
Systematic Review of Human Poisoning and Toxic Exposures in Myanmar

 , , , ,
, , , ,
Abstract
:1. Introduction
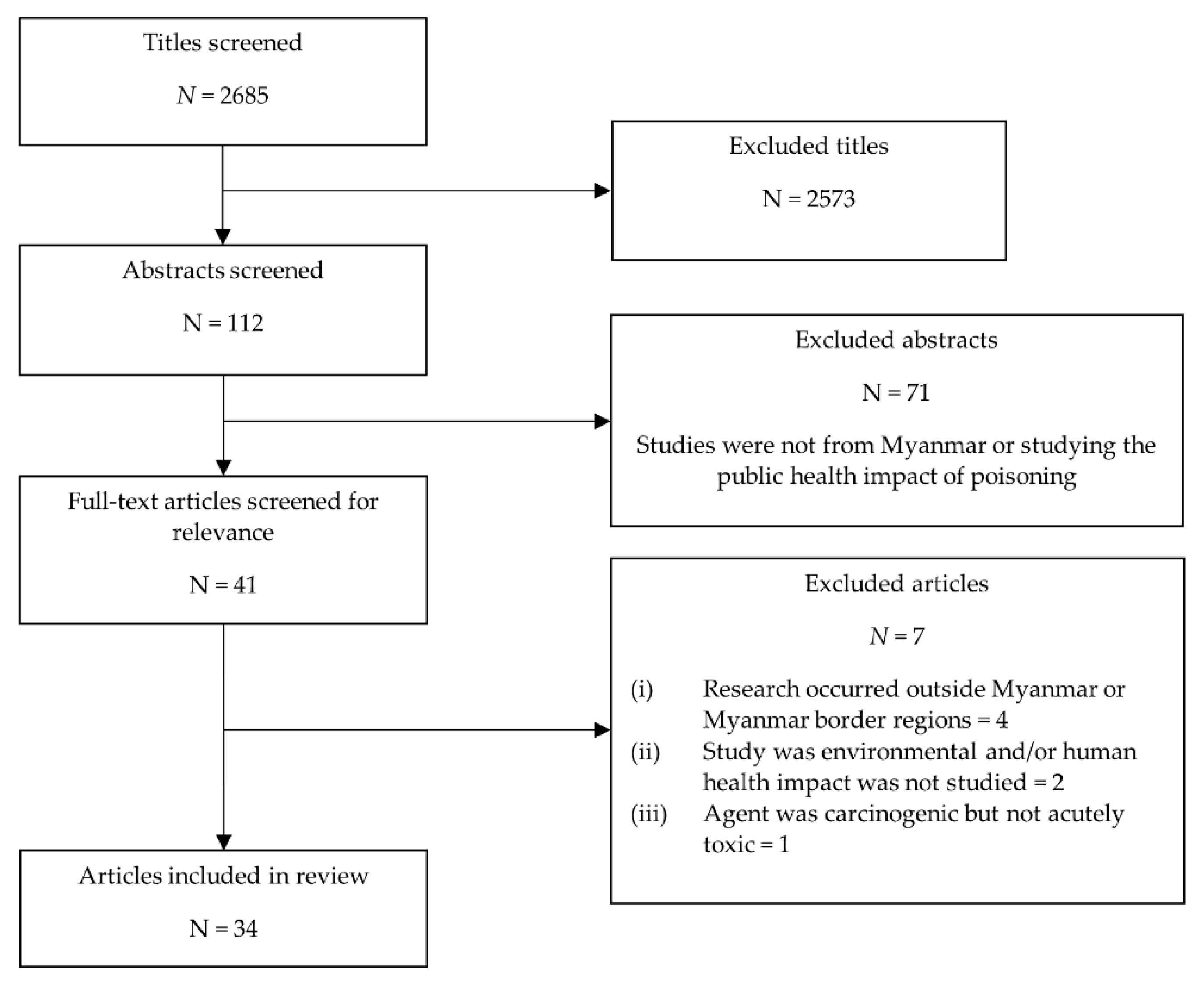
2. Materials and Methods
3. Results
3.1. Envemonation
3.2. Heavy Metals
3.3. Alcohol and Drugs of Abuse
3.4. Agrochemicals
3.5. Traditional Medicine
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Katz, R.; Fischer, J. The revised International Health Regulations: A framework for global pandemic response. Glob. Health Gov. 2010, 3, 1–18. [Google Scholar]
- World Health Organization. International Health Regulations (2005), 3rd ed.; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Van de Pas, R.; van Schaik, L.G. Democratizing the World Health Organization. Public Health 2014, 128, 195–201. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Country Implementation Guide: Voluntary Joint External Evaluation; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. Joint External Evaluation Tool (JEE Tool), 2nd ed.; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- OECD. OECD Environmental Outlook to 2050; OECD Publishing: Paris, France, 2012. [Google Scholar] [CrossRef]
- World Health Organization. International Health Regulations (2005) and Chemical Events; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Settimi, L.; Giordano, F.; Lauria, L.; Celentano, A.; Sesana, F.; Davanzo, F. Surveillance of paediatric exposures to liquid laundry detergent pods in Italy. Inj. Prev. 2018, 24, 5. [Google Scholar] [CrossRef] [PubMed]
- Kamboj, A.; Spiller, H.A.; Casavant, M.J.; Chounthirath, T.; Smith, G.A. Pediatric Exposure to E-Cigarettes, Nicotine, and Tobacco Products in the United States. Pediatrics 2016, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, A.; Law, R.; Lyons, R.; Choudhary, E.; Wolkin, A.; Schier, J. Assessing the public health impact of using poison center data for public health surveillance. Clin. Toxicol. 2018, 56, 646–652. [Google Scholar] [CrossRef] [PubMed]
- FDA Center for Tobacco Products. Final Rule—Tobacco Products Deemed to Be Subject to The Federal Food, Drug, & Cosmetic Act (“Deeming Rule”); U.S. Food and Drug Administration: Silver Spring, MD, USA, 2016.
- FDA Center for Tobacco Products. FDA Requirements for Newly Regulated Tobacco Products; U.S. Food and Drug Administration: Silver Spring, MD, USA, 2017; Volume 2020.
- Satoh, T. Toxicology in Asia—Past, present, and future. Hum. Exp. Toxicol. 2015, 34, 1291–1296. [Google Scholar] [CrossRef] [Green Version]
- Makalinao, I.R.; Awang, R. Poison control centers in developing countries and Asia’s need for toxicology education. Toxicol. Appl. Pharm. 2005, 207, 716–721. [Google Scholar] [CrossRef]
- World Health Organization. Joint External Evaluation of IHR Core Capacities of The Republic of the Union of Myanmar: Executive Summary; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Pyone, T.; Aung, T.T.; Endericks, T.; Myint, N.W.; Inamdar, L.; Collins, S.; Pwint, K.H.; Hein, B.B.; Wilson, A. Health system governance in strengthening International Health Regulations (IHR) compliance in Myanmar. BMJ Glob. Health 2020, 5. [Google Scholar] [CrossRef] [PubMed]
- Thein, M. Economic Development of Myanmar; Institute of Southeast Asian Studies: Singapore, 2004. [Google Scholar]
- UNEP. Global Chemicals Outlook: Towards Sound Management of Chemicals; United Nations Environment Programme: Nairobi, Kenya, 2015. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Mahmood, M.A.; Halliday, D.; Cumming, R.; Thwin, K.T.; Myitzu, M.; White, J.; Alfred, S.; Warrell, D.A.; Bacon, D.; Naing, W.; et al. Inadequate knowledge about snakebite envenoming symptoms and application of harmful first aid methods in the community in high snakebite incidence areas of Myanmar. PLoS Negl. Trop. Dis. 2019, 13, e0007171. [Google Scholar] [CrossRef]
- Mahmood, M.A.; Halliday, D.; Cumming, R.; Thwin, K.-T.; Kyaw, M.M.Z.; White, J.; Alfred, S.; Warrell, D.; Bacon, D.; Naing, W.; et al. Snakebite incidence in two townships in Mandalay Division, Myanmar. PLoS Negl. Trop. Dis. 2018, 12, e0006643. [Google Scholar] [CrossRef] [Green Version]
- Schioldann, E.; Mahmood, M.A.; Kyaw, M.M.; Halliday, D.; Thwin, K.T.; Chit, N.N.; Cumming, R.; Bacon, D.; Alfred, S.; White, J.; et al. Why snakebite patients in Myanmar seek traditional healers despite availability of biomedical care at hospitals? Community perspectives on reasons. PLoS Negl. Trop. Dis. 2018, 12, e0006299. [Google Scholar] [CrossRef] [Green Version]
- White, J.; Alfred, S.; Bates, D.; Mahmood, M.A.; Warrell, D.; Cumming, R.; Thwin, K.T.; Thein, M.M.; Thant, M.; Naung, Z.M.J.T.X. Twelve month prospective study of snakebite in a major teaching hospital in Mandalay, Myanmar; Myanmar Snakebite Project (MSP). Toxicon 2019, 1, 100002. [Google Scholar] [CrossRef]
- Myo-Khin; Theingi-Nyunt; Nyan-Tun-Oo; Ye-Hla. Prognostic indicators in patients with snakebite: Analysis of two-year data from a township hospital in central Myanmar. WHO South-East Asia J. Public Health 2012, 1, 144–150. [Google Scholar] [CrossRef]
- Tun-Pe; Aye-Aye-Myint; Sann-Mya; Khin-Aye-Kyu; Kyaw-Than; Aung-Myint; Tint-Lwin; Myint-Soe; Min-Than. Clinical Features of Russellís Viper (Daboia russelii siamensis) Bite Cases Admitted to Six Township Hospitals of Snakebite Endemic Divisions of Myanmar. In Proceedings of the Management of Snakebite and Research, Yangon, Myanmar, 11–12 December 2001. [Google Scholar]
- Pe, T.; Myint, A.A.; Mya, S.; Kyu, K.A.; Toe, M.M. Incidence, case fatality rate and treatment-seeking behaviour of the snakebite victims from two townships of Myanmar. Myanmar Health Sci. Res. 2005, 17, 72–80. [Google Scholar]
- Aye, K.-P.; Thanachartwet, V.; Soe, C.; Desakorn, V.; Chamnanchanunt, S.; Sahassananda, D.; Supaporn, T.; Sitprija, V. Predictive factors for death after snake envenomation in Myanmar. Wilderness Environ. Med. 2018, 29, 166–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aye, K.-P.; Thanachartwet, V.; Soe, C.; Desakorn, V.; Thwin, K.-T.; Chamnanchanunt, S.; Sahassananda, D.; Supaporn, T.; Sitprija, V. Clinical and laboratory parameters associated with acute kidney injury in patients with snakebite envenomation: A prospective observational study from Myanmar. BMC Nephrol. 2017, 18, 92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aye, M.T.H.; Naing, T.; Myint, K.T. Unusual ocular manifestations following viper bite. BMJ Case Rep. 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Thein, C.M.; Byard, R.W. Characteristics and relative numbers of lethal snake bite cases in medicolegal practice in central Myanmar—A five year study. J. Forensic Leg. Med. 2019, 63, 52–55. [Google Scholar] [CrossRef]
- Pe, T.; Mya, S.; Myint, A.A.; Htay, M.T.; Toe, M.M. Epidemiological study of sea snakebite victims of Kyaikkami Township (Mon State). Myanmar Health Sci. Res. J. 2005, 17, 32–35. [Google Scholar]
- Pe, T.; Myint, A.A.; Mya, S.; Toe, M.M. Sea snakebite in Myanmar: Epidemiology and treatment seeking behaviour. Myanmar Health Sci. Res. J. 2006, 18, 1–5. [Google Scholar]
- Mya, S.; Pe, T.; Myint, A.A.; Maw, A.A. Sea snake bites in Letkokekone: A situation analysis. Myanmar Health Sci. Res. J. 2005, 17, 27–31. [Google Scholar]
- Myint, T.; Pe, T.; Mya, S. Two sea snake bite cases admitted to Yangon General Hospital. Myanmar Health Sci. Res. J. 2006, 18, 161–162. [Google Scholar]
- Myint, A.A.; Pe, T.; Maw, T.Z. An Epidemiological Study of Snakebite and Venomous Snake Survey in Myanmar. In Proceedings of the Management of Snakebite and Research, Yangon, Myanmar, 11–12 December 2001. [Google Scholar]
- Thu, W.N.N.; Htar, L.T.; Htut, T.; Kyaw, S.; Khine, M.M. Changes in Blood Arsenic Level and Haematological Parameters of Male Subjects Living in Kyaungkone Township. Myanmar Health Sci. Res. J. 2010, 22, 164–169. [Google Scholar]
- Oo, T.T.; Thien, Z.L.; Thant, Z.; Ohnmar. Plasma malondialdehyde level and vibration perception threshold in non-exposed subjects and lead-exposed battery workers. Myanmar Health Sci. Res. J. 2018, 30. [Google Scholar]
- Wai, K.M.; Mar, O.; Kosaka, S.; Umemura, M.; Watanabe, C. Prenatal Heavy Metal Exposure and Adverse Birth Outcomes in Myanmar: A Birth-Cohort Study. Int. J. Environ. Res. Public Health 2017, 14, 1339. [Google Scholar] [CrossRef] [Green Version]
- Wai, K.M.; Umezaki, M.; Kosaka, S.; Mar, O.; Umemura, M.; Fillman, T.; Watanabe, C. Impact of prenatal heavy metal exposure on newborn leucocyte telomere length: A birth-cohort study. Environ. Pollut. 2018, 243, 1414–1421. [Google Scholar] [CrossRef] [PubMed]
- Mar Wai, K.; Umezaki, M.; Mar, O.; Umemura, M.; Watanabe, C. Arsenic exposure through drinking Water and oxidative stress Status: A cross-sectional study in the Ayeyarwady region, Myanmar. J. Trace Elem. Med. Biol. Organ. Soc. Miner. Trace Elem. 2019, 54, 103–109. [Google Scholar] [CrossRef]
- Mochizuki, H.; Phyu, K.P.; Aung, M.N.; Zin, P.W.; Yano, Y.; Myint, M.Z.; Thit, W.M.; Yamamoto, Y.; Hishikawa, Y.; Thant, K.Z.; et al. Peripheral neuropathy induced by drinking water contaminated with low-dose arsenic in Myanmar. Environ. Health Prev. Med. 2019, 24, 23. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, T.; Jentes, E.; Ortega, L.; Scalia Sucosky, M.; Jefferies, T.; Bajcevic, P.; Parr, V.; Jones, W.; Brown, M.J.; Painter, J. Lead Poisoning in United States-Bound Refugee Children: Thailand-Burma Border, 2009. Pediatrics 2012, 129, e392. [Google Scholar] [CrossRef] [Green Version]
- Saw, Y.M.; Saw, T.N.; Yasuoka, J.; Chan, N.; Kham, N.P.E.; Khine, W.; Cho, S.M.; Jimba, M.J.H.R.J. Gender difference in early initiation of methamphetamine use among current methamphetamine users in Muse, Northern Shan State, Myanmar. Harm Reduc. 2017, 14, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Balogun, O.; Koyanagi, A.; Stickley, A.; Gilmour, S.; Shibuya, K. Alcohol Consumption and Psychological Distress in Adolescents: A Multi-Country Study. J. Adolesc. Health 2014, 54, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Ezard, N.; Thiptharakun, S.; Nosten, F.; Rhodes, T.; McGready, R. Risky alcohol use among reproductive-age men, not women, in Mae La refugee camp, Thailand, 2009. Confl. Health 2012, 6, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston, L.G.; Soe, P.M.; Aung, M.Y.; Ammassari, S. Estimating the Population Size of Males Who Inject Drugs in Myanmar: Methods for Obtaining Township and National Estimates. AIDS Behav. 2019, 23, 295–301. [Google Scholar] [CrossRef]
- Hail-Jares, K.; Choi, S.; Duoc, L.; Luoc, Z.; Huanga, Z.J. Occupational and demographic factors associated with drug use among female sex workers at the China–Myanmar border. Drug Alcohol Depend. 2016, 161, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Lwin, T.Z.; Than, A.A.; Min, A.Z.; Robson, M.G.; Siriwong, W. Effects of pesticide exposure on reproductivity of male groundnut farmers in Kyauk Kan village, Nyaung-U, Mandalay region, Myanmar. Risk Manag. Healthc. Policy 2018, 11, 235–241. [Google Scholar] [CrossRef] [Green Version]
- Khine, Y.Y. Acute Kidney Injury following Ingestion of Henna Leaf Extract: A Case Report from Myanmar. Blood Purif. 2017, 44 (Suppl. S1), 41–45. [Google Scholar] [CrossRef]
- Myint, A.A.; Myint, T.L.; Pe, T. Poisonous snakebites of Myanmar with special references to the bites and case fatality rate. Myanmar Health Sci. Res. J. 2007, 19, 87–93. [Google Scholar]
- Del Brutto, O.H.; Del Brutto, V.J. Neurological complications of venomous snake bites: A review. Acta Neurol. Scand. 2012, 125, 363–372. [Google Scholar] [CrossRef]
- Zheng, L.; Kuo, C.-C.; Fadrowski, J.; Agnew, J.; Weaver, V.M.; Navas-Acien, A. Arsenic and Chronic Kidney Disease: A Systematic Review. Curr. Environ. Health Rep. 2014, 1, 192–207. [Google Scholar] [CrossRef] [Green Version]
- Obeng-Gyasi, E. Chronic cadmium exposure and cardiovascular disease in adults. J. Environ. Sci. Health Part A 2020, 55, 726–729. [Google Scholar] [CrossRef]
- Wasserman, G.A.; Liu, X.; Factor-Litvak, P.; Gardner, J.M.; Graziano, J.H. Developmental Impacts of Heavy Metals and Undernutrition. Basic Clin. Pharmacol. Toxicol. 2008, 102, 212–217. [Google Scholar] [CrossRef] [PubMed]
- MacTavish, R.C.; Rémillard, L.W.; Davison, C.M. Environmental Lead Exposure and Adult Literacy in Myanmar: An Exploratory Study of Potential Associations at the Township Level. Int. J. Environ. Res. Public Health 2018, 15, 1086. [Google Scholar] [CrossRef] [Green Version]
- Global SMART Programme. Patterns and Trends of Amphetamine-Type Stimulants and Other Drugs: Challenges for Asia and the Pacific; United Nations Office on Drugs and Crime: Vienna, Austria, 2013. [Google Scholar]
- UNODC. Myanmar Country Profile; United Nations Office on Drugs and Crime: Vienna, Austria, 2005. [Google Scholar]
- UNODC. World Drug Report 2020: Booklet 3, Drug Supply; United Nations Office on Drugs and Crime: Vienna, Austria, 2020. [Google Scholar]
- Global SMART Programme. Synthetic Drugs in East and South-East Asia: Trends and Patterns of Amphetamine-type Stimulants and New Psychoactive Substances; United Nations Office on Drugs and Crime: Vienna, Austria, 2019. [Google Scholar]
- UNODC Global SMART Programme. Myanmar: Situation Assessment on Amphetamine-Type Stimulants; United Nations Office on Drugs and Crime: Vienna, Austria, 2010. [Google Scholar]
- Mathers, B.M.; Degenhardt, L.; Phillips, B.; Wiessing, L.; Hickman, M.; Strathdee, S.A.; Wodak, A.; Panda, S.; Tyndall, M.; Toufik, A.J.T.L. Global epidemiology of injecting drug use and HIV among people who inject drugs: A systematic review. Lancet 2008, 372, 1733–1745. [Google Scholar] [CrossRef]
- Aceijas, C.; Stimson, G.V.; Hickman, M.; Rhodes, T.J.A. Global overview of injecting drug use and HIV infection among injecting drug users. AIDS 2004, 18, 2295–2303. [Google Scholar] [CrossRef] [PubMed]
- Lai, L. Treating substance abuse as a consequence of conflict and displacement: A call for a more inclusive global mental health. Med. Confl. Surviv. 2014, 30, 182–189. [Google Scholar] [CrossRef]
- Ezard, N.; Oppenheimer, E.; Burton, A.; Schilperoord, M.; Macdonald, D.; Adelekan, M.; Sakarati, A.; van Ommeren, M. Six rapid assessments of alcohol and other substance use in populations displaced by conflict. Confl. Health 2011, 5, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kesavachandran, C.N.; Fareed, M.; Pathak, M.K.; Bihari, V.; Mathur, N.; Srivastava, A.K. Adverse health effects of pesticides in agrarian populations of developing countries. Rev. Environ. Contam. Toxicol. 2009, 200, 33–52. [Google Scholar]
- New Yangon General Hospital Poison Treatment Centrere (Ed.) Poison Management Guidelines; New Yangon General Hospital: Yangon, Myanmar, 2020. [Google Scholar]
- Kyaw, Z.Z. Outcomes of Poisoning Patients Admitted to Poison Treatment Centre; New Yangon General Hospital, University of Public Health: Yangon, Myanmar, 2017. [Google Scholar]
- Azazh, A. Case series of 2,4-D poisoning in Tikur Anbessa Teaching Hospital. Ethiop. Med. J. 2010, 48, 243–246. [Google Scholar]


{kind=link}
| Criteria Topics | Include | Exclude | Rationale/Comment |
|---|---|---|---|
| Literature | Peer-reviewed literature | Literature that has not been peer-reviewed | Peer-reviewed literature is the academic standard |
| Grey literature of high quality | Low-quality grey literature | High quality grey literature is a useful and trusted source of information. | |
| Epidemiological studies and case studies | Studies on community perception of risk | Epidemiological studies and case studies on poison outcomes demonstrate that poisoning is experienced in Myanmar. Papers that focus on community perceptions of risk or social constructs around poisoning only were excluded from the review. | |
| English language literature | Literature in a language other than English | English is a common second language in Myanmar and university courses are often taught in English. As such, articles published in the Myanmar Health Sciences Research Journal are written in English, and the exclusion of articles written in a Myanmar language did not significantly impact the availability of locally produced research. | |
| Poisoning | Acute and chronic poisoning as a result of short- or long-term exposure to a toxic substance. | Acute and chronic exposure to the majority of biological agents. | Toxic substances will include exposure to pharmaceuticals, drugs of abuse chemicals and envenomation. Reports of adverse reactions to therapeutic does of drugs (rather than overdose) excluded. |
| Food and water exposures | Exposure to heavy metals such as lead and mercury through food or water sources was included in the review. Food poisoning as a result of toxins produced by foodborne bacteria excluded from the study. Food poisoning only included as a result of chemical contamination of food. | ||
| Myanmar | Articles written from border regions that have been displaced from Myanmar. | Myanmar people living in other countries outside of border regions. | Articles on Myanmar people who have migrated to other countries, or on poisoning as a result of Myanmar animal species kept as pets in other countries, have been excluded. |
| Study | Poisoning | Region | Context or Population | Number of Participants | Majority Participant Gender | Age | Self-Harm Studied? |
|---|---|---|---|---|---|---|---|
| Mahmood et al. 2019 [20,21] | Snakebite | Mandalay | Farming townships | 4276 | 50.1% Male | Primarily 18+ | N/A |
| Schioldann et al. 2018 [22] | Snakebite | Mandalay | Farming townships | 135 (7 *) | 57.14% Male * | 12 to 45 years * | N/A |
| Mahmood et al. 2018 [21] | Snakebite | Mandalay | Farming townships | 4276 | 50.1% Male | Primarily 18+ | N/A |
| White et al. 2019 [23] | Snakebite | Mandalay | Mandalay General Hospital | 948 | 61.2% Male | 18+ | N/A |
| Myo-Khin et al. 2012 [24] | Snakebite | Mandalay | Nahtoogyi Township Hospital | 101 | 69% Male | Mean 32.2 (SD: 15.5, range: 3–80 years) | N/A |
| Pe et al. 2002 [25] | Snakebite | National | Six township hospitals from five snakebite endemic divisions | 294 | 77% Male | Average 27 years (range: 7–75 years) | N/A |
| Pe et al. 2005 [26] | Snakebite | Magway and Mandalay Region | Taungdwingyi and Kyaukpadaung townships | 1381 * | 64.8% Male * | Mean: 30 years (range:3–84 years) * | N/A |
| Aye et al. 2018 [27] | Snakebite | Yangon | Tertiary hospitals | 246 | 80.0% Male | Median 31 (IQR: 23–42) | N/A |
| Aye et al. 2017 [28] | Snakebite | Yangon | Tertiary hospitals | 258 | 78.7% Male | Median 31 (IQR: 23–42) | N/A |
| Aye, Naing and Myint, 2018 [29] | Snakebite | Magway | Case study | 1 | Male | 70 years | N/A |
| Thien and Byard, 2019 [30] | Snakebite | Magway | Magway Region General Hospital | 84 † | 64% Male † | Age range 5–75 years, mean 33 years † | N/A |
| Pe et al. 2005 [31] | Sea snake bite | Mon | Fishing communities | 46 | >97% Male | 12–65 years | N/A |
| Pe et al. 2006 [32] | Sea snake bite | Yangon, Mon and Ayeyawady | Fishing communities | 187 * | 89.3% Male * | Mean 35.64 years (range: 10–87 years) * | N/A |
| Mya et al. 2005 [33] | Sea snake bite | Yangon | Fishing communities | 47 | 95.7% Male | 16–87 years | N/A |
| Myint, Pe and Mya, 2006 [34] | Sea snake bite | Yangon | Fishermen | 2 | Males | 21 and 56 years old | N/A |
| Myint, Pe and Maw, 2002 [35] | Snakebite | National | Healthcare data | Not provided | Not provided | Range: 6–77 years | N/A |
| Thu et al. 2010 [36] | Arsenic | Ayeyawady | Community members | 70 | 100% Male | 18–50 years old | N/A |
| Oo et al. 2018 [37] | Lead | Yangon | Men working in small-scale battery workplaces | 56 | 100% Male | 24–45 years | N/A |
| Wai et al. 2017 [38] | Heavy metals | Ayeyawady | Pregnant women and newborns | 419 | 100% Female | Mean: 28 years old (SD: 6.6 years) | N/A |
| Wai et al. 2018 [39] | Heavy metals | Ayeyawady | Pregnant women and newborns | 409 | 100% Female | Mean: 28 years old (SD: 6.6 years) | N/A |
| Wai et al. 2019 [40] | Arsenic | Ayeyawady | Pregnant women | 198 | 100% Female | Mean: 28 years old (SD: 6.6 years) | N/A |
| Mochizuki et al. 2019 [41] | Arsenic | Ayeyawady | Thabaung Township | 1867 | 61% Female | Mean: 35.2 ± 20.4 | N/A |
| Mitchell et al. 2012 [42] | Lead | Thailand-Myanmar border | Displaced children | 642 | 51.7% Male | Range: 6 months to 14 years | |
| Saw et al. 2017 [43] | Methamphetamine | Shan | Students, laborers, housewives, highway drivers, female sex workers (FSW) and men who have sex with men (MSM) near the Chinese border | 1362 | 56.9% Male | 18–35 years | No |
| Balogun et al. 2013 [44] | Alcohol | Not provided | Students | 2804 | 50.8% Male | 13–15 years | No |
| Ezard et al. 2012 [45] | Alcohol | Thailand-Myanmar border | Displaced pregnant women | 636 | 100% Female | Median 26.2 years (range: 15 47 years) | No |
| Johnston et al. 2018 [46] | Drugs of abuse | National | Injecting drug users | ~3920 § | >99% Male | ≥15 years | No |
| Hail-Jares et al. 2016 [47] | Drugs of abuse | Shan | FSW | 101 | 100% Female | Median 25 years (IQR 22–28) | No |
| Lwin et al. 2018 [48] | Organophosphate Pesticides | Mandalay | Groundnut farmers | 400 (100 ‡) | 100% Male ‡ | Mean 37.5 years ±9.45 years (range: 18–49 years) ‡ | No |
| Khine, 2017 [49] | Traditional medicine (Dan Ywet) | Yangon | Hospital patient | 1 | Male | 34 years old | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cook, M.A.; Jagpal, P.S.; Hnin Pwint, K.; San, L.L.; Kyaw Thein, S.S.; Pyone, T.; Thit, W.M.M.; Bradberry, S.M.; Collins, S. Systematic Review of Human Poisoning and Toxic Exposures in Myanmar. Int. J. Environ. Res. Public Health 2021, 18, 3576. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073576
Cook MA, Jagpal PS, Hnin Pwint K, San LL, Kyaw Thein SS, Pyone T, Thit WMM, Bradberry SM, Collins S. Systematic Review of Human Poisoning and Toxic Exposures in Myanmar. International Journal of Environmental Research and Public Health. 2021; 18(7):3576. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073576
Chicago/Turabian StyleCook, Meghan A., Pardeep S. Jagpal, Khin Hnin Pwint, Lai Lai San, Saint Saint Kyaw Thein, Thidar Pyone, Win Moh Moh Thit, Sally M. Bradberry, and Samuel Collins. 2021. "Systematic Review of Human Poisoning and Toxic Exposures in Myanmar" International Journal of Environmental Research and Public Health 18, no. 7: 3576. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073576