
Job Demands, Resources and Strains of Outpatient Caregivers during the COVID-19 Pandemic in Germany: A Qualitative Study

 ,
,
Abstract
:1. Introduction
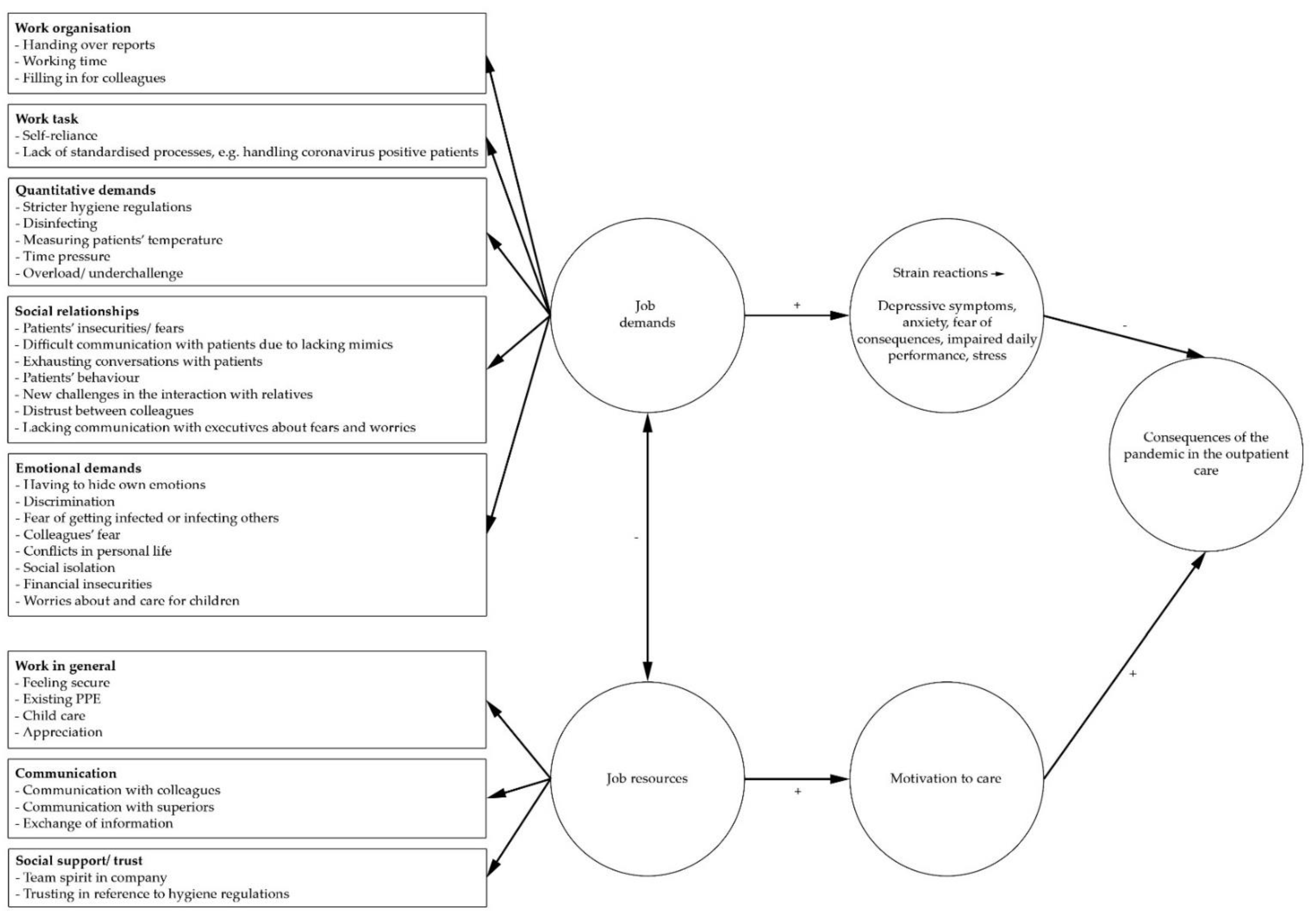
1.1. Theoretical Model
1.2. Current State of Research
1.2.1. Job Demands and Resources in the Outpatient Care
1.2.2. Job Demands, Resources and Strain Reactions in the Course of the COVID-19 Pandemic
1.3. Study Aims and Research Questions
- What are the specific job demands of outpatient caregivers with regard to the COVID-19 pandemic?
- What are job resources outpatient caregivers can rely on while working during the COVID-19 pandemic?
- Which individual strain reactions do outpatient caregivers perceive?
2. Materials and Methods
2.1. Methodological Orientation and Theory
2.2. Study Design
2.3. Participant Selection and Interview Conduct
2.4. Interview Guideline
2.5. Analysis
3. Results
3.1. Sample Characteristics
3.2. Job Demands during the COVID-19 Pandemic
3.2.1. Work Organization
“(…) the topic of handovers is really important in the outpatient care sector. (…) but there is no exchange of information from face-to-face anymore, mainly via documentations in written form. (…) Since you have to be very independent in the outpatient care regarding medication procurement or prescription, there is the possibility of information unwillingly getting lost somewhere which will lead to unnecessary stress the next day. That is difficult.” (Interviewee #7)
“There is more work. (…). Especially at the beginning, when it was starting and we were getting more orders. (…)”. (Interviewee #2)
“I often have to fill in for constantly sick colleagues and there was also the quarantine regulation for people coming back from risk areas who had to stay home for 14 days. That was often occupied by younger colleagues.” (Interviewee #14)
3.2.2. Work Task
“Well, it is kind of difficult to describe (…), but my head is constantly rattling all the steps through, so now each step is reconsidered twice or for three times extra.” (Interviewee #7)
“The procedure in our outpatient care service would make me skip any work shift and stay home until my test result would come in. All clients would be treated by the head of the care service while putting on personal protective equipment only. (…) The course of disease will decide whether the patient needs to get to the hospital or whether outpatient care is still possible or not.” (Interviewee #11)
3.2.3. Quantitative Demands
“(…) I’m always in these gloves while working so I feel like I’m more exposed to disinfectants and my fingers are feeling like that already.” (Interviewee #2)
“We have to pay even more attention than usual to hygiene procedures. We are requested to do daily fever measurements and to document every single symptom (…).” (Interviewee #8)
“Well, we have received the regulatory order to measure temperatures of the patients daily. I find that very annoying.” (Interviewee #11)
“(…) and then all colleagues were driving around for three days, checking every store to get thermometers. You can’t give an employee only one thermometer which they take with them to all the patients. So we need to have one individual thermometer for each client. It was an insane action to get those.” (Interviewee #4)
“For instance we have to get a prescription from a practice or we have to get medications from a pharmacy. Because of the coronavirus we have to wait—for example in the practice there were only two person allowed in there. So we have to wait for like half an hour outside until the other people are finished. And in the pharmacy we have a waiting period, too. Every ten minutes someone is allowed to go in only, while wearing masks and so on.; therefore, there is delay everywhere (…).” (Interviewee #10)
3.2.4. Work Environment and Tools
“(…) it’s not always possible to keep the distance to patients, for instance when showering, applying lotion or putting on their clothes, you cannot keep the distance.” (Interviewee #5)
“Well, there is always a risk. But I’m doing everything that I can to not get infected.” (Interviewee #5)
“Quite low. Because we have all materials, I think we even might be more protected than the general citizens. Since we have hand disinfectants, enough masks and enough gowns. And more important: we know how to use them.” (Interviewee #8)
“(…) when I’m at work I have to keep the mask on the whole time, except for the times I’m driving in my car. I feel I’m not able to receive enough air to breathe.” (Interviewee #2)
“(…) it’s of course annoying at work. Especially when we have to do something, I don’t know, have to shower someone, it’s warm and stuffy and one has a silly mask on. Well that is just annoying (...).” (Interviewee #4)
“It’s of course really difficult looking at the coronavirus situation because there are a lot of gaps, it starts with the masks. This is a great gap. In theory you have to use a new mask after each patient, it doesn’t matter whether it’s fabric or disposable, just to cut off the line there a little bit more.” (Interviewee #12)
“(…) it was burdening that personal protection equipment was not available, such as disinfectants, FFP-2-masks and so on, that was really tiring then. I was afraid, how could I protect myself? (…).“ (Interviewee #6)
3.2.5. Social Relationships
“You would want to care face-to-face because there is usually an emotional connection to clients, no matter if they can communicate or not, you look each other in the eyes, you talk to each other and then the mask, it is somehow not the same.” (Interviewee #7)
“Well, a special challenge is of course handling the patients’ fears or to handle everything in the environment, that is very, very difficult. To convince patients that we are experts and that we know how to protect ourselves and to protect our patients of course and that we don’t expose them to something that they could get sick by. And this conviction takes really a lot of energy and they are so fearful and so on (…).” (Interviewee #9)
“(…) so we had a very difficult case, she really disinfected after us after every move. That was very awful.” (Interviewee #8)
“I had to calm down one patient who was scared of death. She was also dement which was difficult in combination with the fear of death, she was aggressive. But she was bedridden so I wasn’t scared that she could harm me but of course, I had to stay there and be patient and careful, step-by-step I needed to reduce her nervousness.” (Interviewee #10)
“And then the conversion of relatives suddenly being very mad. One has to spend many hours to explain to relatives which measures are needed and that it is not possible to let them enter the room, even if they are treated ambulatory in the treated environment and they don’t get it. And then they try to come in anyways and yes, many are claiming that caregivers have to think of all the interventions themselves and try to bypass all the recommendations.” (Interviewee #13)
“What will happen in the end, you don’t know, I don’t think that anyone will stick to it 100 percent, it’s just like that.” (Interviewee #2)
3.2.6. Emotional Demands
“Well, one always looks whether it is an adequate situation or not. So when I’m with an already crying client because they are scared, of course I won’t say “I’m also scared you might get it”. One is clearly aware of that.” (Interviewee #7)
“And also, when one has sneezed or something like that, it caused sudden panic: ‘Are you healthy? Do you have something?’ Doors were opened and ‘Do you have a cold, are you coughing?’ (…). And when people know what you are doing professionally, like my neighbors in my building, they did fear me. And if I’m thinking about it, my son is living with me, his father clearly stated: ‘You know what your mother is doing professionally, I would like to see you but I’m scared that you will drag in something in my house’.” (Interviewee #11)
“That’s indeed always there.” (Interviewee #13)
“(…) I’m rather scared for my relatives, the clients or colleagues. Me myself, I’m 25, I’m completely/ I’m not afraid.” (Interviewee #7)
“An insanely big fear of mine is to infect clients. Despite of hygiene measures. And if there was a difficult fatal course of events, I think, I don’t know what would be. In the beginning, I even thought or rather I still think that I would need powerful psychological support, because I then would have someone on my conscience. And that’s the opposite of one’s expectations and one’s profession.” (Interviewee #11)
“I’m not that happy anymore because I am not able to create my leisure time as I’m used to. I’m a person who likes alone time but they took my choice to go for like shopping or to see other people. To me that’s really awful, to me that’s kind of social isolation which is really hard to deal with and that make sometimes mad (…).” (Interviewee #9)
“(…). Or that one client suddenly called and said: “Well, I won’t be there anymore. I’ll return when all of this is over.” (…). And that’s difficult because there is no security and financial worries can emerge.” (Interviewee #13)
“One has to be caregiver, mother and teacher all at the same time, that’s just like that (…).” (Interviewee #1)
“Well, to me one big challenge is my family. I have massive fights with my son who is chronically underchallenged, who has arguments with me and who bumps with me, which he usually gets done in the schoolyard. Now he is taking care of that with me at home.” (Interviewee #12)
“(…) Because of my son. Because he’s not able to go to school and you fear that he could grow lonely completely.” (Interviewee #3)
“The overload is the unknown. And how long. How long will that be? How long one can buffer certain things.” (Interviewee #11)
3.3. Work-Related Resources
“Apart from all the materials we have, the main support factor is the support of which is indeed being felt by leadership, colleagues, really, when meeting colleagues in the morning or is calling them, there is clearly a sense of unity. (…).” (Interviewee #7)
3.3.1. Social Support and Trust
“I’m hoping for it, yes, I have to trust in that, otherwise we won’t be able to make it. I wouldn’t be able to work otherwise.” (Interviewee #6)
3.3.2. Communication
“Yes, we are always exchanging information with colleagues, when something doesn’t seem right, they can then give advices and then one will calm down a little by talking to someone.” (Interviewee #5)
“When there is worry or fear my superior has always got a ready ear. For instance, I’ve called her on the weekend. Yes, it was the weekend and she was not in the office but I’ve called her anyways. She even was afraid of and worried for the virus, too as well as for the patients and employees. (…). It helped me a lot, she was positive with me and through that I’ve found strength. She is no psychologist but my boss of course. She couldn’t do more.” (Interviewee #10)
3.3.3. Exchange of Information
“Thus concrete, most of the times we get the latest information and hygiene regulations which are currently valid and we get many facts to bring information over to the patients and they will get educated. And we also had bigger tables about/ we really had conversations about the coronavirus and about fear and so on. We already had two meetings to speak about that with each other.” (Interviewee #6)
3.3.4. Appreciation
“Well yes, they are very proud of us that we keep working despite of the corona pandemic and that we keep being there for them. (…). Exactly. And our care service manager as well and other people, too.” (Interviewee #5)
“(…) the building I’m living in, many older people and one family are living there, and somehow at the beginning of my moving in, no one really knew that I’m a geriatric nurse and now they know they find it very, very nice. And so I’m clearly noticing appreciation and especially in these times, where not everybody was forced to leave the house and many were given the possibility of home office, everyone noticed: “Okay, he nevertheless leaves the house at 5 am to get to work”. I feel appreciation by seeing that people are joyful and find it nice to see what I’m doing. Yes, I’ve been told that many more times in the current situation.” (Interviewee #7)
3.4. Strain Reactions Experienced by Outpatient Caregivers
3.4.1. Depressive Symptoms
“Listless. You can only go to work, do homework with your child and then you go to sleep. And her school’s homework are enormous, what they expect. Well, what does depressive mean, well, yes, I would say it like that.” (Interviewee #1)
3.4.2. Anxiety
“Well, especially at the beginning, by the time everyone was allowed to work from home and one had the feeling to be cannon fodder. Oneself was technically much unprotected at the beginning because until then there was no / it wasn’t like that that everybody was working with a mask.” (Interviewee #11)
3.4.3. Fear of Consequences of the Pandemic
“And in this future with a lot of this virus, we all are scared because we don’t know, what will come the next day? That is the uncertainty. (…) What will come afterwards? What’s the next step?” (Interviewee #10)
3.4.4. Individual Daily Performance
“Yes, well, that is indeed a lot. Because of the fact that children are at home and a full-time job on top, and then doing home-schooling with three kids, that too is a task. Apart from my job, it is a challenge.” (Interviewee #8)
3.4.5. Perception of Stress
“Yes, I’m more irritated. I am indeed more irritated, I notice that at home I have never griped at my daughter that much.” (Interviewee #1)
“Yes, with the/ the self-incrimination for self-protection is higher, definitely the perception of stress.” (Interviewee #2)
4. Discussion
4.1. Discussion of Interview Results
4.1.1. Job Demands Faced by Outpatient Caregivers during the COVID-19 Pandemic
4.1.2. Work-Related Resources
4.1.3. Resultant Strain Reactions Experienced by Outpatient Caregivers
4.2. Strengths and Limitations
4.3. Implications for Further Research and Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pan American Health Organization. Protecting Mental Health during Epidemics; Pan American Health Organization: Washington, DC, USA, 2009; pp. 1–20. [Google Scholar]
- Robert Koch-Institut. SARS-CoV-2: Informationen des Robert Koch-Instituts zu empfohlenen Infektionsschutzmaßnahmen und Zielen. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Empfohlene_Schutzmaßnahmen.html (accessed on 15 June 2020).
- Fallon, A.; Dukelow, T.; Kennelly, S.P.; O’Neill, D. COVID-19 in nursing homes. QJM Mon. J. Assoc. Physicians 2020, 113, 391–392. [Google Scholar] [CrossRef] [Green Version]
- Robert Koch-Institut. Hinweise für ambulante Pflegedienste im Rahmen der COVID-19-Pandemie, Stand: 23.11.2020. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Altenpflegeheime.html (accessed on 23 December 2020).
- Eurofound. Living, Working and COVID-19, COVID-19 Series; Publications Office of the European Union: Luxembourg, 2020. [Google Scholar]
- Statista. Anzahl von Pflegeheimen und Ambulanten Pflegediensten in Deutschland in den Jahren 1999 bis 2019. Available online: https://de.statista.com/statistik/daten/studie/2729/umfrage/anzahl-der-pflegeheime-und-ambulanten-pflegedienste-seit-1999/ (accessed on 16 March 2021).
- Statistisches Bundesamt (Destatis). Pflegestatistik. Pflege im Rahmen der Pflegeversicherung. Deutschlandergebnisse. 2019. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Gesundheit/Pflege/Publikationen/Downloads-Pflege/pflege-deutschlandergebnisse-5224001199004.pdf;jsessionid=A920FAE029477CBCC0CC8243734AA0B9.internet721?__blob=publicationFile (accessed on 12 March 2021).
- Bundesministerium für Gesundheit. Online-Ratgeber Pflege. Pflegedienst und Pflegesachleistungen. Available online: https://www.bundesgesundheitsministerium.de/pflegedienst-und-pflegesachleistungen.html (accessed on 16 March 2021).
- Bleses, P.; Jahns, K. Soziale Innovationen in der ambulanten Pflege. In Zusammen—Arbeit—Gestalten. Soziale Innovationen in Sozialen und Gesundheitsbezogenen Dienstleistungen; Bleses, P., Freirichs, F., Goldmann, M., Hinding, B., Schweer, M.K.W., Eds.; Springer: Wiesbaden, Germany, 2016; pp. 127–144. [Google Scholar]
- Presse- und Informationsamt der Bunderegierung. Bund-Länder-Beschluss. Kontaktbeschränkungen verlängert. Stand: 1 April 2020. Available online: https://www.bundesregierung.de/breg-de/aktuelles/kontaktsperre-verlaengert-1738528 (accessed on 15 June 2020).
- Nienhaus, A. Update: Covid-19 bei Beschäftigten im Gesundheitsdienst und in der Wohlfahrtspflege. Arb. Soz. Umweltmed. 2020, 7, 376–381. [Google Scholar]
- Statistisches Bundesamt (Destatis). Pflegestatistik—Pflege im Rahmen der Pflegeversicherung: Deutschlandergebnisse. 2017. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Gesundheit/Pflege/Publikationen/Downloads-Pflege/pflege-deutschlandergebnisse-5224001179004.pdf?__blob=publicationFile (accessed on 16 March 2021).
- Preti, E.; Di Mattei, V.; Perego, G.; Ferrari, F.; Mazzetti, M.; Taranto, P.; Di Pierro, R.; Madeddu, F.; Calati, R. The Psychological Impact of Epidemic and Pandemic Outbreaks on Healthcare Workers: Rapid Review of the Evidence. Curr. Psychiatry Rep. 2020, 22, 43. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E. The Job Demands-Resources model: State of the art. J. Manag. Psychol. 2007, 22, 309–328. [Google Scholar] [CrossRef] [Green Version]
- Demerouti, E.; Nachreiner, F. Zum Arbeitsanforderungen-Arbeitsressourcen-Modell von Burnout und Arbeitsengagement—Stand der Forschung. Z. Arb. 2019, 73, 119–130. [Google Scholar] [CrossRef] [Green Version]
- Demerouti, E. Das Arbeitsanforderungen-Arbeitsressourcen Modell von Burnout und Arbeitsengagement. In Psychische Belastung und Beanspruchung am Arbeitsplatz. Inklusive DIN EN ISO 10075-1 bis -3; Beuth Verlag GmbH: Berlin, Germany, 2012; pp. 49–57. [Google Scholar]
- Kumbruck, C.; Rumpf, M.; Senghaas-Knobloch, E. Unsichtbare Pflegearbeit: Fürsorgliche Praxis auf der Suche nach Anerkennung; Lit-Verlag: Berlin, Germany, 2010. [Google Scholar]
- Dunkel, W. Wenn Gefühle zum Arbeitsgegenstand werden. Gefühlsarbeit im Rahmen personenbezogener Dienstleistungstätigkeiten. Soziale Welt 1988, 39, 66–85. [Google Scholar]
- Böhle, F.; Stöger, U.; Weihrich, M. Interaktionsarbeit Gestalten: Vorschläge und Perspektiven für humane Dienstleistungsarbeit; Edition Sigma: Berlin, Germany, 2015. [Google Scholar]
- Fischer, U.L. “Der Bäcker backt, der Maler malt, der Pfleger …”—Soziologische Überlegungen zum Zusammenhang von Professionalität und Wertschätzung in der Kranken- und Altenpflege. Arbeit 2010, 19, 239–252. [Google Scholar] [CrossRef]
- Bleses, P.; Busse, B.; Friemer, A.; Kludig, R.; Breuer, J.; Philippi, L.; Bidmon-Berezinski, J.; Schnäpp, M. Verbundprojekt KOLEGE—Interagieren, Koordinieren und Lernen. Chancen und Herausforderungen der Digitalisierung in der Ambulanten Pflege. Zwischenbericht—Ergebnisse der Analysephase, 2nd ed.; Institut Arbeit und Wirtschaft (AWI): Bremen, Germany, 2018. [Google Scholar]
- Glaser, J.; Höge, T. Probleme und Lösungen in der Pflege aus Sicht der Arbeitsund Gesundheitswissenschaften, 1st ed.; Bundesanstalt für Arbeitsschutz und Arbeitsmedizin: Dortmund/Berlin/Dresden, Germany, 2005. [Google Scholar]
- Bundesministerium für Gesundheit. Gesundheitsförderung für Pflegekräfte: Wer pflegt die Pflege? Ausgangslage: Die Arbeitssituation in der Pflege. Prax. Pflege 2017, X.0.1, 1–4. [Google Scholar]
- Becke, G.; Behrens, M.; Bleses, P.; Jahns, K.; Pöser, S.; Ritter, W. Nachhaltige Beschäftigungsfähigkeit in der Ambulanten Pflege: Zwischenbericht des Verbundprojekts ZUKUNFT: PFLEGE. (Artec-Paper, 189); Universität Bremen, Forschungszentrum Nachhaltigkeit (artec): Bremen, Germany, 2013. [Google Scholar]
- Theobald, H.; Szebehely, M.; Preuß, M. Arbeitsbedingungen in der Altenpflege. Die Kontinuität der Berufsverläufe—Ein Deutsch-Schwedischer Vergleich; Edition Sigma: Berlin, Germany, 2013. [Google Scholar]
- Theobald, H.; Leidig, H.A. Pflegearbeit in Deutschland, Japan und Schweden. Wie werden Pflegekräfte mit Migrationshintergrund und Männer in die Pflegearbeit einbezogen? Study der Hans-Böckler-Stiftung: Düsseldorf, Germany, 2018. [Google Scholar]
- Rohwer, E.; Mojtahedzadeh, N.; Harth, V.; Mache, S. Stressoren, Stresserleben und Stressfolgen von Pflegekräften im ambulanten und stationären Setting in Deutschland. Zent. Arb. Arb. Ergon. 2021, 71, 38–43. [Google Scholar]
- Grabbe, Y.; Nolting, H.-D.; Loos, S.; Krämer, K. DAK-BGW-Gesundheitsreport 2006 Ambulante Pflege. Arbeitsbedingungen und Gesundheit in Ambulanten Pflegediensten; Berufsgenossenschaft für Gesundheitsdienst und Wohlfahrtspflege & DAK-Zentrale: Berlin, Bermany, 2006. [Google Scholar]
- Busse, B.; Bleses, P.; Kludig, R. 3.1 Arbeit und Arbeitisorganisation. In Verbundprojekt KOLEGE—Interagieren, koordinieren und lernen. Chancen und Herausforderungen der Digitalisierung in der Ambulanten Pflege. Zwischenbericht—Ergebnisse der Analysephase, 2nd ed.; Bleses, P., Busse, B., Friemer, A., Kludig, R., Breuer, J., Philippi, L., Bidmon-Berezinski, J., Philippi, L., Eds.; Institut Arbeit und Wirtschaft (AWI): Bremen, Germany, 2018. [Google Scholar]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.P.Y.; Yeung, W.S. Staff Mental Health Self-Assessment During the COVID-19 Outbreak. East Asian Arch. Psychiatry 2020, 30, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, J.Z.; Han, M.F.; Luo, T.D.; Ren, A.K.; Zhou, X.P. Mental health survey of medical staff in a tertiary infectious disease hospital for COVID-19. Chin. J. Ind. Hyg. Occup. Dis. 2020, 38, 192–195. [Google Scholar]
- Kang, L.; Ma, S.; Chen, M.; Yang, J.; Wang, Y.; Li, R.; Yao, L.; Bai, H.; Cai, Z.; Xiang Yang, B.; et al. Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: A cross-sectional study. Brain Behav. Immun. 2020, 87, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Ge, J.; Yang, M.; Feng, J.; Qiao, M.; Jiang, R.; Bi, J.; Zhan, G.; Xu, X.; Wang, L.; et al. Vicarious traumatization in the general public, members, and non-membersof medical teams aiding in COVID-19 control. Brain Behav. Immun. 2020, 88, 916–919. [Google Scholar] [CrossRef]
- Liang, Y.; Chen, M.; Zheng, X.; Liu, J. Screening for Chinese medical staff mental health by SDS and SAS during the outbreak of COVID-19. J. Psychosom. Res. 2020, 133, 110102. [Google Scholar] [CrossRef]
- Lu, W.; Wang, H.; Lin, Y.; Li, L. Psychological status of medical workforce during the COVID-19 pandemic: A cross-sectional study. Psychiatry Res. 2020, 288, 112936. [Google Scholar] [CrossRef]
- Mo, Y.; Deng, L.; Zhang, L.; Lang, Q.; Liao, C.; Wang, N.; Qin, M.; Huang, H. Work stress among Chinese nurses to support Wuhan in fighting against COVID-19 epidemic. J. Nurs. Manag. 2020, 28, 1002–1009. [Google Scholar] [CrossRef] [Green Version]
- Xiao, H.; Zhang, Y.; Kong, D.; Li, S.; Yang, N. The Effects of Social Support on Sleep Quality of Medical Staff Treating Patients with Coronavirus Disease 2019 (COVID-19) in January and February 2020 in China. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e923549. [Google Scholar]
- Sun, N.; Wei, L.; Shi, S.; Jiao, D.; Song, R.; Ma, L.; Wang, H.; Wang, C.; Wang, Z.; You, Y.; et al. A qualitative study on the psychological experience of caregivers of COVID-19 patients. Am. J. Infect. Control 2020, 48, 592–598. [Google Scholar] [CrossRef]
- Shen, X.; Zou, X.; Zhong, X.; Yan, J.; Li, L. Psychological stress of ICU nurses in the time of COVID-19. Crit. Care 2020, 24, 200. [Google Scholar] [CrossRef]
- Kim, H.; Park, K.J.; Shin, Y.W.; Lee, J.S.; Chung, S.; Lee, T.; Kim, M.J.; Jung, J.; Lee, J.; Yum, M.S.; et al. Psychological Impact of Quarantine on Caregivers at a Children’s Hospital for Contact with Case of COVID-19. J. Korean Med. Sci. 2020, 35, e255. [Google Scholar] [CrossRef]
- Dal’Bosco, E.B.; Floriano, L.S.M.; Skupien, S.V.; Arcaro, G.; Martins, A.R.; Anselmo, A.C.C. Mental health of nursing in coping with COVID-19 at a regional university hospital. Rev. Bras. Enferm. 2020, 73, e20200434. [Google Scholar] [CrossRef] [PubMed]
- Zerbini, G.; Ebigbo, A.; Reicherts, P.; Kunz, M.; Messman, H. Psychosocial burden of healthcare professionals in times of COVID-19—A survey conducted at the University Hospital Augsburg. Ger. Med. Sci. 2020, 18, Doc05. [Google Scholar] [PubMed]
- Liu, Q.; Luo, D.; Haase, J.E.; Guo, Q.; Wang, X.Q.; Liu, S.; Xia, L.; Liu, Z.; Yang, J.; Yang, B.X. The experiences of health-care providers during the COVID-19 crisis in China: A qualitative study. Lancet Glob. Health 2020, 8, e790–e798. [Google Scholar] [CrossRef]
- Paffenholz, P.; Peine, A.; Hellmich, M.; Paffenholz, S.V.; Martin, L.; Luedde, M.; Haverkamp, M.; Roderburg, C.; Marx, G.; Heidenreich, A.; et al. Perception of the 2020 SARS-CoV-2 pandemic among medical professionals in Germany: Results from a nationwide online survey. Emerg. Microbes Infect. 2020, 9, 1590–1599. [Google Scholar] [CrossRef]
- Zhang, Y.; Wei, L.; Li, H.; Pan, Y.; Wang, J.; Li, Q.; Wu, Q.; Wei, H. The Psychological Change Process of Frontline Nurses Caring for Patients with COVID-19 during Its Outbreak. Issues Ment. Health Nurs. 2020, 41, 525–530. [Google Scholar] [CrossRef]
- Liu, Z.; Wu, J.; Shi, X.; Ma, Y.; Teng, Z.; You, X.; Zhang, Y.; Zhang, W.; Feng, Z.; Long, Q.; et al. Mental Health Status of Healthcare Workers in China for COVID-19 Epidemic. Ann. Glob. Health 2020, 86, 1–8. [Google Scholar] [CrossRef]
- Bohlken, J.; Schömig, F.; Lemke, M.R.; Pumberger, M.; Riedel-Heller, S.G. COVID-19 Pandemic: Stress Experience of Healthcare Workers—A Short Current Review. Psychiatr. Praxis 2020, 47, 190–197. [Google Scholar]
- Wolf-Ostermann, K.; Schmidt, A.; Preuß, B.; Heinze, F.; Seibert, K.; Friedrich, A.-C.; Domhoff, D.; Stolle, C.; Rothgang, H. Pflege in Zeiten von Corona: Ergebnisse einer deutschlandweiten Querschnittbefragung von ambulanten Pflegediensten und teilstationären Einrichtungen. Pflege 2020, 33, 277–288. [Google Scholar] [CrossRef]
- BGW Check, Gefährdungsbeurteilung in der Pflege. In Unternehmer/-Innen PFLEGE; Berufsgenossenschaft für Gesundheitsdienst und Wohlfahrtspflege (BGW) (Ed.) Bonifatius GmbH: Paderborn, Germany, 2017. [Google Scholar]
- Gesetz über die Durchführung von Maßnahmen des Arbeitsschutzes zur Verbesserung der Sicherheit und des Gesundheitsschutzes der Beschäftigten bei der Arbeit (Arbeitsschutzgesetz—ArbSchG). Arbeitsschutzgesetz vom 7. August 1996 (BGBl. I S. 1246), das zuletzt durch Artikel 293 der Verordnung vom 19. Juni 2020 (BGBl. I S. 1328) geändert worden ist. Available online: https://www.gesetze-im-internet.de/arbschg/ (accessed on 30 March 2021).
- Kuckartz, U. Mixed Methods. Methodologie, Forschungsdesigns und Analyse-Verfahren; Springer: Wiesbaden, Germany, 2014. [Google Scholar]
- Bergmann, J.R. Qualitative Methoden der Medienforschung—Einleitung und Rahmung. In Qualitative Methoden der Medienforschung; Bergmann, J., Ayaß, R., Eds.; Verlag für Gesprächsforschung: Mannheim, Germany, 2011; pp. 13–41. [Google Scholar]
- Meyermann, A.; Gebel, T.; Liebig, S. Weitere Datentypen. Organisationsdaten. In Handbuch Methoden der Empirischen Sozialforschung; Baur, N., Blasius, J., Eds.; Springer: Wiesbaden, Germany, 2014; pp. 959–972. [Google Scholar]
- Kaiser, R. Qualitative Experteninterviews. Konzeptionelle Grundlagen und Praktische Durchführung; Springer: Siegen, Germany, 2014. [Google Scholar]
- Bortz, J.; Döring, N. Forschungsmethoden und Evaluation für Human- und Sozialwissenschaftler, 4th ed.; Springer Medizin: Würzburg, Germany, 2006. [Google Scholar]
- Helfferich, C. Die Qualität Qualitativer Daten. Manual für die Durchführung Qualitativer Interviews, 4th ed.; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2011. [Google Scholar]
- Kuckartz, U. Qualitative Inhaltsanalyse. Methoden, Praxis, Computerunterstützung, 2nd ed.; Beltz Juventa: Weinheim, Germany, 2014. [Google Scholar]
- Longhurst, R. Semi-structured Interviews and Focus Groups. In Key Methods in Geography; Clifford, N., Valentine, G., Eds.; SAGE Publications: London, UK; Thousand Oaks, CA, USA; New Delhi, India, 2003; pp. 103–115. [Google Scholar]
- Misoch, S. Qualitative Interviews; De Gruyter: Oldenburg, Germany, 2015. [Google Scholar]
- Mayring, P. Qualitative Inhaltsanalyse [Qualitative content analysis]. Forum Qual. Soc. Res. 2000, 1. [Google Scholar] [CrossRef]
- VERBI Software. MAXQDA 2020 [Computer Software]; VERBI Software: Berlin, Germany, 2019. [Google Scholar]
- Blanco-Donoso, L.M.; Moreno-Jiménez, J.; Amutio, A.; Gallego-Alberto, L.; Moreno-Jiménez, B.; Garrosa, E. Stressors, Job Resources, Fear of Contagion, and Secondary Traumatic Stress Among Nursing Home Workers in Face of the COVID-19: The Case of Spain. J. Appl. Gerontol. 2020, 40, 244–256. [Google Scholar] [CrossRef] [PubMed]
- Hennein, R.; Lowe, S. A hybrid inductive-abductive analysis of health workers’ experiences and wellbeing during the COVID-19 pandemic in the United States. PLoS ONE 2020, 15, e0240646. [Google Scholar] [CrossRef] [PubMed]
- Stolle, C.; Schmidt, A.; Domhoff, D.; Friedrich, A.C.; Heinze, F.; Preuß, B.; Seibert, K.; Rothgang, H.; Wolf-Ostermann, K. Bedarfe der Langzeitpflege in der COVID-19-Pandemie. Z. Gerontol. Geriatr. 2020, 53, 788–795. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Home Care for Patients with COVID-19 Presenting with Mild Symptoms and Management of Their Contacts. Intermin Guidance, 17 March 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Robert Koch-Institut. Nationaler Pandemieplan. Teil I. Strukturen und Maßnahmen. Available online: https://edoc.rki.de/bitstream/handle/176904/187/28Zz7BQWW2582iZMQ.pdf?sequence=1&isAllowed=y (accessed on 23 December 2020).
- Arnetz, J.E.; Goetz, C.M.; Sudan, S.; Eamonn, A.; Janisse, J.; Arnetz, B.B. Personal Protective Equipment and Mental Health Symptoms among Nurses during the COVID-19 Pandemic. J. Occup. Environ. Med. 2020, 62, 892–897. [Google Scholar] [CrossRef] [PubMed]
- Delgado, D.; Wyss Quintana, F.; Perez, G.; Sosa Liprandi, A.; Ponte-Negretti, C.; Mendoza, I.; Baranchuk, A. Personal Safety during the COVID-19 Pandemic: Realities and Perspectives of Healthcare Workers in Latin America. Int. J. Environ. Res. Public Health 2020, 17, 2798. [Google Scholar] [CrossRef] [Green Version]
- Martínez-López, J.A.; Lázaro-Pérez, C.; Gómez-Galán, J.; del Mar Fernández-Martinez, M. Psychological Impact of COVID-19 Emergency on Health Professionals: Burnout Incidence at the Most Critical Period in Spain. J. Clin. Med. 2020, 9, 3029. [Google Scholar] [CrossRef]
- Rheindorf, J.; Blocker, J.; Himmel, C.; Trost, A. Wie erleben Pflegefachpersonen die Corona-Pandemie? Pflege Z. 2020, 73, 50–53. [Google Scholar] [CrossRef]
- Martin-Delgado, J.; Viteri, E.; Mula, A.; Serpa, P.; Pacheco, G.; Prada, D.; Campos de Andrade Lourencão, D.; Campos Pavan Baptista, P.; Ramirez, G.; Mira, J.J. Availability of personal protective equipment and diagnostic and treatment facilities for healthcare workers involved in COVID-19 care: A cross-sectional study in Brazil, Colombia, and Ecuador. PLoS ONE 2020, 15, e0242185. [Google Scholar] [CrossRef]
- Wirth, T.; Ulusoy, N.; Lincke, H.-J.; Nienhaus, A.; Schablon, A. Psychosoziale Belastungen und Beanspruchungen von Beschäftigten in der stationären und ambulanten Altenpflege. Arb. Soz. Umweltmed. 2017, 52, 662–669. [Google Scholar]
- Schablon, A.; Wendeler, D.; Kozak, A.; Nienhaus, A.; Steinke, S. Prevalence and Consequences of Aggression and Violence towards Nursing and Care Staff in Germany—A Survey. Int. J. Environ. Res. Public Health 2018, 15, 1247. [Google Scholar] [CrossRef] [Green Version]
- Kricheldorff, C. Gesundheitsversorgung und Pflege für ältere Menschen in der Zukunft. Z. Gerontol. Geriatr. 2020, 53, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Eggert, S.; Teubner, C.; Budnick, A.; Gellert, P.; Kuhlmey, A. Pflegende Angehörige in der COVID-19-Krise. Ergebnisse einer Bundesweiten Befragung; Zentrum für Qualität in der Pflege (ZQP): Berlin, Germnay, 2020. [Google Scholar]
- Ramaci, T.; Barattucci, M.; Ledda, C.; Rapisarda, V. Social Stigma during COVID-19 and its Impact on HCWs Outcomes. Sustainability 2020, 12, 3834. [Google Scholar] [CrossRef]
- Hien, W.; von Schwarzkopf, H. Corona-Gefährdung im Erleben von Pflegekräften—Eine Explorative Studie mit Hinweisen auf Erweiterte Gesundheitsschutzkonzepte; Berufsgenossenschaft Gesundheitsdienst und Wohlfahrtspflege (BGW): Bremen, Germnay, 2020. [Google Scholar]
- Hower, K.I.; Pfaff, H.; Pförtner, T.K. Pflege in Zeiten von COVID-19: Onlinebefragung von Leitungskräften zu Herausforderungen, Belastungen und Bewältigungsstrategien. Pflege 2020, 33, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Der Bundesregierung, P.I. Telefonschaltkonferenz der Bundeskanzlerin mit den Regierungschefinnen und Regierungschefs der Länder am 15 April 2020. 2020. Available online: https://www.bundesregierung.de/breg-de/aktuelles/telefonschaltkonferenz-der-bundeskanzlerin-mit-den-regierungschefinnen-und-regierungschefs-der-laender-am-15-april-2020-1744228 (accessed on 30 March 2021).
- Bradtke, E.; Clauss, E.; Ernst, C.; Gregersen, S.; Huxholl, H.; Schwarzmann, K.; Taskan-Karamürsel, E.; Theiler, A. Sachgebiet Psyche und Gesundheit in der Arbeitswelt. Psychische Belastung und Beanspruchung von Beschäftigten im Gesundheitsdienst Während der Coronavirus-Pandemie; Deutsche Gesetzliche Unfallversicherung e.V. (DGUV): Berlin, Germany, 2020. [Google Scholar]
- Alizadeh, A.; Khankeh, H.R.; Barati, M.; Ahmadi, Y.; Hadian, A.; Azizi, M. Psychological distress among Iranian health-care providers exposed to coronavirus disease 2019 (COVID-19): A qualitative study. BMC Psychiatry 2020, 20, 494. [Google Scholar] [CrossRef]
- Hou, T.; Zhang, T.; Cai, W.; Song, X.; Chen, A.; Deng, G.; Ni, C. Social support and mental health among health care workers during Coronavirus Disease 2019 outbreak: A moderated mediation model. PLoS ONE 2020, 15, e0233831. [Google Scholar] [CrossRef]
- Zhao, F.; Ahmed, F.; Faraz, N.A. Caring for the caregiver during COVID-19 outbreak: Does inclusive leadership improve psychological safety and curb psychological distress? A cross-sectional study. Int. J. Nurs. Stud. 2020, 110, 103725. [Google Scholar] [CrossRef]
- Lauxen, O.; Schmidt, A.; Bodemann, S. Bei Anruf Pflege. Potenziale der Technik in der ambulanten Pflege. Pflege 2020, 9, 48–51. [Google Scholar] [CrossRef]
- Chew, N.W.S.; Lee, G.K.H.; Tan, B.Y.Q.; Jing, M.; Goh, Y.; Ngiam, N.J.H.; Yeo, L.L.L.; Ahmad, A.; Ahmed Khan, F.; Napolean Shanmugam, G.; et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav. Immun. 2020, 88, 559–565. [Google Scholar] [CrossRef]
- Rothgang, H.; Domhoff, D.; Friedrich, A.-C.; Franziska, H.; Benedikt, P.; Schmidt, A.; Kathrin, S.; Stolle, C.; Wolf-Ostermann, K. Pflege in Zeiten von Corona: Zentrale Ergebnisse einer deutschlandweiten Querschnittsbefragung vollstationärer Pflegeheime. Pflege 2020, 33, 265–275. [Google Scholar] [CrossRef]
- Zhan, Y.; Ma, S.; Jian, X.; Cao, Y.; Zhan, X. The Current Situation and Influencing Factors of Job Stress Among Frontline Nurses Assisting in Wuhan in Fighting COVID-19. Front. Public Health 2020, 8, 579866. [Google Scholar] [CrossRef]
- Burisch, M. Das Burnout-Syndrom. Theorie der Inneren Erschöpfung—Zahlreiche Fallbeispiele—Hilfen zur Selbsthilfe, 5th ed.; Springer: Berlin, Germany, 2014. [Google Scholar]
- Van Nes, F.; Abma, T.; Johnsson, H.; Deeg, D. Language differences in qualitative research: Is meaning lost in translation? Eur. J. Ageing 2010, 7, 313–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bundesministerium für Gesundheit. Pflegekräfte. Beschäftigte in der Pflege. Available online: https://www.bundesgesundheitsministerium.de/themen/pflege/pflegekraefte/beschaeftigte.html (accessed on 14 August 2020).
- Scholl, A. Die Befragung, 3rd ed.; UVK Verlagsgesell-Schaft mbH: Munich, Germany, 2015. [Google Scholar]
- Opdenakker, R.J.G. Advantages and Disadvantages of Four Interview Techniques in Qualitative Research. Forum Qual. Soc. Res. 2006, 7. [Google Scholar] [CrossRef]
- Novick, G. Is there a bias against telephone interviews in qualitative research? Res. Nurs. Health 2008, 31, 391–398. [Google Scholar] [CrossRef] [Green Version]
- Guest, G.; Bunce, A.; Johnson, L. How many interviews are enough? An experiment with data saturation and variability. Field Methods 2006, 18, 59–82. [Google Scholar] [CrossRef]
- Fischer, B.; Geyer, J. Pflege in Corona-Zeiten: Gefährdete Pflegen Besonders Gefährdete. DIW aktuell, No. 38; Deutsches Institut für Wirtschaftsforschung (DIW): Berlin, Germany, 2020. [Google Scholar]
- Brandenburg, U.; Nieder, P. Betriebliches Fehlzeiten-Management. Instrumente und Praxisbeispiele für erfolgreiches Anwesenheits- und Vertrauensmanagement, 2nd ed.; Gabler: Wiesbaden, Germany, 2009. [Google Scholar]
- Badura, B.; Hehlmann, T. Gesundheit, Verhalten, Organisation. In Betriebliche Gesundheitspolitik. Der Weg zur Gesunden Organisation; Badura, B., Hehlmann, T., Eds.; Springer: Berlin/Heidelberg, Germany, 2003; pp. 13–58. [Google Scholar]
- Riedel-Heller, S.G.; Luppa, M.; Seidler, A.; Becker, T.; Stengler, K. Psychische Gesundheit und Arbeit. Konzepte, Evidenz und Implikationen für Forschung und Praxis. Der Nervenarzt 2013, 84, 832–837. [Google Scholar] [CrossRef] [PubMed]
- Pflegepolitik in 5 Minuten, Corona-Schnelltests. Mehr Sicherheit in Pflegeeinrichtungen. Heilberufe 2020, 72, 6–10.
- Richter, P.; Wegge, J. Occupational Health Psychology—Gegenstand, Modelle, Aufgaben. In Klinische Psychologie & Psychotherapie—Ein Lehrbuch, 2nd ed.; Wittchen, H.-U., Hoyer, J., Eds.; Springer: Berlin, Germany, 2011; pp. 337–357. [Google Scholar]
- Badura, B.; Greiner, W.; Rixgens, P.; Ueberle, M.; Behr, M. Sozialkapital—Grundlagen von Gesundheit und Unternehmenserfolg, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Meißner, T. Im Hotspot: Corona und die ambulante Pflege. Pflege 2020, 12, 17–19. [Google Scholar] [CrossRef]


{kind=link}
| Phase of the Interview | Contents |
|---|---|
| 1 Information phase | Introduction: Study information, confidentiality, informed consent |
| 2 Warm-up phase | Qualifications, working activity |
| 3 Main phase | Work-related job demands, emotional demands, effects on personal life Resources in work life Strain reactions |
| 4 Final phase and end of the interview | Socio-demographics of the interviewees and farewell |
| ID | Gender 1 | Age | Children in Household | Date of Interview (MM/DD/YY) | Qualification | Occupation | Work Experience as an Outpatient Caregiver | Work Schedule |
|---|---|---|---|---|---|---|---|---|
| 1 | f | 31 | 1 | 05/07/2020 | Caregiver | Outpatient geriatric nurse | 7 months | Full-time |
| 2 | f | 31 | 0 | 05/07/2020 | Geriatric nurse | Outpatient geriatric nurse | 9 years | Full-time |
| 3 | f | 33 | 1 | 05/07/2020 | Geriatric nurse | Outpatient geriatric nurse | 7 months | Full-time |
| 4 | m | 64 | 0 | 05/08/2020 | Geriatric nurse | Outpatient geriatric nurse | 36 years | Full-time |
| 5 | f | 21 | 0 | 05/12/2020 | Home and family care | Outpatient home and family caregiver | 1 year | Full-time |
| 6 | m | 51 | 0 | 05/12/2020 | Geriatric nurse | Outpatient geriatric nurse | 5 years | Full-time |
| 7 | m | 25 | 1 | 05/15/2020 | Geriatric nurse | Outpatient geriatric nurse | 1.5 years | Full-time |
| 8 | f | 38 | 3 | 05/15/2020 | Healthcare and nursing staff | Outpatient caregiver | 16 years | Full-time |
| 9 | f | 51 | 0 | 05/19/2020 | Geriatric nurse | Outpatient geriatric nurse and office manager in health sector | 23 years | Full-time |
| 10 | f | 36 | 0 | 06/03/2020 | Social manager | Outpatient caregiver | 4 years | Full-time |
| 11 | f | 46 | 1 | 06/11/2020 | Geriatric nurse, additional qualification intensive and palliative care | Outpatient geriatric nurse | 20 years | Full-time |
| 12 | f | 50 | 2 | 06/11/2020 | Wound expert | Care specialist and nutrition manager in the outpatient care | 10 years | Full-time |
| 13 | f | 34 | 0 | 06/15/2020 | Geriatric nurse | Care specialist and deputy care management in the outpatient care | 5 years | Full-time |
| 14 | f | 67 | 0 | 06/19/2020 | Geriatric nurse | Outpatient geriatric nurse | 24 years | Part-time |
| 15 | f | 37 | 0 | 06/29/2020 | Geriatric nurse and wound expert | Outpatient geriatric nurse and wound expert | 5.5 years | Part-time |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mojtahedzadeh, N.; Wirth, T.; Nienhaus, A.; Harth, V.; Mache, S. Job Demands, Resources and Strains of Outpatient Caregivers during the COVID-19 Pandemic in Germany: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 3684. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073684
Mojtahedzadeh N, Wirth T, Nienhaus A, Harth V, Mache S. Job Demands, Resources and Strains of Outpatient Caregivers during the COVID-19 Pandemic in Germany: A Qualitative Study. International Journal of Environmental Research and Public Health. 2021; 18(7):3684. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073684
Chicago/Turabian StyleMojtahedzadeh, Natascha, Tanja Wirth, Albert Nienhaus, Volker Harth, and Stefanie Mache. 2021. "Job Demands, Resources and Strains of Outpatient Caregivers during the COVID-19 Pandemic in Germany: A Qualitative Study" International Journal of Environmental Research and Public Health 18, no. 7: 3684. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073684