
What Role Does Body Image in Relationship between Level of Health Literacy and Symptoms of Eating Disorders in Adolescents?


Abstract
:1. Introduction
2. Materials and Methods
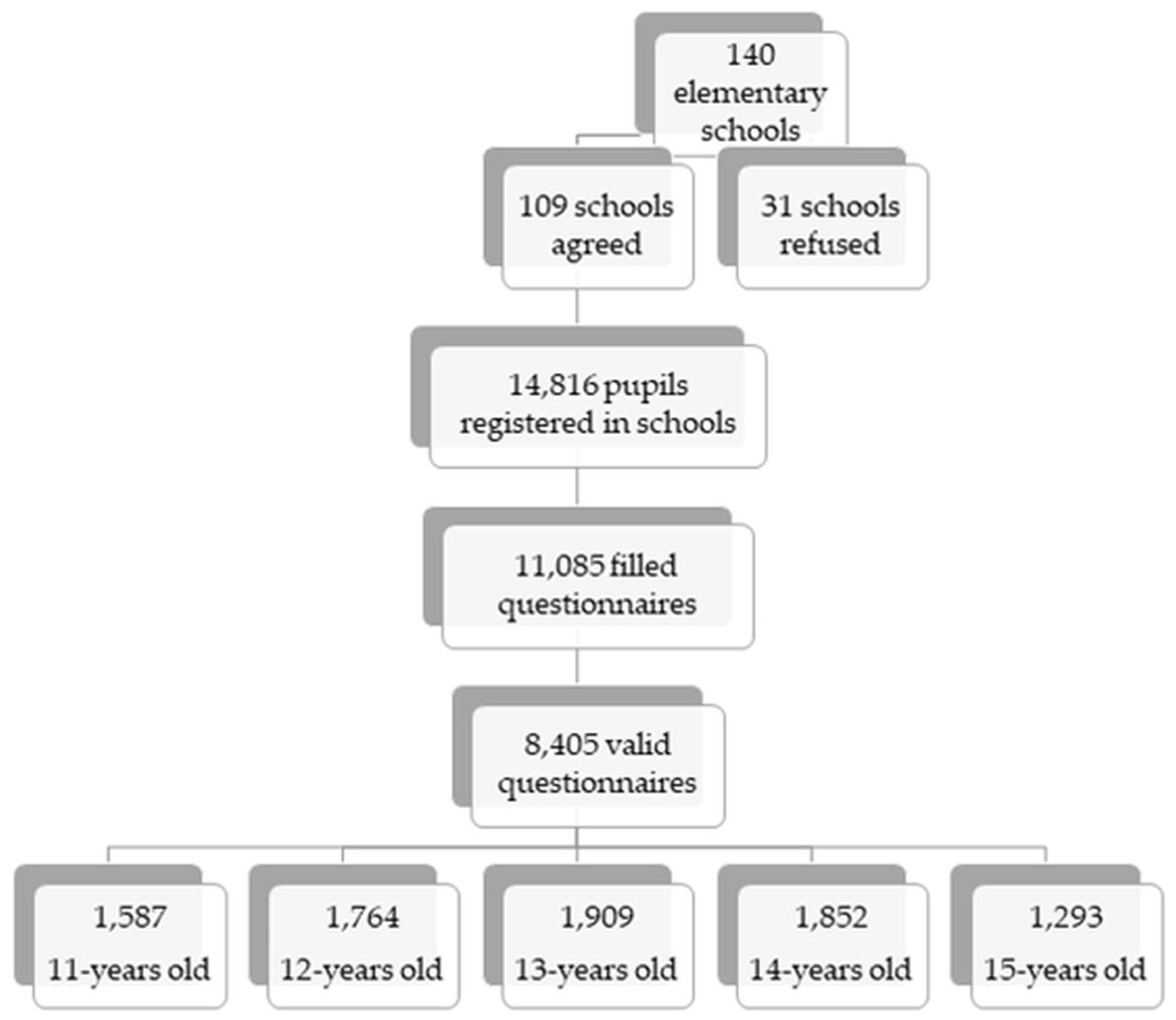
2.1. Sample and Procedure
2.2. Measures
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation (WHO). Report of the commission on ending childhood obesity. Implement. Plan Exec. Summ. 2017, 19. [Google Scholar]
- Chin, S.N.M.; Laverty, A.A.; Filippidis, F.T. Trends and correlates of unhealthy dieting behaviours among adolescents in the United States, 1999–2013. BMC Public Health 2018, 18, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Neumark-Sztainer, D.; Wall, M.; Larson, N.I.; Eisenberg, M.E.; Loth, K. Dieting and disordered eating behaviors from adolescence to young adulthood: Findings from a 10-year longitudinal study. J. Am. Diet. Assoc. 2011, 111, 1004–1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilibarda, B.; Gudelj Rakic, J.; Mitov Scekic, S.; Krstev, S. Smoking as a weight control strategy of Serbian adolescents. Int. J. Public Health 2020, 65, 1319–1329. [Google Scholar] [CrossRef] [PubMed]
- Ojala, K.; Tynjälä, J.; Välimaa, R.; Villberg, J.; Kannas, L. Overweight adolescents’ self-perceived weight and weight control behaviour: HBSC study in Finland 1994–2010. J. Obes. 2012, 2012. [Google Scholar] [CrossRef] [Green Version]
- Gaspar, T.; Santos, T.; de Matos, M.G. Relationship between subjective wellbeing and weight perception in children and adolescents: Gender and age differences. Child Indic. Res. 2017, 10, 811–824. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Wall, M.; Story, M.; Standish, A.R. Dieting and unhealthy weight control behaviors during adolescence: Associations with 10-year changes in body mass index. J. Adolesc. Health 2012, 50, 80–86. [Google Scholar] [CrossRef] [Green Version]
- Dzielska, A.; Kelly, C.; Ojala, K.; Finne, E.; Spinelli, A.; Furstova, J.; Fismen, A.S.; Ercan, O.; Tesler, R.; Melkumova, M.; et al. Weight reduction behaviors among european adolescents—Changes from 2001/2002 to 2017/2018. J. Adolesc. Health 2020, 66, S70–S80. [Google Scholar] [CrossRef]
- Herpertz-Dahlmann, B. Adolescent eating disorders: Update on definitions, symptomatology, epidemiology, and comorbidity. Child Adolesc. Psychiatr. Clin. N. Am. 2015, 24, 177–196. [Google Scholar] [CrossRef] [PubMed]
- Association, A.P. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Philadelphia, PA, USA, 2013. [Google Scholar]
- Mairs, R.; Nicholls, D. Assessment and treatment of eating disorders in children and adolescents. Arch. Dis. Child. 2016, 101, 1168–1175. [Google Scholar] [CrossRef]
- Micali, N.; Solmi, F.; Horton, N.J.; Crosby, R.D.; Eddy, K.T.; Calzo, J.P.; Sonneville, K.R.; Swanson, S.A.; Field, A.E. Adolescent eating disorders predict psychiatric, high-risk behaviors and weight outcomes in young adulthood. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 652–659.e1. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.R.; Zuromski, K.L.; Dodd, D.R. Eating disorders and suicidality: What we know, what we don’t know, and suggestions for future research. Curr. Opin. Psychol. 2018, 22, 63–67. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Promoting health in the SDGs. In Proceedings of the 9th Global Conference, Shanghai, China, 21–24 November 2016; pp. 21–24. [Google Scholar]
- World Health Organization Regional Office for Europe. Draft WHO European Roadmap for Implementation of Health Literacy Initiatives Through the Life Course; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2019; Volume 5, pp. 16–19. [Google Scholar]
- Liu, C.; Wang, D.; Liu, C.; Jiang, J.; Wang, X.; Chen, H.; Ju, X.; Zhang, X. What is the meaning of health literacy? A systematic review and qualitative synthesis. Fam. Med. Community Health 2020, 8, 1–8. [Google Scholar] [CrossRef]
- WHO. The World Health Organization (WHO) Health Promotion Glossary; WHO: Geneve, Switzerland, 1998; p. 10. [Google Scholar]
- Bröder, J.; Okan, O.; Bauer, U.; Bruland, D.; Schlupp, S.; Bollweg, T.M.; Saboga-Nunes, L.; Bond, E.; Sørensen, K.; Bitzer, E.M.; et al. Health literacy in childhood and youth: A systematic review of definitions and models. BMC Public Health 2017, 17, 1–25. [Google Scholar] [CrossRef]
- Fleary, S.A.; Joseph, P.; Pappagianopoulos, J.E. Adolescent health literacy and health behaviors: A systematic review. J. Adolesc. 2018, 62, 116–127. [Google Scholar] [CrossRef]
- Okan, O.; Lopes, E.; Bollweg, T.M.; Bröder, J.; Messer, M.; Bruland, D.; Bond, E.; Carvalho, G.S.; Sørensen, K.; Saboga-Nunes, L.; et al. Generic health literacy measurement instruments for children and adolescents: A systematic review of the literature. BMC Public Health 2018, 18, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Paakkari, L.T.; Torppa, M.P.; Paakkari, O.P.; Välimaa, R.S.; Ojala, K.S.A.; Tynjälä, J.A. Does health literacy explain the link between structural stratifiers and adolescent health? Eur. J. Public Health 2019, 29, 919–924. [Google Scholar] [CrossRef]
- Levin-Zamir, D.; Lemish, D.; Gofin, R. Media Health Literacy (MHL): Development and measurement of the concept among adolescents. Health Educ. Res. 2011, 26, 323–335. [Google Scholar] [CrossRef]
- Chang, L.C. Health literacy, self-reported status and health promoting behaviours for adolescents in Taiwan. J. Clin. Nurs. 2011, 20, 190–196. [Google Scholar] [CrossRef]
- Needham, H.E.; Wiemann, C.M.; Tortolero, S.R.; Chacko, M.R. Relationship between health literacy, reading comprehension, and risk for sexually transmitted infections in young women. J. Adolesc. Health 2010, 46, 506–508. [Google Scholar] [CrossRef]
- Page, R.M.; Huong, N.T.; Chi, H.K.; Tien, T.Q. Smoking media literacy in vietnamese adolescents. J. Sch. Health 2010, 81, 34–41. [Google Scholar] [CrossRef]
- Chisolm, D.J.; Manganello, J.A.; Kelleher, K.J.; Marshal, M.P. Health literacy, alcohol expectancies, and alcohol use behaviors in teens. Patient Educ. Couns. 2014, 97, 291–296. [Google Scholar] [CrossRef] [Green Version]
- Paakkari, L.; Torppa, M.; Mazur, J.; Boberova, Z.; Sudeck, G.; Kalman, M.; Paakkari, O. A comparative study on adolescents’ health literacy in europe: Findings from the HBSC study. Int. J. Environ. Res. Public Health 2020, 17. [Google Scholar] [CrossRef]
- Michou, M.; Panagiotakos, D.B.; Costarelli, V. Low health literacy and excess body weight: A systematic review. Cent. Eur. J. Public Health 2018, 26, 234–241. [Google Scholar] [CrossRef]
- Shih, S.F.; Liu, C.H.; Liao, L.L.; Osborne, R.H. Health literacy and the determinants of obesity: A population-based survey of sixth grade school children in Taiwan. BMC Public Health 2016, 16, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Lam, L.T.; Yang, L. Is low health literacy associated with overweight and obesity in adolescents: An epidemiology study in a 12–16 years old population, Nanning, China, 2012. Arch. Public Health 2014, 72, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Ozturk Haney, M. Health literacy and predictors of body weight in Turkish children. J. Pediatr. Nurs. 2020, 55, e257–e262. [Google Scholar] [CrossRef]
- Farhat, T.; Iannotti, R.J.; Caccavale, L.J. Adolescent overweight, obesity and chronic disease-related health practices: Mediation by body image. Obes. Facts 2014, 7, 1–14. [Google Scholar] [CrossRef]
- Zarychta, K.; Mullan, B.; Luszczynska, A. Am I overweight? A longitudinal study on parental and peers weight-related perceptions on dietary behaviors and weight status among adolescents. Front. Psychol. 2016, 7, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Grogan, S. Promoting positive body image in males and females: Contemporary issues and future directions. Sex Roles 2010, 63, 757–765. [Google Scholar] [CrossRef]
- Paakkari, L.; Paakkari, O. Health literacy as a learning outcome in schools. Health Educ. 2012, 112, 133–152. [Google Scholar] [CrossRef] [Green Version]
- Zuair, A.A.; Sopory, P. Effects of media health literacy school-based interventions on adolescents’ body image concerns, eating concerns, and thin-internalization attitudes: A systematic review and meta-analysis. Health Commun. 2020, 1–9. [Google Scholar] [CrossRef]
- Hautala, L.; Junnila, J.; Alin, J.; Grönroos, M.; Maunula, A.M.; Karukivi, M.; Liuksila, P.R.; Räihä, H.; Välimäki, M.; Saarijärvi, S. Uncovering hidden eating disorders using the SCOFF questionnaire: Cross-sectional survey of adolescents and comparison with nurse assessments. Int. J. Nurs. Stud. 2009, 46, 1439–1447. [Google Scholar] [CrossRef]
- Lichtenstein, M.B.; Hemmingsen, S.D.; Støving, R.K. Identification of eating disorder symptoms in Danish adolescents with the SCOFF questionnaire. Nord. J. Psychiatry 2017, 71, 340–347. [Google Scholar] [CrossRef]
- Garcia-Campayo, J.; Sanz-Carrillo, C.; Ibañez, J.A.; Lou, S.; Solano, V.; Alda, M. Validation of the Spanish version of the SCOFF questionnaire for the screening of eating disorders in primary care. J. Psychosom. Res. 2005, 59, 51–55. [Google Scholar] [CrossRef]
- Luck, A.J.; Morgan, J.F.; Reid, F.; Brien, A.O.; Brunton, J.; Price, C.; Perry, L.; Lacey, J.H.; Bmj, S.; Medical, B.; et al. The SCOFF questionnaire and clinical interview for eating disorders in general practice: Comparative study psychia. JSTOR 2002, 325, 19–21. Available online: https://0-www-jstor-org.brum.beds.ac.uk/stable/25452509 (accessed on 1 March 2021).
- Paakkari, O.; Torppa, M.; Boberova, Z.; Välimaa, R.; Maier, G.; Mazur, J.; Kannas, L.; Paakkari, L. The cross-national measurement invariance of the health literacy for school-aged children (HLSAC) instrument. Eur. J. Public Health 2019, 29, 432–436. [Google Scholar] [CrossRef]
- Inchley, J.; Currie, D.; Cosma, A.; Samdal, O. Health Behaviour in School-Aged Children (HBSC) Study Protocol: Background, Methodology and Mandatory Items for the 2017/18 Survey 2018; St Andrews: Scotland, UK, 2018. [Google Scholar]
- Adelantado-Renau, M.; Beltran-Valls, M.R.; Toledo-Bonifás, M.; Bou-Sospedra, C.; Pastor, M.C.; Moliner-Urdiales, D. The risk of eating disorders and academic performance in adolescents: DADOS study. Nutr. Hosp. 2018, 35, 1201–1207. [Google Scholar] [CrossRef]
- Lena, S.M.; Fiocco, A.J.; Leyenaar, J.A.K. The role of cognitive deficits in the development of eating disorders. Neuropsychol. Rev. 2004, 14, 99–113. [Google Scholar] [CrossRef]
- Paakkari, O.; Torppa, M.; Villberg, J.; Kannas, L.; Paakkari, L. Subjective health literacy among school-aged children. Health Educ. 2018, 118, 182–195. [Google Scholar] [CrossRef] [Green Version]
- Jorm, A.F.; Korten, A.E.; Jacomb, P.A.; Christensen, H.; Rodgers, B.; Pollitt, P. “Mental health literacy”: A survey of the public’s ability to recognise mental disorders and their beliefs about the effectiveness of treatment. Med. J. Aust. 1997, 166, 182–186. [Google Scholar] [CrossRef]
- Skre, I.; Friborg, O.; Breivik, C.; Johnsen, L.I.; Arnesen, Y.; Wang, C.E.A. A school intervention for mental health literacy in adolescents: Effects of a non-randomized cluster controlled trial. BMC Public Health 2013, 13. [Google Scholar] [CrossRef] [Green Version]
- Bullivant, B.; Rhydderch, S.; Griffiths, S.; Mitchison, D.; Mond, J.M. Eating disorders “mental health literacy”: A scoping review. J. Ment. Health 2020, 29, 336–349. [Google Scholar] [CrossRef]
- Paakkari, L. Three approaches to school health education as a means to higher levels of health literacy. In Schools for Health and Sustainability; Simovska, V., McNamara, P.M., Eds.; Springer: Dordrecht, The Netherlands, 2015; pp. 275–289. [Google Scholar]
- Coutinho, S.A.; Neuman, G. A model of metacognition, achievement goal orientation, learning style and self-efficacy. Learn. Environ. Res. 2008, 11, 131–151. [Google Scholar] [CrossRef]
- Ouyang, Y.; Wang, K.; Zhang, T.; Peng, L.; Song, G.; Luo, J. The influence of sports participation on body image, self-efficacy, and self-esteem in college students. Front. Psychol. 2020, 10, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Chung, A.E.; Perrin, E.M.; Skinner, A.C. Accuracy of child and adolescent weight perceptions and their relationships to dieting and exercise behaviors: A NHANES study. Acad. Pediatr. 2013, 13, 371–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarrar, L.; Vilalta, M.; Schneider, N.; Correll, C.U. Body mass index and self-reported body image in German adolescents. J. Eat. Disord. 2020, 8, 1–10. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | n (in %) |
|---|---|
| Gender | |
| Boys | 2613 (51.7) |
| Girls | 2441 (48.3) |
| Age | |
| 13 years | 1909 (37.8) |
| 14 years | 1852 (36.6) |
| 15 years | 1293 (25.6) |
| Health Literacy | |
| Low | 614 (13.9) |
| Middle | 2972 (67.0) |
| High | 847 (19.1) |
| Body Image | |
| Perceived fat | 1316 (26.3) |
| Not percceived fat | 3693 (73.7) |
| Eating Disorders | |
| ≤1 symptom | 3250 (68.7) |
| 2+ symptoms | 1481 (31.3) |
| Studied Variables | Model 1 | Model 2 |
|---|---|---|
| OR (95%CI) | OR (95%CI) | |
| Health Literacy | ||
| High | Ref. | Ref. |
| Medium | 1.37 (1.15–1.65) ** | 1.26 (1.05–1.52) * |
| Low | 2.25 (1.78–2.84) *** | 1.92 (1.51–2.45) *** |
| Body Image | ||
| Not perceived fat | Ref. | Ref. |
| Perceived fat | 3.49 (3.04–4.00) *** | 3.46 (2.99–4.00) *** |
| Change of OR for body image | ||
| Low level of health literacy | - | 26.4% |
| Medium level of health literacy | - | 29.7% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boberová, Z.; Husárová, D. What Role Does Body Image in Relationship between Level of Health Literacy and Symptoms of Eating Disorders in Adolescents? Int. J. Environ. Res. Public Health 2021, 18, 3482. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073482
Boberová Z, Husárová D. What Role Does Body Image in Relationship between Level of Health Literacy and Symptoms of Eating Disorders in Adolescents? International Journal of Environmental Research and Public Health. 2021; 18(7):3482. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073482
Chicago/Turabian StyleBoberová, Zuzana, and Daniela Husárová. 2021. "What Role Does Body Image in Relationship between Level of Health Literacy and Symptoms of Eating Disorders in Adolescents?" International Journal of Environmental Research and Public Health 18, no. 7: 3482. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073482