
The Impact of Dietary Knowledge on Health: Evidence from the China Health and Nutrition Survey


Abstract
:1. Introduction
2. Literature Review
3. Data, Variables and Model
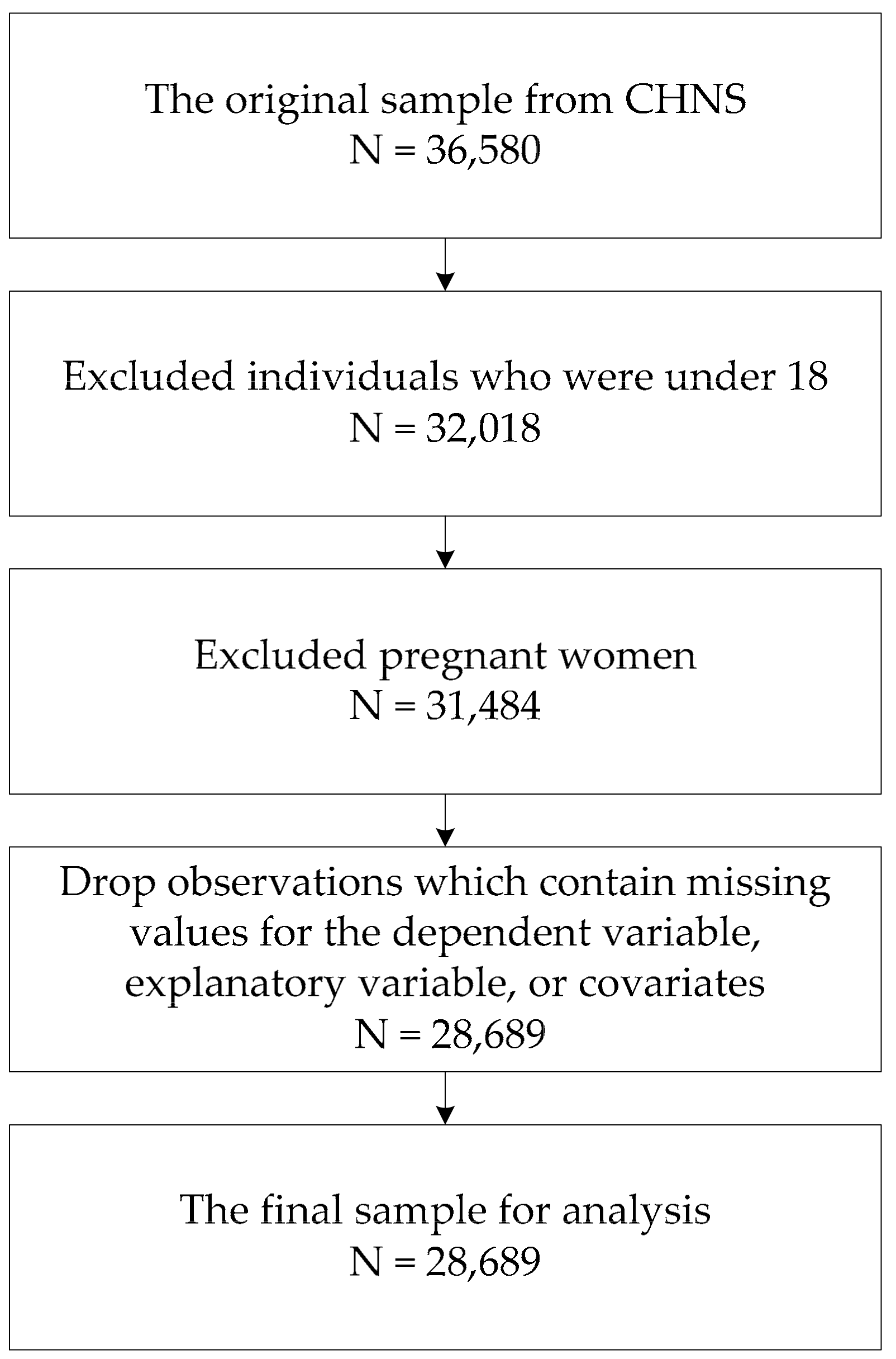
3.1. Data
3.2. Variables
3.2.1. Dependent Variable
3.2.2. Core Explanatory Variable of Interest
3.2.3. Covariates
3.3. Model
4. Results
4.1. The Impact of Dietary Knowledge on Health Status
4.2. The Impact of Spouse’s Dietary Knowledge on Individual Health Status
4.3. Heterogeneity Analysis
4.4. Robustness Check
4.4.1. Changing the Measurement of Dietary Knowledge
4.4.2. Changing the Sample
4.4.3. Changing the Model Specification
5. Conclusions
6. Policy Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


{kind=link}
| Do you Strongly Agree, Somewhat Agree, Somewhat Disagree or Strongly Disagree with This Statement? 1. Strongly Disagree; 2. Disagree; 3. Neutral; 4. Agree; 5. Strongly Agree; 9. Unknown * Please Note That the Question is not Asking about Your Actual Habits | True/False |
|---|---|
| Statement | |
| Choosing a diet with a lot of fresh fruits and vegetables is good for one’s health. | T |
| Eating a lot of sugar is good for one’s health. | F |
| Eating a variety of foods is good for one’s health. | T |
| Choosing a diet high in fat is good for one’s health. | F |
| Choosing a diet with a lot of staple foods [rice and rice products and wheat and wheat products is not good for one’s health. | T |
| Consuming a lot of animal products daily (fish, poultry, eggs and lean meat) is good for one’s health. | F |
| Reducing the amount of fatty meat and animal fat in the diet is good for one’s health. | T |
| Consuming milk and dairy products is good for one’s health. | T |
| Consuming beans and bean products is good for one’s health. | T |
| Physical activities are good for one’s health. | T |
| Sweaty sports or other intense physical activities are not good for one’s health. | T |
| The heavier one’s body is, the healthier he or she is. | F |
| Variables | Part A | Part B | ||||
|---|---|---|---|---|---|---|
| Baseline Model | Marginal Effect | Baseline Model | Marginal Effect | |||
| (i) | (ii) | (iii) | (iv) | (v) | (vi) | |
| diet_knowledge | 0.133 *** | 0.129 *** | 0.028 *** | 0.117 *** | 0.114 *** | 0.025 *** |
| (0.0218) | (0.0131) | (0.0029) | (0.0324) | (0.0186) | (0.0041) | |
| diet_knowledge_sp | −0.074 * | 0.007 | 0.002 | |||
| (0.0337) | (0.0184) | (0.0041) | ||||
| Constant | 3.017 *** | 0.860 *** | 3.269 *** | 0.983 *** | ||
| (0.2959) | (0.1495) | (0.3369) | (0.1690) | |||
| Covariates | Yes | Yes | Yes | Yes | ||
| Province—Fixed Effect | Yes | Yes | Yes | Yes | ||
| Year—Fixed Effect | Yes | Yes | Yes | Yes | ||
| Pseudo R2 | 0.071 | 0.064 | ||||
| Log pseudolikelihood | −23,284.101 | −18,038.650 | ||||
| Observations | 28,749 | 28,749 | 22,216 | 22,216 | ||
| Variables | Part A | Part B | ||||
|---|---|---|---|---|---|---|
| Baseline Model | Marginal Effect | Baseline Model | Marginal Effect | |||
| (i) | (ii) | (iii) | (iv) | (v) | (vi) | |
| diet_knowledge | 0.126 *** | 0.111 *** | 0.024 *** | 0.077 | 0.074 *** | 0.016 *** |
| (0.0282) | (0.0141) | (0.0030) | (0.0403) | (0.0193) | (0.0042) | |
| diet_knowledge_sp | −0.025 | 0.039 * | 0.008 * | |||
| (0.0403) | (0.0192) | (0.0042) | ||||
| Constant | 2.454 *** | 0.630 *** | 2.743 *** | 0.802 *** | ||
| (0.3725) | (0.1641) | (0.4190) | (0.1861) | |||
| Covariates | Yes | Yes | Yes | Yes | ||
| Province—Fixed Effect | Yes | Yes | Yes | Yes | ||
| Year—Fixed Effect | Yes | Yes | Yes | Yes | ||
| Pseudo R2 | 0.069 | 0.064 | ||||
| Log pseudolikelihood | −19,053.292 | −14,625.540 | ||||
| Observations | 24,809 | 24,809 | 19,023 | 19,023 | ||
| Variables | Baseline Model | Marginal Effect | |||
|---|---|---|---|---|---|
| health_self = 1 Bad | health_self = 2 Fair | health_self = 3 Good | |||
| (i) | (ii) | (iii) | (iv) | (v) | |
| diet_knowledge | 0.114 *** | 0.102 *** | −0.007 *** | −0.015 *** | 0.022 *** |
| (0.0233) | (0.0131) | (0.0014) | (0.0028) | (0.0029) | |
| gender | 0.157 *** | 0.210 *** | −0.010 *** | −0.037 *** | 0.046 *** |
| (0.0493) | (0.0258) | (0.0031) | (0.0056) | (0.0056) | |
| ethnic | −0.079 | 0.165 *** | 0.005 | −0.041 *** | 0.036 *** |
| (0.0875) | (0.0460) | (0.0054) | (0.0102) | (0.0101) | |
| age | −0.040 *** | −0.033 *** | 0.002 *** | 0.005 *** | −0.007 *** |
| (0.0018) | (0.0010) | (0.0001) | (0.0002) | (0.0002) | |
| married | 0.095 | 0.017 | −0.006 | 0.002 | 0.004 |
| (0.0641) | (0.0374) | (0.0040) | (0.0081) | (0.0082) | |
| education | |||||
| Lower middle school degree and below | 0.358 *** | 0.261 *** | −0.025 *** | −0.034 *** | 0.059 *** |
| (0.0686) | (0.0420) | (0.0053) | (0.0095) | (0.0096) | |
| Upper middle school degree or vocational degree | 0.615 *** | 0.420 *** | −0.040 *** | −0.055 *** | 0.094 *** |
| (0.0914) | (0.0493) | (0.0060) | (0.0110) | (0.0112) | |
| University degree or higher | 0.732 *** | 0.481 *** | −0.045 *** | −0.062 *** | 0.108 *** |
| (0.1399) | (0.0653) | (0.0077) | (0.0144) | (0.0145) | |
| lnper_income | 0.175 *** | 0.123 *** | −0.011 *** | −0.016 *** | 0.027 *** |
| (0.0217) | (0.0126) | (0.0014) | (0.0027) | (0.0028) | |
| city | −0.083 | −0.136 *** | 0.005 | 0.025 *** | −0.030 *** |
| (0.0523) | (0.0278) | (0.0032) | (0.0061) | (0.0061) | |
| Constant | 3.191 *** | 0.878 *** | |||
| (0.2961) | (0.1498) | ||||
| Province—Fixed Effect | Yes | Yes | |||
| Year—Fixed Effect | Yes | Yes | |||
| Pseudo R2 | 0.069 | ||||
| Log pseudolikelihood | −23,302.611 | ||||
| Observations | 28,689 | 28,689 | |||
References
- Xu, X.; Hall, J.; Byles, J.; Shi, Z. Dietary pattern is associated with obesity in older people in China: Data from China Health and Nutrition Survey (CHNS). Nutrients 2015, 7, 8170–8188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, X.; Pan, J. The Medical Cost Attributable to Obesity and Overweight in China: Estimation Based on Longitudinal Surveys. Health Econ. 2016, 25, 1291–1311. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Li, F.; Harmer, P. Healthy China 2030: Moving from blueprint to action with a new focus on public health. Correspondence 2019, 4, e447. [Google Scholar] [CrossRef] [Green Version]
- Asakura, K.; Todoriki, H.; Sasaki, S. Relationship between nutrition knowledge and dietary intake among primary school children in Japan: Combined effect of children’s and their guardians’ knowledge. J. Epidemiol. 2017, 27, 483–491. [Google Scholar] [CrossRef]
- Clement, M.; Bonnefond, C. Does social class affect nutrition knowledge and food preferences among Chinese urban adults? Camb. J.China Stud. 2015, 10, 20–37. [Google Scholar]
- Kwol, V.S.; Eluwole, K.K.; Avci, T.; Lasisi, T.T. Another look into the Knowledge Attitude Practice (KAP) model for food control: An investigation of the mediating role of food handlers’ attitudes. Food Control. 2020, 110. [Google Scholar] [CrossRef]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef] [Green Version]
- De Vriendt, T.; Matthys, C.; Verbeke, W.; Pynaert, I.; De Henauw, S. Determinants of nutrition knowledge in young and middle-aged Belgian women and the association with their dietary behavior. Appetite 2009, 52, 788–792. [Google Scholar] [CrossRef]
- Reinehr, T.; Kersting, M.; Chahda, C.; Andler, W. Nutritional knowledge of obese compared to non-obese children. Nutr. Res. 2003, 23, 645–649. [Google Scholar] [CrossRef]
- Dallongeville, J.; Mare’caux, N.; Cottel, D.; Bingham, A.; Amouyel, P. Association between nutrition knowledge and nutritional intake in middle-aged men from Northern France. Public Health Nutr. 2001, 4, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; He, D.; Wei, L.; Wang, S.; Mao, Z. Association between diet-related knowledge, attitudes, behaviors, and self-rated health in Chinese adult residents: A population-based study. BMC Public Health. 2020, 20, 720. [Google Scholar] [CrossRef]
- Cruwys, T.; Bevelander, K.E.; Hermans, R.C.J. Social Modeling of eating: A review of when and why social influence affects food intake and choice. Appetite 2015, 86, 3–18. [Google Scholar] [CrossRef]
- Clark, A.E.; Etile, F. Don’t give up on me baby: Spousal correlation in smoking behaviour. J. Health Econ. 2006, 25, 958–978. [Google Scholar] [CrossRef] [Green Version]
- Cobb, L.K.; McAdams-DeMarco, A.M.; Huxley, R.R.; Woodward, M.; Koton, S.; Coresh, J.; Anderson, C.A. The association of spousal smoking status with the ability to quit smoking: The Atherosclerosis Risk in Communities Study. Am. J. Epidemiol. 2014, 179, 1182–1187. [Google Scholar] [CrossRef] [Green Version]
- Falba, T.A.; Sindelar, J.L. Spousal Concordance in Health Behavior Change. Health Serv. Res. 2008, 43, 96–116. [Google Scholar] [CrossRef] [Green Version]
- Meyler, D.; Stimpson, J.P.; Peek, K.M. Health concordance within couples: A systematic review. Soc. Sci. Med. 2007, 64, 2297–2310. [Google Scholar] [CrossRef]
- Popkin, B.M.; Hawkes, C. Sweetening of the global diet, particularly beverages: Patterns, trends, and policy responses. Lancet Diabetes Endocrinol. 2016, 4, 174–186. [Google Scholar] [CrossRef] [Green Version]
- Ni, G.; Zheng, F. An analysis of western fast food’s impact on Children’s health. China Soft Sci. 2012, 6, 73–82. (In Chinese) [Google Scholar]
- Wang, X.; Yang, X.; Li, J.; Liu, F.; Chen, J.; Liu, X.; Cao, J.; Shen, C.; Yu, L.; Lu, F.; et al. Impact of healthy lifestyles on cancer risk in the Chinese population. Cancer 2019. [Google Scholar] [CrossRef]
- Cavaliere, A.; Siletti, E.; Banterle, A. Nutrition information, Mediterranean diet, and weight: A structural equation approach. Agric. Econ. 2020, 66, 10–18. [Google Scholar] [CrossRef]
- Bonaccio, M.; Di Castelnuovo, A.; Costanzo, S.; De Lucia, F.; Olivieri, M.; Donati, M.B.; Bonanni, A. Nutrition knowledge is associated with higher adherence to Mediterranean diet and lower prevalence of obesity. Results from the Moli-sani study. Appetite 2013, 68, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, H.; Chen, Y.; Yu, P.; Tseng, J.T.; Kuo, S.; Hu, Y.H.; Ko, Y.; Chi, I.; Wu, S. Health Awareness, Attitudes, and Behaviors Among Young-Adult Tutors in the Intergenerational Mobile Technology Opportunities Program in Taiwan. J. Soc. Soc. Work Res. 2020. [Google Scholar] [CrossRef]
- Kunitomo, M.; Ekuni, D.; Mizutani, S.; Tomofuji, T.; Irie, K.; Azuma, T.; Morita, M. Association between Knowledge about Comprehensive Food Education and Increase in Dental Caries in Japanese University Students: A Prospective Cohort Study. Nutrients 2016, 8, 114. [Google Scholar] [CrossRef] [Green Version]
- Spillmann, D.M.; Siegrist, M. Consumers’ knowledge of healthy diets and its correlation with dietary behaviour. J. Hum. Nutr. Diet 2010, 24, 54–60. [Google Scholar] [CrossRef]
- Petrovici, D.A.; Ritson, C. Factors influencing consumer dietary health preventative behaviours. BMC Public Health 2006, 6, 222. [Google Scholar] [CrossRef] [Green Version]
- Lusk, J.L.; Schroeter, C. Economic factors and body weight: An empirical analysis. J. Agric. Appl. Econ. 2008, 40, 523–538. [Google Scholar] [CrossRef] [Green Version]
- Zhou, L.; Zeng, Q.; Jin, S.; Cheng, G. The impact of changes in dietary knowledge on adult overweight and obesity in China. PLoS ONE 2017, 12, e0179551. [Google Scholar] [CrossRef] [Green Version]
- Brien, G.; Davies, M. Nutrition knowledge and body mass index. Health Educ. Res. 2006, 22, 571–575. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Han, X.; Wen, H.; Ren, J.; Qi, L. Better Dietary Knowledge and Socioeconomic Status (SES), Better Body Mass Index? Evidence from China-An Unconditional Quantile Regression Approach. Nutrients 2020, 12, 1197. [Google Scholar] [CrossRef]
- Sekabira, H.; Qaim, M. Can mobile phones improve gender equality and nutrition? Panel data evidence from farm households in Uganda. Food Policy 2017, 73, 95–103. [Google Scholar] [CrossRef]
- Ren, Y.; Li, H.; Wang, X. Family income and nutrition-related health: Evidence from food consumption in China. Soc. Sci. Med. 2019. [Google Scholar] [CrossRef]
- Mader, S.; Rubach, M.; Schaecke, W.; Röger, C.; Feldhoffer, I.; Thalmeier, E. Healthy nutrition in Germany: A survey analysis of social causes, obesity and socioeconomic status. Public Health Nutr. 2020, 23, 2109–2123. [Google Scholar] [CrossRef]
- Houldcroft, L.; Haycraft, E.; Farrow, C. Peer and friend influences on children’s eating. Soc. Dev. 2014, 23, 19–40. [Google Scholar] [CrossRef] [Green Version]
- Yakusheva, O.; Kapinos, K.A.; Eisenberg, D. Estimating heterogeneous and hierarchical peer effects on body weight using roommate assignments as a natural experiment. J. Hum. Resour. 2014, 49, 234–261. [Google Scholar] [CrossRef]
- Clark, A.E.; Etile, F. Happy house: Spousal weight and individual well-being. J. Health Econ. 2011, 30, 1124–1136. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, J.; Marksteiner, R. Causal spousal health spillover effects and implications for program evaluation. Am. Econ. J. Econ. Policy 2017, 9, 144–166. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, H.; Wang, Y.; Xue, H.; Wang, Z.; Du, W.; Zhang, B. Dietary patterns and their associations with childhood obesity in China. Br. J. Nutr. 2015, 113, 1978–1984. [Google Scholar] [CrossRef] [Green Version]
- Mossey, J.M.; Shapiro, E. Self-Rated Health: A Predictor of Mortality Among the Elderly. Am. J. Public Health 1982, 72, 800–808. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J. The impact of water quality on health: Evidence from the drinking water infrastructure program in rural China. J. Health Econ. 2012, 31, 122–134. [Google Scholar] [CrossRef]
- Chen, L.; Li, Y. Research on the Path of the Influence of Internet Use on Residents’ Health. Res. Financ. Econ. Issues 2020, 7, 86–93. (In Chinese) [Google Scholar] [CrossRef]
- Yang, K.; He, H. The Impact of Internet Usage on Health of Residents: A Study from the China Labor-force Dynamic Survey 2016. Nankai Econ. Stud. 2020, 3, 182–203. (In Chinese) [Google Scholar] [CrossRef]
- Min, S.; Wang, X.; Yu, X. Does dietary knowledge affect household food waste in the developing economy of China? Food Policy 2020. [Google Scholar] [CrossRef]
- Shimokawa, S. When does dietary knowledge matter to obesity and overweight prevention? Food Policy 2013, 38, 35–46. [Google Scholar] [CrossRef]
- World Health Organization. Development of Food-Based Dietary Guidelines for the Asian Region. 1998. Available online: http://www.who.int/nutrition/publications/nutrientrequirements/dietguide_searo/en/ (accessed on 10 December 2020).
- Mokdad, A.; Marks, J.; Stroup, D.; Gerberding, J. Actual Causes of Death in the United States. J. Am. Med Assoc. 2004, 291, 1238–1245. [Google Scholar] [CrossRef]
- Lei, X.; Yin, N.; Zhao, Y. Socioeconomic status and chronic diseases: The case of hypertension in China. China Econ. Rev. 2012, 20, 105–121. [Google Scholar] [CrossRef]
- GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar]
- Li, M.; Du, W. Effects of Air Pollution on Residents′Health and Group Differences: An Empirical Analysis Based on CFPS (2012) Micro-Survey Data. Econ. Rev. 2018, 3, 142–154. (In Chinese) [Google Scholar] [CrossRef]
- Hajek, A.; Bock, J.O.; Weyerer, S.; König, H.H. Correlates of alcohol consumption among Germans in the second half of life. Results of a population-based observational study. BMC Geriatr. 2017, 17, 207. [Google Scholar] [CrossRef] [Green Version]
- Cheng, L.; Zhang, Y.; Shen, K. Understanding the Pathways of the Education-Health Gradient: Evidence from the Chinese elderly. China Econ. Q. 2015, 14, 305–330. (In Chinese) [Google Scholar] [CrossRef]
- Albanese, A.M.; Huffman, J.C.; Celano, C.M.; Malloy, L.M.; Wexler, D.J.; Freedman, M.E.; Millstein, R.A. The role of spousal support for dietary adherence among type 2 diabetes patients: A narrative review. Soc. Work Health Care 2019, 58, 304–323. [Google Scholar] [CrossRef]
- Wang, Q.; Rizzo, J.; Fang, H. Changes in Smoking Behaviors following Exposure to Health Shocks in China. Int. J. Environ. Res. Public Health 2018, 15, 2905. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Cooney, R.S. Son preference and the one child policy in China: 1979–1988. Popul. Res. Policy Rev. 1993, 12, 277–296. [Google Scholar] [CrossRef]
- MacPhail, F. Gender Equality and the Labor Market: Women, Work, and Migration in the People’s Republic of China. 2017. Available online: http://www.voced.edu.au/content/ngv%3A77487 (accessed on 10 December 2020).
- Bahmani, M.; Aryamanesh, S.; Bahmani, M.; Gholami, S. Equity and Marital Satisfaction in Iranian Employed and Unemployed Women. Procedia. Soc. Behav. Sci. 2013, 84, 421–425. [Google Scholar] [CrossRef] [Green Version]
- Xu, Y.; Zhu, S.; Zhang, T.; Wang, D.; Hu, J.; Gao, J.; Zhou, Z. Explaining Income-Related Inequalities in Dietary Knowledge: Evidence from the China Health and Nutrition Survey. Int. J. Environ. Res. Public Health 2020, 17, 532. [Google Scholar] [CrossRef] [Green Version]
- Xie, S.; Mo, T. The impact of education on health in China. China Econ. Rev. 2014, 29, 1–18. [Google Scholar] [CrossRef]
- Zhao, M.; Konishi, Y.; Glewwe, P. Does information on health status lead to a healthier lifestyle? Evidence from China on the effect of hypertension diagnosis on food consumption. J. Health Econ. 2013, 32, 367–385. [Google Scholar] [CrossRef]
| Variables | Definition | N | Mean | SD | Min | Max |
|---|---|---|---|---|---|---|
| health_self | 1—Bad; 2—Fair; 3—Good | 28,689 | 2.506 | 0.626 | 1 | 3 |
| diet_knowledge | Summation of the scores for 12 statements in the questionnaire | 28,689 | 31.29 | 3.252 | 17 | 36 |
| gender | 1 = Male; 0 = Female | 28,689 | 0.489 | 0.500 | 0 | 1 |
| ethnic | 1 = Han; 0 = Other ethnic | 28,689 | 0.886 | 0.318 | 0 | 1 |
| age | Age of the person | 28,689 | 48.95 | 15.12 | 18 | 97 |
| married | 1 = Yes; 0 = No | 28,689 | 0.850 | 0.357 | 0 | 1 |
| smoking | 1 = Yes; 0 = No | 28,689 | 0.272 | 0.445 | 0 | 1 |
| alcohol | 1 = Yes; 0 = No | 28,689 | 0.317 | 0.465 | 0 | 1 |
| education | ||||||
| Illiteracy | 1 = Yes; 0 = No | 28,689 | 0.149 | 0.356 | 0 | 1 |
| Lower middle school degree and below | 1 = Yes; 0 = No | 28,689 | 0.532 | 0.499 | 0 | 1 |
| Upper middle school degree or vocational degree | 1 = Yes; 0 = No | 28,689 | 0.228 | 0.420 | 0 | 1 |
| University degree or higher | 1 = Yes; 0 = No | 28,689 | 0.091 | 0.287 | 0 | 1 |
| lnper_income | Per capita annual household income inflated to 2015, CNY, in logarithm | 28,689 | 8.982 | 1.197 | 0.594 | 13.94 |
| city | 1 = Urban; 0 = Rural | 28,689 | 0.372 | 0.483 | 0 | 1 |
| Variables | Baseline Model | Marginal Effect | |||
|---|---|---|---|---|---|
| health_self = 1 Bad | health_self = 2 Fair | health_self = 3 Good | |||
| (i) | (ii) | (iii) | (iv) | (v) | |
| diet_knowledge | 0.114 *** | 0.102 *** | −0.007 *** | −0.015 *** | 0.022 *** |
| (0.0233) | (0.0131) | (0.0014) | (0.0028) | (0.0029) | |
| gender | −0.108 | 0.095 ** | 0.007 | −0.028 *** | 0.021 ** |
| (0.0594) | (0.0334) | (0.0037) | (0.0072) | (0.0073) | |
| ethnic | −0.066 | 0.173 *** | 0.004 | −0.042 *** | 0.038 *** |
| (0.0873) | (0.0460) | (0.0054) | (0.0102) | (0.0101) | |
| age | −0.038 *** | −0.033 *** | 0.002 *** | 0.005 *** | −0.007 *** |
| (0.0018) | (0.0010) | (0.0001) | (0.0002) | (0.0002) | |
| married | 0.086 | 0.006 | −0.005 | 0.004 | 0.001 |
| (0.0639) | (0.0374) | (0.0039) | (0.0080) | (0.0082) | |
| smoking | 0.115 | 0.069 * | −0.007 | −0.008 | 0.015 * |
| (0.0676) | (0.0353) | (0.0042) | (0.0077) | (0.0078) | |
| alcohol | 0.510 *** | 0.164 *** | −0.032 *** | −0.004 | 0.036 *** |
| (0.0670) | (0.0333) | (0.0042) | (0.0073) | (0.0073) | |
| education | |||||
| Lower middle school degree and below | 0.374 *** | 0.265 *** | −0.027 *** | −0.034 *** | 0.060 *** |
| (0.0685) | (0.0420) | (0.0053) | (0.0095) | (0.0096) | |
| Upper middle school degree or vocational degree | 0.626 *** | 0.424 *** | −0.041 *** | −0.055 *** | 0.095 *** |
| (0.0913) | (0.0493) | (0.0060) | (0.0110) | (0.0112) | |
| University degree or higher | 0.766 *** | 0.494 *** | −0.047 *** | −0.063 *** | 0.110 *** |
| (0.1402) | (0.0655) | (0.0076) | (0.0144) | (0.0146) | |
| lnper_income | 0.176 *** | 0.123 *** | −0.011 *** | −0.016 *** | 0.027 *** |
| (0.0218) | (0.0126) | (0.0014) | (0.0027) | (0.0028) | |
| city | −0.090 | −0.140 *** | 0.006 | 0.025 *** | −0.031 *** |
| (0.0524) | (0.0279) | (0.0032) | (0.0061) | (0.0061) | |
| Constant | 3.028 *** | 0.848 *** | |||
| (0.2964) | (0.1499) | ||||
| Province—Fixed Effect | Yes | Yes | |||
| Year—Fixed Effect | Yes | Yes | |||
| Pseudo R2 | 0.071 | ||||
| Log pseudolikelihood | –23,259.046 | ||||
| Observations | 28,689 | 28,689 | |||
| Variables | Baseline Model | Marginal Effect | |||
|---|---|---|---|---|---|
| health_self = 1 Bad | health_self = 2 Fair | health_self = 3 Good | |||
| (i) | (ii) | (iii) | (iv) | (v) | |
| diet_knowledge | 0.074 * | 0.074 *** | −0.004 * | −0.012 ** | 0.017 *** |
| (0.0328) | (0.0177) | (0.0020) | (0.0039) | (0.0039) | |
| diet_knowledge_sp | −0.034 | 0.023 | 0.002 | −0.007 | 0.005 |
| (0.0328) | (0.0176) | (0.0020) | (0.0039) | (0.0039) | |
| gender | −0.057 | 0.106 ** | 0.003 | −0.027 *** | 0.024 ** |
| (0.0691) | (0.0385) | (0.0042) | (0.0083) | (0.0085) | |
| ethnic | −0.064 | 0.154 ** | 0.004 | −0.038 *** | 0.034 ** |
| (0.1025) | (0.0526) | (0.0062) | (0.0117) | (0.0117) | |
| age | −0.043 *** | −0.036 *** | 0.003 *** | 0.005 *** | −0.008 *** |
| (0.0023) | (0.0012) | (0.0001) | (0.0003) | (0.0003) | |
| smoking | 0.128 | 0.070 | −0.008 | −0.008 | 0.015 |
| (0.0769) | (0.0395) | (0.0046) | (0.0087) | (0.0088) | |
| alcohol | 0.502 *** | 0.177 *** | −0.030 *** | −0.009 | 0.039 *** |
| (0.0752) | (0.0374) | (0.0046) | (0.0083) | (0.0083) | |
| education | |||||
| Lower middle school degree and below | 0.382 *** | 0.283 *** | −0.027 *** | −0.038 *** | 0.065 *** |
| (0.0788) | (0.0481) | (0.0060) | (0.0109) | (0.0111) | |
| Upper middle school degree or vocational degree | 0.597 *** | 0.458 *** | −0.038 *** | −0.065 *** | 0.104 *** |
| (0.1029) | (0.0559) | (0.0068) | (0.0126) | (0.0128) | |
| University degree or higher | 0.700 *** | 0.485 *** | −0.043 *** | −0.066 *** | 0.109 *** |
| (0.1566) | (0.0751) | (0.0087) | (0.0166) | (0.0168) | |
| lnper_income | 0.189 *** | 0.124 *** | −0.011 *** | −0.016 *** | 0.027 *** |
| (0.0259) | (0.0147) | (0.0016) | (0.0032) | (0.0032) | |
| city | −0.058 | −0.147 *** | 0.003 | 0.029 *** | −0.033 *** |
| (0.0608) | (0.0315) | (0.0037) | (0.0069) | (0.0070) | |
| Constant | 3.247 *** | 0.967 *** | |||
| (0.3378) | (0.1696) | ||||
| Province—Fixed Effect | Yes | Yes | |||
| Year—Fixed Effect | Yes | Yes | |||
| Pseudo R2 | 0.064 | ||||
| Log pseudolikelihood | −18,001.183 | ||||
| Observations | 22,144 | 22,144 | |||
| Variables | Baseline Model | Marginal Effect | |||
|---|---|---|---|---|---|
| health_self = 1 Bad | health_self = 2 Fair | health_self = 3 Good | |||
| (i) | (ii) | (iii) | (iv) | (v) | |
| diet_knowledge | 0.095 * | 0.057 * | −0.005 * | −0.007 | 0.012 * |
| (0.0482) | (0.0250) | (0.0027) | (0.0054) | (0.0055) | |
| diet_knowledge_sp | −0.088 | 0.025 | 0.005 | −0.010 | 0.005 |
| (0.0487) | (0.0248) | (0.0027) | (0.0054) | (0.0054) | |
| Constant | 2.461 *** | 1.055 *** | |||
| (0.4993) | (0.2487) | ||||
| Covariates | Yes | Yes | |||
| Province—Fixed Effect | Yes | Yes | |||
| Year—Fixed Effect | Yes | Yes | |||
| Pseudo R2 | 0.067 | ||||
| Log pseudolikelihood | −8924.568 | ||||
| Observations | 11,276 | 11,276 | |||
| Variables | Baseline Model | Marginal Effect | |||
|---|---|---|---|---|---|
| health_self = 1 Bad | health_self = 2 Fair | health_self = 3 Good | |||
| (i) | (ii) | (iii) | (iv) | (v) | |
| diet_knowledge | 0.061 | 0.091 *** | −0.004 | −0.016 ** | 0.020 *** |
| (0.0451) | (0.0251) | (0.0029) | (0.0056) | (0.0056) | |
| diet_knowledge_sp | 0.008 | 0.021 | −0.001 | −0.004 | 0.005 |
| (0.0447) | (0.0250) | (0.0029) | (0.0056) | (0.0056) | |
| Constant | 3.864 *** | 1.014 *** | |||
| (0.4764) | (0.2389) | ||||
| Covariates | Yes | Yes | |||
| Province—Fixed Effect | Yes | Yes | |||
| Year—Fixed Effect | Yes | Yes | |||
| Pseudo R2 | 0.063 | ||||
| Log pseudolikelihood | −9027.395 | ||||
| Observations | 10,868 | 10,868 | |||
| Explanatory Variable | Dependent Variable | Education | Income | Region | |||
|---|---|---|---|---|---|---|---|
| Low-Education (i) | High-Education (ii) | Low-Income (iii) | High-Income (iv) | Rural (v) | Urban (vi) | ||
| diet_knowledge | health_self = 1 | −0.011 *** | −0.002 | −0.010 *** | −0.005 * | −0.009 *** | −0.004 |
| (0.0019) | (0.0021) | (0.0022) | (0.0018) | (0.0018) | (0.0024) | ||
| health_self = 2 | −0.018 *** | −0.009 | −0.013 *** | −0.018 *** | −0.023 *** | 0.004 | |
| (0.0034) | (0.0051) | (0.0040) | (0.0040) | (0.0035) | (0.0048) | ||
| health_self = 3 | 0.029 *** | 0.011 * | 0.023 *** | 0.022 *** | 0.032 *** | −0.00004 | |
| (0.0034) | (0.0052) | (0.0040) | (0.0041) | (0.0035) | (0.0049) | ||
| Covariates | Yes | Yes | Yes | Yes | Yes | Yes | |
| Province—Fixed Effect | Yes | Yes | Yes | Yes | Yes | Yes | |
| Year—Fixed Effect | Yes | Yes | Yes | Yes | Yes | Yes | |
| Observations | 19,528 | 9161 | 14,344 | 14,345 | 18,004 | 10,685 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, Y.; Dong, D.; Ding, Y. The Impact of Dietary Knowledge on Health: Evidence from the China Health and Nutrition Survey. Int. J. Environ. Res. Public Health 2021, 18, 3736. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073736
Sun Y, Dong D, Ding Y. The Impact of Dietary Knowledge on Health: Evidence from the China Health and Nutrition Survey. International Journal of Environmental Research and Public Health. 2021; 18(7):3736. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073736
Chicago/Turabian StyleSun, Yangyang, Daxin Dong, and Yulian Ding. 2021. "The Impact of Dietary Knowledge on Health: Evidence from the China Health and Nutrition Survey" International Journal of Environmental Research and Public Health 18, no. 7: 3736. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073736