1. Introduction
In 2005, The Centre for Medicines in the Public Interests estimated that falsified medicines’ global market might be worth roughly 70 billion dollars (58 billion Euros) by 2010 [
1]. Recent data provided by the European Commission suggests that in 2015, customs officials seized about 40 million falsified drugs and estimated their value at 650 million Euros [
2]. The Food and Drug Administration (FDA) has stated that between 2007–2008, 246 people died due to a serious allergic adverse event resulting from using falsified heparin [
3]. It is worth mentioning that oncological drugs remain an important target of falsification, of which a good example is a bevacizumab (Avastin). In 2012, several batches of Avastin were falsified and did not contain any active pharmaceutical ingredients (API) [
4]. According to the WHO, nearly 64% of antimalarial drugs dispensed in Africa should be considered falsified [
5]. This problem has been observed not only in developing societies, but also in well-developed countries, which have at least, in theory, several protective mechanisms aimed at diminishing the dangers related to illegal drugs [
6,
7]. From a practical point of view, Poland, as a border country of the EU, remains a strategic place in preventing pharmaceutical crimes.
Consequently, the situation in Poland may have a direct impact on patient safety throughout Europe. In this context, it is worth recalling that in September 2016, near Bydgoszcz in central Poland, police discovered one of the first illegal pharmaceutical factories in Europe, and one of the largest in the world, and seized 430 thousand ampoules and tablets containing steroids and 100 thousand tablets for erectile dysfunction worth over 17 million PLN (Polish currency, approximately 4 million United States dollars) [
8]. Finally, falsified medications should be perceived as a matter of vital importance, highlighting the need for interprofessional collaboration between agencies dedicated to health promotion, law enforcement authorities, as well as those responsible for creating drug policy, which can be seen via the example of cooperation between the WHO, the UN Office of Drugs and Crime (UNODC), and Interpol [
9].
In light of this observation, we have identified in Europe intensified efforts to minimize the potential harm that the pandemic of falsified medications may cause to chronically ill patients, among others, those diagnosed with cardiovascular diseases. The new regulations, called the Falsified Medicines Directive (FMD), have recently been introduced in the European community. Thanks to these regulations, we can finally estimate the scale of the mentioned herein phenomenon throughout legal trade (particularly in community and hospital pharmacies). Secondly, it should ensure the safer profile of dispensed medications and increase access to more accurate data about routine drug dispensation [
10]. It should be added that apart from new responsibilities for producers and wholesalers, one of the most critical issues which the FMD has introduced is authentication, defined as verification of the drug authenticity before dispensing it to the patient. In this sense, the community pharmacy will be dedicated to protecting the patient from falsified drugs from the patient’s perspective. Additionally, authentication will also be introduced into the hospital setting, influencing workflow and possibly generating additional costs and human efforts [
11].
In light of the pandemic of falsified medications and recent legislative efforts, understanding the patient perspective on falsified medicines is warranted, both from the practical point of view and the impact on the current state of knowledge. Our study could be a starting point for designing educational initiatives to improve awareness of the risks related to falsified products among modern societies. The needs of patients suffering from cardiovascular diseases, particularly considering the epidemiology, should be regarded as especially important.
Our study aimed to investigate and understand the perspectives regarding falsified medications among patients diagnosed with cardiovascular diseases and then compare this perspective with patients not suffering from a chronic condition. The study also has educational value in that it contributes to improving patient knowledge about the phenomenon. Finally, our findings can also be understood in the context of public health and could be helpful for governments and other authorities responsible for drug policy in Europe.
4. Discussion
The presented study is the first example in the world of representative research conducted among participants with self-declared cardiovascular diseases aimed at defining the patients’ perspective on falsified (counterfeited) medicinal products. Implementation of a specific protocol based on the study (patients with self-declared cardiovascular diseases) and the control group (not chronically ill) should be considered a unique motive in social pharmacy and the social medicine disciplines. Recently, falsified drugs have become an essential topic in cardiology. Antignac et al. [
14] evaluated that amlodipine and captopril were the most frequently identified cardiovascular drugs with poor quality in Africa.
It should be noted that the results obtained from research conducted thus far have led to highly contradictory and incomplete information. This could be due to the lack of fair representation in prior research groups. In previous studies, one can find a juxtaposition of the healthcare professionals’ perspective compared to the layperson’s perspective. To the best of our knowledge, our study is the first scientific attempt to confront opinions on falsified medications among the chronically ill versus those not chronically ill [
15,
16]. In light of these observations, our research not only helps bridge the gap in current knowledge and remains attractive from a theoretical point of view, but also provides a strong practical background.
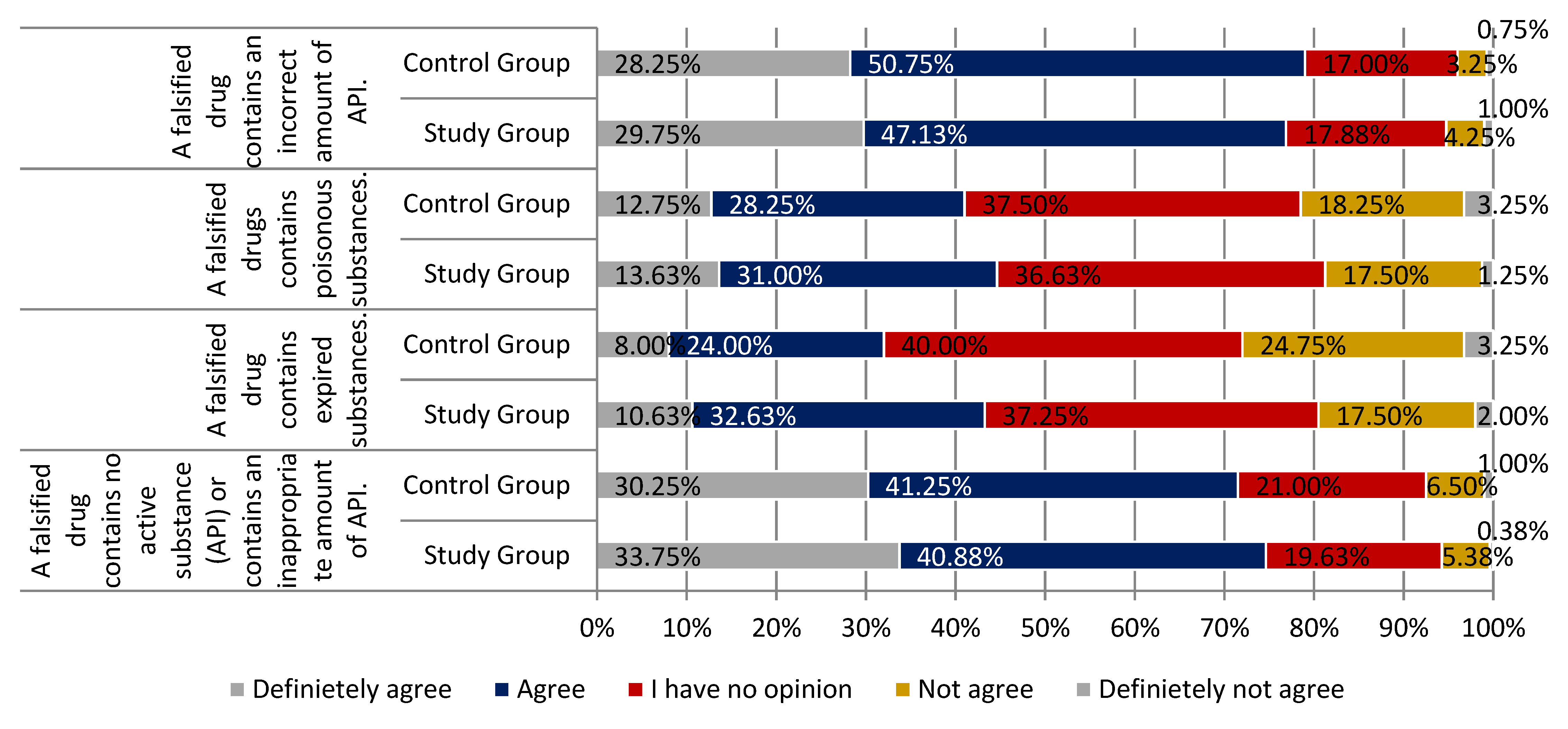
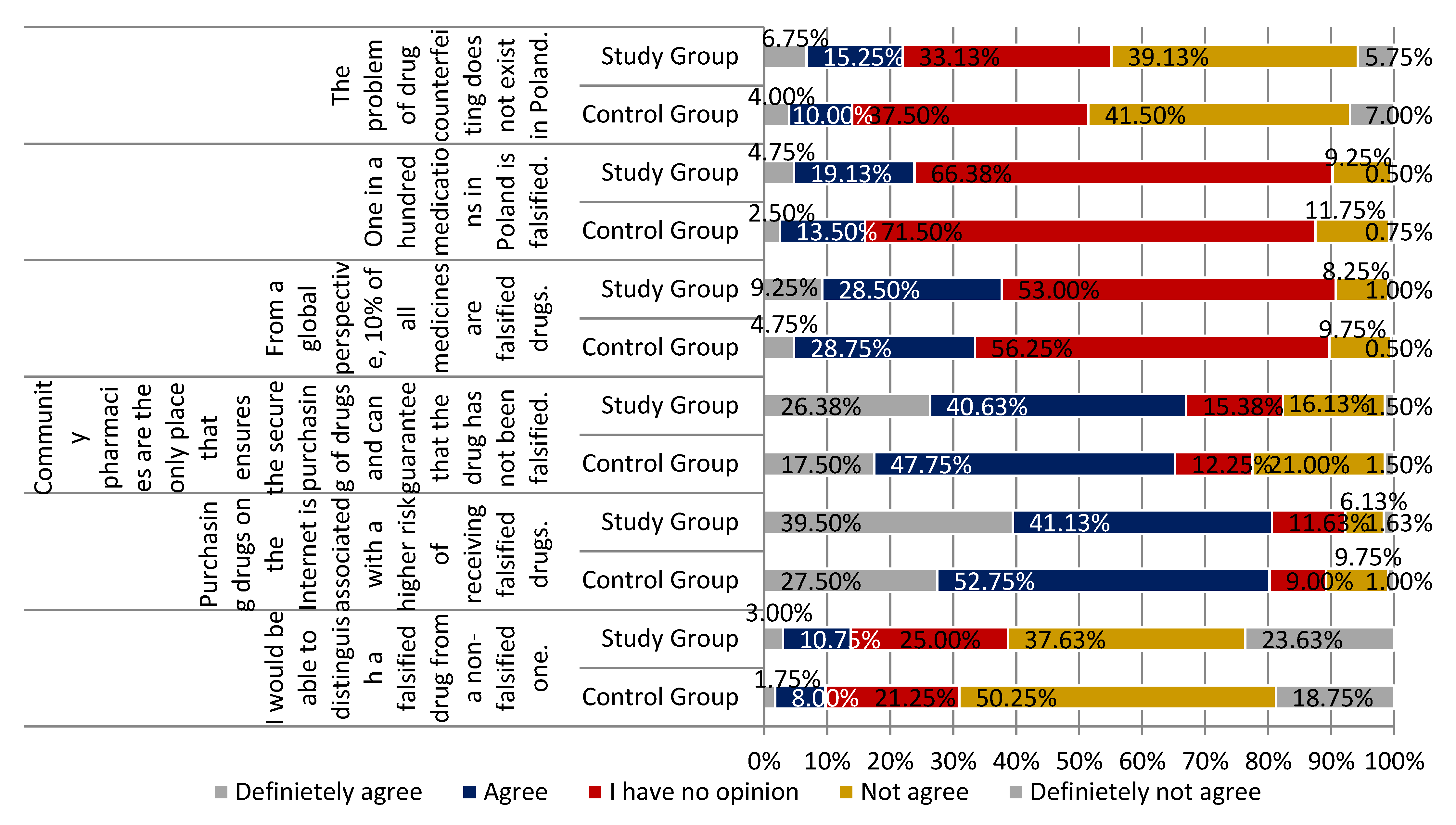
Respondents defined falsified medications as a product not containing an active pharmaceutical ingredient or an incorrect API quantity. Participants were sure about the higher risk associated with purchasing drugs on the Internet than in more traditional ways; however, respondents from the study group (self-declared occurrence of cardiovascular diseases) were more convinced of this. Indeed, online purchasing remains an important place for the distribution of falsified drugs [
17,
18]. These results are optimistic because most participants were aware of the existing dangers related to a non-traditional way of delivering medicinal products. These findings are essential in light of recent studies highlighting the almost unlimited accessibility of anabolic steroids and testosterone via the Internet. Such products are characterized by their very high potential of falsification [
19]. Purchasing medicinal products via the Internet remains the main reason for patients having drugs containing falsified API or not containing any active substances. Such a scenario was seen in Japan with anti-obesity products, where scientists identified sibutramine in the herbal supplements [
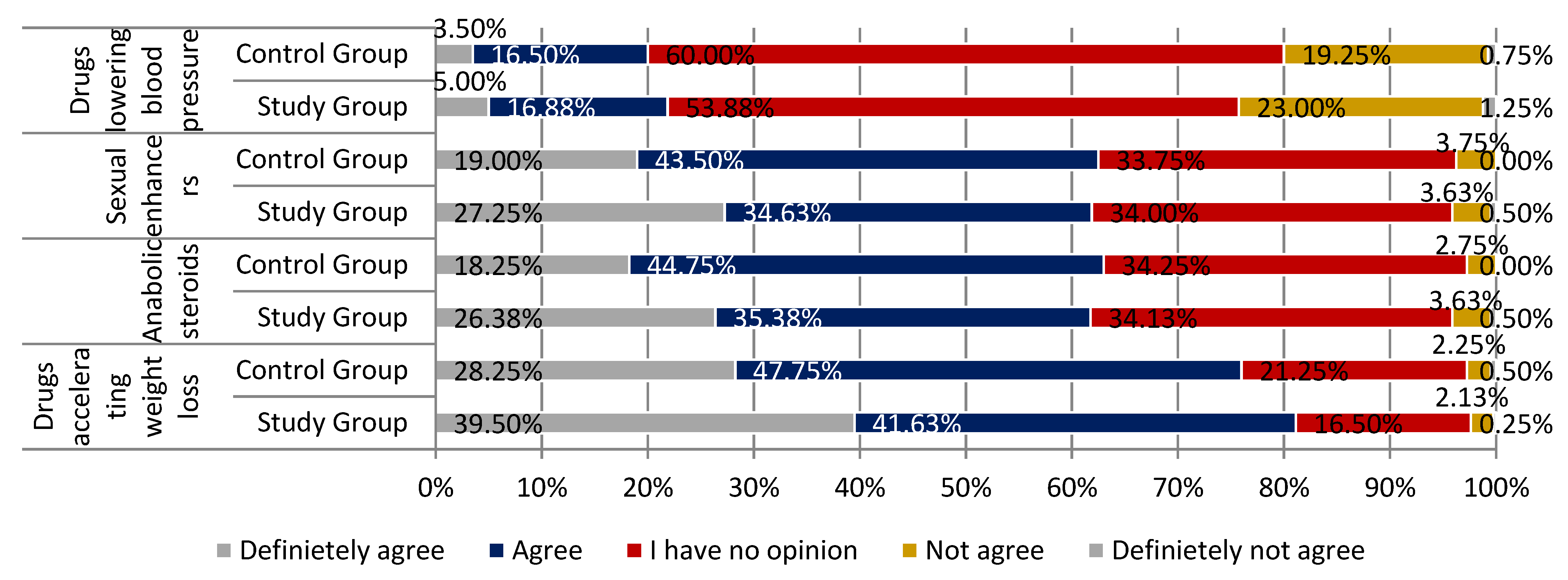
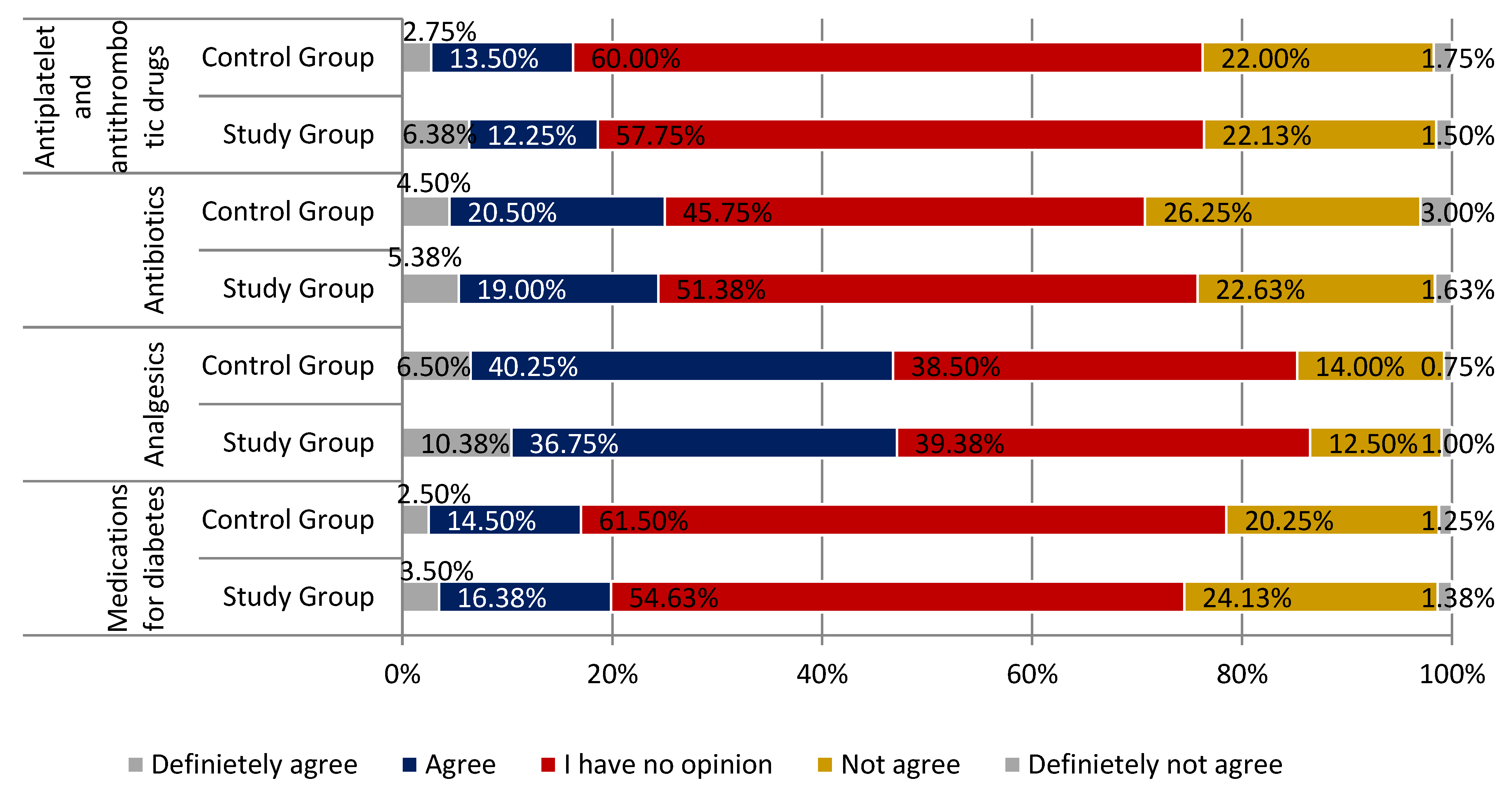
20]. In our study, respondents agreed that community pharmacy subsets were the only place that guaranteed the safety and quality of drugs (the availability of non-falsified medicines). Respondents from the study group were more convinced of this statement. The participants were convinced that they would not distinguish falsified medications and non-falsified drugs, with the respondents from the study group slightly more confident in this matter. Following the patients’ perspectives, the most frequently falsified medications are believed to be drugs included in the following groups: Anti-obesity, anabolic steroids, those for erectile dysfunction, and more rarely, analgesics. More respondents in the study group supported the appropriateness of this statement. Many participants did not have a sufficient level of knowledge to assess the possibility of falsification among hypertensives, antidiabetics, antibiotics, antiplatelet, or antithrombotic agents.
This research can support the designing and implementation of interventions or educational programs dedicated to improving patients’ awareness in the context of the potential harm of falsified medicines. Thus far, the actions provided by governments and international organizations have been focused on chain distribution or implementing new initiatives, e.g., Falsified Medicines Directive (FMD) by the European Commission [
21,
22]. Undoubtedly, authentication seems to be a reasonable solution to detect falsified, expired, or recalled drugs, even if we anticipate that some technical problems may occur during this process [
23,
24]. Experts have suggested that authentication should be supported by an advanced tool such as software with audio and visual feedback, which can improve the accuracy of detection and positively impact the pharmacist’s awareness [
25]. Educational programs and a more systematic approach to the problem mentioned can minimize the potential harm for the patient and raise the awareness of falsification in the public domain [
26]. The introduction of FMD is also crucial from a pharmacovigilance point of view, leading to an easier gathering of adverse events and signal monitoring [
27]. To adequately understand our findings, it is worth mentioning that not only in Europe or in the United States have governments intensified their efforts to combat the pandemic of falsified drugs, but more strict rules have also been introduced to the Middle East, e.g., in the Iranian legal framework [
28], or into Canadian law [
29].
Our study has several limitations. The data obtained during this research is based on the respondents’ declarations and were not confronted with more objective, clinical information. Moreover, we are familiar with the fact that various terms describe fake drugs, falsified or counterfeit medications. Apart from legal matters, these terms can be used interchangeably. Recently, a new term has been coined, which is to be understood as a compromise “falsified (counterfeit) medicines (FFCms)” [
30].














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}