
Knowledge and Perception of COVID-19 Pandemic during the First Wave (Feb–May 2020): A Cross-Sectional Study among Italian Healthcare Workers

 , ,
, ,
Abstract
:1. Background
2. Methods
2.1. Study Design
2.2. Data Collection Procedures
2.3. Sample Size
2.4. Definitions
- -
- Do you believe that information released by international health authorities regarding the pandemic from COVID-19 in China has been clear enough?
- -
- Do you believe that information disseminated by national and regional health authorities regarding the risks associated with COVID-19 for the Italian population has been sufficiently clear?
- -
- Do you think that the definition of a suspected case of COVID-19 infection is sufficiently clear?
- -
- Do you think you have been sufficiently informed by the national health authorities on how to behave if you are faced with a suspected case of COVID-19?
- -
- Since the start of the COVID-19 pandemic, have you changed the way you work?
- -
- Since the start of the COVID-19 pandemic, has there been any impact in the organization of visits?
- -
- Since the beginning of the COVID-19 pandemic, has there been any impact in your relationship with patients?
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HCW | Healthcare workers |
| IPC | Infection prevention and control |
| COVID-19 | Coronavirus Disease 2019 |
| PPE | Personal protective equipment |
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- WHO. Director-General’s opening remarks at the media briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 16 November 2020).
- Lescure, F.-X.; Bouadma, L.; Nguyen, D.; Parisey, M.; Wicky, P.-H.; Behillil, S.; Gaymard, A.; Bouscambert-Duchamp, M.; Donati, F.; Le Hingrat, Q.; et al. Clinical and virological data of the first cases of COVID-19 in Europe: A case series. Lancet Infect. Dis. 2020, 20, 697–706. [Google Scholar] [CrossRef] [Green Version]
- Spiteri, G.; Fielding, J.; Diercke, M.; Campese, C.; Enouf, V.; Gaymard, A.; Bella, A.; Sognamiglio, P.; Moros, M.J.S.; Riutort, A.N.; et al. First cases of coronavirus disease 2019 (COVID-19) in the WHO European Region, 24 January to 21 February 2020. Euro Surveill. 2020, 25, 2000178. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC7068164/ (accessed on 16 November 2020). [CrossRef] [Green Version]
- Giovanetti, M.; Benvenuto, D.; Angeletti, S.; Ciccozzi, M. The first two cases of 2019-nCoV in Italy: Where they come from? J. Med. Virol. 2020, 92, 518–521. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC7166327/ (accessed on 16 November 2020). [CrossRef] [PubMed] [Green Version]
- Guzzetta, G.; Poletti, P.; Ajelli, M.; Trentini, F.; Marziano, V.; Cereda, D.; Tirani, M.; Diurno, G.; Bodina, A.; Barone, A.; et al. Potential short-term outcome of an uncontrolled COVID-19 epidemic in Lombardy, Italy, February to March 2020. Eurosurveillance 2020, 25, 2000293. Available online: https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2020.25.12.2000293 (accessed on 16 November 2020). [CrossRef] [PubMed]
- Indolfi, C.; Spaccarotella, C. The Outbreak of COVID-19 in Italy. JACC Case Rep. 2020, 2, 1414–1418. [Google Scholar] [CrossRef] [PubMed]
- Backer, J.A.; Klinkenberg, D.; Wallinga, J. Incubation period of 2019 novel coronavirus (2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020. Euro Surveill. 2020, 25, 2000062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Decreto Del Presidente Del Consiglio Dei Ministri. Available online: https://www.trovanorme.salute.gov.it/norme/dettaglioAtto?id=73196&articolo=6 (accessed on 23 February 2020).
- Decreto Del Presidente Del Consiglio Dei Ministri. Available online: https://www.trovanorme.salute.gov.it/norme/dettaglioAtto?id=73643 (accessed on 11 March 2020).
- Lai, A.; Bergna, A.; Caucci, S.; Clementi, N.; Vicenti, I.; Dragoni, F.; Cattelan, A.M.; Menzo, S.; Pan, A.; Callegaro, A.; et al. Molecular tracing of SARS-CoV-2 in Italy in the first three months of the epidemic. Viruses 2020, 12, 798. Available online: https://covid19.elsevierpure.com/it/publications/molecular-tracing-of-sars-cov-2-in-italy-in-the-first-three-month (accessed on 16 November 2020). [CrossRef]
- Onder, G.; Giovanni, R.; Silvio, B. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. Available online: http://europepmc.org/article/MED/32203977 (accessed on 16 November 2020). [CrossRef] [PubMed]
- Gámbaro, F.; Behillil, S.; Baidaliuk, A.; Donati, F.; Albert, M.; Alexandru, A.; Vanpeene, M.; Bizard, M.; Brisebarre, A.; Barbet, M.; et al. Introductions and early spread of SARS-CoV-2 in France, 24 January to 23 March 2020. Eurosurveillance 2020, 25, 2001200. Available online: https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2020.25.26.2001200 (accessed on 16 November 2020). [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Shah, S.J.; Barish, P.N.; Prasad, P.A.; Kistler, A.; Neff, N.; Kamm, J.; Li, L.M.; Chiu, C.Y.; Babik, J.M.; Fang, M.C.; et al. Clinical features, diagnostics, and outcomes of patients presenting with acute respiratory illness: A retrospective cohort study of patients with and without COVID-19. EclinicalMedicine 2020, 27, 100518. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC7447618/ (accessed on 16 November 2020). [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Infection Prevention and Control During Health Care when Coronavirus Disease (COVID-19) is Suspected or Confirmed. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-IPC-2020.4 (accessed on 16 November 2020).
- Lan, F.-Y.; Filler, R.; Mathew, S.; Buley, J.; Iliaki, E.; Bruno-Murtha, L.A.; Osgood, R.; Christophi, C.A.; Fernandez-Montero, A.; Kales, S.N. COVID-19 symptoms predictive of healthcare workers’ SARS-CoV-2 PCR results. PLoS ONE 2020, 15. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC7319316/ (accessed on 17 November 2020). [CrossRef]
- Fusco, F.; Pisaturo, M.; Iodice, V.; Bellopede, R.; Tambaro, O.; Parrella, G.; Di Flumeri, G.; Viglietti, R.; Pisapia, R.; Carleo, M.; et al. COVID-19 among healthcare workers in a specialist infectious diseases setting in Naples, Southern Italy: Results of a cross-sectional surveillance study. J. Hosp. Infect. 2020, 105, 596–600. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC7301109/ (accessed on 17 November 2020). [CrossRef]
- El-Boghdadly, K.; Wong, D.J.N.; Owen, R.; Neuman, M.D.; Pocock, S.; Carlisle, J.B.; Johnstone, C.; Andruszkiewicz, P.; Baker, P.A.; Biccard, B.M.; et al. Risks to healthcare workers following tracheal intubation of patients with COVID-19: A prospective international multicentre cohort study. Anaesthesia 2020, 75, 1437–1447. [Google Scholar] [CrossRef]
- Chen, Y.; Tong, X.; Wang, J.; Huang, W.; Yin, S.; Huang, R.; Yang, H.; Chen, Y.; Huang, A.; Liu, Y.; et al. High SARS-CoV-2 antibody prevalence among healthcare workers exposed to COVID-19 patients. J. Infect. 2020, 81, 420–426. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC7270786/ (accessed on 17 November 2020). [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72–314 Cases From the Chinese Center for Disease Control and Prevention. JAMA Netw. 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Report of the WHO—China Joint Mission on Coronavirus Disease 2019 (COVID-19). Available online: https://www.who.int/publications-detail-redirect/report-of-the-who-china-joint-mission-on-coronavirus-disease-2019-(covid-19) (accessed on 16 November 2020).
- Chou, R.; Dana, T.; Buckley, D.I.; Selph, S.; Fu, R.; Totten, A.M. Epidemiology of and Risk Factors for Coronavirus Infection in Health Care Workers: A Living Rapid Review. Ann. Intern. Med. 2020, 173, 120–136. [Google Scholar] [CrossRef] [PubMed]
- Rapporto Istituto Superiore di Sanità COVID-19 n. 2/2020 Rev. 2.21. Available online: https://www.iss.it/rapporti-covid-19/-/asset_publisher/btw1J82wtYzH/content/indicazioni-ad-interim-per-un-utilizzo-razionale-delle-protezioni-per-infezione-da-sars-cov-2-nelle-attivit%25C3%25A0-sanitarie-e-sociosanitarie-assistenza-a-soggetti-affetti-da-covid-19-nell-attuale-scenario-emergenziale-sars-cov-2 (accessed on 16 November 2020).
- DECRETO-LEGGE 9 marzo 2020, n. 14. Disposizioni urgenti per il potenziamento del Servizio sanitario nazionale in relazione all’emergenza COVID-19. Available online: https://www.gazzettaufficiale.it/eli/gu/2020/03/09/62/sg/pdf (accessed on 17 November 2020).
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef] [PubMed]
- Moons, K.G.M.; Donders, R.A.R.T.; Stijnen, T.; Harrell, F.E. Using the outcome for imputation of missing predictor values was preferred. J. Clin. Epidemiol. 2006, 59, 1092–1101. [Google Scholar] [CrossRef] [PubMed]
- Bhagavathula, A.S.; Aldhaleei, W.A.; Rahmani, J.; Mahabadi, M.A.; Bandari, D.K. Knowledge and Perceptions of COVID-19 Among Health Care Workers: Cross-Sectional Study. JMIR Public Health Surveill. 2020, 6, e19160. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Zhou, M.; Tang, F.; Wang, Y.; Nie, H.; Zhang, L.; You, G. Knowledge, attitude, and practice regarding COVID-19 among healthcare workers in Henan, China. J. Hosp. Infect. 2020, 105, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Sommerstein, R.; Fux, C.A.; Vuichard-Gysin, D.; Abbas, M.; Marschall, J.; Balmelli, C.; Troillet, N.; Harbarth, S.; Schlegel, M.; Schlegel, M.; et al. Risk of SARS-CoV-2 transmission by aerosols, the rational use of masks, and protection of healthcare workers from COVID-19. Antimicrob. Resist. Infect. Control. 2020, 9, 100. [Google Scholar] [CrossRef]
- Istituto Superiore di Sanità- Sorveglianza Integrata COVID-19 in Italia (Ordinanza n. 640 del 27/02/2020). Available online: https://www.epicentro.iss.it/coronavirus/bollettino/Infografica_7aprile%20ITA.pdf (accessed on 17 November 2020).
- Boccia, S.; Ricciardi, W.; Ioannidis, J.P.A. What Other Countries Can Learn From Italy During the COVID-19 Pandemic. JAMA Intern. Med. 2020, 180, 927–928. [Google Scholar] [CrossRef] [Green Version]
- Colaneri, M.; Novelli, V.; Cutti, S.; Muzzi, A.; Resani, G.; Monti, M.C.; Rona, C.; Grugnetti, A.M.; Rettani, M.; Rovida, F.; et al. The experience of the health care workers of a severely hit SARS-CoV-2 referral Hospital in Italy: Incidence, clinical course and modifiable risk factors for COVID-19 infection. J Public Health 2020. [Google Scholar] [CrossRef]
- Saqlain, M.; Munir, M.; Rehman, S.; Gulzar, A.; Naz, S.; Ahmed, Z.; Tahir, A.; Mashhood, M. Knowledge, attitude, practice and perceived barriers among healthcare workers regarding COVID-19: A cross-sectional survey from Pakistan. J. Hosp. Infect. 2020, 105, 419–423. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC7211584/ (accessed on 17 November 2020).
- Huynh, G.; Nguyen, T.; Tran, V.; Vo, K.; Vo, V.; Pham, L. Knowledge and attitude toward COVID-19 among healthcare workers at District 2 Hospital, Ho Chi Minh City. Asian Pac. J. Trop. Med. 2020, 260–265. [Google Scholar] [CrossRef]
- Salman, M.; Mustafa, Z.; Asif, N.; Zaidi, H.A.; Shehzadi, N.; Khan, T.M.; Saleem, Z.; Hussain, K. Knowledge, attitude and preventive practices related to COVID-19 among health professionals of Punjab province of Pakistan. J. Infect. Dev. Ctries. 2020, 14, 707–712. [Google Scholar] [CrossRef]
- Kumar, J.; Katto, M.S.; A Siddiqui, A.; Sahito, B.; Jamil, M.; Rasheed, N.; Ali, M. Knowledge, Attitude, and Practices of Healthcare Workers Regarding the Use of Face Mask to Limit the Spread of the New Coronavirus Disease (COVID-19). Cureus 2020, 12, e7737. [Google Scholar] [CrossRef] [Green Version]
- Piché-Renaud, P.-P.; Groves, H.E.; Kitano, T.; Arnold, C.; Thomas, A.; Streitenberger, L.; Alexander, L.; Morris, S.K. Healthcare worker perception of a global outbreak of novel coronavirus (COVID-19) and personal protective equipment: Survey of a pediatric tertiary-care hospital. Infect. Control. Hosp. Epidemiol. 2020, 1–7. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 958) | Pre-Lockdown (n = 694) | Lockdown (n = 264) | |||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | p | |
| Type of participants | 0.022 | ||||||
| Non medical staff | 390 | 40.7 | 267 | 38.5 | 123 | 46.6 | |
| Medical staff | 568 | 59.3 | 427 | 61.5 | 141 | 53.4 | |
| Profession | <0.001 | ||||||
| Allied healthcare | 390 | 40.7 | 267 | 38.5 | 123 | 46.6 | |
| General Practitioner | 320 | 33.4 | 216 | 31.1 | 104 | 39.4 | |
| Pediatrician | 248 | 25.9 | 211 | 30.4 | 37 | 14.0 | |
| Age (range) | 0.043 | ||||||
| Median (IQR) | 52.0 (36–62) | 51.0 (35–62) | 54.0 (40–62) | ||||
| Age (in years) | 0.041 | ||||||
| ≤35 | 215 | 24.1 | 170 | 26.2 | 45 | 18.7 | |
| 36–45 | 150 | 16.8 | 111 | 17.1 | 39 | 16.2 | |
| 46–55 | 136 | 15.3 | 87 | 13.4 | 49 | 20.3 | |
| 56–65 | 312 | 35.0 | 227 | 34.9 | 85 | 35.3 | |
| ≥66 | 78 | 8.8 | 55 | 8.5 | 23 | 9.5 | |
| Sex | <0.001 | ||||||
| Male | 341 | 38.2 | 221 | 34.0 | 120 | 49.6 | |
| Female | 551 | 61.8 | 429 | 66.0 | 122 | 50.4 | |
| Area | 0.545 | ||||||
| North Italy | 427 | 48.1 | 318 | 48.9 | 109 | 45.8 | |
| Central Italy | 266 | 29.9 | 195 | 30.0 | 71 | 29.8 | |
| South Italy | 195 | 22.0 | 137 | 21.1 | 58 | 24.4 | |
| Organization * | 0.828 | ||||||
| Hospital | 222 | 57.2 | 155 | 58.1 | 67 | 55.4 | |
| Residential Care Facility | 60 | 15.5 | 39 | 14.6 | 21 | 17.4 | |
| Private institution | 36 | 9.3 | 27 | 10.1 | 9 | 7.4 | |
| Community healthcare center | 33 | 8.5 | 22 | 8.2 | 11 | 9.1 | |
| Other | 37 | 9.5 | 24 | 9.0 | 13 | 10.7 | |
| Total (n = 958) | Pre-Lockdown (n = 694) | Lockdown (n = 264) | |||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | p | |
| Are the patients you come in contact with, scared of the COVID-19 pandemic? | <0.001 | ||||||
| Not at all frightened | 237 | 25.2 | 197 | 28.9 | 40 | 15.4 | |
| A little scared | 274 | 29.1 | 219 | 32.1 | 55 | 21.2 | |
| Neutral | 221 | 23.5 | 149 | 21.8 | 72 | 27.8 | |
| Quite frightened | 111 | 11.8 | 60 | 8.8 | 51 | 19.7 | |
| Very scared | 98 | 10.4 | 57 | 8.4 | 41 | 15.8 | |
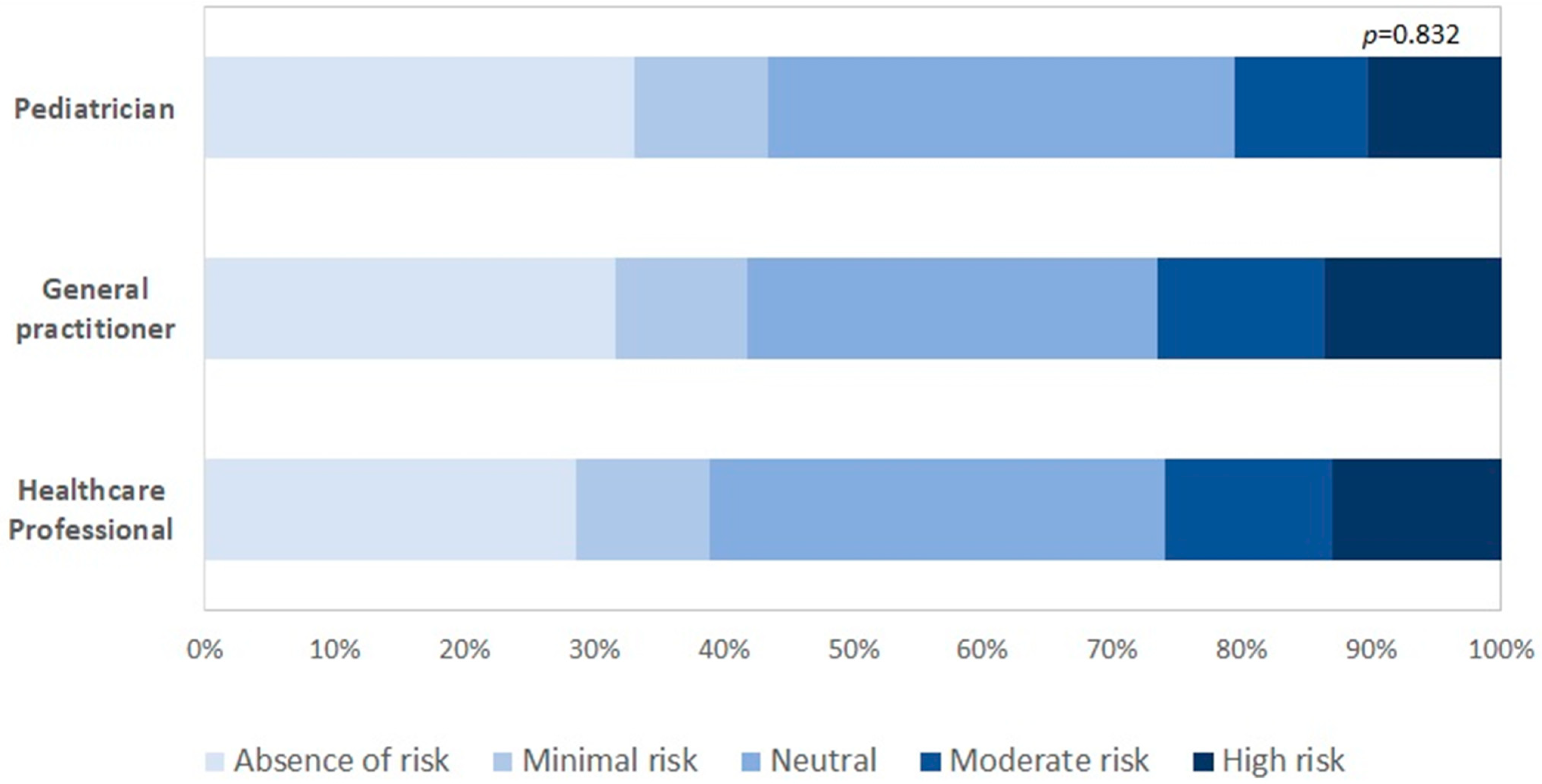
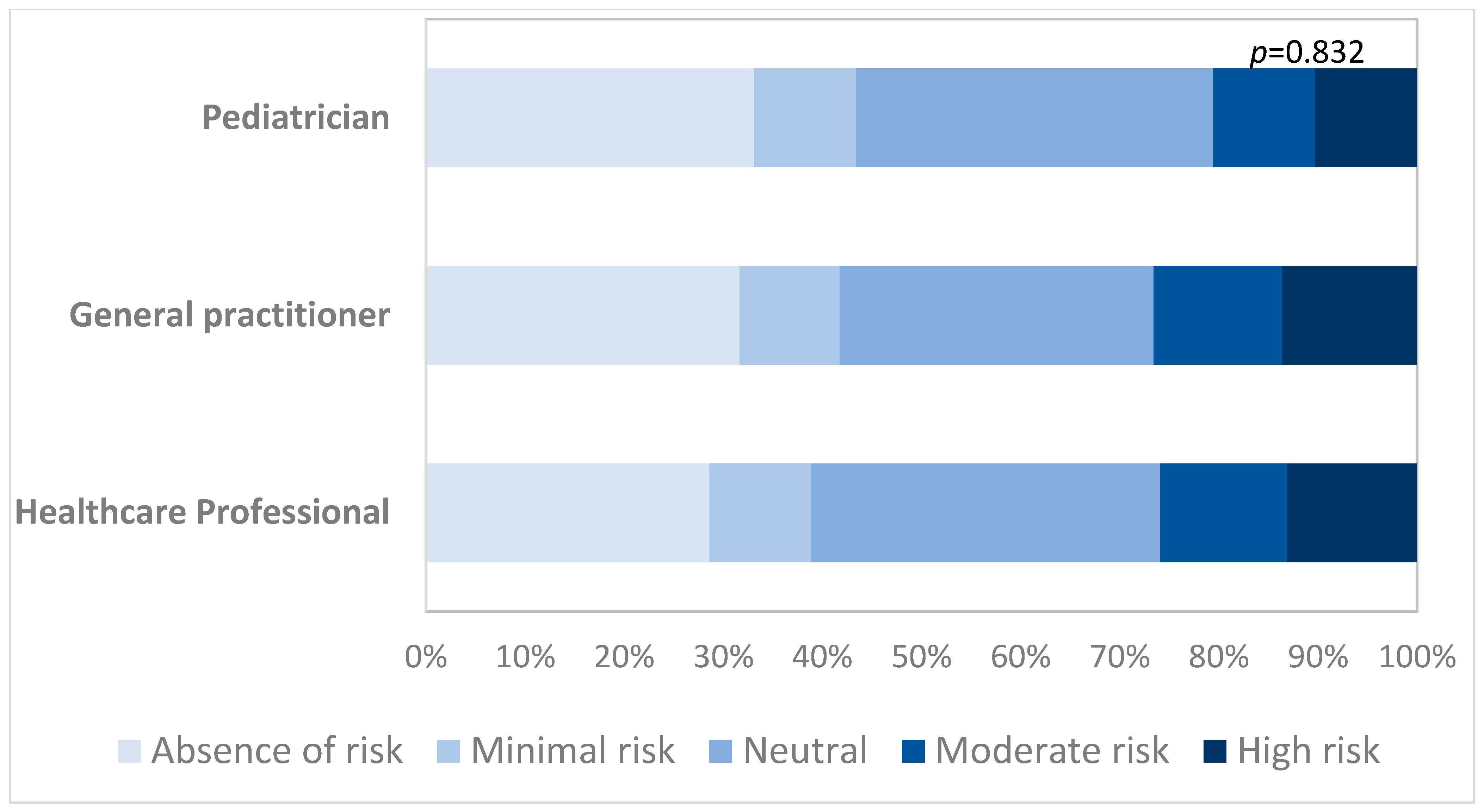
| In the last week, which was for you the risk to come in contact with patients affected by COVID-19? | 0.002 | ||||||
| Absence of risk | 264 | 31.1 | 216 | 33.5 | 48 | 23.3 | |
| Minimal risk | 87 | 10.2 | 69 | 10.7 | 18 | 8.7 | |
| Neutral | 290 | 34.1 | 219 | 34.0 | 71 | 34.5 | |
| Moderate risk | 103 | 12.1 | 74 | 11.5 | 29 | 14.1 | |
| High risk | 106 | 12.5 | 66 | 10.2 | 40 | 19.4 | |
| What containment measures were put in place in your work place? | |||||||
| Isolation of the patient (yes) | 72 | 85.7 | 29 | 96.7 | 43 | 82.7 | 0.063 |
| Contact quarantine (yes) | 40 | 47.6 | 18 | 60.0 | 22 | 40.7 | 0.090 |
| Administration of nasal swabs for close contacts | 35 | 41.7 | 15 | 50.0 | 20 | 35.2 | 0.185 |
| Healthcare worker quarantine (yes) | 25 | 29.8 | 12 | 40.0 | 13 | 24.1 | 0.126 |
| Social containment measures (yes) | 21 | 25.0 | - | - | 21 | 25.0 | <0.001 |
| Use of PPE (yes) | 4 | 4.8 | 2 | 6.7 | 2 | 3.7 | 0.143 |
| Since the start of the COVID-19 pandemic, have you changed the way you work? | <0.001 | ||||||
| Yes, absolutely | 519 | 55.8 | 313 | 46.3 | 206 | 81.1 | |
| Yes, moderately | 335 | 36.0 | 291 | 43.1 | 44 | 17.3 | |
| No, not really | 51 | 5.5 | 49 | 7.2 | 2 | 0.8 | |
| No, not at all | 21 | 2.3 | 19 | 2.8 | 2 | 0.8 | |
| I don’t know | 4 | 0.4 | 4 | 0.6 | - | - | |
| What have you changed in your clinical practice? * | |||||||
| Increased frequency of handwashing (yes) | 256 | 26.7 | 172 | 24.8 | 84 | 31.8 | 0.028 |
| Increased office disinfection (yes) | 624 | 65.1 | 424 | 61.1 | 200 | 75.8 | <0.001 |
| Increased use of masks (yes) | 628 | 65.6 | 398 | 57.4 | 230 | 87.1 | <0.001 |
| Increased use of protective glasses (yes) | 440 | 45.9 | 252 | 36.3 | 188 | 71.2 | <0.001 |
| Increased use of alcohol based hand solution (yes) | 467 | 48.8 | 279 | 40.2 | 188 | 71.2 | <0.001 |
| Do you believe that the information released by international health authorities regarding the COVID-19 pandemic in China has been clear enough? | 0.100 | ||||||
| Yes, absolutely | 152 | 18.0 | 111 | 18.2 | 41 | 17.7 | |
| Yes, moderately | 330 | 39.2 | 255 | 41.7 | 75 | 32.3 | |
| No, not really | 283 | 33.6 | 191 | 31.3 | 92 | 39.7 | |
| No, not at all | 71 | 8.4 | 49 | 8.0 | 22 | 9.5 | |
| I don’t know | 7 | 0.8 | 5 | 0.8 | 2 | 0.9 | |
| Do you believe that the information disseminated by national and regional health authorities regarding the risks associated with COVID-19 for the Italian population have been sufficiently clear? | 0.129 | ||||||
| Yes, absolutely | 174 | 20.9 | 122 | 20.1 | 52 | 23.2 | |
| Yes, moderately | 354 | 42.5 | 271 | 44.6 | 83 | 37.1 | |
| No, not really | 222 | 26.7 | 163 | 26.8 | 59 | 26.3 | |
| No, not at all | 78 | 9.4 | 49 | 8.1 | 29 | 12.9 | |
| I don’t know | 4 | 0.5 | 3 | 0.5 | 1 | 0.5 | |
| Do you think that the definition of a suspected case of a COVID-19 infection is sufficiently clear? | 0.750 | ||||||
| Yes, absolutely | 185 | 22.4 | 133 | 22.1 | 52 | 23.4 | |
| Yes, moderately | 353 | 42.8 | 265 | 43.9 | 88 | 39.6 | |
| No, not really | 235 | 28.5 | 170 | 28.2 | 65 | 29.3 | |
| No, not at all | 48 | 5.8 | 32 | 5.3 | 16 | 7.2 | |
| I don’t know | 4 | 0.5 | 3 | 0.5 | 1 | 0.5 | |
| Do you think you have been sufficiently informed by the national health authorities on how to behave if you are faced with a suspected COVID-19 case? | 0.477 | ||||||
| Yes, absolutely | 195 | 23.3 | 147 | 24.3 | 48 | 20.9 | |
| Yes, moderately | 375 | 44.9 | 276 | 45.5 | 99 | 43.0 | |
| No, not really | 204 | 24.4 | 138 | 22.8 | 66 | 28.7 | |
| No, not at all | 59 | 7.1 | 43 | 7.1 | 16 | 7.0 | |
| I don’t know | 3 | 0.4 | 2 | 0.3 | 1 | 0.4 | |
| Which of the following protective devices is most suitable to avoid the risk of transmission of COVID-19? | <0.001 | ||||||
| Surgical mask | 63 | 7.5 | 24 | 3.9 | 39 | 16.8 | |
| FFP1 mask | 17 | 2.0 | 13 | 2.1 | 4 | 1.7 | |
| FFP2 mask | 16 | 1.9 | 7 | 1.1 | 9 | 3.9 | |
| FFP3 mask | 642 | 75.9 | 510 | 83.1 | 132 | 56.9 | |
| Gas-masks | 1 | 0.1 | 1 | 0.2 | - | - | |
| All the above | 107 | 12.7 | 59 | 9.6 | 48 | 20.7 | |
| How do you keep yourself informed about operational guidelines? * | |||||||
| Emails sent by health authorities (yes) | 595 | 62.1 | 450 | 64.8 | 145 | 54.9 | 0.005 |
| Proactive search for information on official institutions’ websites (yes) | 521 | 54.4 | 360 | 51.9 | 161 | 61.0 | 0.011 |
| Proactive search for information through Ministry of Health toll-free number (yes) | 156 | 16.3 | 113 | 16.3 | 43 | 16.3 | 0.998 |
| Emails received from scientific companies (yes) | 262 | 27.4 | 190 | 27.4 | 72 | 27.3 | 0.974 |
| Exchange of information with other colleagues (yes) | 496 | 51.8 | 339 | 48.8 | 157 | 59.9 | 0.003 |
| Medical-scientific publications (yes) | 291 | 30.4 | 203 | 29.2 | 88 | 33.3 | 0.220 |
| Social networks (yes) | 151 | 15.8 | 116 | 16.7 | 35 | 13.3 | 0.189 |
| From patients (yes) | 7 | 0.7 | 4 | 0.6 | 3 | 1.1 | 0.363 |
| Which of the following social networks do you find most reliable to follow updates on the COVID-19 pandemic? | |||||||
| Facebook (yes) | 111 | 13.2 | 89 | 14.6 | 22 | 9.6 | 0.055 |
| LinkedIn (yes) | 22 | 2.6 | 10 | 1.6 | 12 | 5.2 | 0.004 |
| Instagram (yes) | 16 | 1.9 | 12 | 2.0 | 4 | 1.7 | 0.829 |
| Twitter (yes) | 28 | 3.3 | 18 | 2.9 | 10 | 4.3 | 0.315 |
| They are not reliable for updates (yes) | 684 | 81.4 | 495 | 81.1 | 189 | 82.2 | 0.733 |
| Do you think that the measures put in place by the health authorities to contain the spread of the pandemic in Italy are appropriate? | 0.380 | ||||||
| Yes, absolutely | 211 | 25.0 | 149 | 24.3 | 62 | 27.1 | |
| Yes, moderately | 395 | 46.9 | 284 | 46.2 | 111 | 48.5 | |
| No, not really | 181 | 21.5 | 141 | 23.0 | 40 | 17.5 | |
| No, not at all | 44 | 5.2 | 30 | 4.9 | 14 | 6.1 | |
| I don’t know | 12 | 1.4 | 10 | 1.6 | 2 | 0.9 | |
| Now that the COVID-19 pandemic has arrived in Italy, do you feel ready to face it? | 0.234 | ||||||
| Yes, absolutely | 61 | 7.3 | 40 | 6.6 | 21 | 9.3 | |
| Yes, moderately | 308 | 37.0 | 216 | 35.6 | 92 | 40.7 | |
| No, not really | 351 | 42.1 | 266 | 43.8 | 85 | 37.6 | |
| No, not at all | 94 | 11.3 | 69 | 11.4 | 25 | 11.1 | |
| I don’t know | 19 | 2.3 | 16 | 2.6 | 3 | 1.3 | |
| With reference to the COVID-19 pandemic, do you think that the importance given to, and spread by, the media and society in general is excessive? | 0.001 | ||||||
| Yes, absolutely | 131 | 16.0 | 107 | 18.0 | 24 | 10.6 | |
| Yes, moderately | 216 | 26.3 | 167 | 28.1 | 49 | 21.7 | |
| No, not really | 265 | 32.3 | 186 | 31.3 | 79 | 35.0 | |
| No, not at all | 199 | 24.3 | 126 | 21.2 | 73 | 32.3 | |
| I don’t know | 9 | 1.1 | 8 | 1.4 | 1 | 0.4 | |
| Information | Behavior Change | |||||
|---|---|---|---|---|---|---|
| adjOR | p-Value | 95% CI | adjOR | p-Value | 95% CI | |
| Age | ||||||
| ≤35 | Reference | Reference | ||||
| 36–45 | 0.89 | 0.614 | 0.56–1.42 | 1.71 | 0.027 * | 1.06–2.76 |
| 46–55 | 1.10 | 0.701 | 0.67–1.80 | 1.81 | 0.024 * | 1.08–3.04 |
| 56–65 | 1.60 | 0.061 | 0.98–2.62 | 1.81 | 0.023 * | 1.09–3.02 |
| ≥66 | 2.03 | 0.040 * | 1.03–4.00 | 1.49 | 0.241 | 0.76–2.93 |
| Sex | ||||||
| Male | Reference | Reference | ||||
| Female | 1.23 | 0.225 | 0.88–1.70 | 1.26 | 0.184 | 0.90–1.78 |
| Profession | ||||||
| Healthcare Professional | Reference | Reference | ||||
| General practitioner | 1.03 | 0.886 | 0.67–1.58 | 0.54 | 0.008 * | 0.35–0.85 |
| Pediatrician | 1.78 | 0.015 * | 1.12–2.85 | 0.64 | 0.083 | 0.39–1.07 |
| Region | ||||||
| North Italy | Reference | Reference | ||||
| Central Italy | 1.35 | 0.078 | 0.97–1.88 | 0.73 | 0.066 | 0.51–1.02 |
| South Italy | 1.41 | 0.076 | 0.93–2.08 | 0.67 | 0.049 * | 0.46–1.00 |
| Period | ||||||
| Pre-lockdown | Reference | Reference | ||||
| Lockdown | 1.16 | 0.377 | 0.84–1.59 | 6.22 | <0.001 * | 4.22–9.17 |
| Email sent by health authorities | ||||||
| No | Reference | Reference | ||||
| Yes | 1.81 | <0.001 * | 1.32–2.50 | 1.28 | 0.153 | 0.91–1.79 |
| Ministry of Health toll-free number | ||||||
| No | Reference | Reference | ||||
| Yes | 1.21 | 0.304 | 0.84–1.73 | 2.03 | 0.001 * | 1.35–3.06 |
| Now that the pandemic from COVID-19 has arrived in Italy, do you feel ready to face it? | ||||||
| Yes, absolutely | Reference | Reference | ||||
| Yes, moderately | 0.56 | 0.064 | 0.31–1.03 | 1.88 | 0.028 * | 1.07–3.30 |
| No, not really | 0.27 | <0.001 * | 0.15–0.50 | 1.76 | 0.047 * | 1.01–3.08 |
| No, not at all | 0.13 | <0.001 * | 0.06–0.26 | 1.35 | 0.390 | 0.68–2.64 |
| I don’t know | 0.20 | 0.003 * | 0.07–0.57 | 1.82 | 0.288 | 0.60–5.51 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rizzo, C.; Campagna, I.; Pandolfi, E.; Croci, I.; Russo, L.; Ciampini, S.; Gesualdo, F.; Tozzi, A.E.; Ricotta, L.; Raponi, M.; et al. Knowledge and Perception of COVID-19 Pandemic during the First Wave (Feb–May 2020): A Cross-Sectional Study among Italian Healthcare Workers. Int. J. Environ. Res. Public Health 2021, 18, 3767. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073767
Rizzo C, Campagna I, Pandolfi E, Croci I, Russo L, Ciampini S, Gesualdo F, Tozzi AE, Ricotta L, Raponi M, et al. Knowledge and Perception of COVID-19 Pandemic during the First Wave (Feb–May 2020): A Cross-Sectional Study among Italian Healthcare Workers. International Journal of Environmental Research and Public Health. 2021; 18(7):3767. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073767
Chicago/Turabian StyleRizzo, Caterina, Ilaria Campagna, Elisabetta Pandolfi, Ileana Croci, Luisa Russo, Sara Ciampini, Francesco Gesualdo, Alberto Eugenio Tozzi, Lara Ricotta, Massimiliano Raponi, and et al. 2021. "Knowledge and Perception of COVID-19 Pandemic during the First Wave (Feb–May 2020): A Cross-Sectional Study among Italian Healthcare Workers" International Journal of Environmental Research and Public Health 18, no. 7: 3767. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073767