Two-Year Follow-Up of 4-mm-Long Implants Used as Distal Support of Full-Arch FDPs Compared to 10-mm Implants Installed after Sinus Floor Elevation. A Randomized Clinical Trial


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
- Edentulous maxilla.
- Willing to receive a full arch fixed restoration in the maxilla.
- Latest extraction at least 8 weeks before implant insertion.
- Sinus floor height included between 4 to 6 mm.
- Bone width in the distal segments enough to allow the insertion of a 4-mm-long implant of standard diameter.
- In the anterior maxilla (from first premolar to first premolar), bone width enough to allow the insertion of 10-mm-long implants of standard diameter.
- -
- Natural dentition (at least 10 elements from 3.5 to 4.5).
- -
- FDPs – Fixed dental prosthesis of at least 10 elements (from 3.5 to 4.5) supported by teeth or implants.
- -
- Implant-supported or teeth-supported overdentures.
- -
- Adequate partial removable prostheses.
- Presence of conditions requiring prophylactic use of antibiotics (e.g., history of rheumatic heart disease, bacterial endocarditis, cardiac valvular anomalies, prosthetic joint replacements).
- Major systemic diseases, or medical conditions requiring prolonged use of steroids, or alcoholism or chronic drug abuse.
- Current pregnancy or breastfeeding women.
- Smokers >10 cigarettes per day.
- Physical handicaps that would interfere with the ability to perform adequate oral hygiene.
- Immunocompromised patients including patients infected with HIV.
- Conditions or circumstances, in the opinion of the investigator, which would prevent completion of study participation or interfere with analysis of study results, such as history of noncompliance, or unreliability.
- Patients with an ongoing or previous treatment with bisphosphonates (for at least 2 months for oral therapy or 6 months for IV injection).
- Local inflammation, including untreated periodontitis.
- Pre-cancerous oral lesions.
- History of local irradiation therapy.
- Severe bruxism or clenching habits.
- Patients with inadequate oral hygiene or unmotivated for adequate oral home care.
- Previous GBR or GTR Guided Tissue Regeneration treatment at the implant site.
- Total removable prosthesis in the lower arch.
2.3. Sample Calculation
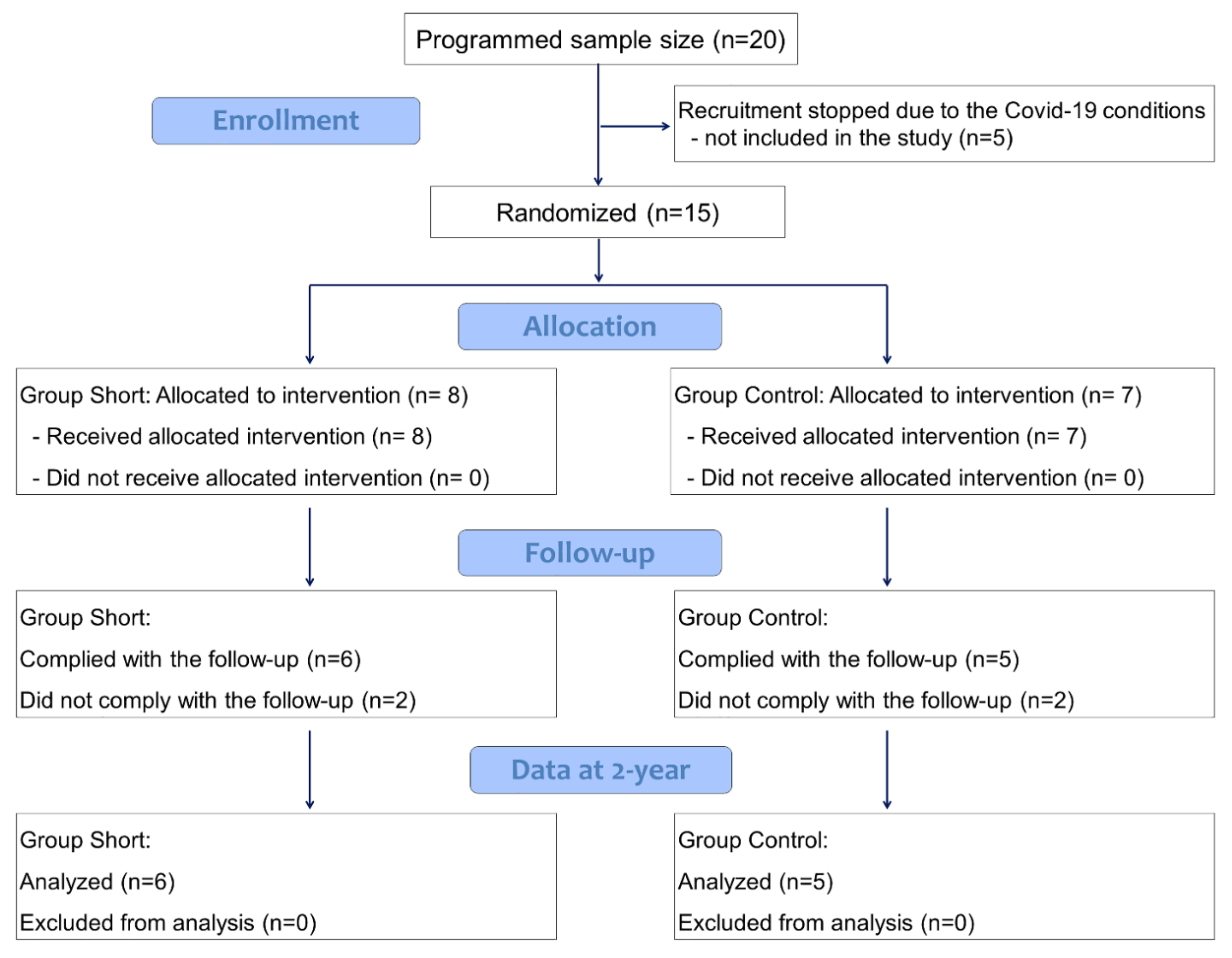
2.4. Randomization and Assignment Concealment
2.5. Implants and Biomaterial Used
2.6. Surgical Procedures in the Short Group (Test)
2.7. Surgical Procedures in the Standard Group (Control)
2.8. Maintenance Care of the Patients
2.9. Prosthetic Procedures
2.10. Clinical Evaluation
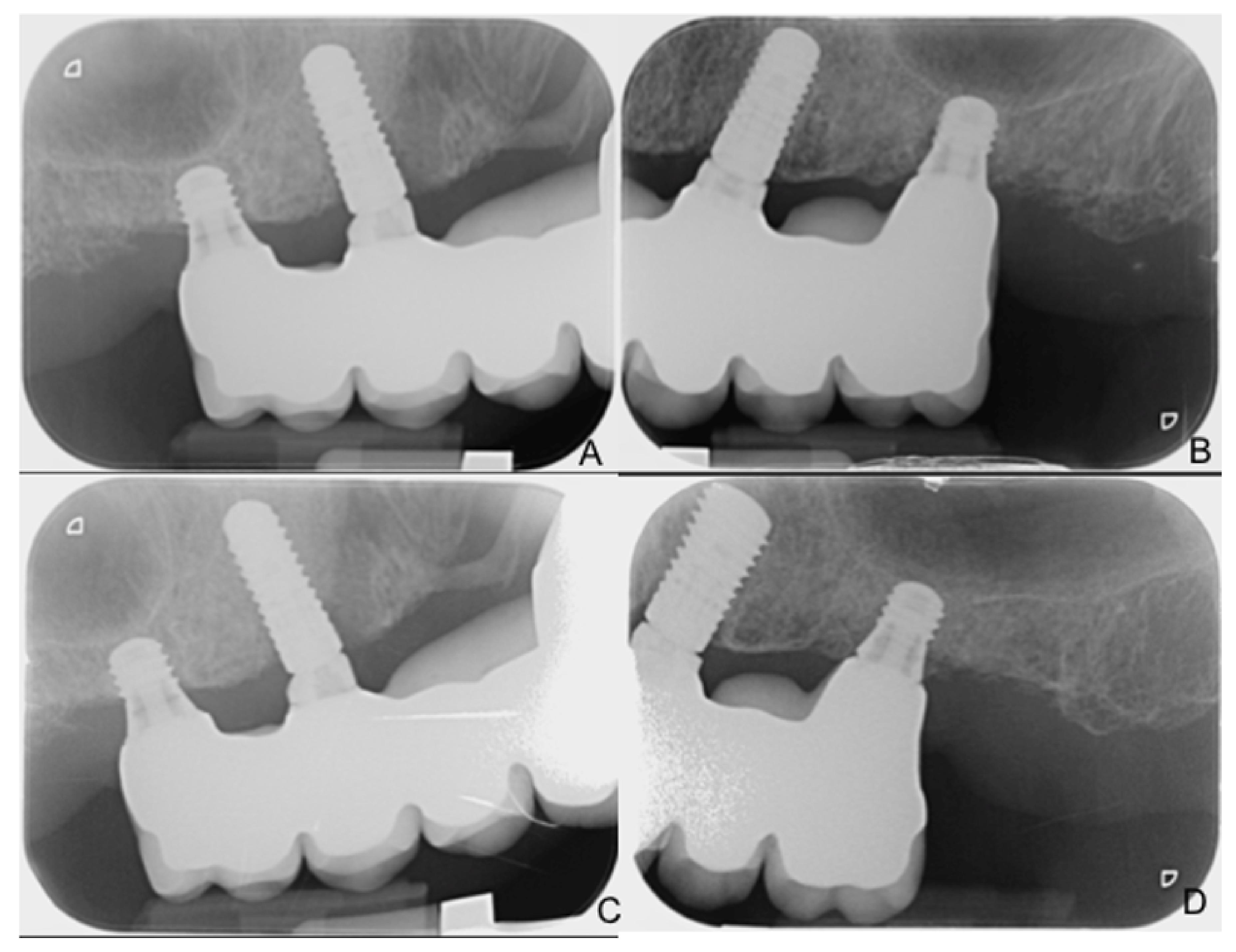
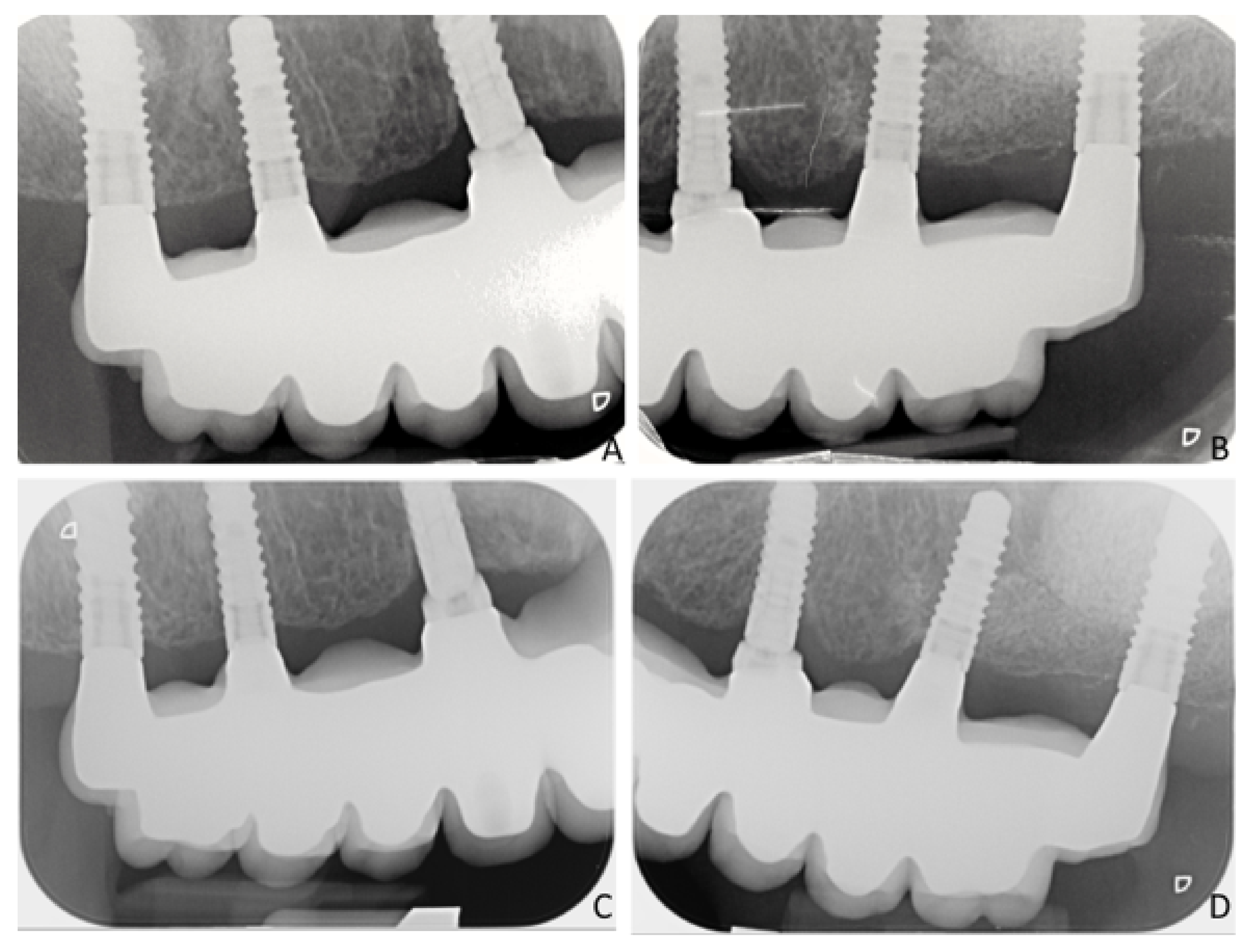
2.11. Radiographic Measurements
2.12. PROMs Evaluation
2.13. Data Analysis
3. Results
PROMs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Apaza Alccayhuaman, K.A.; Soto-Peñaloza, D.; Nakajima, Y.; Papageorgiou, S.N.; Botticelli, D.; Lang, N.P. Biological and technical complications of tilted implants in comparison with straight implants supporting fixed dental prostheses. A systematic review and meta-analysis. Clin. Oral. Implant. Res. 2018, 29 (Suppl. S18), 295–308. [Google Scholar] [CrossRef] [PubMed]
- Cucchi, A.; Ghensi, P. Vertical Guided Bone Regeneration using Titanium-reinforced d-PTFE Membrane and PrehydratedCorticocancellous Bone Graft. Open Dent. J. 2014, 8, 194–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raghoebar, G.M.; Onclin, P.; Boven, G.C.; Vissink, A.; Meijer, H.J.A. Long-term effectiveness of maxillary sinus floor augmentation: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46 (Suppl. S21), 307–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esposito, M.; Grusovin, M.G.; Rees, J.; Karasoulos, D.; Felice, P.; Alissa, R.; Worthington, H.; Coulthard, P. Effectiveness of sinus lift procedures for dental implant rehabilitation: A Cochrane systematic review. Eur. J. Oral. Implantol. 2010, 3, 7–26. [Google Scholar] [PubMed]
- Menchini-Fabris, G.B.; Toti, P.; Crespi, G.; Covani, U.; Crespi, R. Distal Displacement of Maxillary Sinus Anterior Wall Versus Conventional Sinus Lift with Lateral Access: A 3-Year Retrospective Computerized Tomography Study. Int. J. Environ. Res. Public Health 2020, 17, 7199. [Google Scholar] [CrossRef] [PubMed]
- Thoma, D.S.; Zeltner, M.; Hüsler, J.; Hämmerle, C.H.; Jung, R.E. EAO Supplement Working Group 4-EAO CC 2015 Short implants versus sinus lifting with longer implants to restore the posterior maxilla: A systematic review. Clin. Oral. Implant. Res. 2015, 26 (Suppl. S11), 154–169. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Al-Nawas, B.; Araujo, M.; Avila-Ortiz, G.; Barter, S.; Brodala, N.; Chappuis, V.; Chen, B.; De Souza, A.; Almeida, R.F.; et al. Group 1 ITI Consensus Report: The influence of implant length and design and medications on clinical and patient-reported outcomes. Clin. Oral. Implant. Res. 2018, 29 (Suppl. S16), 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossi, F.; Lang, N.P.; Ricci, E.; Ferraioli, L.; Baldi, N.; Botticelli, D. Long-term follow-up of single crowns supported by short, moderately rough implants-A prospective 10-year cohort study. Clin. Oral. Implant. Res. 2018, 29, 1212–1219. [Google Scholar] [CrossRef]
- Bolle, C.; Felice, P.; Barausse, C.; Pistilli, V.; Trullenque-Eriksson, A.; Esposito, M. 4 mm long vs longer implants in augmented bone in posterior atrophic jaws: 1-year post-loading results from a multicentrerandomised controlled trial. Eur. J. Oral. Implantol. 2018, 11, 31–47. [Google Scholar]
- Slotte, C.; Grønningsaeter, A.; Halmøy, A.M.; Öhrnell, L.O.; Mordenfeld, A.; Isaksson, S.; Johansson, L.Å. Four-Millimeter-Long Posterior-Mandible Implants: 5-Year Outcomes of a Prospective Multicenter Study. Clin. Implant. Dent. Relat. Res. 2015, 17 (Suppl. S2), e385–e395. [Google Scholar] [CrossRef] [PubMed]
- Lekholm, U.; Zarb, G.A. Patient selection and preparation. In Tissue Integrated Prostheses: Osseointegration in Clinical Dentistry; Branemark, P.I., Zarb, G.A., Albektsson, T., Eds.; Quintessence: Chicago, IL, USA, 1985; pp. 199–209. [Google Scholar]
- Lang, N.P.; Joss, A.; Orsanic, T.; Gusberti, F.A.; Siegrist, B.E. Bleeding on probing. A predictor for the progression of periodontal disease? J. Clin. Periodontol. 1986, 13, 590–596. [Google Scholar] [CrossRef] [PubMed]
- Feine, J.; Abou-Ayash, S.; Al Mardini, M.; de Santana, R.B.; Bjelke-Holtermann, T.; Bornstein, M.M.; Braegger, U.; Cao, O.; Cordaro, L.; Eycken, D.; et al. Group 3 ITI Consensus Report: Patient-reported outcome measures associated with implant dentistry. Clin. Oral. Implant. Res. 2018, 29 (Suppl. S16), 270–275. [Google Scholar] [CrossRef] [PubMed]
- Torassa, D.; Naldini, P.; Calvo-Guirado, J.L.; Fernández-Bodereau, E. Prospective, Clinical Pilot Study with Eleven 4-Mm Extra-Short Implants Splinted to Longer Implants for Posterior Maxilla Rehabilitation. J. Clin. Med. 2020, 9, 357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvo-Guirado, J.L.; López Torres, J.A.; Dard, M.; Javed, F.; Pérez-Albacete Martínez, C.; Maté Sánchez de Val, J.E. Evaluation of extrashort 4-mm implants in mandibular edentulous patients with reduced bone height in comparison with standard implants: A 12-month results. Clin. Oral. Implant. Res. 2016, 27, 867–874. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Zucchelli, G.; Barausse, C.; Pistilli, R.; Trullenque-Eriksson, A.; Felice, P. Four mm-long versus longer implants in augmented bone in atrophic posterior jaws: 4-month post-loading results from a multicentrerandomised controlled trial. Eur. J. Oral. Implantol. 2016, 9, 393–409. [Google Scholar] [PubMed]
- Rokn, A.R.; Monzavi, A.; Panjnoush, M.; Hashemi, H.M.; Kharazifard, M.J.; Bitaraf, T. Comparing 4-mm dental implants to longer implants placed in augmented bones in the atrophic posterior mandibles: One-year results of a randomized controlled trial. Clin. Implant. Dent. Relat. Res. 2018, 20, 997–1002. [Google Scholar] [CrossRef] [PubMed]
- Yan, Q.; Wu, X.; Su, M.; Hua, F.; Shi, B. Short implants (≤6 mm) versus longer implants with sinus floor elevation in atrophic posterior maxilla: A systematic review and meta-analysis. BMJ Open 2019, 9, e029826. [Google Scholar] [CrossRef] [PubMed]
- Rossi, F.; Lang, N.P.; Ricci, E.; Ferraioli, L.; Marchetti, C.; Botticelli, D. Early loading of 6-mm-short implants with a moderately rough surface supporting single crowns—A prospective 5-year cohort study. Clin. Oral. Implant. Res. 2015, 26, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Moraschini, V.; Mourão, C.F.d.A.B.; Montemezzi, P.; Kischinhevsky, I.C.C.; de Almeida, D.C.F.; Javid, K.; Shibli, J.A.; Gran-jeiro, J.M.; Calasans-Maia, M.D. Clinical Comparation of Extra-Short (4 mm) and Long (>8 mm) Dental Implants Placed in Mandibular Bone: A Systematic Review and Metanalysis. Healthcare 2021, 9, 315. [Google Scholar] [CrossRef]
- Thoma, D.S.; Haas, R.; Sporniak-Tutak, K.; Garcia, A.; Taylor, T.D.; Hämmerle, C.H.F. Randomized controlled multicentre study comparing short dental implants (6 mm) versus longer dental implants (11–15 mm) in combination with sinus floor elevation procedures: 5-Year data. J. Clin. Periodontol. 2018, 45, 1465–1474. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male | Female | Mean Age | Smokers | Maxilla | Bone Type 1 I, II, III, IV | Insertion Torque 1 (Ncm) | Antagonist 1 | |
|---|---|---|---|---|---|---|---|---|
| 3 | 3 | 59.8 | 4 out of 6 | 16 and 26 | Type I: 0 Type II: 0 Type III: 6 Type IV: 6 | <15: 0 15 < x< 35: 6 ≥35: 6 | ND: 2 FDP: 2 OD: 0 Mix: 8 | |
| STANDARD | 3 | 2 | 60.8 | 2 out of 5 | 16 and 26 | Type I: 0 Type II: 0 Type III: 6 Type IV: 4 | <15: 0 15 < x < 35: 6 ≥35: 4 | ND: 2 FDP: 0 OD: 2 Mix: 6 |
| MBL Short | MBL Control | Progressive Changes Short | Progressive Changes Control | |
|---|---|---|---|---|
| Prosthesis delivering (BL) | 0.17 ± 0.41 | 0.28 ± 0.21 | NA | NA |
| 6 months | 0.18 ± 0.34 | 0.49 ± 0.44 | −0.01 ± 0.11 | −0.21 ± 0.33 |
| 12 months | 0.21 ± 0.35 | 0.58 ± 0.44 | −0.04 ± 0.13 | −0.30 ± 0.32 |
| 18 months | 0.34 ± 0.35 | 0.68 ± 0.51 | −0.17 ± 0.29 | −0.40 ± 0.37 |
| 24 months | 0.44 ± 0.37 | 0.84 ± 0.68 | −0.28 ± 0.37 | −0.54 ± 0.49 |
| (A) | |||||
| Functional Limitation | Physical Pain | Physical Disability | Psychological Discomfort | Social Disability | |
| Mean Pre-Sur SD Pre-Sur | 3.2 0.6 | 4.5 0.1 | 3.1 0.7 | 3.6 0.5 | 4.1 1.0 |
| Mean 6 m SD 6 m | 4.9 0.2 | 5.0 0.8 | 5.3 0.4 | 5.4 0.3 | 5.8 0.2 |
| Mean 12 m SD 12 m | 4.9 0.1 | 5.2 0.6 | 5.6 0.4 | 5.5 0.2 | 5.8 0.2 |
| Mean 24 m SD 24 m | 5.5 0.6 | 5.2 0.3 | 5.7 0.3 | 5.8 0.2 | 4.9 2.4 |
| (B) | |||||
| Functional Limitation | Physical Pain | Physical Disability | Psychological Discomfort | Social Disability | |
| Mean Pre-Sur SD Pre-Sur | 3.3 0.7 | 4.9 0.0 | 3.6 1.0 | 3.9 0.7 | 4.9 0.6 |
| Mean 6 m SD 6 m | 6.0 0.1 | 5.8 0.1 | 5.9 0.1 | 5.8 0.1 | 5.9 0.1 |
| Mean 12 m SD 12 m | 5.9 0.2 | 5.9 0.1 | 6.0 0.0 | 6.0 0.0 | 6.0 0.0 |
| Mean 24m SD 24m | 5.9 0.2 | 5.8 0.1 | 6.0 0.0 | 6.0 0.0 | 6.0 0.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, F.; Tuci, L.; Ferraioli, L.; Ricci, E.; Suerica, A.; Botticelli, D.; Pellegrino, G.; Felice, P. Two-Year Follow-Up of 4-mm-Long Implants Used as Distal Support of Full-Arch FDPs Compared to 10-mm Implants Installed after Sinus Floor Elevation. A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2021, 18, 3846. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073846
Rossi F, Tuci L, Ferraioli L, Ricci E, Suerica A, Botticelli D, Pellegrino G, Felice P. Two-Year Follow-Up of 4-mm-Long Implants Used as Distal Support of Full-Arch FDPs Compared to 10-mm Implants Installed after Sinus Floor Elevation. A Randomized Clinical Trial. International Journal of Environmental Research and Public Health. 2021; 18(7):3846. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073846
Chicago/Turabian StyleRossi, Fabio, Lorenzo Tuci, Lorenzo Ferraioli, Emanuele Ricci, Andreea Suerica, Daniele Botticelli, Gerardo Pellegrino, and Pietro Felice. 2021. "Two-Year Follow-Up of 4-mm-Long Implants Used as Distal Support of Full-Arch FDPs Compared to 10-mm Implants Installed after Sinus Floor Elevation. A Randomized Clinical Trial" International Journal of Environmental Research and Public Health 18, no. 7: 3846. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073846