
Evaluation of the Effectiveness of an Interdisciplinary Preventive Oral Hygiene Program for Children with Congenital Heart Disease

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Setting
2.2. Dental and Gingival Examination
2.3. Preventive Oral Hygiene Program (POHP)
2.4. Statistical Analysis
3. Results
3.1. Caries Experience
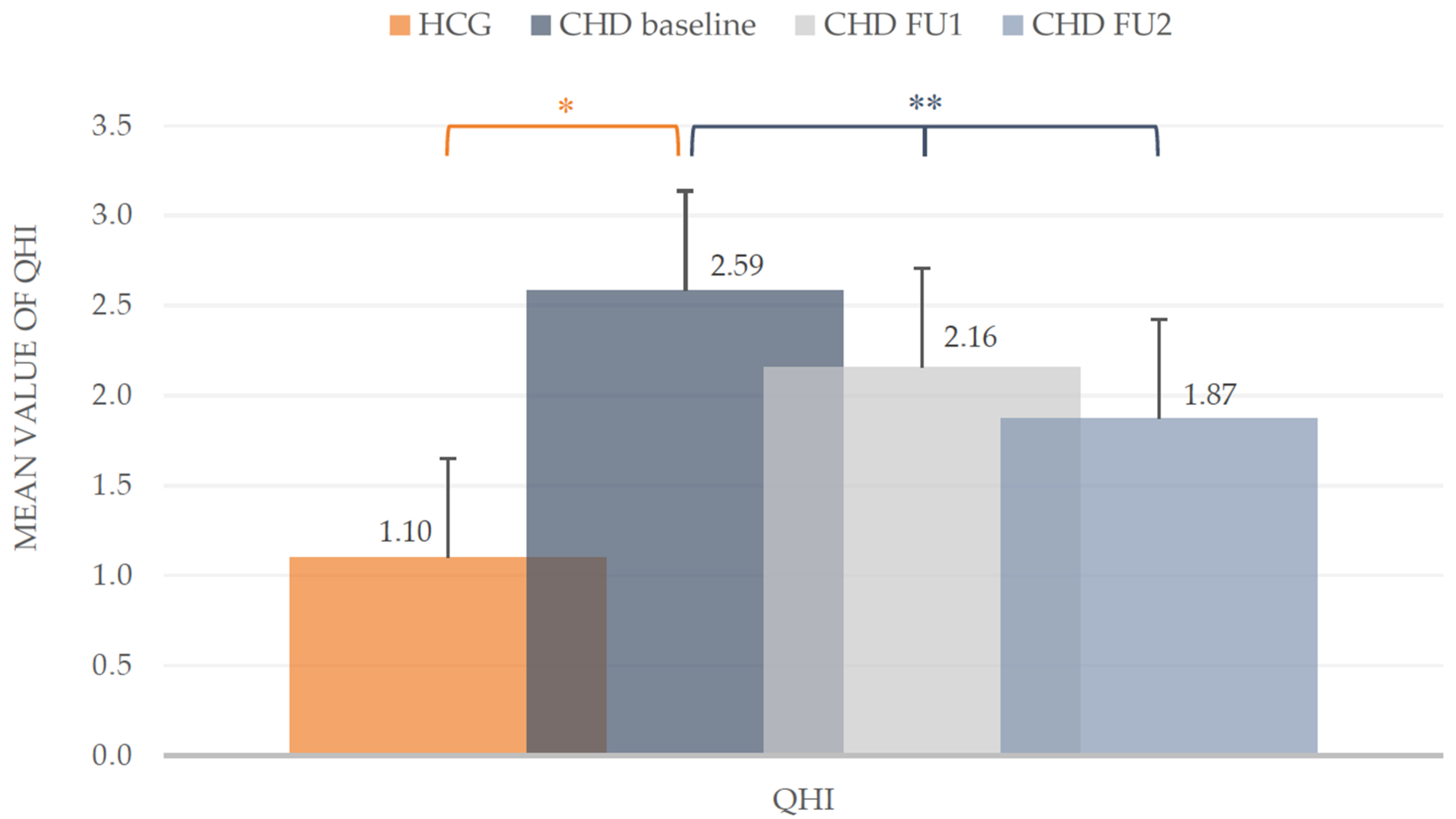
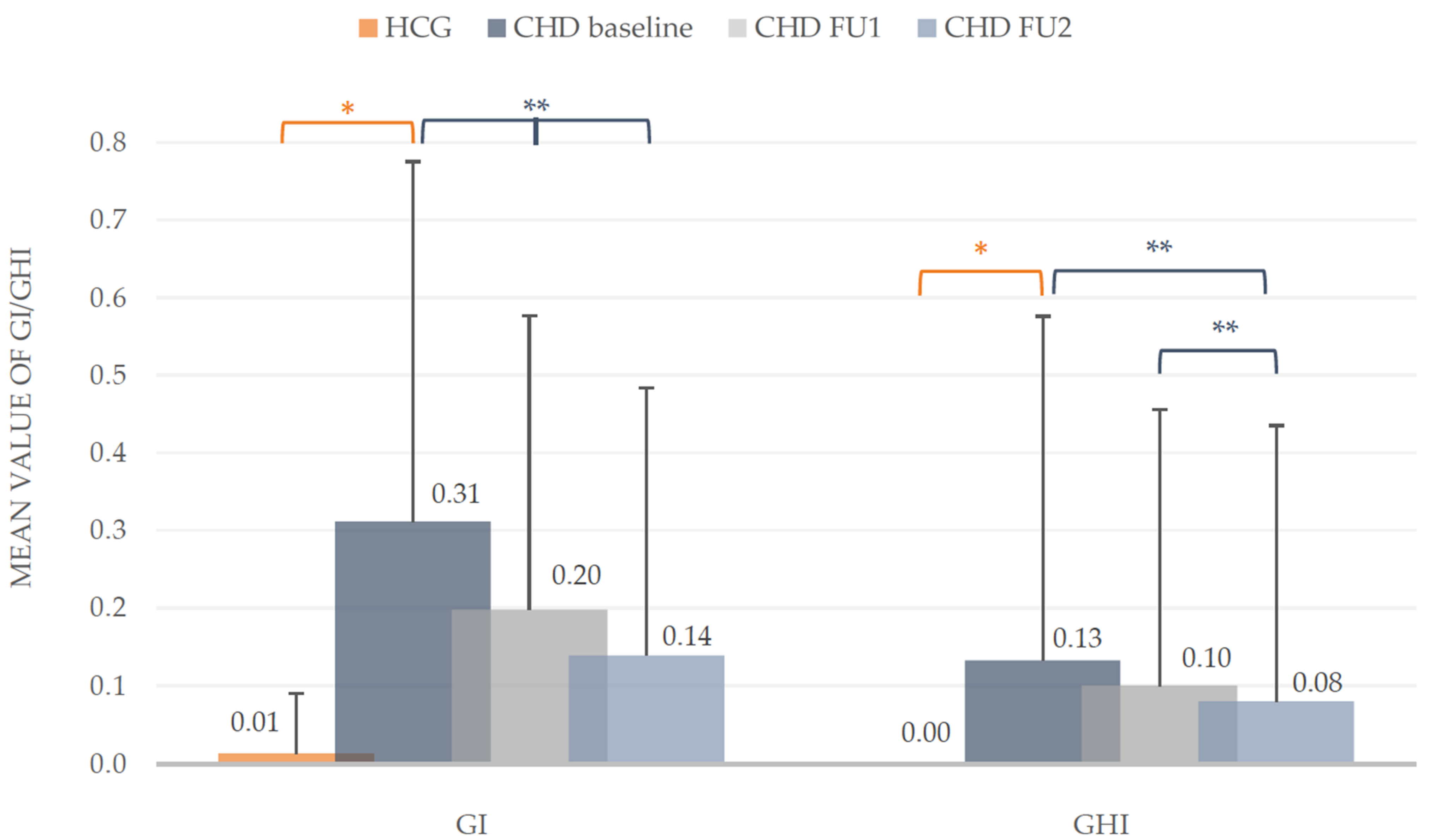
3.2. Oral Hygiene Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lindinger, A.; Schwedler, G.; Hense, H.W. Prevalence of congenital heart defects in newborns in Germany: Results of the first registration year of the PAN Study (July 2006 to June 2007). Klin. Padiatr. 2010, 222, 321–326. [Google Scholar] [CrossRef] [Green Version]
- Schwedler, G.; Lindinger, A.; Lange, P.E.; Sax, U.; Olchvary, J.; Peters, B.; Bauer, U.; Hense, H.W. Frequency and spectrum of congenital heart defects among live births in Germany: A study of the Competence Network for Congenital Heart Defects. Clin. Res. Cardiol. 2011, 100, 1111–1117. [Google Scholar] [CrossRef] [PubMed]
- Ali, H.M.; Mustafa, M.; Hasabalrasol, S.; Elshazali, O.H.; Nasir, E.F.; Ali, R.W.; Berggreen, E.; Skeie, M.S. Presence of plaque, gingivitis and caries in Sudanese children with congenital heart defects. Clin. Oral Investig. 2017, 21, 1299–1307. [Google Scholar] [CrossRef] [Green Version]
- Hallett, K.B.; Radford, D.J.; Seow, W.K. Oral health of children with congenital cardiac diseases: A controlled study. Pediatr. Dent. 1992, 14, 224–230. [Google Scholar]
- Sivertsen, T.B.; Assmus, J.; Greve, G.; Astrom, A.N.; Skeie, M.S. Oral health among children with congenital heart defects in Western Norway. Eur. Arch. Paediatr. Dent. 2016, 17, 397–406. [Google Scholar] [CrossRef]
- Ansari, F.; Ferring, V.; Schulz-Weidner, N.; Wetzel, W.E. Concomitant oral findings in children after cardiac transplant. Pediatr. Transplant. 2006, 10, 215–219. [Google Scholar] [CrossRef]
- Da Silva, D.B.; Souza, I.P.; Cunha, M.C. Knowledge, attitudes and status of oral health in children at risk for infective endocarditis. Int. J. Paediatr. Dent. 2002, 12, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Pourmoghaddas, Z.; Meskin, M.; Sabri, M.; Norousali Tehrani, M.H.; Najafi, T. Dental Caries and Gingival Evaluation in Children with Congenital Heart Disease. Int. J. Prev. Med. 2018, 9, 52. [Google Scholar] [CrossRef]
- Stecksén-Blicks, C.; Rydberg, A.; Nyman, L.; Asplund, S.; Svanberg, C. Dental caries experience in children with congenital heart disease: A case-control study. Int. J. Paediatr. Dent. 2004, 14, 94–100. [Google Scholar] [CrossRef]
- Sivertsen, T.B.; Astrom, A.N.; Greve, G.; Assmus, J.; Skeie, M.S. Effectiveness of an oral health intervention program for children with congenital heart defects. BMC Oral Health 2018, 18, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balmer, R.; Bu’Lock, F.A. The experiences with oral health and dental prevention of children with congenital heart disease. Cardiol. Young 2003, 13, 439–443. [Google Scholar] [CrossRef]
- Pine, C.M.; Harris, R.V.; Burnside, G.; Merrett, M.C. An investigation of the relationship between untreated decayed teeth and dental sepsis in 5-year-old children. Br. Dent. J. 2006, 200, 45–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busuttil, N.A.; Mooney, G.; El-Bahannasawy, E.; Vincent, C.; Wadhwa, E.; Robinson, D.; Welbury, R.R.; Fung, D.E. The dental health and preventative habits of cardiac patients attending the Royal Hospital for Sick Children Glasgow. Eur. Arch. Paediatr. Dent. 2006, 1, 23–30. [Google Scholar] [CrossRef]
- Suvarna, R.; Rai, K.; Hegde, A.M. Knowledge and Oral Health Attitudes among Parents of Children with Congenital Heart Disease. Int. J. Clin. Pediatr. Dent. 2011, 4, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Al-Sarheed, M.; Angeletou, A.; Ashley, P.F.; Lucas, V.S.; Whitehead, B.; Roberts, G.J. An investigation of the oral status and reported oral care of children with heart and heart-lung transplants. Int. J. Paediatr. Dent. 2000, 10, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Ali, H.M.; Mustafa, M.; Nasir, E.F.; Lie, S.A.; Hasabalrasol, S.; Elshazali, O.H.; Ali, R.W.; Skeie, M.S. Oral-health-related background factors and dental service utilisation among Sudanese children with and without a congenital heart defects. BMC Oral Health 2016, 16, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suma, G.; Mohan Das, U.; Ambika, G. Oral health status of normal children and those affiliated with cardiac diseases. J. Clin. Pediatr. Dent. 2011, 35, 315–318. [Google Scholar] [CrossRef]
- Talebi, M.; Khordi Mood, M.; Mahmoudi, M.; Alidad, S. A study on oral health of children with cardiac diseases in Mashhad, Iran in 2004. J. Dent. Res. Dent. Clin. Dent. Prospects 2007, 1, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Rai, K.; Supriya, S.; Hegde, A.M. Oral health status of children with congenital heart disease and the awareness, attitude and knowledge of their parents. J. Clin. Pediatr. Dent. 2009, 33, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Carrilo, C.; Russell, J.; Judd, P.; Casas, M. Oral Health of Children with Congenital Heart Disease at a Pediatric Health Sciene Centre. J. Can. Dent. Assoc. 2018, 84, 1–5. [Google Scholar]
- Siahi-Benlarbi, R.; Nies, S.M.; Sziegoleit, A.; Bauer, J.; Schranz, D.; Wetzel, W.E. Caries-, Candida- and Candida antigen/antibody frequency in children after heart transplantation and children with congenital heart disease. Pediatr. Transplant. 2010, 14, 715–721. [Google Scholar] [CrossRef]
- Thumeyer, A. Die Umsetzung des Zuckerfreien Vormittags durch Verhältnisprävention. DHZ 2009, 4, 314–316. [Google Scholar]
- Thumeyer, A. Meine Kindertagesstätte will Zähne Putzen üben. Available online: https://docplayer.org/17209075-Meine-kindertagesstaette-kindergarten-will-zaehne-putzen-ueben.html (accessed on 23 March 2021).
- Thumeyer, A. Gruppenprophylaxe für Kinder von 0 bis 6 Jahren. Zahnmedizin up2date 2018, 12, 507–522. [Google Scholar] [CrossRef]
- Thumeyer, A.; Buschmann, C. Die KAI-Zahnputz-Systematik. Ein der Entwicklung von Kindern angepasstes Mundpflegekonzept. Oralprophylaxe Kinderzahnheilkd. 2012, 34, 124–128. [Google Scholar]
- Landesarbeitsgemeinschaft für Jugendzahnpflege Hessen (LAGH). Konzept “5 Sterne für gesunde Zähne”. Available online: https://www.lagh.de/wer-wir-sind/5-sterne-fuer-gesunde-zaehne (accessed on 23 March 2021).
- World Health Organization (WHO). Dental caries indices: Tooth (DMFT, dmft) and surface levels (DMFS, dmfs). In Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization (WHO): Geneva, Switzerland, 2013; pp. 51–56. [Google Scholar]
- Pieper, K.; Blumenstein, A. Die Zahnmedizinische Untersuchung im Rahmen der Gruppenprophylaxe: Ein Leitfaden für die EDV-Gestützte Erfolgskontrolle; Pieper, K., Blumenstein, A., Eds.; Verlag Nicht Ermittelbar: Marburg, Germany, 1993. [Google Scholar]
- Fleiss, J.L.; Park, M.H.; Chilton, N.W.; Alman, J.E.; Feldman, R.S.; Chauncey, H.H. Representativeness of the "Ramfjord teeth" for epidemiologic studies of gingivitis and periodontitis. Community Dent. Oral Epidemiol. 1987, 15, 221–224. [Google Scholar] [CrossRef]
- Ramfjord, S.P. Indices for Prevalence and Incidence of Periodontal Disease. J. Periodontol. 1959, 30, 51–59. [Google Scholar] [CrossRef] [Green Version]
- Silness, J.; Loe, H. Periodontal Disease in Pregnancy. II. Correlation between Oral Hygiene and Periodontal Condtion. Acta Odontol. Scand. 1964, 22, 121–135. [Google Scholar] [CrossRef]
- Quigley, G.A.; Hein, J.W. Comparative cleansing efficiency of manual and power brushing. J. Am. Dent. Assoc. 1962, 65, 26–29. [Google Scholar] [CrossRef]
- Bundesausschuss für Risikobewertung. Durchschnittlicher Fluoridgehalt in Trinkwasser ist in Deutschland Niedrig. Available online: https://www.bfr.bund.de/cm/343/durchschnittlicher_fluoridgehalt_in_trinkwasser_ist_in_deutschland_niedrig.pdf (accessed on 23 March 2021).
- Warnes, C.A.; Liberthson, R.; Danielson, G.K.; Dore, A.; Harris, L.; Hoffman, J.I.; Somerville, J.; Williams, R.G.; Webb, G.D. Task force 1: The changing profile of congenital heart disease in adult life. J. Am. Coll. Cardiol. 2001, 37, 1170–1175. [Google Scholar] [CrossRef] [Green Version]
- Balmer, R.; Booras, G.; Parsons, J. The oral health of children considered very high risk for infective endocarditis. Int. J. Paediatr. Dent. 2010, 20, 173–178. [Google Scholar] [CrossRef]
- Da Fonseca, M.A.; Evans, M.; Teske, D.; Thikkurissy, S.; Amini, H. The impact of oral health on the quality of life of young patients with congenital cardiac disease. Cardiol. Young 2009, 19, 252–256. [Google Scholar] [CrossRef]
- Schulz-Weidner, N.; Bulski, J.C.; Siahi-Benlarbi, R.; Bauer, J.; Logeswaran, T.; Jux, C.; Wetzel, W.E.; Kramer, N. Symptom-orientated oral hygiene for children after heart transplantation: Effectiveness of a standardized prophylactic program. Pediatr. Transplant. 2020, 24, e13845. [Google Scholar] [CrossRef]
- Franco, E.; Saunders, C.P.; Roberts, G.J.; Suwanprasit, A. Dental disease, caries related microflora and salivary IgA of children with severe congenital cardiac disease: An epidemiological and oral microbial survey. Pediatr. Dent. 1996, 18, 228–235. [Google Scholar]
- Schulz-Weidner, N.; Logeswaran, T.; Schlenz, M.A.; Kramer, N.; Bulski, J.C. Parental Awareness of Oral Health and Nutritional Behavior in Children with Congenital Heart Diseases Compared to Healthy Children. Int. J. Environ. Res. Public Health 2020, 17, 7057. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| CHD | Baseline | FU1 | FU2 | |||
|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |
| d-t | 0.42 A | 1.21 | 0.50 A | 1.46 | 0.42 A | 1.23 |
| m-t | 0.11 A,B | 0.52 | 0.11 A | 0.51 | 0.20 B | 0.68 |
| f-t | 0.62 A | 1.77 | 0.75 A | 1.92 | 0.88 A | 1.97 |
| dmf-t | 1.15 A | 2.5 | 1.37 B | 2.65 | 1.52 B | 2.73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schulz-Weidner, N.; Logeswaran, T.; Jux, C.; Schlenz, M.A.; Krämer, N.; Bulski, J.C. Evaluation of the Effectiveness of an Interdisciplinary Preventive Oral Hygiene Program for Children with Congenital Heart Disease. Int. J. Environ. Res. Public Health 2021, 18, 3497. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073497
Schulz-Weidner N, Logeswaran T, Jux C, Schlenz MA, Krämer N, Bulski JC. Evaluation of the Effectiveness of an Interdisciplinary Preventive Oral Hygiene Program for Children with Congenital Heart Disease. International Journal of Environmental Research and Public Health. 2021; 18(7):3497. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073497
Chicago/Turabian StyleSchulz-Weidner, Nelly, Thushiha Logeswaran, Christian Jux, Maximiliane Amelie Schlenz, Norbert Krämer, and Julia Camilla Bulski. 2021. "Evaluation of the Effectiveness of an Interdisciplinary Preventive Oral Hygiene Program for Children with Congenital Heart Disease" International Journal of Environmental Research and Public Health 18, no. 7: 3497. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073497