
Geographic Factors Associated with Poorer Outcomes in Patients Diagnosed with COVID-19 in Primary Health Care

 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
- (1)
- Sociodemographic data: sex and age.
- (2)
- Previous medical history: previous cardiovascular diseases (CVD): chronic heart disease, heart failure, cerebrovascular disease, hypertension, dyslipidaemia, previous chronic respiratory diseases, chronic renal diseases, chronic liver diseases, chronic neurological disorders, chronic haematological diseases (leukaemia, lymphoma, myeloma), cancer/neoplasia, HIV and other immunodeficiencies, obesity, diabetes, dermatological diseases, rheumatological diseases, mental disorders and dementia. The diseases were classified according to the International Classification of Diseases 11th Revision [19].
- (3)
- Geographic variables: The size of the area of residence (rural areas were defied as municipalities with a population of fewer than 2000 inhabitants, suburban areas were defined as towns with 2000 to 10,000 inhabitants, and urban areas were defined as having more than 10,000 inhabitants), municipalities with nursing home care (yes/no), distance (Km) from the residence to the hospital and the driving time (minutes) from the residence to the hospital.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Weekly Epidemiological Update. WHO. 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update---5-january-2021 (accessed on 7 January 2021).
- Spanish Ministry of Health. Update No 284. Coronavirus Disease (COVID-19); Spanish Ministry of Health: Madrid, Spain, 2021; Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Actualizacion_284_COVID-19.pdf (accessed on 5 January 2021).
- Spanish Ministry of Health. Management of COVID-19 in Primary Health Care and Home Care; Spanish Ministry of Health: Madrid, Spain, 2020; Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/home.htm (accessed on 7 January 2021).
- Orús, A. Number of Coronavirus Medical Tests Performed Per Million Inhabitants in the Most Affected Countries in the World. 2020. Available online: https://es.statista.com/estadisticas/1107740/covid-19-tasa-de-pruebas-realizadas-en-paises-seleccionados-del-mundo/ (accessed on 8 January 2021).
- OECD. Beyond Containment: Health Systems Responses to COVID 19 in the OECD; OECD: Paris, France, 2020; Available online: https://0-read-oecd--ilibrary-org.brum.beds.ac.uk/view/?ref=119_119689-ud5comtf84&title=Beyond_Containment:Health_systems_responses_to_COVID-19_in_the_OECD (accessed on 21 December 2020).
- WHO Europe. European Observatory of Health Systems and Policies COVID-19 Health System Response Monitor Spain; WHO Europe: Geneva, Switzerland, 2020; Available online: https://www.covid19healthsystem.org/countries/spain/livinghit.aspx?Section=3.1Planningservices&Type=Section (accessed on 7 January 2021).
- Government of Spain. Covid-19 in Spanish Rural Areas. Risk Factors and Opportunities to Improve the Quality of Life of the Elderly; Government of Spain: Madrid, Spain, 2020. Available online: http://envejecimiento.csic.es/documentos/documentos/enred-indicadoresbasicos2020.pdf (accessed on 21 December 2020).
- Pérez Díaz, J.; Abellán García, A.; Aceituno Nieto, P.; Ramiro Fariñas, D. Un perfil de las personas mayores en España, 2020. In Indicadores Estadísticos Básicos; CSHH-CSIC: Madrid, Spain, 2020; Available online: http://envejecimiento.csic.es/documentos/documentos/enred-indicadoresbasicos2020.pdf (accessed on 16 October 2020).
- Fóti, K. Eurofound. Is rural Europe being left behind? European Quality of Life Survey 2016; Publications Office of the European Union: Luxembourg, 2019; Available online: https://www.eurofound.europa.eu/publications/policy-brief/2019/is-rural-europe-being-left-behind (accessed on 15 November 2020).
- Ministerio de Sanidad y Política Social. National Health System Spain; Ministerio de Sanidad y Política Social: Madrid, Spain, 2010. [Google Scholar]
- Corominas, C. Spain Sets a New Minimum of Primary Health Centers and Falls to 2012 Levels; Redacción Médica: Madrid, Spain, 2017; Available online: https://www.redaccionmedica.com/secciones/sanidad-hoy/espana-marca-un-nuevo-minimo-de-centros-de-salud-13-163-al-nivel-de-2012-7402 (accessed on 16 November 2020).
- Gera, I. Covid-19: A Fourth of all Deaths Are in Rural, Semi-Urban India; Financial Express: Delhi, India, 2020; Available online: https://www.financialexpress.com/lifestyle/health/covid-19-a-fourth-of-all-deaths-are-in-rural-semi-urban-india/2092903/ (accessed on 29 September 2020).
- Zhang, C.H.; Schwartz, G.G. Spatial Disparities in Coronavirus Incidence and Mortality in the United States: An Ecological Analysis as of May 2020. J. Rural Heath 2020, 36, 433–445. [Google Scholar] [CrossRef]
- Statistics National Institute. Statistical Information for the Analysis of the Impact of the COVID-19 Crisis. 2020. Available online: https://www.ine.es/covid/covid_inicio.htm (accessed on 7 January 2021).
- Regional Quantitative Analysis Research Group (AQR–UB). Differences between Urban and Rural Municipalities in the Spread of COVID-19 in the Catalan Territory; AQR–University of Barcelona: Barcelona, Spain, 2020; Available online: http://www.ub.edu/ (accessed on 21 December 2020).
- Jain, V.; Yuan, J.M. Predictive symptoms and comorbidities for severe COVID-19 and intensive care unit admission: A systematic review and meta-analysis. Int. J. Public Health 2020, 65, 533–546. [Google Scholar] [CrossRef]
- Pugliese, G.; Vitale, M.; Resi, V.; Orsi, E. Is diabetes mellitus a risk factor for COronaVIrus Disease 19 (COVID-19)? Acta Diabetol. 2020, 57, 1275–1285. [Google Scholar] [CrossRef] [PubMed]
- Tian, W.; Jiang, W.; Yao, J.; Nicholson, C.J.; Li, R.H.; Sigurslid, H.H.; Wooster, L.; Rotter, J.I.; Guo, X.; Malhotra, R. Predictors of mortality in hospitalized COVID-19 patients: A systematic review and meta-analysis. J. Med. Virol. 2020, 92, 1875–1883. [Google Scholar] [CrossRef] [PubMed]
- World Health Orgaization. CIE-11. Available online: https://icd.who.int/es (accessed on 16 January 2021).
- Kolassa, J.E. An Introduction to Nonparametric Statistics; CRC Press, Taylor and Francis Group: Boca Raton, FL, USA, 2020; ISBN 9780367194840. [Google Scholar]
- Kleinbaum, D.G.; Klein, M. Survival Analysis: A Self-Learning Text, 3rd ed.; Springer: New York, NY, USA, 2012. [Google Scholar]
- Villers Gómez, S.; Vásquez Guerra, C.F.; Ramírez Teodoro, L.A. Modelos de Supervivencia. [Survival Models]. Available online: https://carlosfernandovg.github.io/supervivencia_y_series_FC2021-1/an%C3%A1lisis-de-supervivencia.html (accessed on 31 March 2021).
- Ingram, E.; Ledden, S.; Beardon, S.; Gomes, M.; Hogarth, S.; McDonald, H.; Osborn, D.P.; Sheringham, J. Household and area-level social determinants of multimorbidity: A systematic review. J. Epidemiol. Community Health 2020. [Google Scholar] [CrossRef]
- Angulo-Pueyo, E.; Martínez-Lizaga, N.; Bernal-Delgado, E. Wide systematic variations in potentially avoidable hospitalisations of chronically ill patients: Ecological study of basic health areas and healthcare areas. Rev. Clin. Esp. 2020. [Google Scholar] [CrossRef]
- CDC COVID-19 Response Team. Geographic Differences in COVID-19 Cases, Deaths, and Incidence—United States. MMWR Morb. Mortal. Wkly. Rep. 2020, 17, 465–471. [Google Scholar] [CrossRef] [Green Version]
- Barek, M.A.; Aziz, M.A.; Islam, M.S. Impact of age, sex, comorbidities and clinical symptoms on the severity of COVID-19 cases: A meta-analysis with 55 studies and 10014 cases. Heliyon 2020, 6, e05684. [Google Scholar] [CrossRef]
- Chen, T.; Dai, Z.; Mo, P.; Li, X.; Ma, Z.; Song, S.; Chen, X.; Luo, M.; Liang, K.; Gao, S.; et al. Clinical Characteristics and Outcomes of Older Patients with Coronavirus Disease 2019 (COVID-19) in Wuhan, China: A Single-Centered, Retrospective Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2020, 75, 1788–1795. [Google Scholar] [CrossRef] [PubMed]
- Khalatbari-Soltani, S.; Cumming, R.C.; Delpierre, C.; Kelly-Irving, M. Importance of collecting data on socioeconomic determinants from the early stage of the COVID-19 outbreak onwards. J. Epidemiol. Community Health 2020, 74, 620–623. [Google Scholar] [CrossRef]
- Pivonello, R.; Auriemma, R.S.; Pivonello, C.; Isidori, A.M.; Corona, G.; Colao, A.; Millar, R.P. Sex disparities in Covid-19 severity and outcomes: Are men weaker or women stronger? Neuroendocrinology 2020. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Arora, A.; Sharma, P.; Anikhindi, S.A.; Bansal, N.; Singla, V.; Khare, S.; Srivastava, A. Is diabetes mellitus associated with mortality and severity of COVID-19? A meta-analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 535–545. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Wong, J.; Henry, B.M. Hypertension in patients with coronavirus disease 2019 (COVID-19): A pooled analysis. Pol. Arch. Intern. Med. 2020, 130, 304–309. [Google Scholar] [CrossRef] [Green Version]
- Pranata, R.; Huang, I.; Lim, M.A.; Wahjoepramono, E.J.; July, J. Impact of cerebrovascular and cardiovascular diseases on mortality and severity of COVID-19–systematic review, meta-analysis, and meta-regression. J. Stroke Cerebrovasc. Dis. 2020, 29. [Google Scholar] [CrossRef]
- Pranata, R.; Lim, M.A.; Huang, I.; Raharjo, S.B.; Lukito, A.A. Hypertension is associated with increased mortality and severity of disease in COVID-19 pneumonia: A systematic review, meta-analysis and meta-regression. JRAAS J. Renin Angiotensin Aldosterone Syst. 2020, 21. [Google Scholar] [CrossRef]
- Huang, Y.; Lu, Y.; Huang, Y.-M.; Wang, M.; Ling, W.; Sui, Y.; Zhao, H.-L. Obesity in patients with COVID-19: A systematic review and meta-analysis. Metabolism 2020, 113, 154378. [Google Scholar] [CrossRef]
- Cuschieri, S.; Grech, S. Obesity population at risk of COVID-19 complications. Glob. Health Epidemiol. Genom. 2020, 5. [Google Scholar] [CrossRef]
- Caci, G.; Albini, A.; Malerba, M.; Noonan, D.M.; Pochetti, P.; Polosa, R. COVID-19 and Obesity: Dangerous Liaisons. J. Clin. Med. 2020, 9, 2511. [Google Scholar] [CrossRef]
- Kubota, T.; Kuroda, N. Exacerbation of neurological symptoms and COVID-19 severity in patients with preexisting neurological disorders and COVID-19: A systematic review. Clin. Neurol. Neurosurg. 2020. [Google Scholar] [CrossRef]
- Ryoo, N.; Pyun, J.-M.; Baek, M.J.; Suh, J.; Kang, M.J.; Wang, M.J.; Youn, Y.C.; Yang, D.W.; Kim, S.Y.; Park, Y.H.; et al. Coping with Dementia in the Middle of the COVID-19 Pandemic. Int. J. Agric. Biol. 2020, 35, 1–21. [Google Scholar] [CrossRef]
- OECD Health Policy Studies. Geographic Variations in Health Care. In What Do We Know and What Can Be Done to Improve Health System Performance? OECD: Paris, France, 2014. [Google Scholar]
- Bambra, C.; Riordan, R.; Ford, J.; Matthews, F. The COVID-19 pandemic and health inequalities. J. Epidemiol. Community Health 2020, 74, 964–968. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Data | Hospital Admission | ICU Admission | Death | ||||||
|---|---|---|---|---|---|---|---|---|---|
| No | Yes | p | No | Yes | p | No | Yes | p | |
| n (%) | 3797 (60.40%) | 2489 (39.60%) | 6034 (95.99%) | 252 (4.01%) | 5313 (84.52%) | 973 (15.48%) | |||
| Age * | 52 (39–72) | 75 (61–86) | <0.001 | 45 (60–83) | 67 (59–74) | 0.002 | 56 (43–74) | 86 (79–92) | <0.001 |
| Sex | <0.001 | <0.001 | <0.001 | ||||||
| Male | 1434 (37.77%) | 1304 (52.39%) | 2557 (42.38%) | 181 (71.83%) | 2237 (42.10%) | 501 (51.49%) | |||
| Female | 2363 (62.23%) | 1185 (47.61%) | 3477 (57.62%) | 71 (28.71%) | 3076 (57.90%) | 472 (48.51%) | |||
| Municipality classification | 0.002 | 0.009 | <0.001 | ||||||
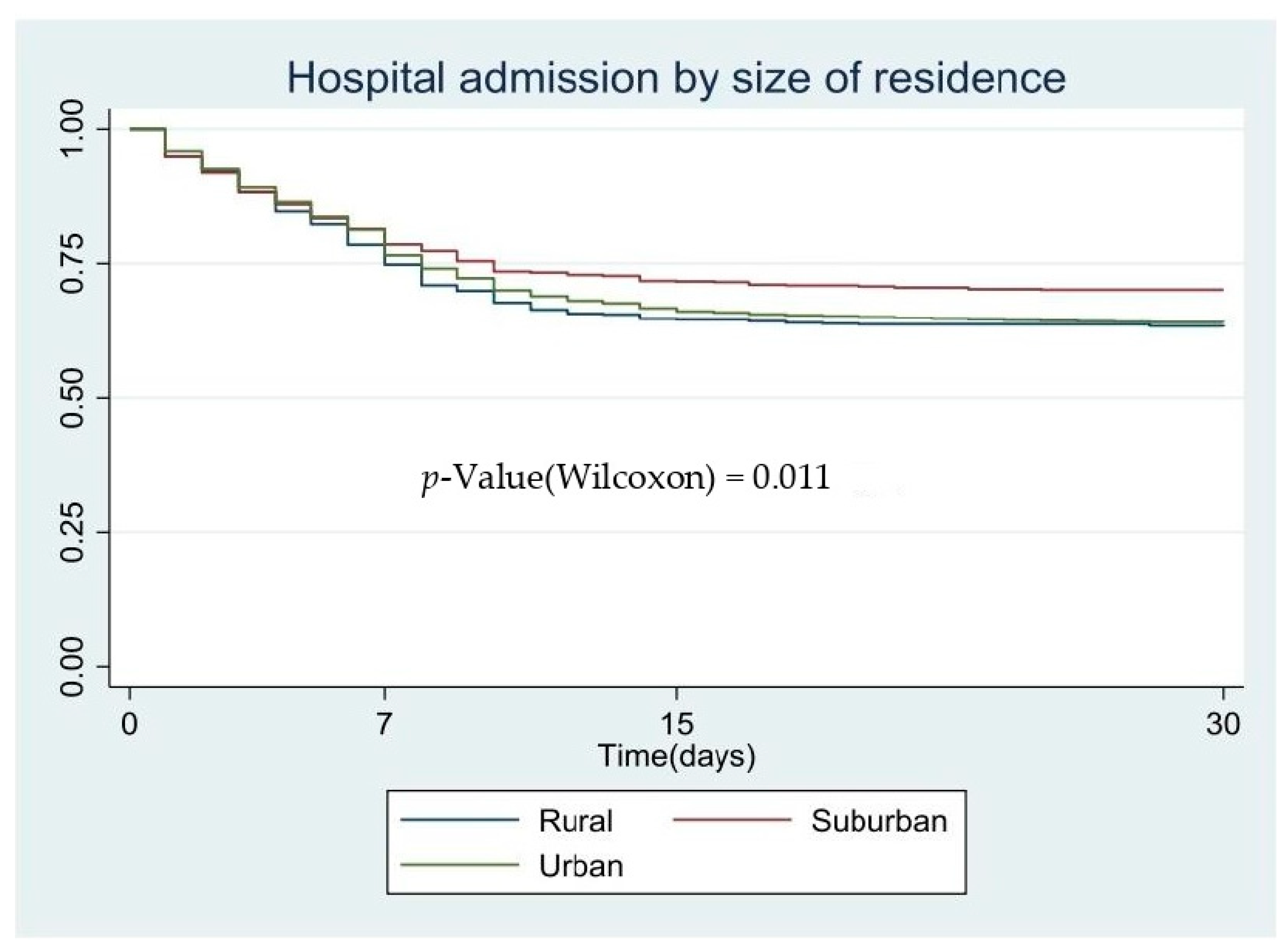
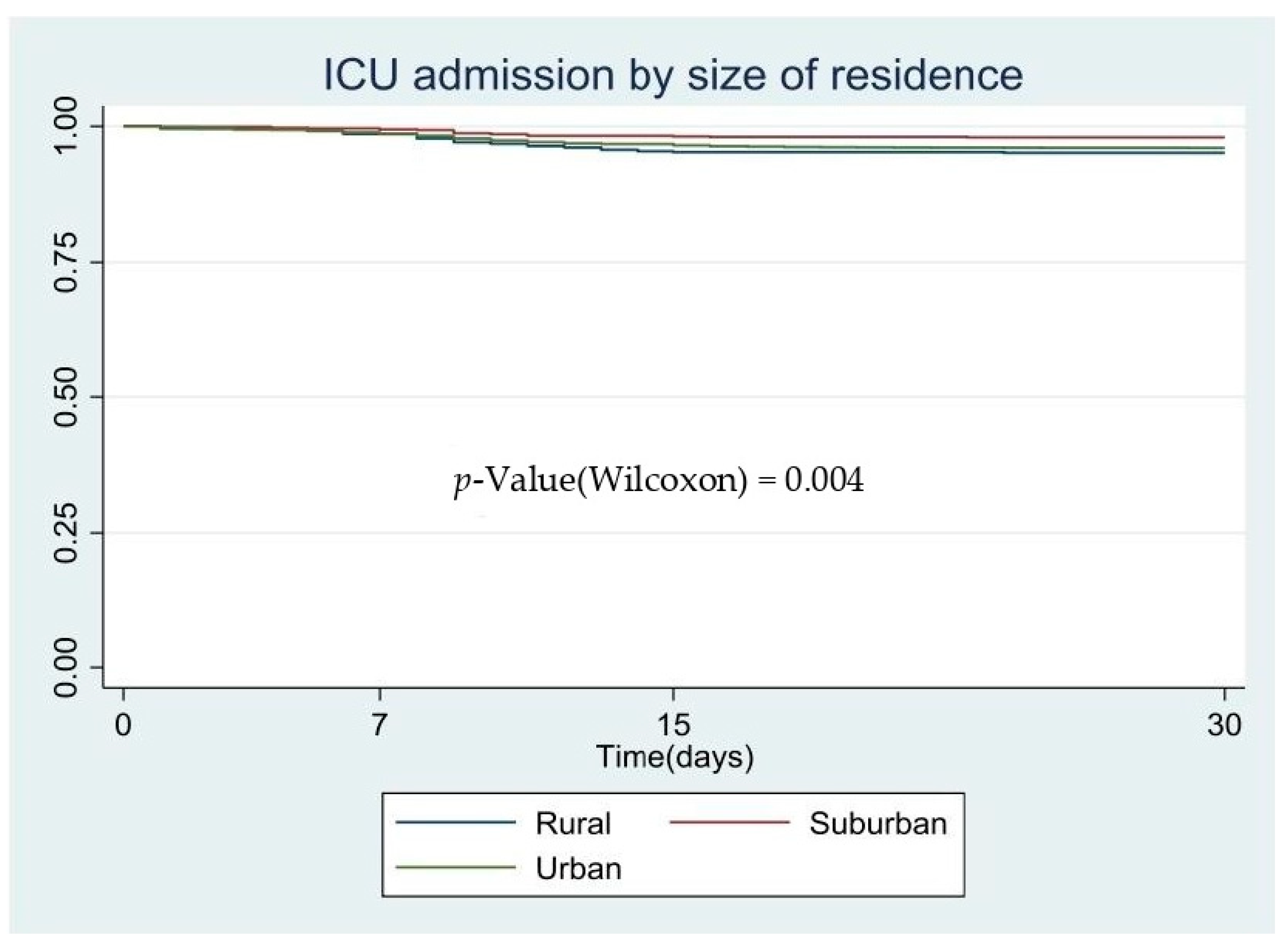
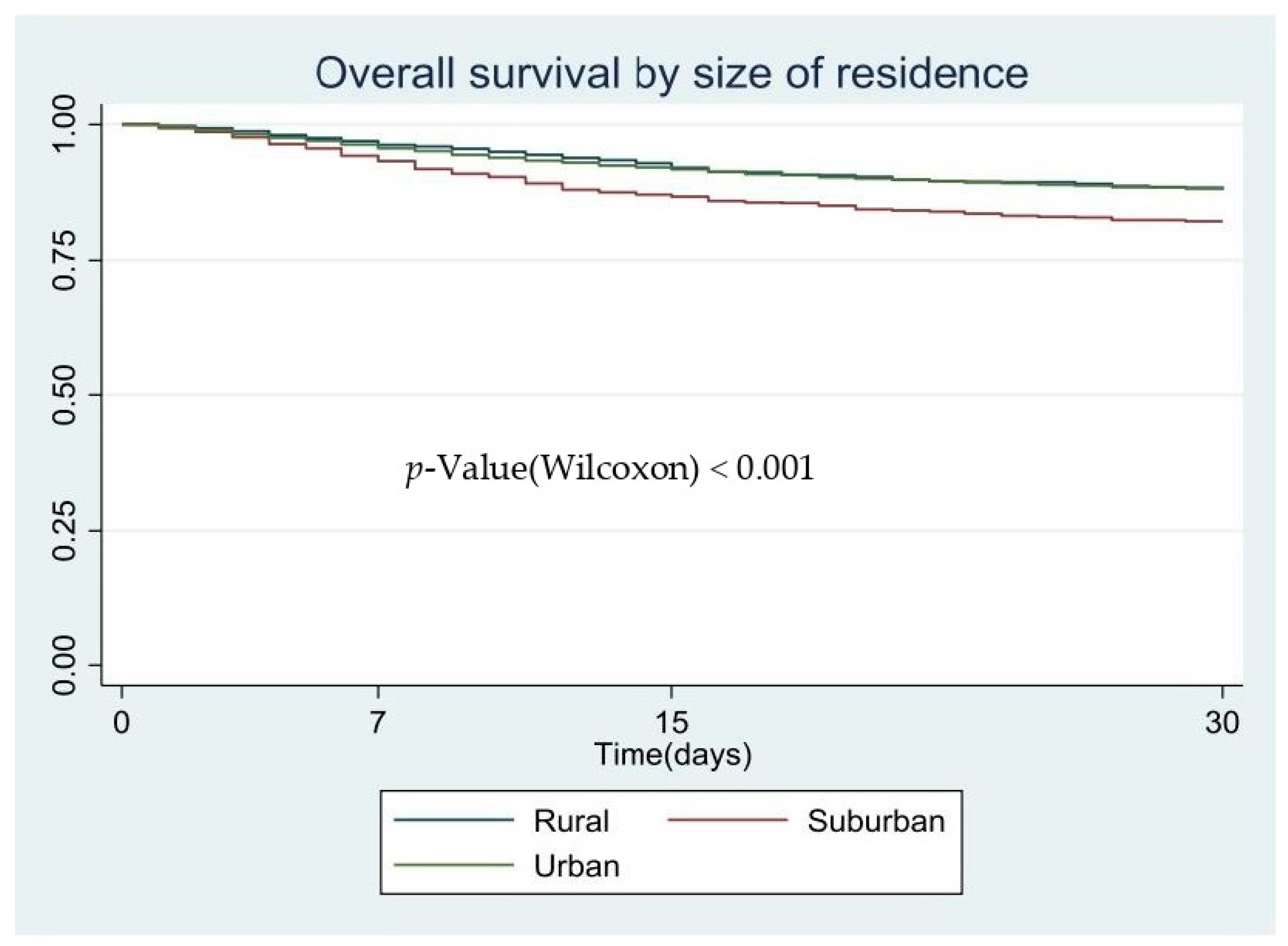
| Rural | 430 (11.52%) | 302 (12.24%) | 696 (11.69%) | 36 (14.63%) | 622 (11.88%) | 110 (11.40%) | |||
| Suburban | 559 (17.93%) | 358 (14.51%) | 1003 (16.85%) | 24 (9.76%) | 803 (15.34%) | 224 (23.21%) | |||
| Urban | 2633 (70.55%) | 1807 (73.25%) | 4254 (71.46%) | 186 (75.61%) | 3809 (72.77%) | 631 (65.39%) | |||
| Municipality—hospital distance, km * | 0 (0–27.55) | 0 (0–18.70) | <0.001 | 0 (0–25.20) | 0 (0–17.70) | 0.136 | 0 (0–25.20) | 0 (0–27.70) | 0.018 |
| Drive time from municipality to hospital, min * | 0 (0–23) | 0 (0–19) | <0.001 | 0 (0–23) | 0 (0–17) | 0.127 | 0 (0–22) | 0 (0–25) | 0.015 |
| Hospital Admission | ICU Admission | Death | |||||||
|---|---|---|---|---|---|---|---|---|---|
| No | Yes | p | No | Yes | p | No | Yes | p | |
| Previous cardiovascular disease | 1013 (26.68%) | 1168 (46.93%) | <0.001 | 1013 (26.68%) | 1168 (46.93%) | <0.001 | 1013 (26.68%) | 1168 (46.93%) | <0.001 |
| Hypertension | 961 (25.31%) | 1290 (51.83%) | <0.001 | 2124 (35.20%) | 127 (50.40%) | <0.001 | 1612 (30.34%) | 639 (65.57%) | <0.001 |
| Dyslipidaemia | 897 (23.62%) | 1060 (42.83%) | <0.001 | 1828 (30.29%) | 135 (53.57%) | <0.001 | 1551 (29.19%) | 412 (42.34%) | <0.001 |
| Previous respiratory disease | 306 (8.06%) | 348 (13.98%) | <0.001 | 306 (8.06%) | 348 (13.98%) | <0.001 | 306 (8.06%) | 348 (13.98%) | <0.001 |
| Chronic kidney disease | 212 (5.58%) | 352 (14.14%) | <0.001 | 542 (8.98%) | 22 (8.73%) | 0.891 | 348 (6.55%) | 216 (22.20%) | <0.001 |
| Chronic liver disease | 51 (1.34%) | 64 (2.57%) | <0.001 | 104 (1.72%) | 11 (4.37%) | 0.002 | 98 (1.84%) | 17 (1.75%) | 0.835 |
| Chronic neurological disorder | 586 (15.43%) | 475 (19.08%) | <0.001 | 1027 (17.02%) | 34 (13.49%) | 0.143 | 869 (16.36%) | 192 (19.73%) | 0.010 |
| Immunosuppression/previous transplantation | 71 (1.87%) | 118 (4.74%) | <0.001 | 174 (2.88%) | 15 (5.95%) | 0.005 | 143 (2.69%) | 46 (4.73%) | 0.001 |
| Chronic haematological disease (including leukaemia, lymphoma, myeloma) | 1205 (31.74%) | 1185 (47.61%) | <0.001 | 2263 (37.50%) | 127 (50.40%) | <0.001 | 1828 (34.41%) | 562 (57.76%) | <0.001 |
| Neoplasia | 258 (6.79%) | 369 (14.83%) | <0.001 | 596 (9.88%) | 31 (12.30%) | 0.208 | 436 (8.21%) | 191 (19.63%) | <0.001 |
| HIV and other immunodeficiencies | 25 (0.66%) | 28 (1.12%) | 0.048 | 50 (0.83%) | 3 (1.19%) | 0.538 | 40 (0.75%) | 13 (1.34%) | 0.067 |
| Obesity | 321 (8.45%) | 366 (14.70%) | <0.001 | 629 (10.42%) | 58 (23.02%) | <0.001 | 574 (10.80%) | 113 (11.61%) | 0.457 |
| Malnutrition | 549 (14.46%) | 522 (20.97%) | <0.001 | 1022 (16.94%) | 49 (19.44%) | 0.300 | 819 (15.42%) | 252 (25.90%) | <0.001 |
| Diabetes | 319 (8.40%) | 496 (19.93%) | <0.001 | 758 (12.56%) | 57 (22.62%) | <0.001 | 569 (10.71%) | 246 (25.28%) | <0.001 |
| Mental illness | 784 (20.65%) | 694 (27.88%) | <0.001 | 1433 (23.75%) | 45 (17.86%) | 0.031 | 1163 (21.89%) | 315 (32.37%) | <0.001 |
| Dementia | 311 (8.19%) | 365 (14.66%) | <0.001 | 673 (11.15%) | 3 (1.19%) | <0.001 | 381 (7.17%) | 295 (30.32%) | <0.001 |
| Dermatological disease | 1355 (35.69%) | 1063 (42.71%) | <0.001 | 2317 (38.40%) | 101 (40.08%) | 0.591 | 1982 (37.30%) | 436 (44.81%) | <0.001 |
| Rheumatological disease | 478 (12.59%) | 554 (22.26%) | <0.001 | 998 (16.54%) | 34 (13.49%) | 0.201 | 769 (14.47%) | 263 (27.03%) | <0.001 |
| Variables | Hospital Admission | ICU Admission | Death | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HR | p | 95% CI | HR | p | 95% CI | HR | p | 95% CI | |||||
| Age | 1.03 | <0.001 | 1.02 | 1.03 | 1.08 | <0.001 | 1.07 | 1.09 | |||||
| Sex | |||||||||||||
| Male | Ref | Ref | Ref | ||||||||||
| Female | 0.59 | <0.001 | 0.54 | 0.64 | 0.28 | <0.001 | 0.21 | 0.38 | 0.54 | <0.001 | 0.47 | 0.62 | |
| Area | |||||||||||||
| Rural | Ref | Ref | Ref | ||||||||||
| Suburban | 0.77 | 0.002 | 0.65 | 0.91 | 0.50 | 0.011 | 0.29 | 0.85 | 1.31 | 0.022 | 1.04 | 1.66 | |
| Urban | 1.14 | 0.054 | 1.00 | 1.30 | 1.02 | 0.930 | 0.71 | 1.46 | 1.23 | 0.047 | 1.00 | 1.51 | |
| Municipality—hospital distance | 0.99 | 0.001 | 0.98 | 0.99 | |||||||||
| Comorbidities | |||||||||||||
| Previous cardiovascular disease | 1.14 | 0.006 | 1.04 | 1.26 | 1.18 | 0.018 | 1.03 | 1.35 | |||||
| Hypertension | 1.12 | 0.034 | 1.01 | 1.24 | 1.43 | 0.010 | 1.09 | 1.89 | |||||
| Dyslipidaemia | 1.35 | <0.001 | 1.23 | 1.47 | 2.18 | 0.000 | 1.66 | 2.86 | |||||
| Previous respiratory disease | 1.14 | 0.040 | 1.01 | 1.29 | |||||||||
| Chronic neurological disorder | 1.14 | 0.021 | 1.02 | 1.27 | |||||||||
| Ulcerative disease/immunosuppression/previous transplant | 1.40 | 0.001 | 1.15 | 1.71 | |||||||||
| Chronic haematological disease (including leukaemia, lymphoma, myeloma) | 1.08 | 0.098 | 0.99 | 1.18 | 1.33 | 0.038 | 1.02 | 1.74 | 1.20 | 0.007 | 1.05 | 1.37 | |
| Neoplasia | 1.12 | 0.049 | 1.00 | 1.27 | |||||||||
| Obesity | 1.29 | <0.001 | 1.14 | 1.46 | 2.04 | <0.001 | 1.49 | 2.78 | |||||
| Diabetes | 1.15 | 0.017 | 1.02 | 1.28 | 1.20 | 0.018 | 1.03 | 1.39 | |||||
| Dementia | 0.86 | 0.024 | 0.75 | 0.98 | 0.10 | <0.001 | 0.03 | 0.31 | 1.38 | <0.001 | 1.20 | 1.59 | |
| Dermatological disease | 1.08 | 0.085 | 0.99 | 1.18 | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magallón-Botaya, R.; Oliván-Blázquez, B.; Ramírez-Cervantes, K.L.; Méndez-López-de-la-Manzanara, F.; Aguilar-Palacio, I.; Casajuana-Closas, M.; Andrés-Esteban, E. Geographic Factors Associated with Poorer Outcomes in Patients Diagnosed with COVID-19 in Primary Health Care. Int. J. Environ. Res. Public Health 2021, 18, 3842. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073842
Magallón-Botaya R, Oliván-Blázquez B, Ramírez-Cervantes KL, Méndez-López-de-la-Manzanara F, Aguilar-Palacio I, Casajuana-Closas M, Andrés-Esteban E. Geographic Factors Associated with Poorer Outcomes in Patients Diagnosed with COVID-19 in Primary Health Care. International Journal of Environmental Research and Public Health. 2021; 18(7):3842. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073842
Chicago/Turabian StyleMagallón-Botaya, Rosa, Bárbara Oliván-Blázquez, Karen Lizzette Ramírez-Cervantes, Fátima Méndez-López-de-la-Manzanara, Isabel Aguilar-Palacio, Marc Casajuana-Closas, and Eva Andrés-Esteban. 2021. "Geographic Factors Associated with Poorer Outcomes in Patients Diagnosed with COVID-19 in Primary Health Care" International Journal of Environmental Research and Public Health 18, no. 7: 3842. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073842