
Modelling the Contribution of Metacognitions, Impulsiveness, and Thought Suppression to Behavioural Addictions in Adolescents



Abstract
:1. Introduction
1.1. Impulsiveness and the Suppression of Thoughts in Addictive Behaviors
1.2. Metacognitions as Drivers of Thought Suppression and Impulsiveness
1.3. Possible Confounding Effects for Religiosity and Gender in Behavioral Addictions
2. Study 1
2.1. Method
2.1.1. Participants
2.1.2. Self-Report Measures
Metacognitions
Impulsiveness
Thought Suppression
2.1.3. Internet Gaming Disorder
2.2. Procedure
2.3. Data Analysis
2.4. Results
2.4.1. Bivariate Correlations
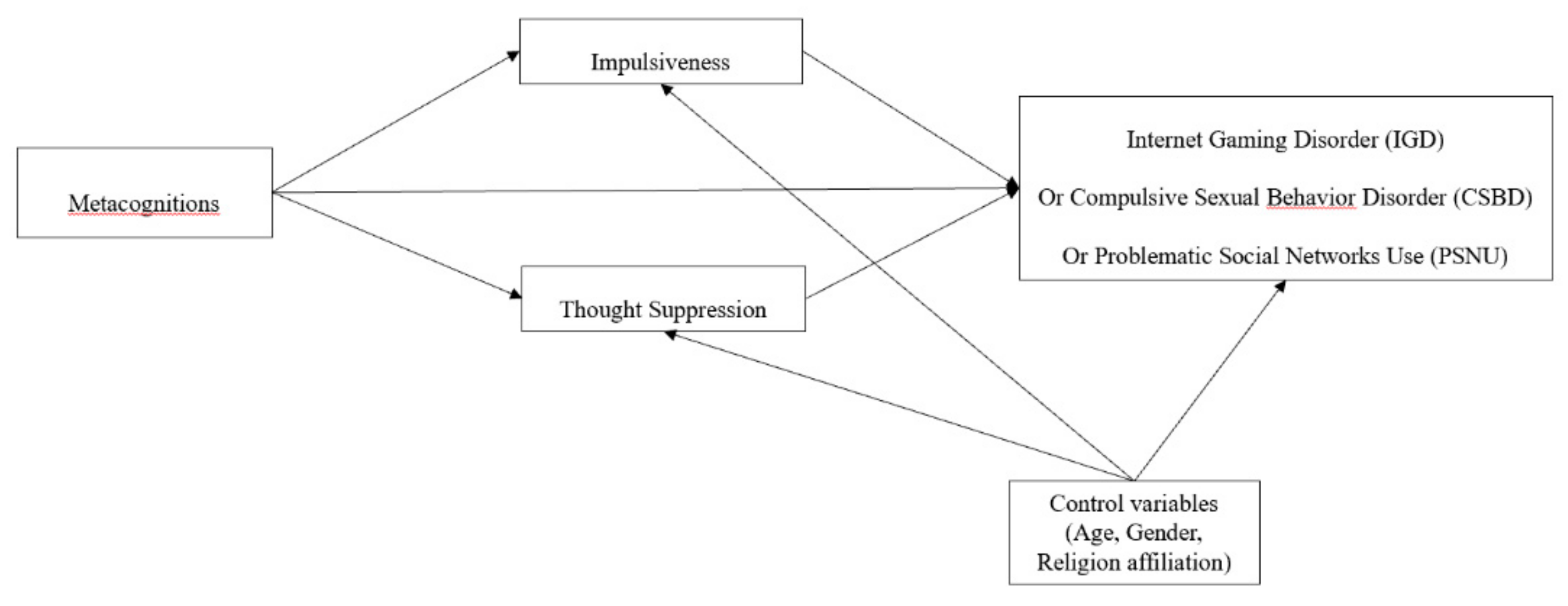
2.4.2. Path Analysis: Do Thought Suppression and Impulsiveness Mediate the Association between Metacognitions and IGD?
2.5. Discussion
3. Study 2
3.1. Method
3.1.1. Participants
3.1.2. Self-Report Measures
Metacognitions
Impulsiveness
Thought Suppression
Compulsive Sexual Behavior Disorder
3.2. Procedure
3.3. Data Analysis
3.4. Results
3.4.1. Bivariate Correlations
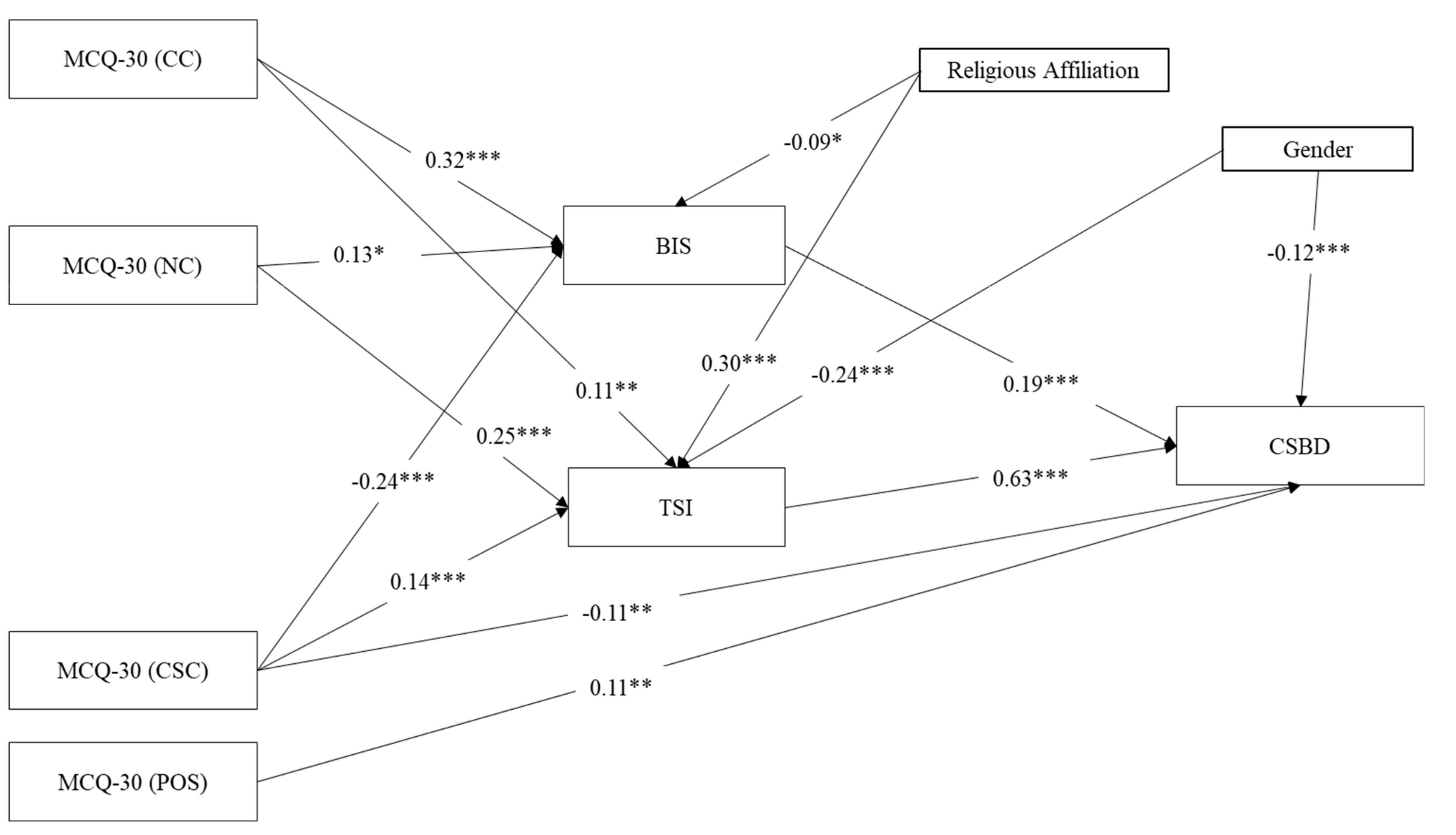
3.4.2. Path Analysis: Do Thought Suppression and Impulsiveness Mediate the Association between Metacognitions and CSBD?
3.5. Discussion
4. Study 3
4.1. Method
4.1.1. Participants
4.1.2. Self-Report Measures
Metacognitions
Impulsiveness
Thought Suppression
Problematic Social Networks Use
4.2. Procedure
4.3. Data Analysis
4.4. Results
4.4.1. Bivariate Correlations
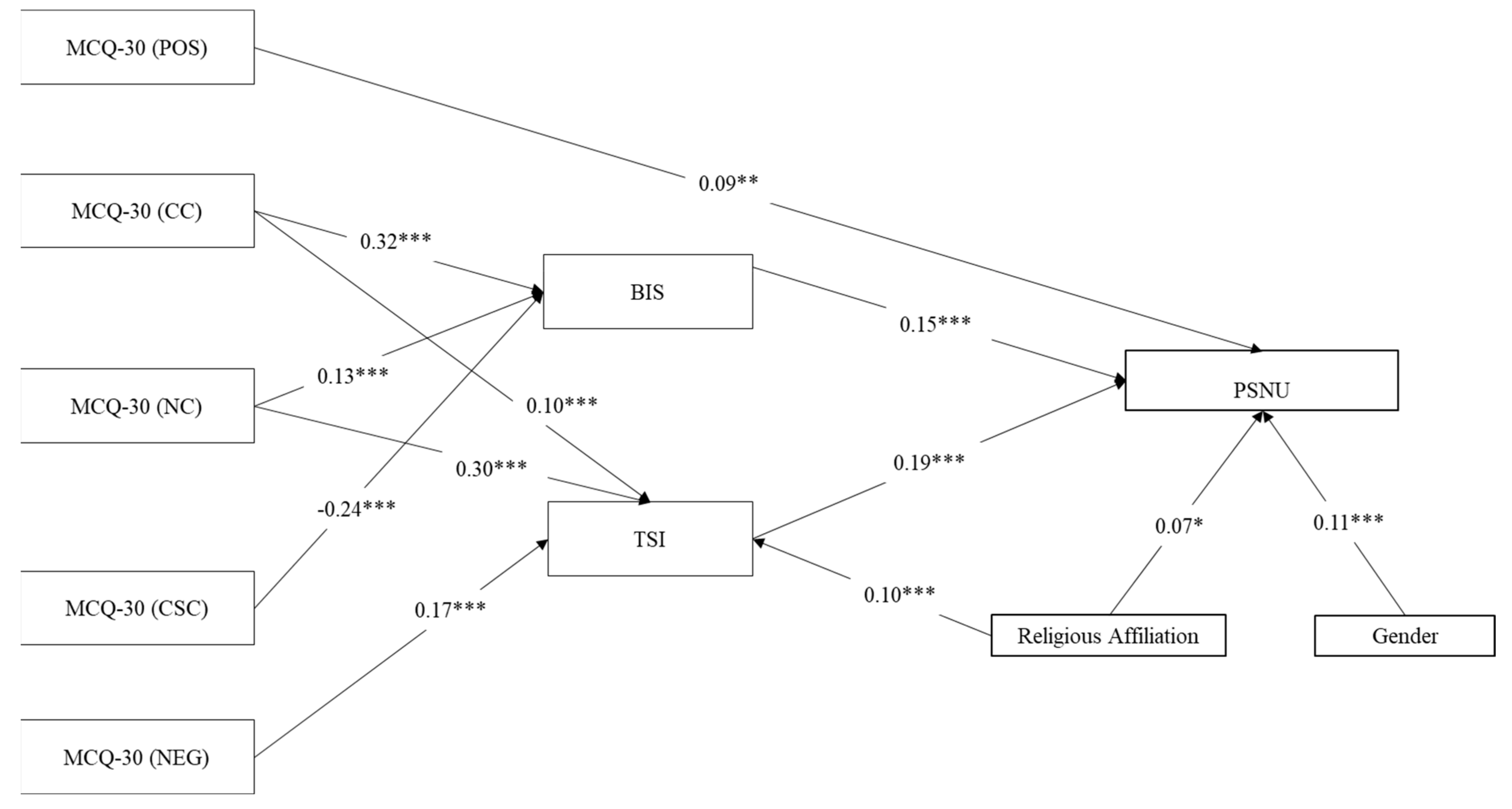
4.4.2. Path Analysis: Do Thought Suppression and Impulsiveness Mediate the Association between Metacognitions and PSNU?
5. Discussion
5.1. General Summary Discussion
5.2. Therapeutic Implications of the Current Research
5.3. Limitations
6. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Ethics Approval
Informed Consent
References
- World Health Organization. International Classification of Diseases for Mortality and Morbidity Statistics-Eleventh Revision (ICD-11); World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Yau, M.Y.H.; Potenza, M.N. Gambling disorder and other behavioral addictions: Recognition and treatment. Harv. Rev. Psychiatry 2015, 23, 134. [Google Scholar] [CrossRef] [PubMed]
- Paulus, F.W.; Ohmann, S.; Von Gontard, A.; Popow, C. Internet gaming disorder in children and adolescents: A systematic review. Dev. Med. Child Neurol. 2018, 60, 645–659. [Google Scholar] [CrossRef] [PubMed]
- Efrati, Y.; Dannon, P. Normative and clinical self-perceptions of sexuality and their links to psychopathology among adolescents. Psychopathology 2018, 51, 380–389. [Google Scholar] [CrossRef]
- Efrati, Y.; Gola, M. Understanding and predicting profiles of compulsive sexual behavior among adolescents. J. Behav. Addict. 2018, 7, 1004–1014. [Google Scholar] [CrossRef]
- Andreassen, C.S. Online social network site addiction: A comprehensive review. Curr. Addict. Rep. 2015, 2, 175–184. [Google Scholar] [CrossRef]
- Li, J.B.; Wu, A.M.; Feng, L.F.; Deng, Y.; Li, J.H.; Chen, Y.X.; Mo, P.K.H.; Lau, J.T. Classification of probable online social networking addiction: A latent profile analysis from a large-scale survey among Chinese adolescents. J. Behav. Addict. 2020, 9, 698–708. [Google Scholar] [CrossRef]
- Ryan, T.; Chester, A.; Reece, J.; Xenos, S. The uses and abuses of Facebook: A review of Facebook addiction. J. Behav. Addict. 2014, 3, 133–148. [Google Scholar] [CrossRef] [Green Version]
- Gola, M.; Potenza, M.N. Promoting educational, classification, treatment, and policy initiatives: Commentary on: Compulsive sexual behaviour disorder in the ICD-11 (Kraus et al., 2018). J. Behav. Addict. 2018, 7, 208–210. [Google Scholar] [CrossRef]
- Kafka, M.P. Hypersexual disorder: A proposed diagnosis for DSM-V. Arch. Sex. Behav. 2010, 39, 377–400. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. ICD-11 (Mortality and Morbidity Statistics). 6C72 Compulsive Sexual Behaviour Disorder. 2018. Available online: https://icd.who.int/dev11/lm/en#/http://id.who.int/icd/entity/1630268048 (accessed on 1 September 2019).
- Kraus, S.W.; Krueger, R.B.; Briken, P.; First, M.B.; Stein, D.J.; Kaplan, M.S.; Voon, V.; Abdo, C.H.N.; Grant, J.E.; Atalla, E.; et al. Compulsive sexual behaviour disorder in the ICD-11. World Psychiatry 2018, 17, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraus, S.W.; Voon, V.; Potenza, M.N. Should compulsive sexual behavior be considered an addiction? Addiction 2016, 111, 2097–2106. [Google Scholar] [CrossRef]
- Potenza, M.N.; Gola, M.; Voon, V.; Kor, A.; Kraus, S.W. Is excessive sexual behaviour an addictive disorder? Lancet Psychiatry 2017, 4, 663–664. [Google Scholar] [CrossRef] [Green Version]
- Miller, W.R.; Forcehimes, A.A.; Zweben, A. Treating Addiction: A Guide for Professionals, 2nd ed.; The Guilford Press: New York, NY, USA, 2019. [Google Scholar]
- Grant, J.E.; Potenza, M.N.; Weinstein, A.; Gorelick, D.A. Introduction to behavioral addictions. Am. J. Drug Alcohol. Abus. 2010, 36, 233–241. [Google Scholar] [CrossRef] [Green Version]
- Wines, D. Exploring the applicability of criteria for substance dependence to sexual addiction. Sex. Addict. Compuls. J. Treat. Prev. 1997, 4, 195–220. [Google Scholar] [CrossRef]
- Bőthe, B.; Tóth-Király, I.; Griffiths, M.D.; Potenza, M.N.; Orosz, G.; Demetrovics, Z. Are sexual functioning problems associated with frequent pornography use and/or problematic pornography use? Results from a large community survey including males and females. Addict. Behav. 2021, 112, 106603. [Google Scholar] [CrossRef]
- Hormes, J.M.; Kearns, B.; Timko, C.A. Craving F acebook? Behavioral addiction to online social networking and its association with emotion regulation deficits. Addictive 2014, 109, 2079–2088. [Google Scholar] [CrossRef] [PubMed]
- Kuss, D.J.; Griffiths, M.D. Online social networking and addiction—A review of the psychological literature. Int. J. Environ. Res. Public Health 2011, 8, 3528–3552. [Google Scholar] [CrossRef] [Green Version]
- Wise, K.; Alhabash, S.; Park, H. Emotional responses during social information seeking on Facebook. Cyberpsychol. Behav. Soc. Netw. 2010, 13, 555–562. [Google Scholar] [CrossRef] [Green Version]
- Pontes, H.M.; Schivinski, B.; Sindermann, C.; Li, M.; Becker, B.; Zhou, M.; Montag, C. Measurement and conceptualization of Gaming Disorder according to the World Health Organization framework: The development of the Gaming Disorder Test. Int. J. Ment. Health Addict. 2019, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Wenzlaff, R.M.; Wegner, D.M. Thought suppression. Annu. Rev. Psychol. 2000, 51, 59–91. [Google Scholar] [CrossRef]
- Brockman, R.; Ciarrochi, J.; Parker, P.; Kashdan, T. Emotion regulation strategies in daily life: Mindfulness, cognitive reappraisal and emotion suppression. Cogn. Behav. Ther. 2017, 46, 91–113. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.J.; John, O.P. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. J. Personal. Soc. Psychol. 2003, 85, 348. [Google Scholar] [CrossRef]
- Abramowitz, J.S.; Tolin, D.F.; Street, G.P. Paradoxical effects of thought suppression: A meta-analysis of controlled studies. Clin. Psychol. Rev. 2001, 21, 683–703. [Google Scholar] [CrossRef]
- Wenzlaff, R.M.; Luxton, D.D. The role of thought suppression in depressive rumination. Cogn. Ther. Res. 2003, 27, 293–308. [Google Scholar] [CrossRef]
- Efrati, Y. God, I can’t stop thinking about sex! The rebound effect in unsuccessful suppression of sexual thoughts among religious adolescents. J. Sex. Res. 2019, 56, 146–155. [Google Scholar] [CrossRef]
- Efrati, Y.; Kolubinski, C.D.; Caselli, G.; Spada, M.M. Desire thinking as a predictor of compulsive sexual behaviour in adolescents: Evidence from a cross-cultural validation of the Hebrew version of the Desire Thinking Questionnaire. J. Behav. Addict. 2020, 9, 797–807. [Google Scholar] [CrossRef]
- Gong, X.; Chen, C.; Lee, M.K. What drives problematic online gaming? The role of IT identity, maladaptive cognitions, and maladaptive emotions. Comput. Hum. Behav. 2020, 110, 106386. [Google Scholar] [CrossRef]
- Klein, A.A. Suppression-induced hyperaccessibility of thoughts in abstinent alcoholics: A preliminary investigation. Behav. Res. Ther. 2007, 45, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Erskine, J.A.; Ussher, M.; Cropley, M.; Elgindi, A.; Zaman, M.; Corlett, B. Effect of thought suppression on desire to smoke and tobacco withdrawal symptoms. Psychopharmacology 2012, 219, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Riley, B. Experiential avoidance mediates the association between thought suppression and mindfulness with problem gambling. J. Gambl. Stud. 2014, 30, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.A.; Hagger, M.S.; Chatzisarantis, N.L.D. Ironic Effects of Thought Suppression: A Meta-Analysis. Perspect. Psychol. Sci. 2020, 15, 778–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spada, M.M.; Caselli, G.; Nikčević, A.V.; Wells, A. Metacognition in addictive behaviors. Addict. Behav. 2015, 44, 9–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalley, J.W.; Everitt, B.J.; Robbins, T.W. Impulsivity, compulsivity, and top-down cognitive control. Neuron 2011, 69, 680–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Qiu, X.; Ren, Q.; Zhou, Z.; Zhou, H.; Du, J.; Voo, V.; Zhang, C.; Liu, W. Psychometric Properties of the Chinese version of UPPS-P Impulsive Behavior Scale. Front. Psychiatry 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Bőthe, B.; Tóth-Király, I.; Potenza, M.N.; Griffiths, M.D.; Orosz, G.; Demetrovics, Z. Revisiting the role of impulsivity and compulsivity in problematic sexual behaviors. J. Sex. Res. 2019, 56, 166–179. [Google Scholar] [CrossRef] [Green Version]
- Wetterneck, C.T.; Burgess, A.J.; Short, M.B.; Smith, A.H.; Cervantes, M.E. The role of sexual compulsivity, impulsivity, and experiential avoidance in internet pornography use. Psychol. Rec. 2012, 62, 3–18. [Google Scholar] [CrossRef]
- Wegmann, E.; Müller, S.M.; Turel, O.; Brand, M. Interactions of impulsivity, general executive functions, and specific inhibitory control explain symptoms of social-networks-use disorder: An experimental study. Sci. Rep. 2020, 10, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Fumero, A.; Marrero, R.J.; Bethencourt, J.M.; Peñate, W. Risk factors of internet gaming disorder symptoms in Spanish adolescents. Comput. Hum. Behav. 2020, 111, 106416. [Google Scholar] [CrossRef]
- Castellani, B.; Rugle, L. A comparison of pathological gamblers to alcoholics and cocaine misusers on impulsivity, sensation seeking, and craving. Int. J. Addict. 1995, 30, 275–289. [Google Scholar] [CrossRef]
- Hartmann, A.; Zeeck, A.; Barrett, M.S. Interpersonal problems in eating disorders. Int. J. Eat. Disord. 2010, 43, 619–627. [Google Scholar] [CrossRef]
- Lee, R.S.; Hoppenbrouwers, S.; Franken, I. A systematic meta-review of impulsivity and compulsivity in addictive behaviors. Neuropsychol. Rev. 2019, 29, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Efrati, Y.; Gola, M. The effect of early life trauma on compulsive sexual behavior among members of a 12-step group. J. Sex. Med. 2019, 16, 803–811. [Google Scholar] [CrossRef]
- Efrati, Y.; Shukron, O.; Epstein, R. Compulsive sexual behavior and sexual offending: Differences in cognitive schemas, sensation seeking, and impulsivity. J. Behav. Addict. 2019, 8, 432–441. [Google Scholar] [CrossRef]
- Wells, A.; Matthews, G. Modelling cognition in emotional disorder: The S-REF model. Behav. Res. Ther. 1996, 34, 881–888. [Google Scholar] [CrossRef]
- Wells, A.; Matthews, G. Attention and emotion: A clinical perspective. Clin. Psycbol. Psychother 1994, 2, 134. [Google Scholar]
- Spada, M.M.; Proctor, D.; Caselli, G.; Strodl, E. Metacognition in substance misuse. Princ. Addict. Compr. Addict. Behav. Disord. 2013, 1, 355–362. [Google Scholar]
- Cartwright-Hatton, S.; Wells, A. Beliefs about worry and intrusions: The Meta-Cognitions Questionnaire and its correlates. J. Anxiety Disord. 1997, 11, 279–296. [Google Scholar] [CrossRef]
- Wells, A.; Cartwright-Hatton, S. A short form of the metacognitions questionnaire: Properties of the MCQ-30. Behav. Res. Ther. 2004, 42, 385–396. [Google Scholar] [CrossRef]
- Wells, A. Advances in metacognitive therapy. Int. J. Cogn. 2013, 6, 186–201. [Google Scholar] [CrossRef]
- Hamonniere, T.; Varescon, I. Metacognitive beliefs in addictive behaviours: A systematic review. Addict. Behav. 2018, 85, 51–63. [Google Scholar] [CrossRef]
- Akbari, M. Metacognitions or distress intolerance: The mediating role in the relationship between emotional dysregulation and problematic internet use. Addict. Behav. Rep. 2017, 6, 128–133. [Google Scholar] [CrossRef]
- Jauregui, P.; Urbiola, I.; Estevez, A. Metacognition in pathological gambling and its relationship with anxious and depressive symptomatology. J. Gambl. Stud. 2016, 32, 675–688. [Google Scholar] [CrossRef]
- Lindberg, A.; Fernie, B.A.; Spada, M.M. Metacognitions in problem gambling. J. Gambl. Stud. 2011, 27, 73–81. [Google Scholar] [CrossRef]
- Mansueto, G.; Pennelli, M.; De Palo, V.; Monacis, L.; Sinatra, M.; De Caro, M.F. The role of metacognition in pathological gambling: A mediation model. J. Gambl. Stud. 2016, 32, 93–106. [Google Scholar] [CrossRef]
- Mansueto, G.; Caselli, G.; Ruggiero, G.M.; Sassaroli, S. Metacognitive beliefs and childhood adversities: An overview of the literature. Psychol. Health Med. 2019, 24, 542–550. [Google Scholar] [CrossRef]
- Marino, C.; Vieno, A.; Moss, A.C.; Caselli, G.; Nikčević, A.V.; Spada, M.M. Personality, motives and metacognitions as predictors of problematic Facebook use in university students. Personal. Individ. Differ. 2016, 101, 70–77. [Google Scholar] [CrossRef] [Green Version]
- Moneta, G.B. Metacognition, emotion, and alcohol dependence in college students: A moderated mediation model. Addict. Behav. 2011, 36, 781–784. [Google Scholar] [CrossRef]
- Nikcevic, A.V.; Spada, M.M. Metacognitions across the continuum of smoking dependence. Behav. Cogn. Psychother. 2008, 36, 333. [Google Scholar] [CrossRef]
- Spada, M.M.; Mohiyeddini, C.; Wells, A. Measuring metacognitions associated with emotional distress: Factor structure and predictive validity of the Metacognitions Questionnaire 30. Personal. Individ. Differ. 2008, 45, 238–242. [Google Scholar] [CrossRef]
- Spada, M.M.; Marino, C. Metacognitions and emotion regulation as predictors of problematic internet use in adolescents. Clin. Neuropsychiatry 2017, 14, 59–63. [Google Scholar]
- Spada, M.M.; Nikčević, A.V.; Moneta, G.B.; Wells, A. Metacognition as a mediator of the relationship between emotion and smoking dependence. Addict. Behav. 2007, 32, 2120–2129. [Google Scholar] [CrossRef] [PubMed]
- Spada, M.M.; Roarty, A. The relative contribution of metacognitions and attentional control to the severity of gambling in problem gamblers. Addict. Behav. Rep. 2015, 1, 7–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spada, M.M.; Wells, A. Metacognitions, emotion and alcohol use. Clin. Psychol. Psycholther. 2005, 12, 150–155. [Google Scholar] [CrossRef]
- Spada, M.M.; Zandvoort, M.; Wells, A. Metacognitions in problem drinkers. Cogn. Res. 2007, 31, 709–716. [Google Scholar] [CrossRef]
- Aydın, O.; Güçlü, M.; Ünal-Aydın, P.; Spada, M.M. Metacognitions and emotion recognition in Internet Gaming Disorder among adolescents. Addict. Behav. Rep. 2020, 12, 100296. [Google Scholar] [PubMed]
- Marino, C.; Marci, T.; Ferrante, L.; Altoè, G.; Vieno, A.; Simonelli, A.; Spada, M.M. Attachment and problematic Facebook use in adolescents: The mediating role of metacognitions. J. Behav. Addict. 2019, 8, 63–78. [Google Scholar] [CrossRef]
- Miller, L.R.; Walshe, E.A.; McIntosh, C.W.; Romer, D.; Winston, F.K. “What Were They Thinking?”: Metacognition and Impulsivity Play a Role in Young Driver Risk-Taking. J. Psychiatry Behav. Sci. 2021, 4, 1048. [Google Scholar]
- Gomes, F.C.; de Andrade, A.G.; Izbicki, R.; Almeida, A.M.; de Oliveira, L.G. Religion as a protective factor against drug use among Brazilian university students: A national survey. Rev. Bras. Psiquiatr. 2013, 35, 29–37. [Google Scholar] [CrossRef] [Green Version]
- Hodge, D.R.; Andereck, K.; Montoya, H. The protective influence of spiritual-religious lifestyle profiles on tobacco use, alcohol use, and gambling. Soc. Work. Res. 2007, 31, 211–219. [Google Scholar] [CrossRef]
- Montgomery, B.E.; Stewart, K.E.; Bryant, K.J.; Ounpraseuth, S.T. Dimensions of religion, depression symptomatology, and substance use among rural African American cocaine users. J. Ethn. Subst. Abus. 2014, 13, 72–90. [Google Scholar] [CrossRef] [Green Version]
- Faigin, C.A.; Pargament, K.I.; Abu-Raiya, H. Spiritual struggles as a possible risk factor for addictive behaviors: An initial empirical investigation. Int. J. Psychol. Relig. 2014, 24, 201–214. [Google Scholar] [CrossRef]
- Grubbs, J.B.; Perry, S.L.; Wilt, J.A.; Reid, R.C. Pornography problems due to moral incongruence: An integrative model with a systematic review and meta-analysis. Arch. Sex. Behav. 2019, 48, 397–415. [Google Scholar] [CrossRef] [PubMed]
- Grubbs, J.B.; Perry, S.L. Moral incongruence and pornography use: A critical review and integration. J. Sex. Res. 2019, 56, 29–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Efrati, Y. Adolescent compulsive sexual behavior: Is it a unique psychological phenomenon? J. Sex. Marital. Ther. 2018, 44, 687–700. [Google Scholar] [CrossRef] [PubMed]
- Efrati, Y. A response to Pirutinsky’s (2019) religion and compulsive sexuality. J. Sex Res. 2019, 56, 144–145. [Google Scholar] [CrossRef] [PubMed]
- Grubbs, J.B.; Grant, J.T. Spirituality/Religion and Behavioral Addictions. In Handbook of Spirituality, Religion, and Mental Health; Academic Press: Cambridge, MA, USA, 2020; pp. 139–157. [Google Scholar]
- Braun, B.; Kornhuber, J.; Lenz, B. Gaming and religion: The impact of spirituality and denomination. J. Relig. Health 2016, 55, 1464–1471. [Google Scholar] [CrossRef] [PubMed]
- Kowalewska, E.; Gola, M.; Kraus, S.W.; Lew-Starowicz, M. Spotlight on Compulsive Sexual Behavior Disorder: A Systematic Review of Research on Women. Neuropsychaiatr. Dis. Treat. 2020, 16, 2025. [Google Scholar] [CrossRef]
- Peter, J.; Valkenburg, P.M. Adolescents and pornography: A review of 20 years of research. J. Sex. Res. 2016, 5, 509–531. [Google Scholar] [CrossRef] [Green Version]
- Efrati, Y.; Amichai-Hamburger, Y. Adolescents who solely engage in online sexual experiences are at higher risk for compulsive sexual behavior. Addict. Behav. 2021, 118, 106874. [Google Scholar] [CrossRef]
- Griffiths, M.D.; Kuss, J.D.; King, L.D. Video game addiction: Past, present and future. Curr. Psychol. Rev. 2012, 8, 308–318. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.S.; Han, D.H.; Kim, S.M.; Renshaw, P.F. Substance abuse precedes internet addiction. Addict. Beyond Behav. 2013, 38, 2022–2025. [Google Scholar] [CrossRef] [Green Version]
- Şaşmaz, T.; Öner, S.; Kurt, A.Ö.; Yapıcı, G.; Yazıcı, A.E.; Buğdaycı, R.; Şiş, M. Prevalence and risk factors of Internet addiction in high school students. Eur. J. Public Health 2014, 24, 15–20. [Google Scholar] [CrossRef] [Green Version]
- Sugaya, N.; Shirasaka, T.; Takahashi, K.; Kanda, H. Bio-psychosocial factors of children and adolescents with internet gaming disorder: A systematic review. Biopsychosoc. Med. 2019, 13, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Festl, R.; Scharkow, M.; Quandt, T. Problematic computer game use among adolescents, younger and older adults. Addiction 2013, 108, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Mihara, S.; Higuchi, S. Cross-sectional and longitudinal epidemiological studies of I nternet gaming disorder: A systematic review of the literature. Psychol. Clin. Neuropsychiatry 2017, 71, 425–444. [Google Scholar]
- Peris, M.; de la Barrera, U.; Schoeps, K.; Montoya-Castilla, I. Psychological risk factors that predict social networking and internet addiction in adolescents. Int. J. Environ. Res. Public Health 2020, 17, 4598. [Google Scholar] [CrossRef] [PubMed]
- Patton, J.H.; Stanford, M.S.; Barratt, E.S. Factor structure of the Barratt Impulsiveness Scale. J. Clin. Psychol. 1995, 51, 768–774. [Google Scholar] [CrossRef]
- Glicksohn, J.; Leshem, R.; Aharoni, R. Impulsivity and time estimation: Casting a net to catch a fish. Personal. Individ. Differ. 2006, 40, 261–271. [Google Scholar] [CrossRef]
- Vasconcelos, A.G.; Malloy-Diniz, L.; Correa, H. Systematic review of psychometric proprieties of Barratt Impulsiveness Scale Version 11 (BIS-11). Clin. Neuropsychiatry 2012, 9, 61–74. [Google Scholar]
- Barnes, R.D.; Fisak, B.; Tantleff-Dunn, S. Validation of the Food Thought Suppression Inventory. J. Health Psychol. 2009, 15, 373–381. [Google Scholar] [CrossRef]
- Barnes, R.D.; White, M.A. Psychometric properties of the Food Thought Suppression Inventory in men. J. Health Psychol. 2010, 15, 1113–1120. [Google Scholar] [CrossRef]
- Pontes, H.M.; Griffiths, M.D. Measuring DSM-5 Internet gaming disorder: Development and validation of a short psychometric scale. Comput. Hum. Behav. 2015, 45, 137–143. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Health Disorders, 5th ed.; American Psychiatric Associat: Arlington, VA, USA, 2013. [Google Scholar]
- Qualtrics LLC. Qualtrics XM. 2019, Qualtrics, Provo. Available online: https://www.qualtrics.com/au/research-core/survey-software/ (accessed on 5 December 2020).
- IBM Corp. IBM SPSS Statistics for Windows; Version 25; IBM Corp.: Armonk, NY, USA, 2017. [Google Scholar]
- Rosseel, Y. Lavaan: An R package for structural equation modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing [Computer Software Manual]; R Core Team: Vienna, Austria, 2013; Available online: http://www.R-project.org/ (accessed on 1 October 2020).
- Satorra, A.; Bentler, P.M. Corrections to test statistics and standard errors in covariance structure analysis. In Latent Variable Analysis. Applications for Developmental Research; Von Eye, A., Clogg, C.C., Eds.; Sage: Thousand Oaks, CA, USA, 1994; pp. 399–419. [Google Scholar]
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173. [Google Scholar] [CrossRef]
- Hayes, A.F. Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Commun. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Bollen, K.A. Structural Equations with Latent Variables; Wiley: New York, NY, USA, 1989. [Google Scholar]
- Jöreskog, K.G.; Sörbom, D. LISREL 8: User’s Reference Guide; Scientific Software International: Chicago, IL, USA, 1996. [Google Scholar]
- Cohen, J. Statistical Power Analysis for Behavioral Science, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Marino, C.; Spada, M.M. Dysfunctional cognitions in online gaming and internet gaming disorder: A narrative review and new classification. Curr. Addict. Rep. 2017, 4, 308–316. [Google Scholar] [CrossRef]
- Sun, X.; Zhu, C.; So, S.H.W. Dysfunctional metacognition across psychopathologies: A meta-analytic review. Eur. Psychiatry 2017, 45, 139–153. [Google Scholar] [CrossRef]
- Wells, A. Emotional Disorders and Metacognition: Innovative Cognitive Therapy; Wiley: London, UK, 2000. [Google Scholar]
- Efrati, Y.; Mikulincer, M. Individual-based Compulsive Sexual Behavior Scale: Its development and importance in examining compulsive sexual behavior. J. Sex. Mar. Ther. 2018, 44, 249–259. [Google Scholar] [CrossRef]
- Efrati, Y.; Gola, M. Adolescents’ compulsive sexual behavior: The role of parental competence, parents’ psychopathology, and quality of parent–child communication about sex. J. Behav. Addict. 2019, 8, 420–431. [Google Scholar] [CrossRef]
- Efrati, Y.; Gola, M. Compulsive sexual behavior: A twelve-step therapeutic approach. J. Behav. Addict. 2018, 7, 445–453. [Google Scholar] [CrossRef]
- Efrati, Y.; Gerber, Z.; Tolmacz, R. The relation of intra-psychic and relational aspects of the self to compulsive sexual behavior. J. Sex. Marital. Ther. 2019, 45, 618–631. [Google Scholar] [CrossRef] [PubMed]
- Efrati, Y.; Shukron, O.; Epstein, R. Early Maladaptive Schemas Are Highly Indicative of Compulsive Sexual Behavior. Eval. Health Prof. 2020. [Google Scholar] [CrossRef]
- Van Den Eijnden, R.J.; Lemmens, J.S.; Valkenburg, P.M. The social media disorder scale. Comput. Hum. Behav. 2016, 61, 478–487. [Google Scholar] [CrossRef] [Green Version]
- Kolić-Vehovec, S.; Bajšanski, I.; Zubković, B.R. Metacognition and reading comprehension: Age and gender differences. In Trends and Prospects in Metacognition Research; Springer: Boston, MA, USA, 2010; pp. 327–344. [Google Scholar]
- Robichaud, M.; Dugas, M.J.; Conway, M. Gender differences in worry and associated cognitive-behavioral variables. J. Anxiety Disord. 2003, 17, 501–516. [Google Scholar] [CrossRef]
- Wells, A. Metacognitive Therapy for Anxiety and Depression; The Guilford Press: NewYork, NY, USA, 2009. [Google Scholar]
- Caselli, G.; Martino, F.; Spada, M.M.; Wells, A. Metacognitive therapy for alcohol use disorder: A systematic case series. Front. Psychol. 2018, 9, 2619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inchausti, F.; Ortuño-Sierra, J.; García-Poveda, N.V.; Ballesteros-Prados, A. Metacognitive abilities in adults with substance abuse treated in therapeutic community Habilidades metacognitivas en adultos con abuso de sustancias bajo tratamiento en comunidad terapéutica. Adicciones 2017, 29, 74–82. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IGD n = 471–474 | CSBD n = 453 | PSNU n = 1003 | |
|---|---|---|---|
| 1. Gender | |||
| Correlation | −0.26 ** | −0.28 ** | 0.13 ** |
| 2. Age | |||
| Correlation | −0.09 * | −0.09 | 0.05 |
| 3. Religious Affiliation | |||
| Correlation | 0.10 * | 0.15 ** | 0.09 ** |
| 4. MCQ-30 (POS) | |||
| Mean | 12.14 | 12.55 | 12.17 |
| Standard Deviation | 3.97 | 4.04 | 3.99 |
| Correlation | 0.12 * | 0.15 ** | 0.15 ** |
| 5. MCQ-30 (NEG) | |||
| Mean | 13.09 | 13.07 | 13.26 |
| Standard Deviation | 4.55 | 4.51 | 4.49 |
| Correlation | 0.15 ** | 0.14 ** | 0.15 ** |
| 6. MCQ-30 (CC) | |||
| Mean | 11.15 | 10.95 | 11.05 |
| Standard Deviation | 4.46 | 4.16 | 4.35 |
| Correlation | 0.22 ** | 0.24 ** | 0.15 ** |
| 7. MCQ-30 (NC) | |||
| Mean | 13.50 | 13.06 | 13.45 |
| Standard Deviation | 3.57 | 3.51 | 3.61 |
| Correlation | 0.17 ** | 0.28 ** | 0.13 ** |
| 8. MCQ-30 (CSC) | |||
| Mean | 16.95 | 16.70 | 16.72 |
| Standard Deviation | 3.86 | 4.11 | 4.03 |
| Correlation | 0.17 ** | 0.04 | 0.04 |
| 9. BIS | |||
| Mean | 65.67 | 66.84 | 67.33 |
| Standard Deviation | 10.05 | 10.55 | 11.24 |
| Correlation | 0.28 ** | 0.29 ** | 0.21 ** |
| 10. TSI | |||
| Mean | 26.48 | 37.13 | 32.83 |
| Standard Deviation | 12.70 | 14.97 | 14.31 |
| Correlation | 0.68 ** | 0.68 ** | 0.32 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Efrati, Y.; Kolubinski, D.C.; Marino, C.; Spada, M.M. Modelling the Contribution of Metacognitions, Impulsiveness, and Thought Suppression to Behavioural Addictions in Adolescents. Int. J. Environ. Res. Public Health 2021, 18, 3820. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073820
Efrati Y, Kolubinski DC, Marino C, Spada MM. Modelling the Contribution of Metacognitions, Impulsiveness, and Thought Suppression to Behavioural Addictions in Adolescents. International Journal of Environmental Research and Public Health. 2021; 18(7):3820. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073820
Chicago/Turabian StyleEfrati, Yaniv, Daniel C. Kolubinski, Claudia Marino, and Marcantonio M. Spada. 2021. "Modelling the Contribution of Metacognitions, Impulsiveness, and Thought Suppression to Behavioural Addictions in Adolescents" International Journal of Environmental Research and Public Health 18, no. 7: 3820. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073820