
An Empirical Study on Diabetes Depression over Distress Evaluation Using Diagnosis Statistical Manual and Chi-Square Method

 ,
,  , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Consents
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection and Explanation
2.4. Measurements
2.5. Attributes and Statistical Analysis
3. Results
4. Discussion
Strength and Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vargatu, I. Williams Textbook of Endocrinology. In Acta Endocrinologica (Bucharest), 13th ed.; Elsevier: Bucharest, Romania, 2016; Volume 12, pp. 113–147. [Google Scholar]
- International Diabetes Federation. IDF Diabetes Atlas Ninth edition 2019; IDF: Brussels, Belgium, 2019. [Google Scholar]
- Kazi, A.A.; Blonde, L. Classification of Diabetes Mellitus, 2019th ed.; World Health Organization: Cham, Switzerland, 2019; Volume 21, pp. 33–120. [Google Scholar]
- American Diabetes Association. 1. Improving care and promoting health in populations: Standards of medical care in diabetesd2019. Diabetes Care 2019, 42, S7–S12. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2014, 37, S81–S90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geiss, L.S.; Bullard, K.M.K.; Brinks, R.; Gregg, E.W. Considerations in epidemiologic definitions of undiagnosed diabetes. Diabetes Care 2018, 41, 1835–1838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muhammad, M.U.; Jiadong, R.; Sohail, M.N.; Irshad, M.; Bilal, M.; Osi, A.A. A logistic regression modeling on the prevalence of diabetes mellitus in the North Western Part of Nigeria. Benin J. Stat. 2018, 1, 1–10. [Google Scholar]
- Sohail, M.N.; Jiadong, R.; Uba, M.M.; Irshad, M.; Iqbal, W.; Arshad, J.; John, A.V. A hybrid Forecast Cost Benefit Classification of diabetes mellitus prevalence based on epidemiological study on Real-life patient’s data. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gentile, A.; Bianco, A.; Nordstrӧm, A.; Nordstrӧm, P. Use of alcohol, drugs, inhalants, and smoking tobacco and the long-term risk of depression in men: A nationwide Swedish cohort study from 1969–2017. Drug Alcohol Depend. 2021, 221, 108559. [Google Scholar] [CrossRef]
- Tran, N.M.H.; Nguyen, Q.N.L.; Vo, T.H.; Le, T.T.A.; Ngo, N.H. Depression Among Patients with Type 2 Diabetes Mellitus: Prevalence and Associated Factors in Hue City, Vietnam. Diabetes Metab. Syndr. Obes. Targets Ther. 2021, 14, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, P.; La Valle, E.; Falbo, R.; Limonta, G.; Signorini, S.; Cappellini, F.; Mocarelli, P. Normal fasting plasma glucose and risk of type 2 diabetes. Diabetes Care 2011, 34, 1372–1374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costacou, T.; Orchard, T.J. Cumulative kidney complication risk by 50 years of type 1 diabetes: The effects of sex, age, and calendar year at onset. Diabetes Care 2018, 41, 426–433. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Obesity management for the treatment of type 2 diabetes: Standards of medical care in diabetesd2019. Diabetes Care 2019, 42, S81–S89. [Google Scholar] [CrossRef] [Green Version]
- Alzughbi, T.; Badedi, M.; Darraj, H.; Hummadi, A.; Jaddoh, S.; Solan, Y.; Sabai, A. Diabetes-related distress and depression in Saudis with type 2 diabetes. Psychol. Res. Behav. Manag. 2020, 13, 453–458. [Google Scholar] [CrossRef]
- Tunsuchart, K.; Lerttrakarnnon, P.; Srithanaviboonchail, K.; Likhitsathian, S.; Skulphan, S. Type 2 diabetes mellitus related distress in Thailand. Int. J. Environ. Res. Public Health 2020, 17, 2329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsobgny-Tsague, N.F.; Lontchi-Yimagou, E.; Nana, A.R.; Tankeu, A.T.; Katte, J.C.; Dehayem, M.Y.; Bengondo, C.M.; Sobngwi, E. Effects of nonsurgical periodontal treatment on glycated haemoglobin on type 2 diabetes patients (PARODIA 1 study): A randomized controlled trial in a sub-Saharan Africa population. BMC Oral Health 2018, 18, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devarajooh, C.; Chinna, K. Depression, distress and self-efficacy: The impact on diabetes self-care practices. PLoS ONE 2017, 12, e0175096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huynh, G.; Tran, T.T.; Do, T.H.; Truong, T.T.; Ong, P.T.; Nguyen, T.N.; Pham, L.A. Diabetes-Related Distress Among People with Type 2 Diabetes in Ho Chi Minh City, Vietnam: Prevalence and Associated Factors. Diabetes Metab. Syndr. Obes. Targets Ther. 2021, 14, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Coccaro, E.F.; Lazarus, S.; Joseph, J.; Wyne, K.; Drossos, T.; Phillipson, L.; de Groot, M. Emotional Regulation and Diabetes Distress in Adults With Type 1 and Type 2 Diabetes. Diabetes Care 2021, 44, 20–25. [Google Scholar] [CrossRef]
- Fisher, L.; Skaff, M.M.; Mullan, J.T.; Arean, P.; Glasgow, R.; Masharani, U. A longitudinal study of affective and anxiety disorders, depressive affect and diabetes distress in adults with type 2 diabetes. Diabet. Med. 2008, 25, 1096–1101. [Google Scholar] [CrossRef] [Green Version]
- Fisher, L.; Mullan, J.T.; Skaff, M.M.; Glasgow, R.E.; Arean, P.; Hessler, D. Predicting diabetes distress in patients with Type 2 diabetes: A longitudinal study. Diabet. Med. 2009, 26, 622–627. [Google Scholar] [CrossRef]
- Bener, A.; Al-Hamaq, A.O.A.A.; Dafeeah, E.E. High Prevalence of Depression, Anxiety and Stress Symptoms Among Diabetes Mellitus Patients. Open Psychiatr. J. 2011, 5, 5–12. [Google Scholar] [CrossRef] [Green Version]
- Sohail, M.N.; Jiadong, R.; Uba, M.M.; Irshad, M.; Bilal, M.; Akbar, U.; Rizwan, T. Forecast Regression analysis for Diabetes Growth: An inclusive data mining approach. Int. J. Adv. Res. Comput. Eng. Technol. 2018, 7, 715–721. [Google Scholar]
- Srikanta, P. Recent Developments in Intelligent Computing, Communication and Devices; Springer: Singapore, 2019; Volume 752. [Google Scholar]
- Sohail, N.; Jiadong, R.; Uba, M.M.; Irshad, M.; Khan, A. Classification and cost benefit Analysis of Diabetes mellitus Dominance. IJCSNS Int. J. Comput. Sci. Netw. Secur. 2018, 18, 29–35. [Google Scholar]
- Muhammad, M.U.; Asiribo, O.E.; Noman, S.M. Application of Logistic Regression Modeling Using Fractional Polynomials of Grouped Continuous Covariates. In Proceedings of the Nigeria Statistical Society, 2017; Volume 1, pp. 144–147. Available online: http://nss.com.ng/2017_edited_proceedings (accessed on 18 January 2019).
- Muhammad, M.U.; Jiadong, R.; Muhammad, N.S.; Nawaz, B. Stratified diabetes mellitus prevalence for the Northwestern Nigerian States, a data mining approach. Int. J. Environ. Res. Public Health 2019, 16, 4089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uba, M.M.; Jiadong, R.; Sohail, M.N.; Irshad, M.; Yu, K. Data mining process for predicting diabetes mellitus based model about other chronic diseases: A case study of the northwestern part of Nigeria. Healthc. Technol. Lett. 2019, 6, 98–102. [Google Scholar] [CrossRef]
- Sohail, M.N.; Jiadong, R.; Muhammad, M.U.; Chauhdary, S.T.; Arshad, J.; Verghese, A.J. An accurate clinical implication assessment for diabetes mellitus prevalence based on a study from Nigeria. Processes 2019, 7, 289. [Google Scholar] [CrossRef] [Green Version]
- Sohail, N.; Jiadong, R.; Irshad, M.; Uba, M.M.; Abir, S.I. Data mining techniques for Medical Growth: A Contribution of Researcher reviews. IJCSNS Int. J. Comput. Sci. Netw. Secur. 2018, 18, 5–10. [Google Scholar]
- Sohail, M.N.; Ren, J.; Muhammad, M.U.; Rizwan, T.; Iqbal, W.; Abir, S.I.; Irshad, M.; Bilal, M. Group covariates assessment on real-life Diabetes patients by Fractional Polynomials: A study based on Logistic Regression Modeling. J. Biotech Res. 2019, 10, 116–125. [Google Scholar]
- Westhoff-Bleck, M.; Winter, L.; Aguirre Davila, L.; Herrmann-Lingen, C.; Treptau, J.; Bauersachs, J.; Bleich, S.; Kahl, K.G. Diagnostic evaluation of the hospital depression scale (HADS) and the Beck depression inventory II (BDI-II) in adults with congenital heart disease using a structured clinical interview: Impact of depression severity. Eur. J. Prev. Cardiol. 2020, 27, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Roy, M.; Sengupta, N.; Sahana, P.K.; Das, C.; Talukdar, P.; Baidya, A.; Goswami, S. Type 2 diabetes and influence of diabetes-specific distress on depression. Diabetes Res. Clin. Pract. 2018, 143, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Kuniss, N.; Kramer, G.; Müller, N.; Kloos, C.; Lehmann, T.; Lorkowski, S.; Wolf, G.; Müller, U.A. Diabetes-Related Burden and Distress is Low in People with Diabetes at Outpatient Tertiary Care Level. Exp. Clin. Endocrinol. Diabetes 2016, 124, 307–312. [Google Scholar] [CrossRef]
- Sohail, M.N.; Ren, J.; Muhammad, M.U. A euclidean group assessment on semi-supervised clustering for healthcare clinical implications based on real-life data. Int. J. Environ. Res. Public Health 2019, 16, 1581. [Google Scholar] [CrossRef] [Green Version]
- Muhammad, M.U.; Jiadong, R.; Muhammad, N.S.; Hussain, M.; Muhammad, I. Principal component analysis of categorized polytomous variable-based classification of diabetes and other chronic diseases. Int. J. Environ. Res. Public Health 2019, 16, 3593. [Google Scholar] [CrossRef] [Green Version]
- Niles, A.N.; O’Donovan, A. Comparing anxiety and depression to obesity and smoking as predictors of major medical illnesses and somatic symptoms. Heal. Psychol. 2019, 38, 172–181. [Google Scholar] [CrossRef]
- Valente, M.J.; Rijnhart, J.J.M.; Smyth, H.L.; Muniz, F.B.; MacKinnon, D.P. Causal Mediation Programs in R, Mplus, SAS, SPSS, and Stata. Struct. Equ. Model. 2020, 54, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Alavi, M.; Visentin, D.C.; Thapa, D.K.; Hunt, G.E.; Watson, R.; Cleary, M. Chi-square for model fit in confirmatory factor analysis. J. Adv. Nurs. 2020, 76, 2209–2211. [Google Scholar] [CrossRef] [PubMed]
- Cho, N.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Kunugi, H. Intermittent fasting, dietary modifications, and exercise for the control of gestational diabetes and maternal mood dysregulation: A review and a case report. Int. J. Environ. Res. Public Health 2020, 17, 9379. [Google Scholar] [CrossRef]
- Napoli, A.; Lamis, D.A.; Berardelli, I.; Canzonetta, V.; Sarubbi, S.; Rogante, E.; Napoli, P.L.; Serafini, G.; Erbuto, D.; Tambelli, R.; et al. Anxiety, Prenatal Attachment, and Depressive Symptoms in Women with Diabetes in Pregnancy. Int. J. Environ. Res. Public Health 2020, 17, 425. [Google Scholar] [CrossRef] [Green Version]
- Löwe, B.; Kroenke, K.; Herzog, W.; Gräfe, K. Measuring depression outcome with a brief self-report instrument: Sensitivity to change of the Patient Health Questionnaire (PHQ-9). J. Affect. Disord. 2004, 81, 61–66. [Google Scholar] [CrossRef]
- Gilbody, S.; Richards, D.; Brealey, S.; Hewitt, C. Screening for depression in medical settings with the Patient Health Questionnaire (PHQ): A diagnostic meta-analysis. J. Gen. Intern. Med. 2007, 22, 1596–1602. [Google Scholar] [CrossRef] [Green Version]
- Caneo, C.; Toro, P.; Ferreccio, C. Validity and Performance of the Patient Health Questionnaire (PHQ-2) for Screening of Depression in a Rural Chilean Cohort. Community Ment. Health J. 2020, 56, 1284–1291. [Google Scholar] [CrossRef]
- Rababah, J.; Al-Hammouri, M.M.; Drew, B.L.; Alawawdeh, A.; Dawood, Z.; Jawhar, W.E. Validation of the Arabic version of the center for epidemiologic studies depression-revised: A comparison of the CESD-R and CESDR-12. J. Affect. Disord. 2020, 274, 450–456. [Google Scholar] [CrossRef] [PubMed]
- Lašaitė, L.; Dobrovolskienė, R.; Danytė, E.; Stankutė, I.; Ražanskaitė-Virbickienė, D.; Schwitzgebel, V.; Marčiulionytė, D.; Verkauskienė, R. Diabetes distress in males and females with type 1 diabetes in adolescence and emerging adulthood. J. Diabetes Complicat. 2016, 30, 1500–1505. [Google Scholar] [CrossRef] [Green Version]
- Parsa, S.; Aghamohammadi, M.; Abazari, M. Diabetes distress and its clinical determinants in patients with type II diabetes. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 1275–1279. [Google Scholar] [CrossRef] [PubMed]
- Gahlan, D.; Rajput, R.; Gehlawat, P.; Gupta, R. Prevalence and determinants of diabetes distress in patients of diabetes mellitus in a tertiary care centre. Diabetes Metab. Syndr. Clin. Res. Rev. 2018, 12, 333–336. [Google Scholar] [CrossRef] [PubMed]
- Nazir, T.; Irtaza, A.; Javed, A.; Malik, H.; Hussain, D.; Naqvi, R.A. Retinal Image Analysis for Diabetes-Based Eye Disease Detection Using Deep Learning. Appl. Sci. 2020, 10, 6185. [Google Scholar] [CrossRef]
- Roy, T.; Lloyd, C.E.; Pouwer, F.; Holt, R.I.G.; Sartorius, N. Screening tools used for measuring depression among people with Type 1 and Type 2 diabetes: A systematic review. Diabet. Med. 2012, 29, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Xu, C.P.; Wu, H.X.; Xue, X.J.; Xu, Z.J.; Li, Y.; Gao, Q.; Liu, Q.Z. Comparative study of the influence of diabetes distress and depression on treatment adherence in Chinese patients with type 2 diabetes: A cross-sectional survey in the People’s Republic of China. Neuropsychiatr. Dis. Treat. 2013, 9, 1289–1294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whiting, D.R.; Guariguata, L.; Weil, C.; Shaw, J. IDF Diabetes Atlas: Global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res. Clin. Pract. 2011, 94, 311–321. [Google Scholar] [CrossRef]
- Ogurtsova, K.; da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.E.; Makaroff, L.E. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Nanayakkara, N.; Pease, A.; Ranasinha, S.; Wischer, N.; Andrikopoulos, S.; Speight, J.; De Courten, B.; Zoungas, S. Depression and diabetes distress in adults with type 2 diabetes: Results from the Australian National Diabetes Audit (ANDA) 2016. Sci. Rep. 2018, 8, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Salinero-Fort, M.A.; Gómez-Campelo, P.; San Andrés-Rebollo, F.J.; Cárdenas-Valladolid, J.; Abánades-Herranz, J.C.; de Santa Pau, E.C.; Chico-Moraleja, R.M.; Beamud-Victoria, D.; de Miguel-Yanes, J.M.; Jimenez-Garcia, R.; et al. Prevalence of depression in patients with type 2 diabetes mellitus in Spain (the DIADEMA Study): Results from the MADIABETES cohort. BMJ Open 2018, 8, 20768. [Google Scholar] [CrossRef] [PubMed]
- Wong, E.M.; Afshar, R.; Qian, H.; Zhang, M.; Elliott, T.G.; Tang, T.S. Diabetes Distress, Depression and Glycemic Control in a Canadian-Based Specialty Care Setting. Can. J. Diabetes 2017, 41, 362–365. [Google Scholar] [CrossRef] [PubMed]
- Zahid, N.; Asghar, S.; Claussen, B.; Hussain, A. Depression and diabetes in a rural community in Pakistan. Diabetes Res. Clin. Pract. 2008, 79, 124–127. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Hospital | Age Distribution | Male (n = 368) | Female (n = 344) | Total (n = 712) |
|---|---|---|---|---|
| Kebbi | ≥20 to <40 | 30 (8.15%) | 51 (14.83%) | 226 (31.74%) |
| ≥40 to <60 | 49 (13.31%) | 30 (8.72%) | ||
| ≥60 to ≤86 | 37 (10.05%) | 29 (8.43%) | ||
| Sokoto | ≥20 to <40 | 23 (6.25%) | 46 (13.73%) | 296 (41.57%) |
| ≥40 to <60 | 61 (16.57%) | 61 (17.73%) | ||
| ≥60 to ≤86 | 53 (14.40%) | 52 (15.12%) | ||
| Kaduna | ≥20 to <40 | 45 (12.23%) | 24 (6.98%) | 190 (26.69%) |
| ≥40 to <60 | 34 (9.24%) | 22 (6.39%) | ||
| ≥60 to ≤86 | 36 (9.79%) | 29 (8.43%) |
| Distress Subscale | Average Items | Items Break Down | Mean Score |
|---|---|---|---|
| Emotional Burden | 5 | 1, 4, 7, 10, 14 |
|
| Regimen distress | 5 | 3, 6, 8, 12, 16 | |
| Physician distress | 4 | 2, 5, 11, 15 | |
| Interpersonal distress | 3 | 9, 13, 17 |
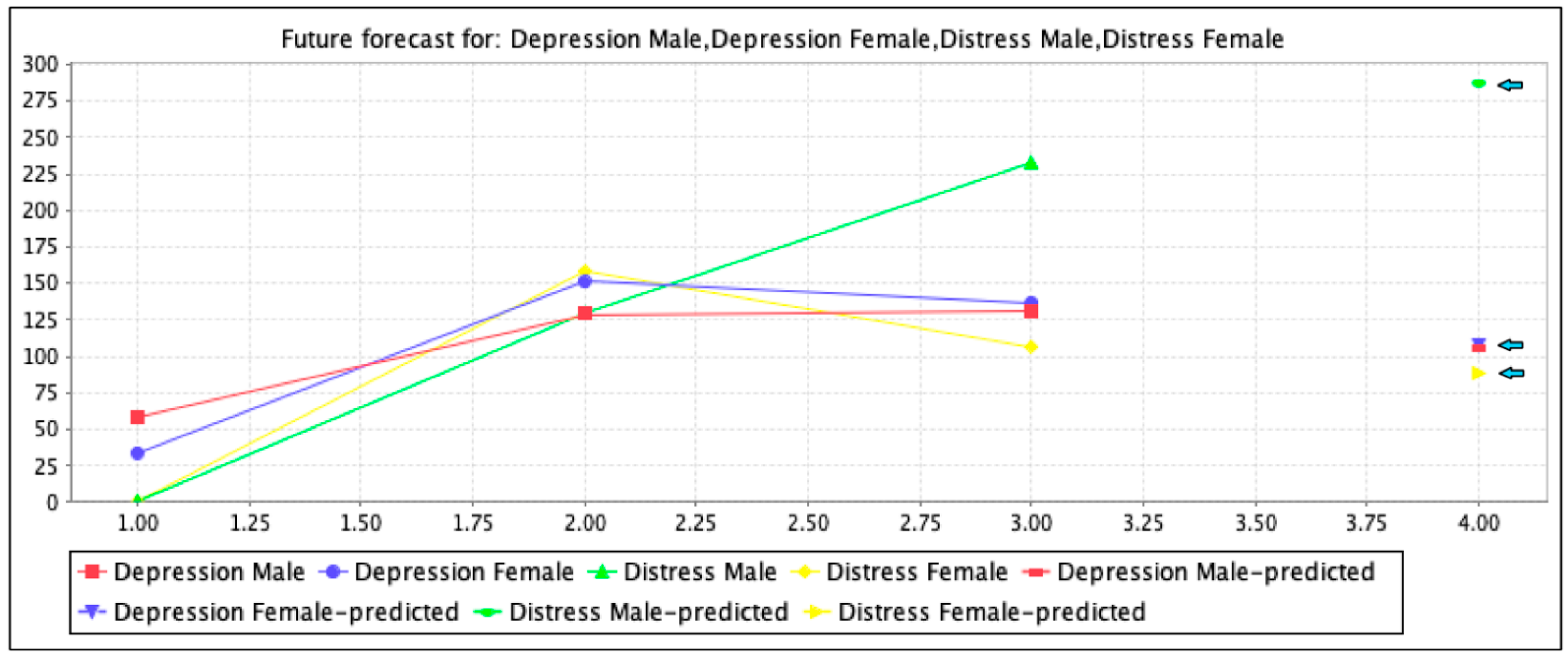
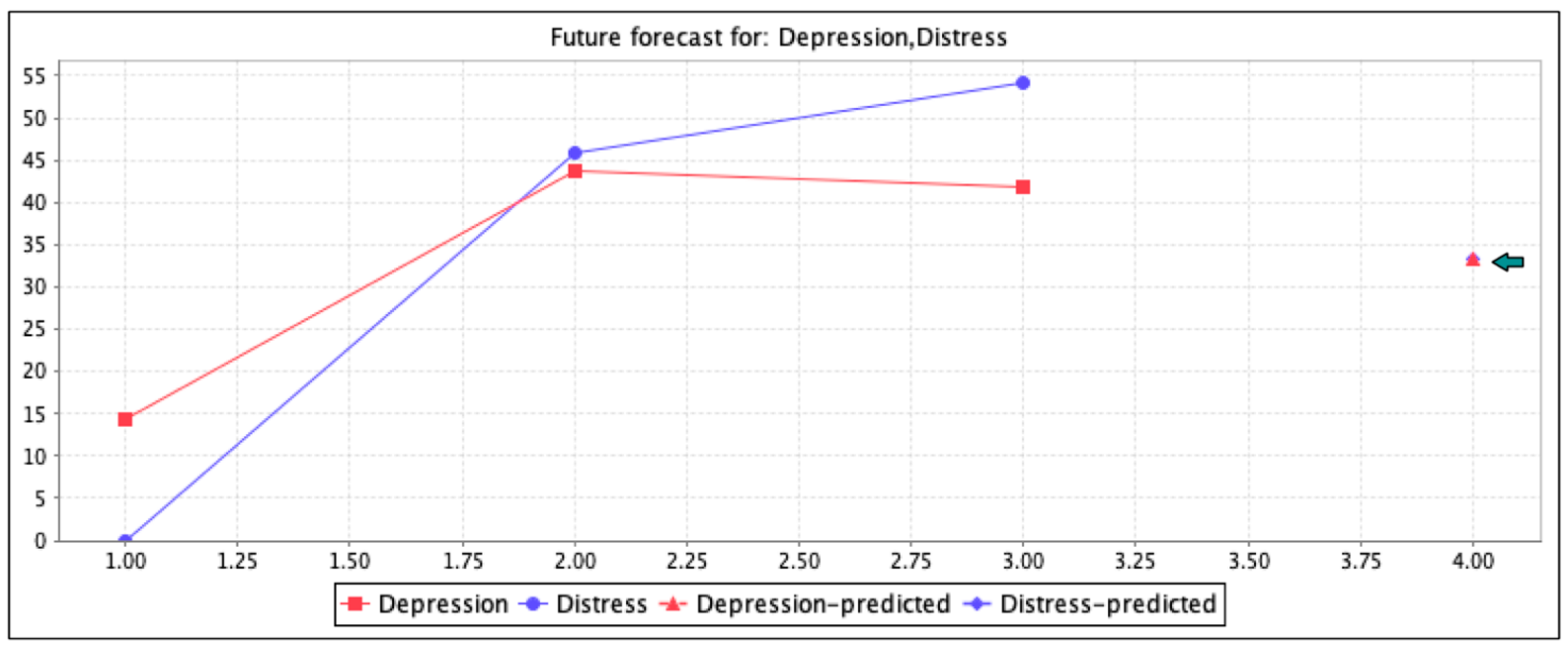
| Patients (n = 712) | Depression Present (n = 640, 89.89%) | Distress Present (n = 628, 88.20%) | |||
|---|---|---|---|---|---|
| Little | Moderate | Severe | Moderate | Severe | |
| Male | 58 (9.06%) | 129 (20.16%) | 131 (20.47%) | 130 (20.70%) | 233 (37.10%) |
| Female | 34 (5.31%) | 151 (23.59%) | 137 (21.40%) | 158 (25.16%) | 107 (17.04%) |
| Total | 92 (14.37%) | 280 (43.75%) | 268 (41.87%) | 288 (45.86%) | 340 (54.14%) |
| Distress | Depression Absent | Depression Present | Odd Ratio (95% CI) |
|---|---|---|---|
| Absent | 18 | 0 | 1.61 (1.34–2.96) |
| Present | 40 | 12 |
| Associated Attributes | Total (n = 712) | Multivariate Assessment | |
|---|---|---|---|
| Distress OR | Depression OR | ||
| Age | 2.8 (1.4–4.9) | 3.3 (1.1–5.8) | |
| ≥20 to <40 | 219 (30.76%) | ||
| ≥40 to <60 | 257 (36.09%) | ||
| ≥60 to ≤86 | 236 (33.15%) | ||
| Gender | 4.8 (2.9–6.9) | 4.9 (2.7–7.1) | |
| Male | 368 (51.68%) | ||
| Female | 344 (48.31%) | ||
| Smoking | 3.5 (2.1–4.3) | 3.3 (2.1–4.1) | |
| Yes | 328 (46.07%) | ||
| No | 384 (53.93%) | ||
| Diabetes history | 3.7 (1.7–6.7) | 4.2 (2.2–6.2) | |
| ≤5 years | 517 (72.61%) | ||
| >5 years | 195 (27.38%) | ||
| Physical exercise | 3.3 (1.3–6.3) | 3.9 (1.5–6.6) | |
| Yes | 277 (38.90%) | ||
| No | 435 (61.09%) | ||
| Countries | Prevalence Ratio | References | |
|---|---|---|---|
| Distress | Depression | ||
| Nigeria | 24.08% | 22.06% | Current study |
| Saudi Arabia | 23.03% | 20% | [14] |
| Australia | 7% | 6.02% | [2,40,53,54,55] |
| Germany | 8.09% | 7.04% | [2,34,40,53,54] |
| India | 18% | 17% | [33,49] |
| Spain | 18.06% | 20% | [2,40,53,54,56] |
| Canada | 23% | 12% | [2,40,53,54,57] |
| Pakistan | 20.05% | 14.07% | [2,40,53,54,58] |
| Iran | 21.04% | 18.04% | [2,40,48,53,54] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noman, S.M.; Arshad, J.; Zeeshan, M.; Rehman, A.U.; Haider, A.; Khurram, S.; Cheikhrouhou, O.; Hamam, H.; Shafiq, M. An Empirical Study on Diabetes Depression over Distress Evaluation Using Diagnosis Statistical Manual and Chi-Square Method. Int. J. Environ. Res. Public Health 2021, 18, 3755. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073755
Noman SM, Arshad J, Zeeshan M, Rehman AU, Haider A, Khurram S, Cheikhrouhou O, Hamam H, Shafiq M. An Empirical Study on Diabetes Depression over Distress Evaluation Using Diagnosis Statistical Manual and Chi-Square Method. International Journal of Environmental Research and Public Health. 2021; 18(7):3755. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073755
Chicago/Turabian StyleNoman, Sohail M., Jehangir Arshad, Muhammad Zeeshan, Ateeq Ur Rehman, Amir Haider, Shahzada Khurram, Omar Cheikhrouhou, Habib Hamam, and Muhammad Shafiq. 2021. "An Empirical Study on Diabetes Depression over Distress Evaluation Using Diagnosis Statistical Manual and Chi-Square Method" International Journal of Environmental Research and Public Health 18, no. 7: 3755. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073755