Pediatr. Health Care 2017, 31, 327–333. [Google Scholar] [CrossRef]
- Treasure, J.; Kan, C.; Stephenson, L.; Warren, E.; Smith, E.; Heller, S.; Ismail, K. Developing a theoretical maintenance model for disordered eating in Type 1 diabetes. Diabet. Med. 2015, 32, 1541–1545. [Google Scholar] [CrossRef]
- Hanlan, M.E.; Griffith, J.; Patel, N.; Jaser, S.S. Eating Disorders and Disordered Eating in Type 1 Diabetes: Prevalence, Screening, and Treatment Options. Curr. Diabetes Rep. 2013, 13, 909–916. [Google Scholar] [CrossRef]
- Colton, P.; Olmsted, M.; Daneman, D.; Rydall, A.; Rodin, G. Disturbed Eating Behavior and Eating Disorders in Preteen and Early Teenage Girls with Type 1 Diabetes: A case-controlled study. Diabetes Care 2004, 27, 1654–1659. [Google Scholar] [CrossRef] [Green Version]
- Iafusco, D.; Vanelli, M.; Gugliotta, M.; Iovane, B.; Chiari, G.; Prisco, F. Prevalence of Eating Disorders in Young Patients with Type 1 Diabetes From Two Different Italian Cities. Diabetes Care 2004, 27, 2278. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, S. Eating disorders in females with type 1 diabetes: An update of a meta-analysis. Eur. Eat. Disord. Rev. 2002, 10, 241–254. [Google Scholar] [CrossRef]
- Peveler, R.C.; Bryden, K.S.; Neil, H.A.W.; Fairburn, C.G.; Mayou, R.A.; Dunger, D.B.; Turner, H.M. The Relationship of Disordered Eating Habits and Attitudes to Clinical Outcomes in Young Adult Females With Type 1 Diabetes. Diabetes Care 2005, 28, 84–88. [Google Scholar] [CrossRef] [Green Version]
- Goebel-Fabbri, A.E.; Fikkan, J.; Franko, D.L.; Pearson, K.; Anderson, B.J.; Weinger, K. Insulin Restriction and Associated Morbidity and Mortality in Women with Type 1 Diabetes. Diabetes Care 2008, 31, 415–419. [Google Scholar] [CrossRef] [Green Version]
- Ley, S.H.; Hamdy, O.; Mohan, V.; Hu, F.B. Prevention and management of type 2 diabetes: Dietary components and nutritional strategies. Lancet 2014, 383, 1999–2007. [Google Scholar] [CrossRef] [Green Version]
- Cooper, Z.; Cooper, P.J.; Fairburn, C.G. The Validity of the Eating Disorder Examination and its Subscales. Br. J. Psychiatry 1989, 154, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Chiba, H.; Nagamitsu, S.; Sakurai, R.; Mukai, T.; Shintou, H.; Koyanagi, K.; Yamashita, Y.; Kakuma, T.; Uchimura, N.; Matsuishi, T. Children’s Eating Attitudes Test: Reliability and validation in Japanese adolescents. Eat. Behav. 2016, 23, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Nyman-Carlsson, E.; Engström, I.; Norring, C.; Nevonen, L. Eating Disorder Inventory-3, validation in Swedish patients with eating disorders, psychiatric outpatients and a normal control sample. Nord. J. Psychiatry 2014, 69, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Sancanuto, C.; Jimenez-Rodriguez, D.; Javier Tebar, F.; Jose Hernandez-Morante, J. Translation and validation of the Diabetes Eating Problem Survey to screen eating disorders in patients with type-1 diabetes mellitus. Med. Clin. 2017, 148, 548–554. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Patterson, J.; Mellin, A.; Ackard, D.M.; Utter, J.; Story, M.; Sockalosky, J. Weight Control Practices and Disordered Eating Behaviors Among Adolescent Females and Males With Type 1 Diabetes: Associations with sociodemographics, weight concerns, familial factors, and metabolic outcomes. Diabetes Care 2002, 25, 1289–1296. [Google Scholar] [CrossRef] [Green Version]
- Johnson, C. Initial consultation for patients with bulimia and anorexia nervosa. In Handbook of Psychotherapy for Anorexia Nervosa and Bulimia; Guilford Publications: New York, NY, USA, 1985; pp. 19–51. [Google Scholar]
- Tse, J.; Nansel, T.R.; Haynie, D.L.; Mehta, S.N.; Laffel, L.M. Disordered Eating Behaviors Are Associated with Poorer Diet Quality in Adolescents with Type 1 Diabetes. J. Acad. Nutr. Diet. 2012, 112, 1810–1814. [Google Scholar] [CrossRef] [Green Version]
- Rodin, G.; Craven, J.; Littlefield, C.; Murray, M.; Daneman, D. Eating Disorders and Intentional Insulin Undertreatment in Adolescent Females with Diabetes. J. Psychosom. Res. 1991, 32, 171–176. [Google Scholar] [CrossRef]
- Markowitz, J.T.; Butler, D.A.; Volkening, L.K.; Antisdel, J.E.; Anderson, B.J.; Laffel, L.M.B. Brief Screening Tool for Disordered Eating in Diabetes Internal consistency and external validity in a contemporary sample of pediatric patients with type 1 diabetes. Diabetes Care 2010, 33, 495–500. [Google Scholar] [CrossRef] [Green Version]
- Bantle, J.P.; Wylie-Rosett, J.; Albright, A.L.; Apovian, C.M.; Clark, N.G.; Franz, M.J.; Hoogwerf, B.J.; Lichtenstein, A.H.; Mayer-Davis, E.; Mooradian, A.D.; et al. Nutrition Recommendations and Interventions for Diabetes-2006: A position statement of the American Diabetes Association. Diabetes Care 2008, 31, S61–S78. [Google Scholar]
- Saßmann, H.; Albrecht, C.; Busse-Widmann, P.; Hevelke, L.K.; Kranz, J.; Markowitz, J.T.; Marshall, L.F.; Meurs, S.; de Soye, I.H.; Lange, K. Psychometric properties of the German version of the Diabetes Eating Problem Survey-Revised: Additional benefit of disease-specific screening in adolescents with Type 1 diabetes. Diabet. Med. 2015, 32. [Google Scholar] [CrossRef] [PubMed]
- Wisting, L.; Froisland, D.H.; Skrivarhaug, T.; Dahl-Jorgensen, K.; Ro, O. Psychometric Properties, Norms, and Factor Structure of the Diabetes Eating Problem Survey-Revised in a Large Sample of Children and Adolescents With Type 1 Diabetes. Diabetes Care 2013, 36, 2198–2202. [Google Scholar] [CrossRef] [Green Version]
- Yasemin, A.A.; Suriye, Ö.; Reci, M.; Samim, Ö.; Şükran, D.; Damla, G. Reliability and Validity of the Diabetes Eating Problem Survey in Turkish Children and Adolescents with Type 1 Diabetes Mellitus. J. Clin. Res. Pediatr. Endocrinol. 2017, 9. [Google Scholar] [CrossRef]
- Pinna, F.; Diana, E.; Sanna, L.; Deiana, V.; Manchia, M.; Nicotra, E.; Fiorillo, A.; Albert, U.; Nivoli, A.; Volpe, U.; et al. Assessment of eating disorders with the diabetes eating problems survey—Revised (DEPS-R) in a representative sample of insulin-treated diabetic patients: A validation study in Italy. BMC Psychiatry 2017, 17, 262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryman, B.; MacIsaac, J.; Robinson, T.; Miller, M.R.; Herold Gallego, P. Assessing the clinical utility of the diabetes eating problem survey-revised (DEPS-R) in adolescents with type 1 diabetes. Endocrinol. Diabetes Metab. 2019, 2, e00067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swami, V.; Barron, D. Translation and validation of body image instruments: Challenges, good practice guidelines, and reporting recommendations for test adaptation. Body Image 2019, 31, 204–220. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.T.; Dixon, J. Instrument translation and evaluation of equivalence and psychometric properties: The Chinese Sense of Coherence Scale. J. Nurs. Meas. 2002, 10, 59–76. [Google Scholar] [CrossRef]
- Weng, J.; Zhou, Z.; Guo, L.; Zhu, D.; Ji, L.; Luo, X.; Mu, Y.; Jia, W.; Yang, W.; Grp, T.D.C.S. Incidence of type 1 diabetes in China, 2010–2013: Population based study. BMJ 2018, 360. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Shen, B.; Wu, M.; Chen, C.; Wang, J. Effects of socioeconomic status on risk of ischemic stroke: A case-control study in the Guangzhou population. BMC Public Health 2019, 19, 648. [Google Scholar] [CrossRef]
- Jones, P.S.; Lee, J.W.; Phillips, L.R.; Zhang, X.W.E.; Jaceldo, K.B. An Adaptation of Brislin’s Translation Model for Cross-cultural Research. Nurs. Res. 2001, 50, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Luo, J.; Huang, L.; Yang, J.; Whittemore, R. Adaptation and Feasibility Testing of a Coping Skills Training Program for Chinese Youth with Type 1 Diabetes. Pediatr. Nurs. 2020, 54, e78–e83. [Google Scholar] [CrossRef] [PubMed]
- Julian, L.J. Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (HADS-A). Arthritis Rheum. 2011, 63, S467–S472. [Google Scholar] [CrossRef] [Green Version]
- Cao, Y.; Liu, Z. Factor structure and factorial invariance of the State-Trait Anxiety Inventory for Chinese children and adolescents. Psych J. 2015, 4, 74–87. [Google Scholar] [CrossRef]
- Hu, L.; Huang, X.; You, C.; Li, J.; Hong, K.; Li, P.; Wu, Y.; Wu, Q.; Wang, Z.; Gao, R.; et al. Prevalence of overweight, obesity, abdominal obesity and obesity-related risk factors in southern China. PLoS ONE 2017, 12, e0183934. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.L.; Esquivel, J.H.; Guo, J.; Chesla, C.A.; Tang, S. Risk factors for obesity in preschool-aged children in China. Int. Nurs. Rev. 2017, 65, 217–224. [Google Scholar] [CrossRef]
- Battelino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes Care 2019, 42, 1593–1603. [Google Scholar] [CrossRef] [Green Version]
- Lindell, R.; Ding, L. Establishing reliability and validity: An ongoing process. In Proceedings of the 2012 Physics Education Research Conference, Philadelphia, PA, USA, 1–2 August 2012; pp. 27–29. [Google Scholar]
- Wisting, L.; Wonderlich, J.; Skrivarhaug, T.; Dahl-Jorgensen, K.; Ro, O. Psychometric properties and factor structure of the diabetes eating problem survey - revised (DEPS-R) among adult males and females with type 1 diabetes. J. Eat. Disord. 2019, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- McHorney, C.A.; Tarlov, A.R. Individual-patient monitoring in clinical practice: Are available health status surveys adequate? Qual. Life Res. 1995, 4, 293–307. [Google Scholar] [CrossRef] [PubMed]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.A.; de Vet, H.C.W. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonneville, K.R.; Thurston, I.B.; Milliren, C.E.; Gooding, H.C.; Richmond, T.K. Weight misperception among young adults with overweight/obesity associated with disordered eating behaviors. Int. J. Eat. Disord. 2016, 49, 937–946. [Google Scholar] [CrossRef] [Green Version]
- Cherubini, V.; Skrami, E.; Iannilli, A.; Cesaretti, A.; Paparusso, A.M.; Alessandrelli, M.C.; Carle, F.; Ferrito, L.; Gesuita, R. Disordered eating behaviors in adolescents with type 1 diabetes: A cross-sectional population-based study in Italy. Int. J. Eat. Disord. 2018, 51, 890–898. [Google Scholar] [CrossRef] [PubMed]
- Colman, M.H.E.; Quick, V.M.; Lipsky, L.M.; Dempster, K.W.; Liu, A.; Laffel, L.M.B.; Mehta, S.N.; Nansel, T.R. Disordered Eating Behaviors Are Not Increased by an Intervention to Improve Diet Quality but Are Associated with Poorer Glycemic Control Among Youth With Type 1 Diabetes. Diabetes Care 2018, 41, 869–875. [Google Scholar] [CrossRef] [Green Version]
- Wisting, L.; Skrivarhaug, T.; Dahl-Jorgensen, K.; Ro, O. Prevalence of disturbed eating behavior and associated symptoms of anxiety and depression among adult males and females with type 1 diabetes. J. Eat. Disord 2018, 6, 28. [Google Scholar] [CrossRef] [Green Version]
- Bächle, C.; Lange, K.; Stahl-Pehe, A.; Castillo, K.; Scheuing, N.; Holl, R.W.; Giani, G.; Rosenbauer, J. Symptoms of Eating Disorders and Depression in Emerging Adults with Early-Onset, Long-Duration Type 1 Diabetes and Their Association with Metabolic Control. PLoS ONE 2015, 10, e0131027. [Google Scholar] [CrossRef] [Green Version]
- Cecilia-Costa, R.; Volkening, L.K.; Laffel, L.M. Factors associated with disordered eating behaviours in adolescents with Type 1 diabetes. Diabet. Med. 2018, 36, 1020–1027. [Google Scholar] [CrossRef]


{kind=link}
| Youths (n = 89) | Adults (n = 61) | |||
|---|---|---|---|---|
| Mean ± SD | N (%) | Mean ± SD | N (%) | |
| Age (years) | 12.97 ± 2.48 | 32.98 ± 14.47 | ||
| children (8–12) | 38 (42.7%) | |||
| adolescents (13–17) | 51 (57.3%) | |||
| Sex | ||||
| male | 33 (37.1%) | 29 (47.5%) | ||
| female | 56 (62.9%) | 32 (52.5%) | ||
| Diabetes duration (years) | 4.83 ± 3.11 | 8.30 ± 4.97 | ||
| <5 | 53 (59.6%) | 15 (24.6%) | ||
| ≥5 | 36 (40.4%) | 46 (75.4%) | ||
| Insulin pump therapy | ||||
| yes | 23 (25.8%) | 9 (14.8%) | ||
| no | 66 (74.2%) | 52 (85.2%) | ||
| HbA1c (%) | 8.54 ± 2.32 | 7.55 ± 1.48 | ||
| normal | 35 (39.3%) | 25 (41.0%) | ||
| abnormal | 54 (60.7%) | 36 (59.0%) | ||
| BMI (kg/m2) | 18.83 ± 2.69 | 21.44 ± 2.16 | ||
| underweight or normal | 83 (93.3%) | 53 (86.9%) | ||
| overweight or obese | 6 (6.7%) | 8 (13.1%) | ||
| STAI | ||||
| STAI-S | 40.51 ± 11.71 | 42.59 ± 9.85 | ||
| STAI-T | 40.15 ± 10.12 | 42.49 ± 11.07 | ||
| C-DEPS-R | 20.96 ± 9.73 | 20.65 ± 11.07 | ||
| ≤20 | 54 (60.7%) | 33 (54.1%) | ||
| >20 | 35 (39.3%) | 28 (45.9%) | ||
| Items | Youths | Adults | |||
|---|---|---|---|---|---|
| Items Scores Mean (SD) | r | Items Scores Mean (SD) | r | ||
| 1 | Losing weight is an important goal to me. | 1.80 (1.69) | 0.411 ** | 1.67 (1.61) | 0.632 ** |
| 2 | I skip meals and/or snacks. | 0.83 (0.95) | 0.412 ** | 0.80 (0.98) | 0.465 ** |
| 3 | Other people have told me that my eating is out of control. | 1.95 (1.26) | 0.591 ** | 1.95 (1.19) | 0.665 ** |
| 4 | When I overeat, I don’t take enough insulin to cover the food. | 1.44 (1.27) | 0.406 ** | 1.54 (1.23) | 0.673 ** |
| 5 | I eat more when I am alone than when I am with others. | 1.28 (1.28) | 0.389 ** | 1.15 (1.16) | 0.452 ** |
| 6 | I feel that it’s difficult to lose weight and control my diabetes at the same time. | 1.39 (1.38) | 0.655 ** | 1.57 (1.44) | 0.625 ** |
| 7 | I avoid checking my blood sugar when I feel like it is out of range. | 0.84 (1.22) | 0.613 ** | 0.74 (1.12) | 0.633 ** |
| 8 | I make myself vomit. | 0.22 (0.64) | 0.329 ** | 0.21 (0.69) | 0.572 ** |
| 9 | I try to keep my blood sugar high so that I will lose weight. | 0.22 (0.66) | 0.356 ** | 0.33 (0.85) | 0.465 ** |
| 10 | I try to eat to the point of spilling ketones in my urine. | 1.22 (1.47) | 0.400 ** | 1.16 (1.50) | 0.413 ** |
| 11 | I feel fat when I take all of my insulin. | 1.58 (1.65) | 0.605 ** | 1.48 (1.61) | 0.622 ** |
| 12 | Other people tell me to take better care of my diabetes. | 3.19 (1.30) | 0.402 ** | 3.07 (1.34) | 0.507 ** |
| 13 | After I overeat, I skip my next insulin dose. | 0.27 (0.69) | 0.480 ** | 0.25 (0.68) | 0.587 ** |
| 14 | I feel that my eating is out of control. | 1.96 (1.34) | 0.637 ** | 2.07 (1.20) | 0.620 ** |
| 15 | I alternate between eating very little and eating huge amounts. | 1.90 (1.38) | 0.608 ** | 1.92 (1.46) | 0.705 ** |
| 16 | I would rather be thin than to have good control of my diabetes. | 0.74 (1.23) | 0.505 ** | 0.75 (1.35) | 0.424 ** |
| Total score Mean (SD) | 20.96 ± 9.73 | 20.65 ± 11.07 | |||
| Items | Score Mean (SD) | Option N (%) | |||||
|---|---|---|---|---|---|---|---|
| Never | Rarely | Sometimes | Often | Usually | Always | ||
| 1 | 1.80 (1.69) | 26 (29.2%) | 20 (22.5%) | 12 (13.5%) | 11 (12.3%) | 9 (10.1%) | 11 (12.4%) |
| 2 | 0.83 (0.95) | 38 (42.7%) | 34 (38.2%) | 12 (13.5%) | 3 (3.4%) | 2 (2.2%) | 0 (0.0%) |
| 3 | 1.95 (1.26) | 11 (12.4%) | 28 (31.4%) | 20 (22.5%) | 18 (20.2%) | 9 (10.1%) | 3 (3.4%) |
| 4 | 1.44 (1.27) | 25 (28.0%) | 32 (35.9%) | 15 (16.9%) | 11 (12.4%) | 3 (3.4%) | 3 (3.4%) |
| 5 | 1.28 (1.28) | 27 (30.3%) | 31 (34.9%) | 14 (15.7%) | 7 (7.9%) | 8 (9.0%) | 2 (2.2%) |
| 6 | 1.39 (1.38) | 35 (39.3%) | 22 (24.7%) | 14 (15.7%) | 11 (12.4%) | 6 (6.7%) | 1 (1.1%) |
| 7 | 0.84 (1.22) | 46 (51.7%) | 26 (29.2%) | 2 (2.2%) | 10 (11.3%) | 3 (3.4%) | 2 (2.2%) |
| 8 | 0.22 (0.64) | 76 (85.4%) | 8 (9.0%) | 3 (3.4%) | 2 (2.2%) | 0 (0.0%) | 0 (0.0%) |
| 9 | 0.22 (0.66) | 80 (90.0%) | 6 (6.7%) | 2 (2.2%) | 1 (1.1%) | 0 (0.0%) | 0 (0.0%) |
| 10 | 1.22 (1.47) | 41 (46.0%) | 14 (15.7%) | 15 (16.9%) | 12 (13.5%) | 3 (3.4%) | 4 (4.5%) |
| 11 | 1.58 (1.65) | 34 (38.2%) | 14 (15.7%) | 12 (13.5%) | 13 (14.6%) | 9 (10.1%) | 7 (7.9%) |
| 12 | 3.19 (1.30) | 1 (1.1%) | 7 (7.9%) | 18 (20.2%) | 20 (22.5%) | 26 (29.2%) | 17 (19.1%) |
| 13 | 0.27 (0.69) | 72 (81.0%) | 13(14.6%) | 1 (1.1%) | 2 (2.2%) | 1 (1.1%) | 0 (0.0%) |
| 14 | 1.96 (1.34) | 16 (14.7%) | 37 (24.7%) | 44 (29.4%) | 24 (16%) | 18 (12%) | 5 (3.3%) |
| 15 | 1.90 (1.38) | 14 (15.7%) | 25 (28.1%) | 19 (21.3%) | 20 (22.5%) | 9 (10.1%) | 2 (2.2%) |
| 16 | 0.74 (1.23) | 54 (60.7%) | 17 (19.1%) | 12 (13.5%) | 3(3.4%) | 0 (0.0%) | 3 (3.4%) |
| Items | Score Mean (SD) | Option N (%) | |||||
|---|---|---|---|---|---|---|---|
| Never | Rarely | Sometimes | Often | Usually | Always | ||
| 1 | 1.67 (1.61) | 22 (36.1%) | 9 (14.7%) | 10 (16.4%) | 10 (16.4%) | 7 (11.5%) | 3 (4.9%) |
| 2 | 0.80 (0.98) | 31 (50.8%) | 16 (26.2%) | 9 (14.8%) | 5 (8.2%) | 0 (0.0%) | 0 (0.0%) |
| 3 | 1.95 (1.19) | 6 (9.8%) | 20 (32.8%) | 12 (19.7%) | 17 (27.9%) | 6 (9.8%) | 0 (0.0%) |
| 4 | 1.54 (1.23) | 14 (23.0%) | 17 (27.9%) | 19 (31.1%) | 6 (9.8%) | 4 (6.6%) | 1 (1.6%) |
| 5 | 1.15 (1.16) | 23 (37.7%) | 17 (27.9%) | 13 (21.3%) | 5 (8.2%) | 3 (4.9%) | 0 (0.0%) |
| 6 | 1.57 (1.44) | 18 (29.5%) | 16 (26.2%) | 10 (16.4%) | 10 (16.4%) | 5 (8.2%) | 2 (3.3%) |
| 7 | 0.74 (1.12) | 35 (57.4%) | 16 (26.2%) | 4 (6.6%) | 4 (6.6%) | 1 (1.6%) | 1 (1.6%) |
| 8 | 0.21 (0.69) | 53 (87.0%) | 6 (9.8%) | 0 (0.0%) | 1 (1.6%) | 1 (1.6%) | 0 (0.0%) |
| 9 | 0.33 (0.85) | 50 (82.0%) | 6 (9.8%) | 3 (4.9%) | 0 (0.0%) | 2 (3.3%) | 0 (0.0%) |
| 10 | 1.16 (1.50) | 30 (49.1%) | 14 (23.0%) | 4 (6.6%) | 3 (4.9%) | 10 (16.4%) | 0 (0.0%) |
| 11 | 1.48 (1.61) | 26 (42.6%) | 9 (14.8%) | 9 (14.8%) | 8 (13.1%) | 6 (9.8%) | 3 (4.9%) |
| 12 | 3.07 (1.34) | 2 (3.3%) | 7 (11.5%) | 11 (18.0%) | 14 (23.0%) | 19 (31.1%) | 8 (13.1%) |
| 13 | 0.25 (0.68) | 51 (83.6%) | 7 (11.5%) | 2 (3.3%) | 0 (0.0%) | 1 (1.6%) | 0 (0.0%) |
| 14 | 2.07 (1.20) | 6 (9.8%) | 14 (23.0%) | 20 (32.8%) | 13 (21.3%) | 7 (11.5%) | 1 (1.6%) |
| 15 | 1.92 (1.46) | 12 (19.6%) | 14 (23.0%) | 15 (24.6%) | 11 (18.0%) | 5 (8.2%) | 4 (6.6%) |
| 16 | 0.75 (1.35) | 42 (68.8%) | 6 (9.8%) | 5 (8.2%) | 4 (6.6%) | 2 (3.3%) | 2 (3.3%) |
| Measures | Scores (Mean ± SD) | C-DEPS-R |
|---|---|---|
| STAI-S | ||
| Youths | 40.51 ± 11.71 | r = 0.310; p = 0.003 |
| Adults | 42.59 ± 9.85 | r = 0.373; p = 0.003 |
| STAI-T | ||
| Youths | 41.15 ± 10.12 | r = 0.313; p = 0.003 |
| Adults | 42.49 ± 11.07 | r = 0.317; p = 0.013 |
| BMI | ||
| Youths | 18.83 ± 2.69 | r = 0.255; p = 0.016 |
| Adults | 21.44 ± 2.16 | r = 0.083; p = 0.523 |
| HbA1c | ||
| Youths | 8.54 ± 2.32 | r = 0.459; p = 0.000 |
| Adults | 7.55 ± 1.48 | r = 0.215; p = 0.097 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lv, W.; Zhong, Q.; Guo, J.; Luo, J.; Dixon, J.; Whittemore, R. Instrument Context Relevance Evaluation, Translation, and Psychometric Testing of the Diabetes Eating Problem Survey-Revised (DEPS-R) among People with Type 1 Diabetes in China. Int. J. Environ. Res. Public Health 2021, 18, 3450. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073450
Lv W, Zhong Q, Guo J, Luo J, Dixon J, Whittemore R. Instrument Context Relevance Evaluation, Translation, and Psychometric Testing of the Diabetes Eating Problem Survey-Revised (DEPS-R) among People with Type 1 Diabetes in China. International Journal of Environmental Research and Public Health. 2021; 18(7):3450. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073450
Chicago/Turabian StyleLv, Wencong, Qinyi Zhong, Jia Guo, Jiaxin Luo, Jane Dixon, and Robin Whittemore. 2021. "Instrument Context Relevance Evaluation, Translation, and Psychometric Testing of the Diabetes Eating Problem Survey-Revised (DEPS-R) among People with Type 1 Diabetes in China" International Journal of Environmental Research and Public Health 18, no. 7: 3450. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073450