
Regulation/Non-Regulation/Dys-Regulation of Health Behavior, Psychological Reactance, and Health of University Undergraduate Students


Abstract
:1. Introduction
1.1. Self-Regulation Behavior (SR)
1.2. The Theory of Self Regulation vs. External Regulation
1.2.1. Self-Regulation, Non-Regulation and Dys-Regulation of Health Behavior
- (1)
- (2)
- (3)
- Dys-Regulated Health behavior (DRH) refers to a degree of negative proactivity in one’s behavior, that is, active but inadequate behavior. The individual may find advantages in such dysregulation, which enables them to avoid the effort involved in positive, proactive health regulation. Examples include self-handicapping strategies, procrastination in matters of health or other risky behaviors [34,35,36,37,38,39].
1.2.2. Contexts of External Regulation, External Non-Regulation, and External Dys-Regulation of Health Behavior
- (1)
- Externally-regulated health behavior (ERH). In this context, individuals are encouraged to show positive or adequate proactivity and to practice self-regulation of health [42]. External indicators or promptings promote and increase the likelihood of self-regulated health behaviors. These may take the form of antecedents (patterns, norms, limits, expectations of successful health regulation, value given to health regulation) or of contextual consequences (positive and negative contingencies that favor health regulation, adaptation, etc.). Positive events that result in regulated health are strongly predicted in this context [43]).
- (2)
- External non-regulation of health behavior (ENH). The context does nothing to encourage one’s personal health regulation, but it does not contain health-dysregulating factors. No external indicators or promptings encourage self-regulated or dysregulated health behaviors, nor do they increase the likelihood of one or the other. A non-regulatory context requires the individual to employ a moderate level of their own health-regulating behavior, given that contextual elements offer no direction. Positive events that result in regulated health are not predicted in this context [44]).
- (3)
- External dys-regulation of health (EDH), actively promoting non-adaptive health behaviors. Inadequate or negative proactivity is encouraged in this type of context. There are many external indicators that encourage and increase the likelihood of active, dysregulating behavior. This behavior is also stimulated by contextual antecedents (modeling, rules, limits, negative expectations of self-regulation, negative value given to self-regulation, etc.) and by contextual consequences (positive and negative contingencies, molding, etc.) that encourage dysregulation. A great deal of effort is required from the individual who wishes to practice health-regulating behavior in this context. This context is highly predictive of negative events that result in dysregulated health.
1.2.3. Combinations of Self/External Regulation, Non-Regulation, and Dys-Regulation of Health
1.3. Psychological Reactance
1.4. Student Health
1.5. Objectives and Hypotheses
2. Method
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Data Analyses
3. Results
3.1. Previous Analyses
3.2. Linear Association
3.3. Linear and Structural Prediction
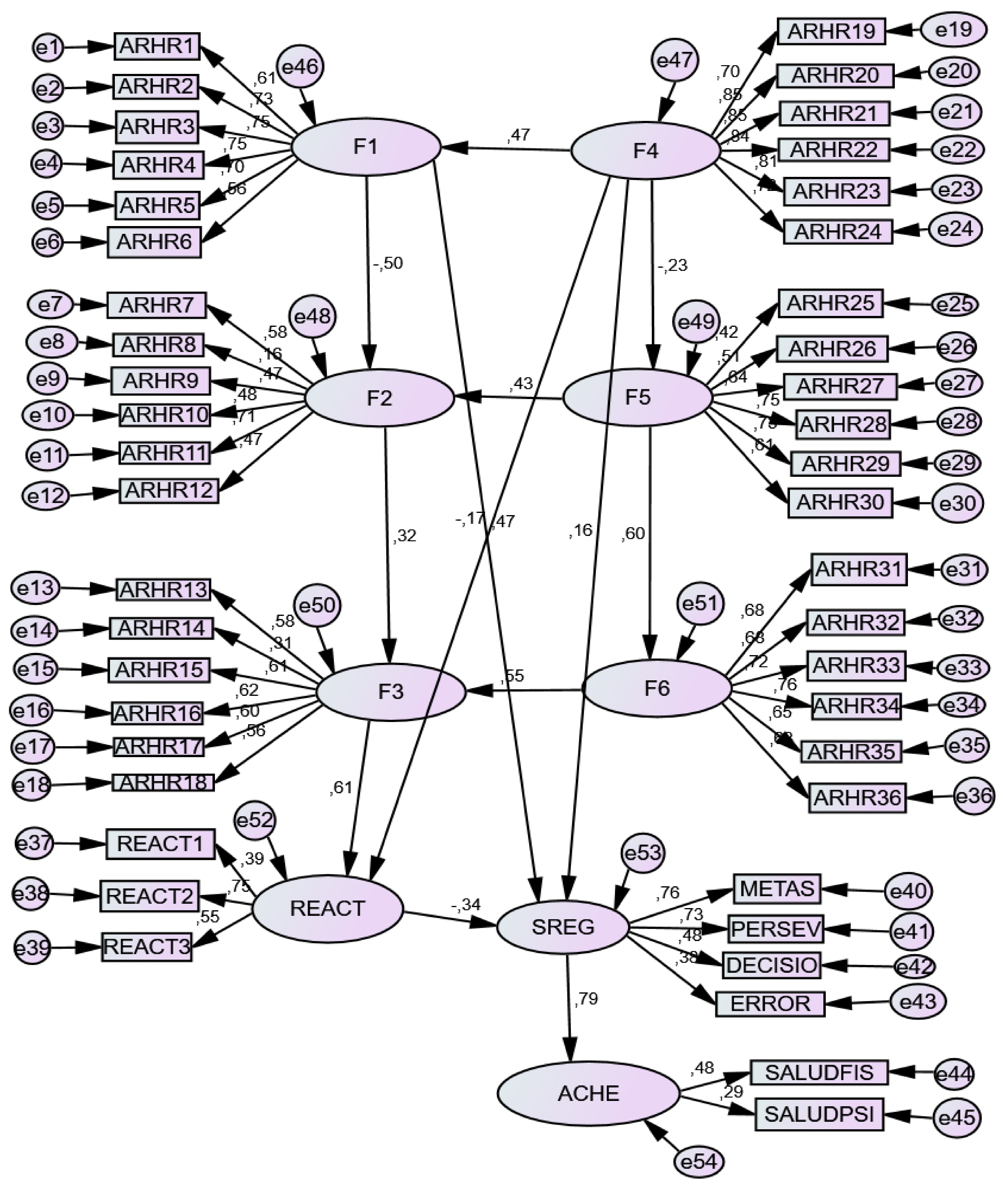
3.3.1. Structural Models
3.3.2. Direct and Indirect Effects
4. Discussion
4.1. Discussion of Hypotheses
4.2. Limitations
4.3. Goodness and Future Research
4.4. Professional Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stewart-Brown, S.; Evans, J.; Petersen, S.; Doll, H.; Regis, D. The health of students in institutes of higher education: An important and neglected public health problem? J. Public Health 2000, 22, 492–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ridner, S.; Newton, K.; Staten, R.; Crawford, T.; Hall, L. Predictors of well-being among college students. J. Am. Coll. Health 2016, 64, 116–124. [Google Scholar] [CrossRef]
- Organización Mundial de la Salud. Salud Mental del Adolescente. Available online: https://www.who.int/es/news-room/fact-sheets/detail/adolescent-mental-health (accessed on 20 November 2020).
- Garzón-Umerenkova, A.; de la Fuente, J.; Amate, J.; Paolini, P.V.; Fadda, S.; Pérez, J.F. A Linear empirical model of self-regulation on flourishing, health, procrastination, and achievement, among university students. Front. Psychol. 2018, 9, 536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laird, D.; Frazer, A. Psychological reactance and negative emotional reactions in the link between psychological control and adolescent adjustment robert. Soc. Dev. 2019, 29. [Google Scholar] [CrossRef]
- Lazarus, R.S. Puzzles in the Study of Daily Hassles. In Development as Action in Context; Silbereisen, R.K., Eyferth, K., Rudinger, G., Eds.; Springer: Berlin/Heidelberg, Germany, 1986; pp. 39–53. [Google Scholar] [CrossRef]
- Brown, J.M.; Miller, W.R.; Lawendowski, L.A. The Self-Regulation Questionnaire. In Innovations in Clinical Practice: A Source Book.; Vandecreek, L., Jackson, T.L., Eds.; Professional Resources Press: Sarasota, FL, USA, 1999; Volume 17, pp. 281–293. [Google Scholar]
- De la Fuente, J.; Zapata, L.; Martínez-Vicente, J.M.; Sander, P.; Cardelle-Elawar, M. The role of personal self-regulation and regulatory teaching to predict motivational-affective variables, achievement, and satisfaction: A structural model. Front. Psychol. 2015, 6, 399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De la Fuente, J. Theory of Self- vs. Externally- Regulated Learning TM: Fundamentals, evidence, and applicability. Front. Psychol. 2017, 8, 1675. [Google Scholar] [CrossRef] [PubMed]
- De la Fuente, J.; Amate, J.; González-Torres, M.C.; Artuch, R.; García-Torrecillas, J.M.; Fadda, S. Effects of levels of self-regulation and regulatory teaching on strategies for coping with academic stress in undergraduate students. Front. Psychol. 2020, 11, 22. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.X.; Wu, A.M.S. Effects of smartphone addiction on sleep quality among Chinese university students: The mediating role of self-regulation and bedtime procrastination. Addict. Behav. 2020, 111. [Google Scholar] [CrossRef] [PubMed]
- McLarnon, M.J.W.; Rothstein, M.G.; King, G.A. Resiliency, self-regulation, and reemployment after job loss. J. Employ. Couns. 2020, 57, 115–129. [Google Scholar] [CrossRef]
- Romer, A.L.; Hariri, A.; Strauman, T.J. Regulatory focus and the p factor: Evidence for self-regulatory dys-function as a transdiagnostic feature of general psychopathology. J. Psychiatr. Res. 2021, 137, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Caspi, A.; Moffitt, T.E. All for one and one for all: Mental disorders in one dimension. Am. J. Psychiatry 2018, 175, 831–844. [Google Scholar] [CrossRef] [Green Version]
- Caspi, A.; Houts, R.M.; Belsky, D.W.; Goldman-Mellor, S.J.; Harrington, H.; Israel, S.; Meier, M.H.; Ramrakha, S.; Shalev, I.; Poulton, R.; et al. The p factor: One general psychopathology factor in the structure of psychiatric disorders? Clin. Psychol. Sci. 2013, 2, 119–137. [Google Scholar] [CrossRef]
- Caspi, A.; Houts, R.M.; Ambler, A.; Danese, A.; Elliot, M.L.; Hariri, A.; Harrington, H.; Hogan, S.; Poulton, R.; Ramrakha, S.; et al. Longitudinal Assessment of mental health disorders and comorbidities across 4 decades among participants in the dunedin birth cohort study. JAMA Netw. Open 3. JAMA Netw. Open 2020, 3, e203221. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.M. Self-Regulation and the Addictive Behaviors. In Treating Addictive Behaviors; Miller, W.R., Heather, N., Eds.; Plenum Press: New York, NY, USA, 1998; pp. 61–73. [Google Scholar]
- De la Fuente, J. Self- vs. Externally- Regulation Scale in Health Questionary, SR-ER HEALTH; University of Navarra: Pamplona, Spain, 2020; Manuscrito pendiente de publicar. [Google Scholar]
- Zimmerman, B.J.; Labuhn, A.S. Self-Regulation of Learning: Process Approaches to Personal Development. In APA Educational Psychology Handbook; Theories, constructs, and critical issues; American Psychological Association: Worcester, MA, USA, 2012; Volume 1, pp. 399–425. [Google Scholar]
- De la Fuente, J.; Berbén, A.B.; Zapata, L. How regulatory teaching impacts university students’ perceptions of the teaching-learning process: The role of teacher training. Infancia Aprendizaje 2013, 36, 375–385. [Google Scholar] [CrossRef]
- De la Fuente, J.; Sander, P.; Martínez-Vicente, J.M.; Vera, M.M.; Garzón, A.; Fadda, S. Combined effect of levels in personal self-regulation and regulatory teaching on meta-cognitive, on meta-motivational, and on academic achievement variables in undergraduate students. Front. Psychol. 2017, 8, 232. [Google Scholar] [CrossRef] [Green Version]
- De la Fuente, J.; Martínez-Vicente, J.M.; Peralta-Sánchez, F.J.; Garzón-Umerenkova, A.; Vera, M.M.; Paolini, P. Applying the SRL vs ERL Theory to the Knowledge of Achievement Emotions in Undergraduate University Students. Front. Psychol. 2019, 10, 2070. [Google Scholar] [CrossRef] [PubMed]
- De la Fuente, J.; González-Torres, M.C.; Aznárez-Sanado, M.; Martínez-Vicente, J.M.; Peralta-Sánchez, F.J.; Vera, M.M. Implications of Unconnected Micro, Molecular, and Molar Level Research in Psychology: The Case of Executive Functions, Self-Regulation, and External Regulation. Front. Psychol. 2019, 10, 1919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De la Fuente, J.; Peralta-Sánchez, F.J.; Martínez-Vicente, J.M.; Sander, P.; Garzón-Umerenkova, A.; Zapata, L. Effects of Self- vs External Regulation on the Factors and Symptoms of Academic Stress in Undergraduate Students. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef]
- De la Fuente, J.; Paolini, P.V.; Vera-Martínez, M.M.; Garzón-Umerenkova, A. Effect of levels of self-regulation and situational Stress on Achievement Emotions in Undergraduate Students: Class, Study and Testing. Int. J. Environ. Res. Public Health 2020, 17, 4293. [Google Scholar] [CrossRef]
- Zimmerman, B.J.; Moylan, A.R. Self-Regulation: Where Metacognition and Motivation Intersect. In The Educational Psychology Series. Handbook of Metacognition in Education; Hacker, J., Dunlosky, A., Graesser, C., Eds.; Routledge/Taylor & Francis Group: London, UK, 2009; pp. 299–315. [Google Scholar]
- Zimmerman, B.J. Attaining Self-Regulation: A Social Cognitive Perspective. In Handbook of Self-Regulation; Boekaerts, M., Pintrich, P., Zeidner, M., Eds.; Elsevier: Amsterdam, The Netherlands, 2000; pp. 13–39. [Google Scholar] [CrossRef]
- Zimmerman, B.J.; Schunk, D.H. Self-Regulated Learning and Academic Achievement: Theoretical Perspectives; Routledge: Abingdon, UK, 2001. [Google Scholar]
- De la Fuente, J.; Paoloni, P.; Kauffman, D.; Yilmaz Soylu, M.; Sander, P.; Zapata, L. Big Five, Self-Regulation, and Coping Strategies as Predictors of Achievement Emotions in Undergraduate Students. Int. J. Environ. Res. Public Health 2020, 17, 3602. [Google Scholar] [CrossRef]
- Agostinelli, G.; Brown, J.M.; Miller, W.R. Effects of normative feedback on consumption among heavy drinking college students. J. Drug Educ. 1995, 25, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Hennessy, E.A.; Johnson, B.T.; Acabchuk, R.L.; McCloskey, K.; Stewart-James, J. Self-Regulation Mechanisms in Health Behaviour Change: A Systematic Meta-Review of Meta-Analyses, 2006–2017. Health Psychol. Rev. 2019, 1, 142. [Google Scholar] [CrossRef]
- Rienties, B.; Tempelaar, D.; Nguyen, Q.; Littlejohn, A. Unpacking the Intertemporal Impact of Self-Regulation in a Blended Mathematics Environment. Comput. Hum. Behav. 2019, 100, 345–357. [Google Scholar] [CrossRef]
- Balkis, M.; Duro, E. Gender Differences in the Relationship between Academic Procrastination, Satifaction with Academic Life and Academic Performance. Electron. J. Res. Educ. Psychol. 2017, 15, 105–125. [Google Scholar] [CrossRef] [Green Version]
- Beauchaine, T.P.; Crowell, S.E. (Eds.) The Oxford Handbook of Emotion Dysregulation; Oxford University Press: New York, NY, USA, 2020. [Google Scholar]
- Haghbin, M.; Pychyl, T.A. Measurement of Health-Related Procrastination: Development and Validation of the Exercise and Healthy Diet Procrastination Scales. In Procrastination, Health, and Well-Being; Academic Press: Cambridge, MA, USA, 2016; pp. 121–142. [Google Scholar]
- Clariana, M. Personalidad, Procrastinación y Conducta Deshonesta En Alumnado de Distintos Grados Universitarios. Electron. J. Res. Educ. Psychol. 2013, 11, 451–472. [Google Scholar] [CrossRef] [Green Version]
- Lew-Starowicz, M.; Lewczuk, K.; Nowakowska, I.; Kraus, S.; Gola, M. Compulsive Sexual Behavior and Dysregulation of Emotion. Sex. Med. Rev. 2020, 8, 191–205. [Google Scholar] [CrossRef] [PubMed]
- Richard, E. Developing Employee Resilience: The Role of Leader-Facilitated Emotion Management. Adv. Dev. Hum. Resour. 2020, 22, 387–403. [Google Scholar] [CrossRef]
- Quinn, P.D.; Fromme, K. Self-Regulation as a Protective Factor against Risky Drinking and Sexual Behavior. Psychol. Addict. Behav. 2010, 24, 376–385. [Google Scholar] [CrossRef] [Green Version]
- De la Fuente, J.; Sander, P.; Kauffman, D.; Yilmaz-Soylu, M. Differential Effects of Self- vs External- Regulation on Learning Approaches, Academic Achievement and Satisfaction in Undergraduate Students. Front. Psychol. 2020, 11, 543884. [Google Scholar] [CrossRef]
- Miller, A.L.; Lo, S.L.; Bauer, K.W.; Fredericks, E.M. Developmentally Informed Behaviour Change Techniques to Enhance Self-Regulation in a Health Promotion Context: A Conceptual Review. Health Psychol. Rev. 2020, 14, 116–131. [Google Scholar] [CrossRef]
- Mezuk, B.; Ratliff, S.; Concha, J.B.; Abdou, C.M.; Rafferty, J.; Lee, H.; Jackson, J.S. Stress, Self-Regulation, and Context: Evidence from the Health and Retirement Survey. SSM Popul. Health 2017, 3, 455–463. [Google Scholar] [CrossRef]
- Marquez, S.M. Relational and Contextual Antecedents of Emotion Regulation: Integrating the Easi Model into Existing Emotional Labor Models. Doctoral Dissertation, Michigan State University, Michigan, DT, USA, 2020. [Google Scholar]
- Steindl, C.; Jonas, E.; Sittenthaler, S.; Traut-Mattausch, E.; Greenberg, J. Understanding Psychological Reactance. Z. Psychol. 2015, 233, 205–214. [Google Scholar]
- Miron, A.M.; Brehm, J.W. Reactance Theory—40 Years Later. Z. Soz. 2006, 37, 9–18. [Google Scholar] [CrossRef]
- Brehm, J.W. A Theory of Psychological Reactance; Academic Press: Oxford, UK, 1966. [Google Scholar]
- Brehm, J.W.; Brehm, S.S. Psychological Reactance: A Theory Offeedom and Control; Academic Press: San Diego, CA, USA, 1981. [Google Scholar]
- Dowd, E.T.; Wallbrown, F. Motivational Components of Client Reactance. J. Couns. Dev. 1993, 71, 533–538. [Google Scholar] [CrossRef]
- Joubert, C.E. Relationship among Self-Esteem, Psychological Reactance, and Other Personality Variables. Psychol. Rep. 1990, 66, 147–151. [Google Scholar] [CrossRef]
- Hockenberry, S.L.; Billingham, R.E. Psychological Reactance and Violence within Dating Relationships. Psychol. Rep. 1993, 73, 1203–1208. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.M.; Faedda, S. Refinement of the Hong Psychological Reactance Scale. Educ. Psychol. Meas. 1996, 56, 173–182. [Google Scholar] [CrossRef]
- Organización Mundial de la Salud. Constitución de La Organización Mundial de La Salud, 45th ed.; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Belloc, N.B.; Breslow, L. Relationship of Physical Health Status and Health Practices. Prev. Med. 1972, 1, 409–421. [Google Scholar] [CrossRef]
- Pozo, C.; Garzón, A.; Charry, C.; Bretones, B. Psychometric Properties and Dimensionality of the “Flourishing Scale” in Spanish-Speaking Population. Electr. J. Res. Educ. Psychol. 2016, 14, 175–192. [Google Scholar] [CrossRef] [Green Version]
- Seligman, M.E.P. Flourishing: A New Understanding of Happiness and Well-Being–and How to Achieve Them; Nicholas Brealey Publishing: Boston, MA, USA, 2011. [Google Scholar]
- Dallo, F. Predictors of Self-Rated Health among Undergraduate College Students in the United States. Coll. Stud. J. 2018, 52, 431–440. [Google Scholar]
- De Mendonca Freire, L.; Dalamaria, T.; de Aguino Cunha, M.; Florencio de Souza, O. Self-Rated Health in University Students from Rio Branco in the Estern Brazilian Amazon. Health 2014, 6, 2245–2249. [Google Scholar] [CrossRef] [Green Version]
- Vaez, M.; Kristenson, M.; Laflamme, L. Perceived Quality of Life and Self-Rated Health among First-Year University Students. Soc. Indic. Res. 2004, 68, 221–234. [Google Scholar] [CrossRef]
- Howell, A.J. Flourishing: Achievement-Related Correlates of Students’ Well-Being. J. Posit. Psychol. 2009, 4, 1–13. [Google Scholar] [CrossRef]
- Barra, E. Social Support, Stress and Health. Psicología Salud 2004, 14, 237–243. [Google Scholar] [CrossRef]
- Miller, W.R.; Brown, J.M. Self-Regulation as a Conceptual Basis for the Prevention and Treatment of Addictive Behaviours. In Self-Control. and the Addictive Behaviours; Heather, W.R., Miller, W.R., Greeley, J., Eds.; Maxwell Macmillan Publishing Australia: Sydney, NSW, Australia, 1991; pp. 3–79. [Google Scholar]
- Pichardo, C.; Justicia, F.; de la Fuente, J.; Martínez-Vicente, J.M.; Berbén, A.B. Factor Structure of the Self-Regulation Questionnaire (SRQ) at Spanish Universities. Span. J. Psychol. 2014, 17, 1–8. [Google Scholar] [CrossRef]
- Pichardo, M.C.; Cano, F.; Garzón, A.; de la Fuente, J.; Peralta, F.J.; Amate, J. Self-Regulation Questionnaire (SRQ) in Spanish Adolescents: Factor Structure and Rasch Analysis. Front. Psychol. 2018, 9, 1370. [Google Scholar] [CrossRef] [Green Version]
- Ato, M.; López, J.; Benavente, A. Un Sistema de Clasificación de Los Diseños de Investigación En Psicología. An. Psicol. 2013, 29, 1038–1059. [Google Scholar] [CrossRef] [Green Version]
- Tabachnick, B.G.; Fidell, L.S. Principal Components and Factor Analysis. Using Multivar. Stat. 2001, 4, 582–633. [Google Scholar]
- Lohr, S. Sampling: Design and Analysis; Cengage Learning: Boston, MA, USA, 1999. [Google Scholar]
- Weston, R.; Gore, P.A. A Brief Guide to Structural Equation Modeling. Couns. Psychol. 2006, 34, 719–751. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; The Guilford Press: New York, NY, USA, 2005. [Google Scholar]
- Rodríguez, M.N. Indicadores de Rendimiento de Estudiantes Universitarios: Calificaciones versus Créditos Acumulados. Rev. Educ. 2011, 355, 467–492. [Google Scholar] [CrossRef]
- Mardia, K.V. Measures of Multivariate Skewness and Kurtosis with Applications. Biometrika 1970, 57, 519–530. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Modeling 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Jöreskog, K.G.; Sörbom, D. LISREL 8: Structural Equation Modeling with the SIMPLIS Command Language; Scientific Software International: Lincolnwood, IL, USA, 1993. [Google Scholar]
- Flora, D.B.; Curran, P.J. An Empirical Evaluation of Alternative Methods of Estimation for Confirmatory Factor Analysis with Ordinal Data. Psychol. Methods 2004, 9, 466–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IBM. SPSS Statistics for Windows; IBM Corp.: Armonk, NY, USA, 2019. [Google Scholar]
- Arbuckle, J.L. Amos (Version 23.0); IBM SPSS: Chicago, IL, USA, 2014. [Google Scholar]
- De la Fuente, J.; Amate, J.; Sander, P. Relationships between Cognitive Strategies, Motivational Strategies and Academic Stress in Professional Examination Candidates. Electron. J. Res. Educ. Psychol. 2018, 16. [Google Scholar] [CrossRef] [Green Version]
- Avarzamani, L.; Hosein Mozafarian, M.; Shahmiri Barzoki, H.; Mohsen Rahnejat, A.; Ebrahimi, M. Comparison of Emotional Intelligence in Young Male Patients with Borderline Personality Disorder or Traits and Healthy Controls. In Professional Psychology: Research and Practice; American Psychological Association: Worcester, MA, USA, 2021. [Google Scholar]
- Wegmann, E.; Brand, M. Affective and cognitive processes involved in behavioral addictions. Addict. Behav. 2021, 118. [Google Scholar] [CrossRef]
- Freeman, N.; Muraven, M. Self-control depletion leads to increased risk taking. Soc. Psychol. Personal. Sci. 2010, 1, 175–181. [Google Scholar] [CrossRef] [Green Version]
- Friese, M.; Engeler, M.; Florack, A. Self-perceived successful weight regulators are less affected by self-regulatory depletion in the domain of eating behavior. Eat. Behav. 2015, 16, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Kedia, S.; Ahuja, N.; Wyant, D.K.; Dillon, P.J.; Akkus, C.; Relyea, G. Compositional and contextual factors associated with drug overdose deaths in the United States. J. Addict. Dis. 2020, 1–10. [Google Scholar] [CrossRef]
- Weiss, N.H.; Sullivan, T.P.; Tull, M.T. Explicating the role of emotion dysregulation in risky behaviors: A review and synthesis of the literature with directions for future research and clinical practice. Curr. Opin. Psychol. 2015, 3, 22–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Carroll, R.E. Self-Regulation Interventions—What Do We Know and Where Should We Go? Health Psychol. Rev. 2020, 14, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Van den Toren, S.J.; van Grieken, A.; de Kroon, M.L.; Mulder, W.C.; Vanneste, Y.T.; Raat, H. Young Adults’ Self-Sufficiency in Daily Life: The Relationship with Contextual Factors and Health Indicators. BMC Psychol. 2020, 8, 89. [Google Scholar] [CrossRef] [PubMed]
- Powers, J.P.; Moshontz, H.; Hoyle, R.H. Self-Control and Affect Regulation Styles Predict Anxiety Longitudinally in University Students. Collabra Psychol. 2020, 6, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Carbone, J.T. Allostatic Load and Mental Health: A Latent Class Analysis of Physiological Dysregulation. Stress Int. J. Biol. Stress 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wiss, D.A.; Avena, N.; Gold, M. Food addiction and psychosocial adversity: Biological embedding, contextual factors, and public health implications. Nutrients 2020, 12, 3521. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Kim, H.; Carney, J.V.; Chung, K.S.; Hazler, R.J. Individual and Contextual Factors Associated with School Connectedness in the Context of Counseling in Schools. J. Couns. Dev. 2020, 98, 391–401. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics of Health Behavior Regulation | (1) Self-Regulated Health (SRH) POSITIVE PRO-ACTIVITY (+1) | (2) Non-Regulated Health (NRH) RE-ACTIVITY (0) | (3) Dys-Regulated Health (DRH) NEGATIVE PRO-ACTIVITY (−1) |
|---|---|---|---|
| Before (planning) Self-analysis Self-defined goals Self-motivation | Before (no planning) No self-analysis No goals No motivation | Before (planning amiss) Erroneous self-analysis Erroneous goals Self-demotivation | |
| During (self-monitoring) Self-observation Self-analysis Self-correction | During (no monitoring) No self-observation No self-analysis No self-correction | During (misguided monitoring) Self-distraction Cognitive self-avoidance Self-handicapping, procrastination | |
| After (self-assessment) Personal reflection Self-attributions Positive self-affect | After (no assessment) No reflection No attributions Indifferent in affect | After (misguided assessment) Erroneous self-assessment Erroneous self-attributions Negative self-affect | |
| Type of Activity | Self-Regulated Health (SRH) | Non-Regulated Health (NRH) | Dys-Regulated Health (DRH) |
| Health Behavior | SR Health | No norms/limits | Self-induced excesses/deficits |
| Characteristics of the External Regulatory Context | 1. External Regulation of Health (ERH) POSITIVE PROACTIVITY (+1) | 2. External Non-Regulation of Health (ENH) NEUTRAL (0) | 3. External Dys-Regulation of Health (EDH) NEGATIVE PRO-ACTIVITY (−1) |
|---|---|---|---|
| Before (planning) Introduces tasks Favors well-adjusted goals Favors self-motivation | Before (no planning) Does not present tasks Does not suggest goals Does not induce motivation | Before (planning amiss) Erroneous tasks Favors self-handicapping goals Induces demotivation | |
| During (favors monitoring) Promotes self-observation Promotes self-analysis Promotes self-correction | During (indifferent) No self-observation No self-analysis No self-correction | During (discourages monitoring) Promotes self-distraction, Cognitive self-avoidance, Self-handicapping, Procrastination | |
| After (prompts assessment) Promotes self-reflection Promotes adjusted self-attributions Promotes positive adjusted self-affect | After (ignores assessment) No reflection No attributions Indifferent in affect | After (misguides assessment) Promotes erroneous self-assessment Erroneous self-attributions Promotes maladjusted self-affect | |
| Example: alcohol use Context (environmental characteristics) | Externally regulatory Norms/limits on consumption | Non-regulatory No norms/consequences | Dys-regulatory Encourages alcohol abuse |
| External Regulation | Self-Regulation | ||
|---|---|---|---|
| SRH (+1) | NRH (0) | DRH (−1) | |
| ERH (+1) | + | − | − |
| ENH (0) | − | + | − |
| EDH (−1) | − | + | + |
| Statistical Index | SR | SRH | NRH | DRH | ERH | ENH | EDH | REACT | SH |
|---|---|---|---|---|---|---|---|---|---|
| Mean | 3.437 | 3.576 | 2.670 | 2.564 | 3.497 | 2.480 | 2.254 | 2.657 | 3.571 |
| Mean Standard Error | 0.035 | 0.045 | 0.039 | 0.043 | 0.055 | 0.046 | 0.048 | 0.033 | 0.038 |
| Mode | 3.24 | 3.33 | 2.83 | 2.50 | 3.67 | 2.50 | 2.00 | 2.44 | 3.60 |
| Standard Deviation | 0.588 | 0.753 | 0.652 | 0.716 | 0.905 | 0.753 | 0.800 | 0.552 | 0.630 |
| Asymmetry | 0.088 | −0.168 | 0.182 | 0.091 | −0.359 | 0.318 | 0.443 | 0.257 | −0.262 |
| Standard asymmetry error | 0.149 | 0.149 | 0.149 | 0.149 | 0.149 | 0.149 | 0.149 | 0.149 | 0.149 |
| Kurtosis | −0.480 | −0.143 | −0.062 | −0.345 | −0.157 | −0.180 | −0.214 | 0.263 | −0.079 |
| Standard kurtosis error | 0.296 | 0.296 | 0.297 | 0.297 | 0.296 | 0.297 | 0.296 | 0.296 | 0.296 |
| Range | 3.09 | 3.67 | 3.50 | 3.67 | 4.00 | 3.83 | 3.67 | 3.25 | 3.30 |
| Minimum | 1.86 | 1.33 | 1.17 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.70 |
| Maximum | 4.95 | 5.00 | 4.67 | 4.67 | 5.00 | 4.83 | 4.67 | 4.25 | 5.00 |
| Variables | SR | SRH | NRH | DRH | ERH | ENH | EDH |
|---|---|---|---|---|---|---|---|
| SR | |||||||
| SRH | 405 *** | ||||||
| NRH | −0.321 *** | −0.418 *** | |||||
| DRH | −0.140 * | −0.018 | 0.321 *** | ||||
| ERH | 365 *** | 310 *** | −0.016 | −0.097 | |||
| ENH | −0.341 *** | −0.139 * | 0.395 *** | −0.394 *** | −0.336 *** | ||
| EDH | −0.231 *** | 0.032 | 0.245 *** | 0.492 ** | −0.211 ** | 0.499 *** |
| Variable | SRH | NRH | DRH | ERH | ENH | EDH | REACT | SH |
|---|---|---|---|---|---|---|---|---|
| REACTAN | −0.035 | 0.106 | 0.341 *** | −0.232 *** | 0.285 *** | 0.284 *** | ||
| SH | 183 ** | −0.123 * | −0.113 | 0.252 *** | −0.201 ** | −0.156 * | −0.151 * |
| Model | Chi2 | DF | CH/df | SRMR | p< | NFI | RFI | IFI | TLI | CFI | RMSEA | HOELT 0.05 | HOELT 0.01 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 227.217 | 51 | 4.455 | 0.12 | 0.001 | 0.798 | 0.735 | 0.724 | 0.876 | 0.823 | 0.086 | 81 | 92 |
| 2 | 227.217 | 51 | 4.455 | 0.12 | 0.001 | 0.810 | 0.889 | 0.820 | 834 | 0.818 | 0.084 | 181 | 192 |
| 3 | 2028.759 | 932 | 2.77 | 0.05 | 0.001 | 0.944 | 0.904 | 0.970 | 0.938 | 0.965 | 0.064 | 133 | 137 |
| Variables | F1 (SRH) | F2 (NRH) | F3 (DRH) | F4 (ERH) | F5 (ENH) | F6 (EDH) | SR | REACT | SH |
|---|---|---|---|---|---|---|---|---|---|
| F1 | 0.316 | ||||||||
| F2 | −0.550 | 0.433 | |||||||
| F3 | 0.203 | 0.584 | |||||||
| F4 | |||||||||
| F5 | −0.409 | ||||||||
| F6 | 0.604 | ||||||||
| SR | 0.440 | 0.226 | −0.322 | ||||||
| REACT | 0.543 | −0.208 | |||||||
| SH | 0.790 | ||||||||
| SRERH1 | 0.719 | ||||||||
| SHERH2 | 0.771 | ||||||||
| SRERH3 | 0.719 | ||||||||
| SRERH4 | 0.684 | ||||||||
| SRERH5 | 0.692 | ||||||||
| SRERH6 | 0.579 | ||||||||
| SRERH7 | 0.568 | ||||||||
| SRERH8 | −0.212 | ||||||||
| SRERH9 | 0.457 | ||||||||
| SRERH10 | 0.527 | ||||||||
| SRERH11 | 0.747 | ||||||||
| SRERH12 | 0.471 | ||||||||
| SRERH13 | 0.589 | ||||||||
| SRERH14 | 0.226 | ||||||||
| SRERH15 | 0.481 | ||||||||
| SRERH16 | 0.549 | ||||||||
| SRERH17 | 0.609 | ||||||||
| SRERH18 | 0.566 | ||||||||
| SRERH19 | 0.768 | ||||||||
| SRERH20 | 0.813 | ||||||||
| SRERH21 | 0.846 | ||||||||
| SRERH22 | 0.808 | ||||||||
| SRERH23 | 0.755 | ||||||||
| SHERH24 | 0.663 | ||||||||
| SRERH25 | 0.411 | ||||||||
| SRERH26 | 0.459 | ||||||||
| SRERH27 | 0.551 | ||||||||
| SRERH28 | 0.723 | ||||||||
| SRERH29 | 0.804 | ||||||||
| SRERH30 | 0.659 | ||||||||
| SRERH31 | 0.714 | ||||||||
| SRERH32 | 650 | ||||||||
| SRERH33 | 0.696 | ||||||||
| SRERH34 | 0.731 | ||||||||
| SRERH35 | 0.572 | ||||||||
| SRERH36 | 0.696 | ||||||||
| GOALS | 0.733 | ||||||||
| PERSEV | 0.712 | ||||||||
| DECIS | 0.448 | ||||||||
| MISTAKES | 0.654 | ||||||||
| REACT1 | 0.834 | ||||||||
| REACT2 | 0.533 | ||||||||
| REACT3 | 0.641 | ||||||||
| HEALTH1 | 0.497 | ||||||||
| HEALTH2 | 0.284 |
| Variables | F1 (SRH) | F2 (NRH) | F3 (DRH) | F4 (ERH) | F5 (ENH) | F6 (EDH) | SR | REACT | SH |
|---|---|---|---|---|---|---|---|---|---|
| F1 | |||||||||
| F2 | −0.351 | ||||||||
| F3 | −0.111 | −0.216 | 0.441 | ||||||
| F4 | |||||||||
| F5 | |||||||||
| F6 | 0.247 | ||||||||
| SR | 0.019 | −0.035 | −0.175 | 0.243 | −0.077 | −0.102 | |||
| REACT | −0.060 | 0.110 | −0.117 | 0.239 | 0.317 | ||||
| HEALTH | 0.363 | −0.028 | −0.138 | 0.371 | −0.061 | −0.081 | −0.254 | ||
| SRERH1 | 0.227 | ||||||||
| SHERH2 | 0.243 | ||||||||
| SRERH3 | 0.227 | ||||||||
| SHERH4 | 0.216 | ||||||||
| SRERH5 | 0.218 | ||||||||
| SRERH6 | 0.183 | ||||||||
| SRERH7 | −0.313 | −0.075 | 0.246 | ||||||
| SRERH8 | 0.117 | −0.160 | −0.092 | ||||||
| SRERH9 | −0.251 | −0.185 | 0.198 | ||||||
| SRERH10 | −0.290 | −0.262 | 0.228 | ||||||
| SRERH11 | −0.411 | −0.165 | 0.323 | ||||||
| SRERH12 | −0.259 | −0.165 | 0.204 | ||||||
| SRERH13 | −0.066 | 0.119 | −0.127 | 0.260 | 0.344 | ||||
| SRERH14 | −0.025 | 0.046 | −0.049 | 0.100 | 0.132 | ||||
| SRERH15 | −0.054 | 0.098 | −0.104 | 0.212 | 0.281 | ||||
| SRERH16 | −0.061 | 0.111 | −0.118 | 0.242 | 0.321 | ||||
| SRERH17 | −0.068 | 0.123 | −0.131 | 0.269 | 0.356 | ||||
| SRERH18 | −0.063 | 0.115 | −0.122 | 0.249 | 0.331 | ||||
| SRERH19 | 0.260 | 0.344 | |||||||
| SRERH20 | 0.100 | 0.132 | |||||||
| SRERH21 | |||||||||
| SRERH22 | |||||||||
| SRERH23 | |||||||||
| SHERH24 | |||||||||
| SRERH25 | −0.168 | ||||||||
| SRERH26 | −0.188 | ||||||||
| SRERH27 | −0.225 | ||||||||
| SRERH28 | −0.296 | ||||||||
| SRERH29 | −0.329 | ||||||||
| SRERH30 | −0.270 | ||||||||
| SRERH31 | −0.176 | 0.431 | |||||||
| SRERH32 | −0.161 | 0.393 | |||||||
| SRERH33 | −0.172 | 0.420 | |||||||
| SRERH34 | −0.181 | 0.442 | |||||||
| SRERH35 | −0.141 | 0.346 | |||||||
| SRERH36 | −0.162 | 0.396 | |||||||
| GOALS | 0.337 | −0.026 | −0.128 | 0.344 | −0.056 | −0.075 | |||
| PERSEV | 0.327 | −0.025 | −0.124 | 0.334 | −0.055 | −0.073 | −0.236 | ||
| DECIS | 0.206 | −0.016 | −0.078 | 0.210 | −0.035 | −0.046 | −0.229 | ||
| MISTAKES | 0.300 | −0.023 | −0.114 | 0.307 | −0.050 | −0.067 | −0.144 | ||
| REACT1 | −0.050 | 0.092 | 0.453 | −0.271 | 0.200 | 0.265 | −0.211 | ||
| REACT2 | −0.032 | 0.059 | 0.289 | −0.173 | 0.127 | 0.169 | |||
| REACT3 | −0.039 | 0.070 | 0.348 | −0.208 | 0.153 | 0.203 | |||
| HEALTH1 | 0.180 | −0.014 | −0.069 | 0.185 | −0.040 | −0.040 | 0.393 | −0.127 | |
| HEALTH2 | 0.103 | −0.008 | −0.039 | 0.105 | −0.023 | −0.023 | 0.224 | −0.072 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pachón-Basallo, M.; de la Fuente, J.; Gonzáles-Torres, M.C. Regulation/Non-Regulation/Dys-Regulation of Health Behavior, Psychological Reactance, and Health of University Undergraduate Students. Int. J. Environ. Res. Public Health 2021, 18, 3793. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073793
Pachón-Basallo M, de la Fuente J, Gonzáles-Torres MC. Regulation/Non-Regulation/Dys-Regulation of Health Behavior, Psychological Reactance, and Health of University Undergraduate Students. International Journal of Environmental Research and Public Health. 2021; 18(7):3793. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073793
Chicago/Turabian StylePachón-Basallo, Mónica, Jesús de la Fuente, and María Carmen Gonzáles-Torres. 2021. "Regulation/Non-Regulation/Dys-Regulation of Health Behavior, Psychological Reactance, and Health of University Undergraduate Students" International Journal of Environmental Research and Public Health 18, no. 7: 3793. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073793