
Exploring Food Literacy Domains in an Adult Samoan Population

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
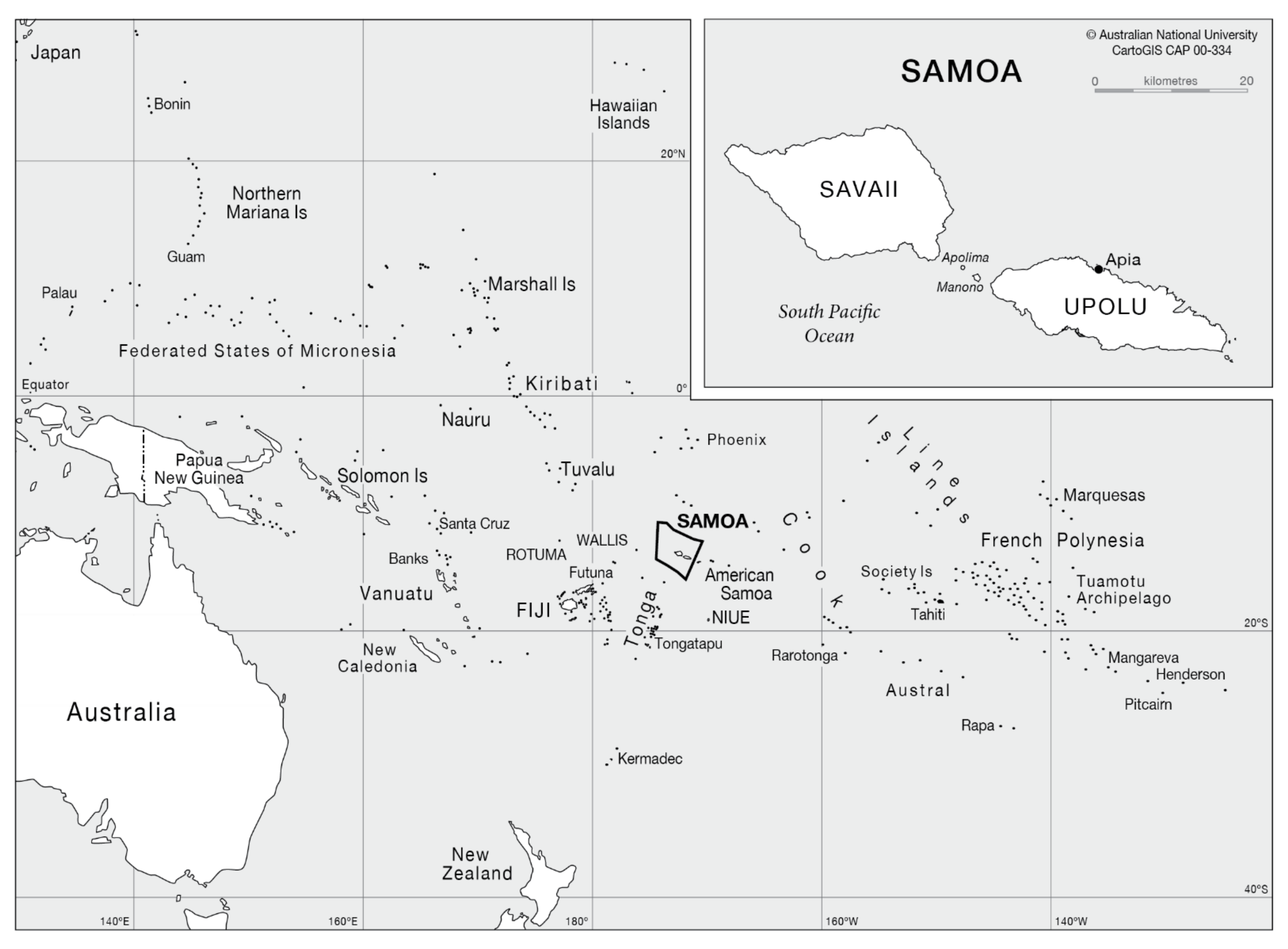
2.1. Study Setting and Design
2.2. Participant Recruitment
2.3. Data Collection Tool
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. Demographic Characteristics of Participants
3.2. Food Literacy Domains
3.2.1. Plan and Manage
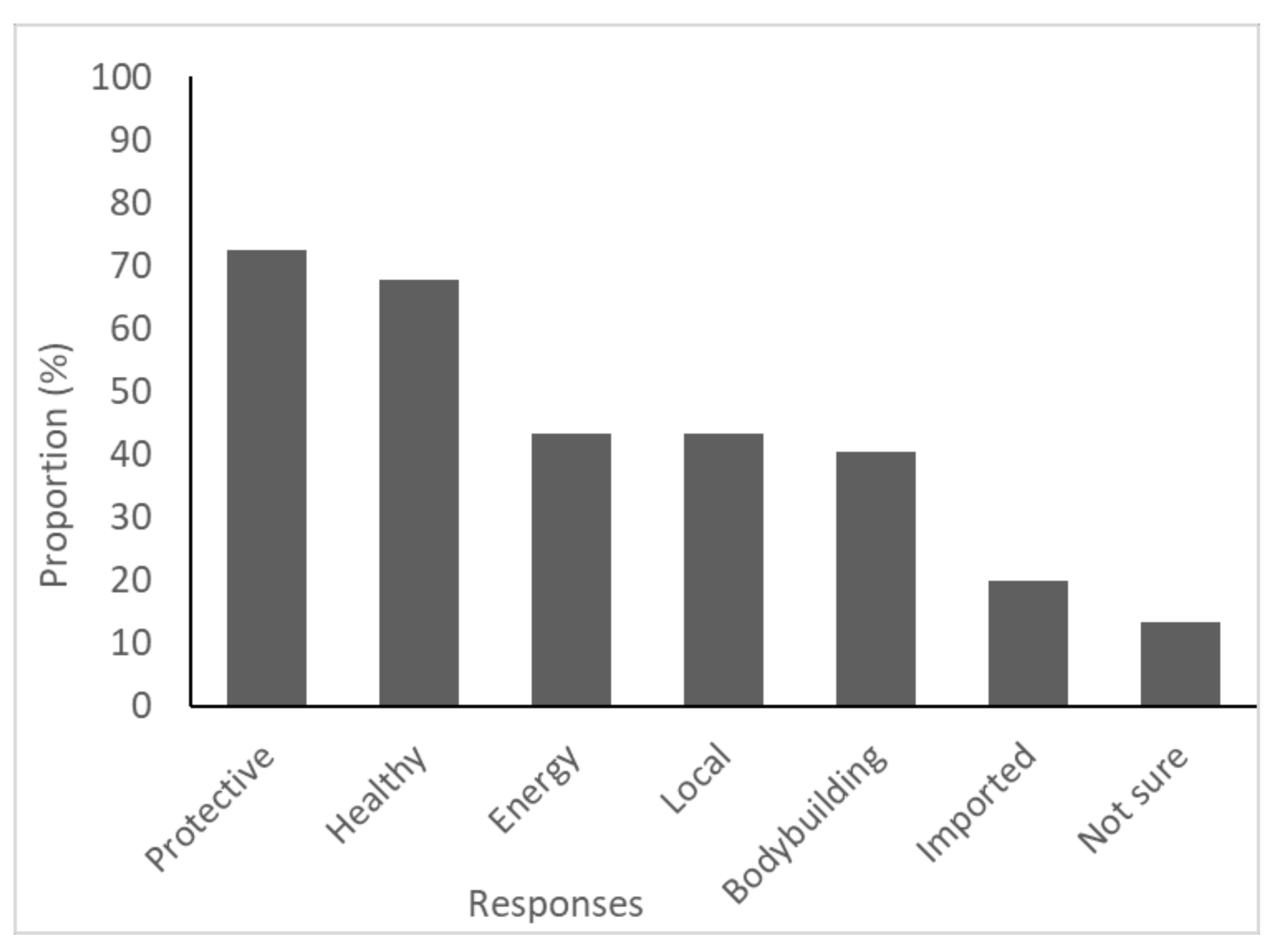
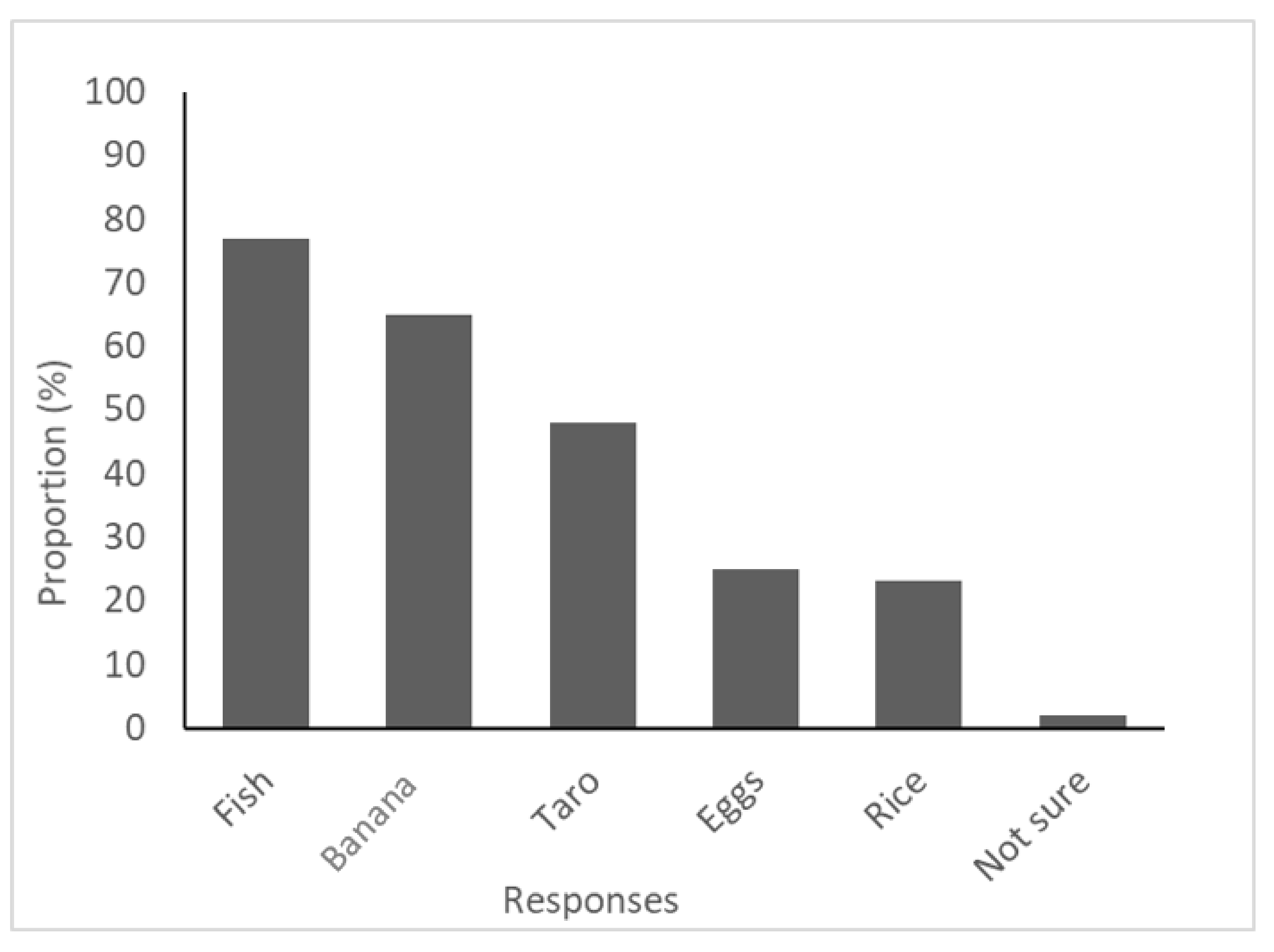
3.2.2. Select
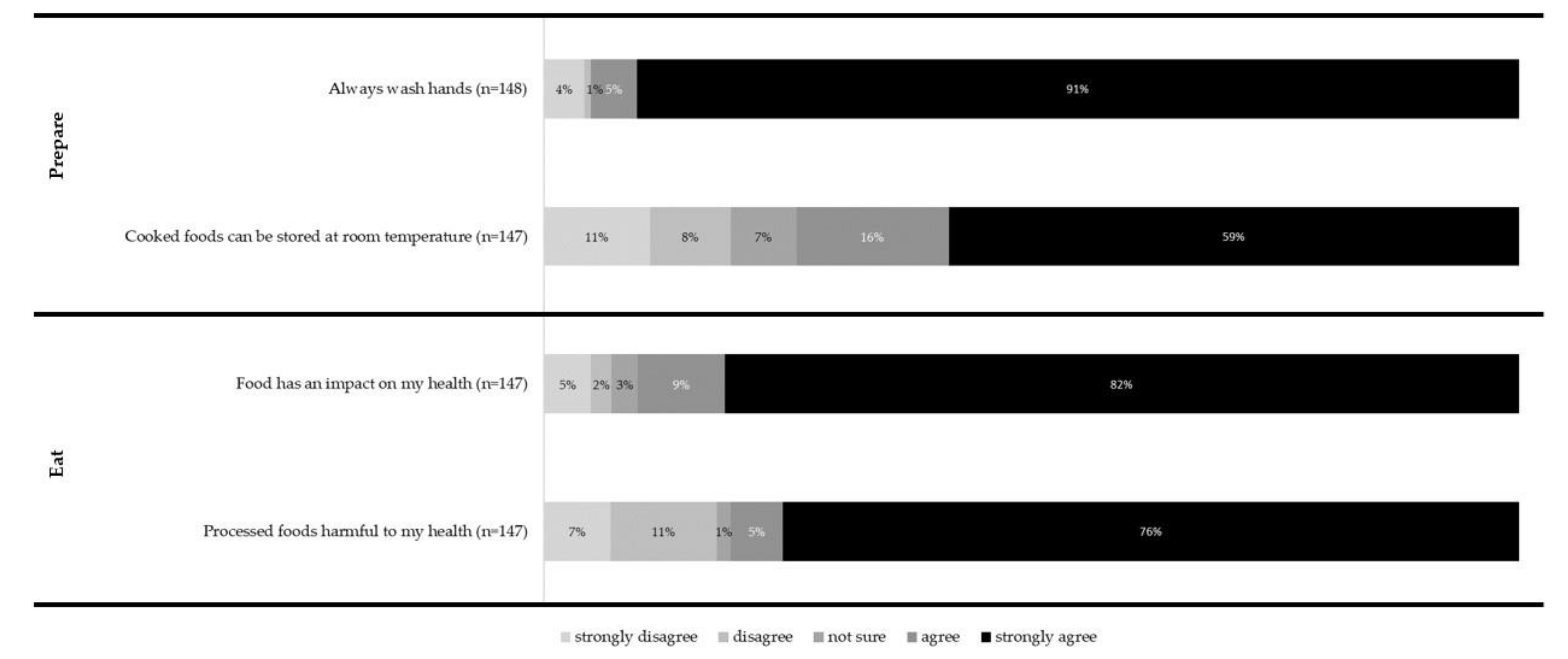
3.2.3. Prepare
3.2.4. Eat
4. Discussion
4.1. Plan and Manage
4.2. Select
4.3. Prepare
4.4. Eat
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- FAO. Dynamic Development, Shifting Demographics, Changing Diets; FAO: Bangkok, Thailand, 2018; p. 172. Available online: http://www.fao.org/3/I8499EN/i8499en.pdf (accessed on 25 October 2020).
- Sahal Estimé, M.; Lutz, B.; Strobel, F. Trade as a structural driver of dietary risk factors for noncommunicable diseases in the Pacific: An analysis of household income and expenditure survey data. Glob. Health 2014, 10, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlton, K.E.; Russell, J.; Gorman, E.; Hanich, Q.; Delisle, A.; Campbell, B.; Bell, J. Fish, food security and health in Pacific Island countries and territories: A systematic literature review. BMC Public Health 2016, 16, 285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessaram, T.; McKenzie, J.; Girin, N.; Roth, A.; Vivili, P.; Williams, G.; Hoy, D. Noncommunicable diseases and risk factors in adult populations of several Pacific Islands: Results from the WHO STEPwise approach to surveillance. Aust. N. Z. J. Public Health 2015, 39, 336–343. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Noncommunicable Diseases Country Profiles 2018; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Public Health Division of the Pacific Community. Pacific Guidelines for Healthy Living: A Handbook for Health Professionals and Educators; Public Health Division of the Pacific Community: Noumea, New Caledonia, 2018; Available online: https://spccfpstore1.blob.core.windows.net/digitallibrary-docs/files/ba/baf6a038be97061f945d822c3695b8b1.pdf?sv=2015-12-11&sr=b&sig=6s%2Fkn%2Fhq%2Bs8J3CPxPTWjAhX7XY6yUQ%2F17QbICUPw%2Bws%3D&se=2019-10-26T23%3A37%3A38Z&sp=r&rscc=public%2C%20max-age%3D864000%2C%20max-stale%3D86400&rsct=application%2Fpdf&rscd=inline%3B%20filename%3D%22Pacific_guidelines_for_a_Healthy_diet_and_lifestyle___a_handbook_for_health_profesionals_and_educators.pdf%22 (accessed on 25 October 2020).
- Vidgen, H.A.; Gallegos, D. Defining food literacy and its components. Appetite 2014, 76, 50–59. [Google Scholar] [CrossRef]
- Bollars, C.; Sørensen, K.; de Vries, N.; Meertens, R. Exploring health literacy in relation to noncommunicable diseases in Samoa: A qualitative study. BMC Public Health 2019, 19, 1151. [Google Scholar] [CrossRef] [Green Version]
- Krause, C.; Sommerhalder, K.; Beer-Borst, S.; Abel, T. Just a subtle difference? Findings from a systematic review on definitions of nutrition literacy and food literacy. Health Promot. Int. 2018, 33, 378–389. [Google Scholar] [CrossRef] [Green Version]
- FAO. Dietary Patterns of Households in Samoa: Identifying the Factors and Food Items Most Important to Understanding Nutrition; FAO: Apia, Samoa, 2017; Available online: http://www.fao.org/3/a-i5973e.pdf (accessed on 25 October 2020).
- Reeve, E.; Thow, A.-M.; Bell, C.; Soti-Ulberg, C.; Sacks, G. Identifying opportunities to strengthen school food environments in the Pacific: A case study in Samoa. Res. Sq. 2020. [Google Scholar] [CrossRef]
- Farrell, P.; Thow, A.M.; Schuster, S.; Vizintin, P.; Negin, J. Access to a Nutritious Diet in Samoa: Local Insights. Ecol. Food Nutr. 2019, 58, 189–206. [Google Scholar] [CrossRef]
- Tanawattanacharoen, V.K.; Choy, C.C.; Anesi, T.J.; Naseri, T.; Soti-Ulberg, C.; Reupena, M.S.; Hawley, N.L. Piloting a food photo sorting activity in Samoa to assess maternal beliefs and their role in child diet. Matern. Child Nutr. 2020, 16, e12974. [Google Scholar] [CrossRef] [Green Version]
- Butcher, H.; Burkhart, S.; Paul, N.; Tiitii, U.; Tamuera, K.; Eria, T.; Swanepoel, L. Role of Seaweed in Diets of Samoa and Kiribati: Exploring Key Motivators for Consumption. Sustainability 2020, 12, 7356. [Google Scholar] [CrossRef]
- Jones, A.M.P.; Dempewolf, H.; Armstrong, R.; Gallucci, K.; Tavana, N.U.G. Staple food choices in Samoa: Do changing dietary trends reflect local food preferences? Ethnobot. Res. Appl. 2011, 9, 455–462. [Google Scholar] [CrossRef] [Green Version]
- Samoa Bureau of Statistics. Village Directory 2016: Census 2016 Preliminary Count; Samoa Bureau of Statistics: Apia, Samoa, 2016; p. 19. Available online: https://www.sbs.gov.ws/digi/1-Preliminary%20count%20report%202016.V2.pdf (accessed on 12 February 2021).
- Samoa Bureau of Statistics. Statistical Abstract 2017; Samoa Bureau of Statistics: Apia, Samoa, 2018. Available online: https://www.sbs.gov.ws/digi/2017%20-%20Samoa%20Bureau%20of%20Statistics%20-%20Statistical%20Abstract.pdf (accessed on 12 March 2021).
- CartoGIS Services, The Australian National University. The South Pacific Ocean Showing the Location of Samoa with Inset of the Main Islands and Its Capital Apia; Australian National University: Canberra, Australia, 2020; Available online: https://asiapacific.anu.edu.au/mapsonline/base-maps/samoa-pacific (accessed on 20 October 2020).
- Begley, A.; Paynter, E.; Dhaliwal, S.S. Evaluation Tool Development for Food Literacy Programs. Nutrients 2018, 10, 1617. [Google Scholar] [CrossRef] [Green Version]
- Doustmohammadian, A.; Omidvar, N.; Keshavarz-Mohammadi, N.; Abdollahi, M.; Amini, M.; Eini-Zinab, H. Developing and validating a scale to measure Food and Nutrition Literacy (FNLIT) in elementary school children in Iran. PLoS ONE 2017, 12, e0179196. [Google Scholar] [CrossRef] [Green Version]
- Poelman, M.; Dijkstra, S.; Sponselee, H.; Kamphuis, C.; Battjes-Fries, M.; Gillebaart, M.; Seidell, J. Towards the measurement of food literacy with respect to healthy eating: The development and validation of the self perceived food literacy scale among an adult sample in the Netherlands. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Gréa Krause, C.; Beer-Borst, S.; Sommerhalder, K.; Hayoz, S.; Abel, T. A short food literacy questionnaire (SFLQ) for adults: Findings from a Swiss validation study. Appetite 2018, 120, 275–280. [Google Scholar] [CrossRef]
- Farran, S. Pacific Perspectives: Fa’afafine and Fakaleiti in Samoa and Tonga: People Between Worlds. Liverp. Law Rev. 2010, 31, 13–28. [Google Scholar] [CrossRef]
- Samoa Bureau of Statistics. 2016 Census Brief No. 2 Population Dynamics and Trends; Samoa Bureau of Statistics: Apia, Samoa, 2018; p. 45. Available online: https://www.sbs.gov.ws/digi/3-2016%20Census%20Brief%20No.2.pdf (accessed on 11 March 2021).
- Begley, A.; Paynter, E.; Butcher, L.M.; Dhaliwal, S.S. Examining the Association between Food Literacy and Food Insecurity. Nutrients 2019, 11, 445. [Google Scholar] [CrossRef] [Green Version]
- Nathalie Troubat, E.F.; Aliyeva, R. Food Secuirty and Food Consumption in Samoa—Based on the Analysis of the 2018 Household Income and Expenditure Survey; FAO and SBS: Apia, Samoa, 2020; Available online: https://reliefweb.int/report/samoa/food-security-and-food-consumption-samoa-based-analysis-2018-household-income-and (accessed on 18 February 2021).
- Maubach, N.; Hoek, J. A qualitative study of New Zealand parents’ views on front-of-pack nutrition labels. Nutr. Diet. 2010, 67, 90–96. [Google Scholar] [CrossRef]
- Campos, S.; Doxey, J.; Hammond, D. Nutrition labels on pre-packaged foods: A systematic review. Public Health Nutr. 2011, 14, 1496–1506. [Google Scholar] [CrossRef] [Green Version]
- Lassetter, J.H.; Clark, L.; Morgan, S.E.; Brown, L.B.; Van Servellen, G.; Duncan, K.; Hopkins, E.S. Health literacy and obesity among native Hawaiian and Pacific Islanders in the United States. Public Health Nurs. 2015, 32, 15–23. [Google Scholar] [CrossRef]
- Soon, H.N.W. Food Literacy: What Does Food Literacy Mean for Samoan Families? Auckland University of Technology: Auckland, New Zealand, 2016. [Google Scholar]
- Gorton, D. Nutrition Labelling—Update of Scientific Evidence on Consumer Use and Understanding of Nutrition Labels and Claims; The University of Auckland: Auckland, New Zealand, 2007; Available online: https://www.mpi.govt.nz/dmsdocument/26015/direct (accessed on 15 October 2020).
- Ministry of Health. Food (Safety and Quality) Regulations 2017; Legislative Assembly of Samoa, Ed.; Ministry of Health: Apia, Samoa, 2017; Available online: https://samoa.tradeportal.org/media/Food%20(Safety%20and%20Quality)%20Regulations%202017.pdf (accessed on 15 October 2020).
- Snowdon, W.; Raj, A.; Reeve, E.; Guerrero, R.L.T.; Fesaitu, J.; Cateine, K.; Guignet, C. Processed foods available in the Pacific Islands. Glob. Health 2013, 9, 53. [Google Scholar] [CrossRef] [Green Version]
- Mills, M.A. “Cooking with Love”: Food, Gender, and Power; Georgia State University: Atlanta, GA, USA, 2010. [Google Scholar]
- World Health Organization. Five Keys to Safer Food Manual; World Health Organization: Geneva, Switzerland, 2006; Available online: https://www.who.int/foodsafety/publications/consumer/manual_keys.pdf (accessed on 16 October 2020).
- World Health Organization. WHO Estimates of the Global Burden of Foodborne Disease; World Health Organization: Geneva, Switerland, 2015; Available online: https://apps.who.int/iris/bitstream/handle/10665/199350/9789241565165_eng.pdf?sequence=1 (accessed on 15 October 2020).
- Samoa National Codex Committee. Samoa National Codex Strategic Plan 2017–2021; Ministry of Commerce, Industry & Labour: Apia, Samoa, 2017. Available online: https://www.mcil.gov.ws/storage/2017/08/SAMOA_FOOD_SAFETY_CONSUMER_PROTECTION_STRATEGIC_PLAN-2017.pdf (accessed on 15 October 2020).
- Ihara, E.S.; Vakalahi, H.F.O. Spirituality: The Essence of Wellness Among Tongan and Samoan Elders. J. Relig. Spiritual. Soc. Work Soc. Thought 2011, 30, 405–421. [Google Scholar] [CrossRef]
- Tui Atua, T.T.T.E. Bioethics and the Samoan indigenous reference. Int. Soc. Sci. J. 2009, 60, 115–124. [Google Scholar] [CrossRef]
- Spronk, I.; Kullen, C.; Burdon, C.; O’Connor, H. Relationship between nutrition knowledge and dietary intake. Br. J. Nutr. 2014, 111, 1713–1726. [Google Scholar] [CrossRef] [Green Version]
- Fiti-Sinclair, R. Knowledge, Attitudes, Beliefs and Practices Related to the Consumption of Fruit and Vegetables in Samoa; FAO Sub-Regional Office for the Pacific Islands, Apia, Samoa. 2004. Available online: http://www.fao.org/3/an432e/an432e00.pdf (accessed on 10 August 2020).
- Abdelhamid, A.S.; Brown, T.J.; Brainard, J.S.; Biswas, P.; Thorpe, G.C.; Moore, H.J.; Deane, K.H.O.; Summerbell, C.D.; Worthington, H.V.; Song, F.; et al. Omega-3 fatty acids for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2020. [Google Scholar] [CrossRef]
- FAO. School Nutrition Education Programmes Scoping Study and Capacity Needs Assessment—Final Report; FAO: Apia, Samoa, 2019; p. 130. Available online: http://www.fao.org/3/ca2935en/ca2935en.pdf (accessed on 12 November 2020).
- Fruean, A. Project to Review Dietary Guidelines in Samoa, Pacific. Available online: https://www.samoaobserver.ws/category/samoa/72516 (accessed on 20 October 2020).
- World Health Organization. Healthy Islands: Best Practices in Health Promotion in the Pacific; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Althubaiti, A. Information bias in health research: Definition, pitfalls, and adjustment methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristic (Total Responses n) | Frequency | Total (%) * |
|---|---|---|
| Gender (n = 144) | ||
| Male | 65 | 45 |
| Female | 78 | 54 |
| Fa’afafine ^ | 1 | 1 |
| Age group (n = 150) | ||
| 20–34 | 23 | 15 |
| 35–44 | 58 | 39 |
| 45–54 | 38 | 25 |
| 55+ | 31 | 21 |
| Marital status (n = 150) | ||
| Single | 18 | 12 |
| Never married | 7 | 5 |
| Married | 111 | 74 |
| Divorced | 7 | 5 |
| Widowed | 4 | 3 |
| Prefer not to say | 3 | 2 |
| Employment status (n = 148) | ||
| Work on plantation | 12 | 8 |
| Part-time employed | 9 | 6 |
| Full-time employed | 68 | 46 |
| Unemployed and looking for job | 18 | 12 |
| Unemployed and not looking for job | 36 | 24 |
| Prefer not to say | 5 | 4 |
| Highest level of completed education (n = 147) | ||
| Did not attend school | 0 | 0 |
| Primary | 28 | 19 |
| Secondary/High school | 88 | 60 |
| Technical college/Vocational/Trade college | 14 | 9 |
| University | 17 | 12 |
| Food Literacy Domain | Food Literacy Behaviour (n = Number of Total Responses) | Never or Rarely n (%) | Sometimes n (%) | Most of the Time n (%) | Always n (%) |
|---|---|---|---|---|---|
| Plan and manage | Plan meals ahead of time (145) | 8 (6) | 28 (19) | 35 (24) | 74 (51) |
| Make a list before you go shopping (144) | 26 (18) | 19 (13) | 12 (8) | 87 (61) | |
| Plan to include healthy food (143) | 4 (3) | 13 (9) | 29 (20) | 97 (68) | |
| Budget money for food (142) | 13 (9.0) | 4 (3) | 12 (8) | 113 (80) | |
| Select | Use the nutrition information when deciding what to eat (121) | 21 (17) | 32 (26) | 25 (21) | 43 (36) |
| Prepare | Cook meals at home (146) | 8 (5) | 28 (19) | 30 (21) | 80 (55) |
| Feel confident cooking a variety of foods (143) | 11 (8) | 36 (25) | 21 (15) | 75 (52) | |
| Change recipes to make them heathier (143) | 12 (8) | 42 (29) | 25 (18) | 64 (45) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kammholz, G.; Craven, D.; Boodoosingh, R.; Akeli Amaama, S.; Abraham, J.; Burkhart, S. Exploring Food Literacy Domains in an Adult Samoan Population. Int. J. Environ. Res. Public Health 2021, 18, 3587. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073587
Kammholz G, Craven D, Boodoosingh R, Akeli Amaama S, Abraham J, Burkhart S. Exploring Food Literacy Domains in an Adult Samoan Population. International Journal of Environmental Research and Public Health. 2021; 18(7):3587. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073587
Chicago/Turabian StyleKammholz, Grace, Dana Craven, Ramona Boodoosingh, Safua Akeli Amaama, Jyothi Abraham, and Sarah Burkhart. 2021. "Exploring Food Literacy Domains in an Adult Samoan Population" International Journal of Environmental Research and Public Health 18, no. 7: 3587. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073587