
Importance of Immediate Electronic-Based Feedback to Enhance Feedback for First-Time CPR Trainees


 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
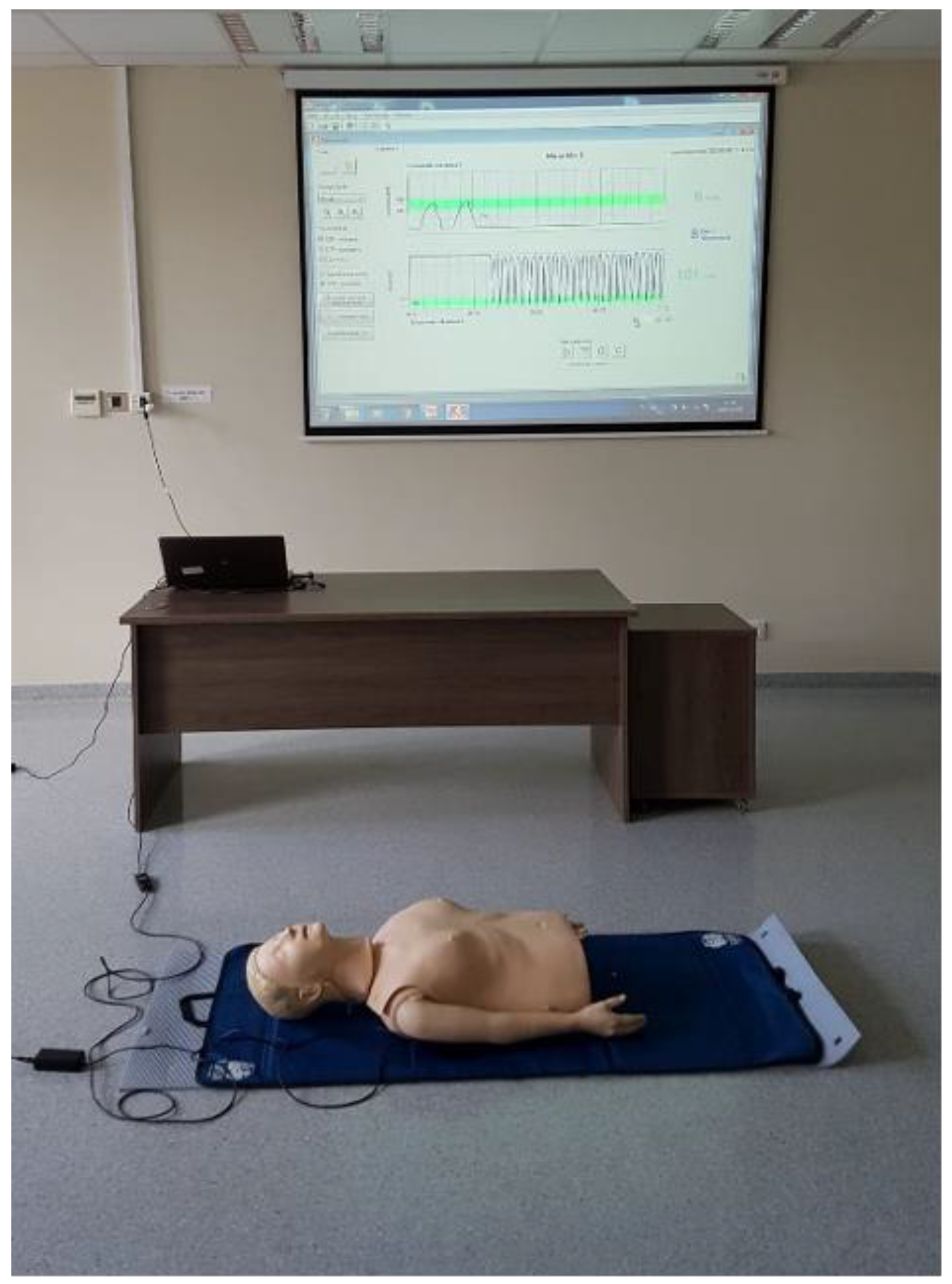
2.1. Study Design
2.2. Next Phase
- Current and average compression rate,
- The exact number of compressions implemented,
- The ratio of the number of chest compressions to the number of rescue breaths,
- Compression depth given in millimeters,
- Relaxation error,
- Hand position error, indicating the direction of the wrong hand position,
- The airway patency,
- The exact amount of air supplied,
- The speed with which the air is introduced during rescue breaths,
- Resuscitation time.
2.3. Study Location and Population
2.4. Questionnaire
2.5. Statistical Analysis
2.6. Ethics Approval and Consent to Participate
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
The Questionnaire
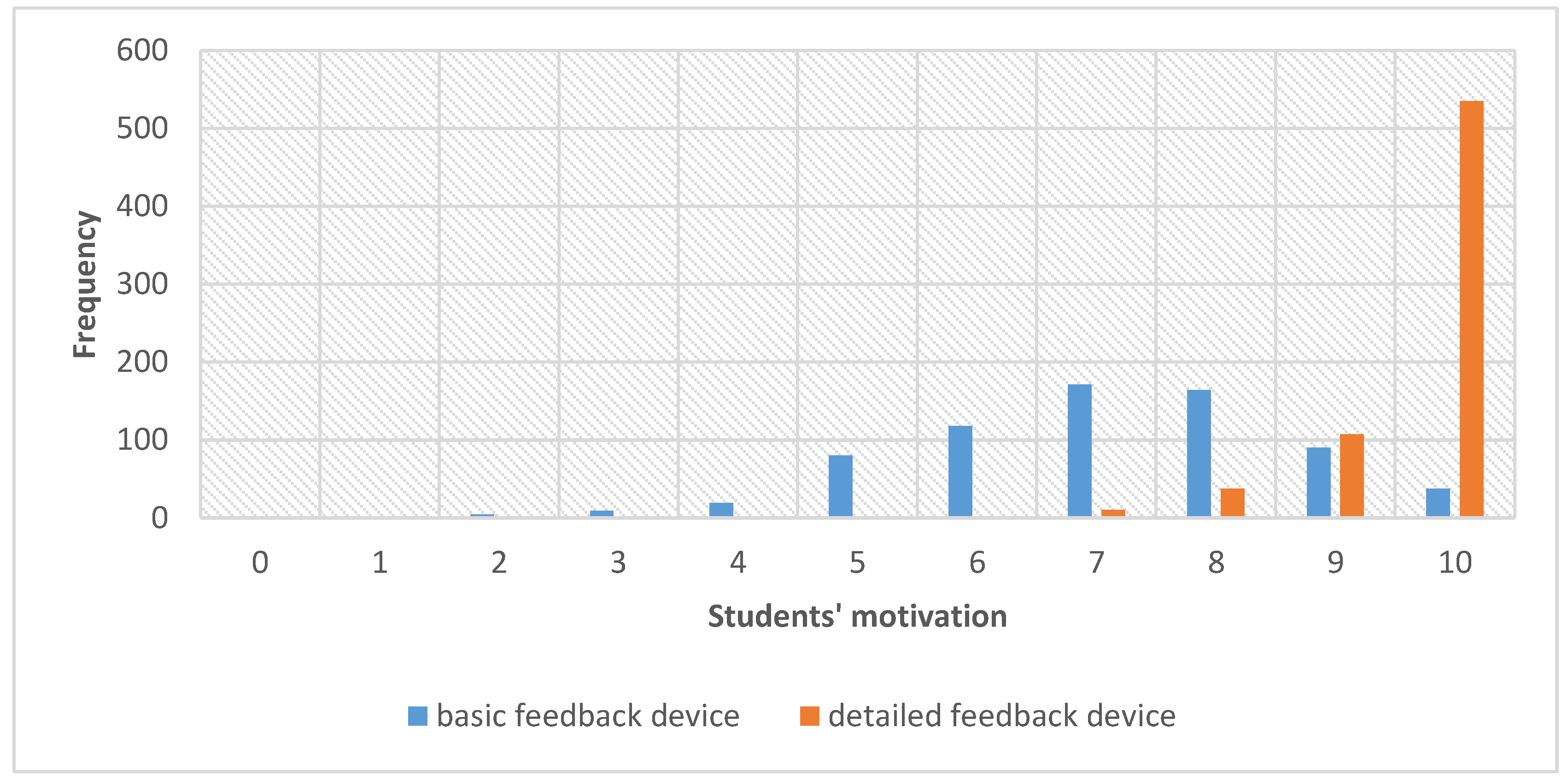
- How would you rate your motivation to learn CPR on a simple mannequin that gives green- or red-light feedback (good/bad)? Did you have a strong desire to improve your skills while practicing on this mannequin?
- 2.
- How do you evaluate your motivation to learn CPR on a high-fidelity mannequin that provides detailed projector feedback on a large screen? While learning on this mannequin, did you have a strong desire to improve your skills?
- 3.
- Did it bother you that the effect of your work was displayed on the projector screen or did it motivate you to work better?
- It bothered me, it intimidated me
- It motivated me to work better, to improve my skills
- It did not bother me or motivate me
- Other
- 4.
- How would you rate your CPR skills overall?
- 5.
- Do you think simple low-fidelity mannequins are sufficient to teach first aid as part of your field of study or should classes be taught on high-fidelity mannequins with advanced feedback?
- Simple low-fidelity phantoms are sufficient
- Classes should be conducted on high-fidelity phantoms with detailed feedback
- 6.
- Faculty
- Dietetics
- Physiotherapy
- Cosmetology
- Medical Rescue
- Other
- 7.
- Year of study
- First
- Second
- Third
- 8.
- Gender
- Male
- Female
- 9.
- Age
- 19
- 20
- 21
- 22
- 23
- 24
- Other
References
- Gräsner, J.-T.; Wnent, J.; Herlitz, J.; Perkins, G.D.; Lefering, R.; Tjelmeland, I.; Koster, R.W.; Masterson, S.; Rossell-Ortiz, F.; Maurer, H.; et al. Survival after out-of-hospital cardiac arrest in Europe—Results of the EuReCa TWO study. Resuscitation 2020, 148, 218–226. [Google Scholar] [CrossRef]
- Strömsöe, A.; Svensson, L.; Axelsson, Å.B.; Claesson, A.; Göransson, K.E.; Nordberg, P.; Herlitz, J. Improved outcome in Sweden after out-of-hospital cardiac arrest and possible association with improvements in every link in the chain of survival. Eur. Hear. J. 2014, 36, 863–871. [Google Scholar] [CrossRef]
- Holmgren, C.; Abdon, N.J.; Bergfeldt, L.; Edvardsson, N.; Herlitz, J.; Karlsson, T.; Nyström, B.; Åstrand, B. Out-of-hospital cardiac arrest: Causes according to autopsy and electrocardiography—Analysis of 781 patients with neither hospital care nor prescribed medication during the preceding two years. Resuscitation 2020, 150, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Perkins, G.D.; Graesner, J.T.; Semeraro, F.; Olasveengen, T.; Soar, J.; Lott, C.; de Voorde, P.V.; Madar, J.; Zideman, D.; Mentzelopoulos, S.; et al. European Resuscitation Council Guidelines 2021: Executive summary. Resuscitation 2021. [Google Scholar] [CrossRef] [PubMed]
- Morley, P.T.; Atkins, D.L.; Finn, J.C.; Maconochie, I.; Nolan, J.P.; Rabi, Y.; Singletary, E.M.; Wang, T.-L.; Welsford, M.; Olasveengen, T.M.; et al. Evidence Evaluation Process and Management of Potential Conflicts of Interest: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Circulation 2020, 142, S28–S40. [Google Scholar] [CrossRef] [PubMed]
- Magid, D.J.; Aziz, K.; Cheng, A.; Hazinski, M.F.; Hoover, A.V.; Mahgoub, M.; Panchal, A.R.; Sasson, C.; Topjian, A.A.; Rodriguez, A.J.; et al. Part 2: Evidence Evaluation and Guidelines Development: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S358–S365. [Google Scholar] [CrossRef]
- Kwiecień-Jaguś, K.; Mędrzycka-Dąbrowska, W.; Galdikienė, N.; Clavero, G.V.; Kopeć, M. A Cross-International Study to Evaluate Knowledge and Attitudes Related to Basic Life Support among Undergraduate Nursing Students—A Questionnaire Study. Int. J. Environ. Res. Public Health 2020, 17, 4116. [Google Scholar] [CrossRef] [PubMed]
- Goodman, J.S.; Wood, R.E.; Hendrickx, M. Feedback Specificity, Exploration, and Learning. J. Appl. Psychol. 2004, 89, 248–262. [Google Scholar] [CrossRef] [Green Version]
- Johnson, D.A. A Component Analysis of the Impact of Evaluative and Objective Feedback on Performance. J. Organ. Behav. Manag. 2013, 33, 89–103. [Google Scholar] [CrossRef]
- Lee, K.; Shon, D.; Oah, S. The Relative Effects of Global and Specific Feedback on Safety Behaviors. J. Organ. Behav. Manag. 2014, 34, 16–28. [Google Scholar] [CrossRef]
- Marshall, J.; Rossett, A. Perceptions of Barriers to the Evaluation of Workplace Learning Programs. Perform. Improv. Q. 2014, 27, 7–26. [Google Scholar] [CrossRef]
- Williams, R.C.; Nafukho, F.M. Technical Training Evaluation Revisited: An Exploratory, Mixed-Methods Study. Perform. Improv. Q. 2015, 28, 69–93. [Google Scholar] [CrossRef]
- Malsy, M.; Leberle, R.; Graf, B. Germans learn how to save lives: A nationwide CPR education initiative. Int. J. Emerg. Med. 2018, 11, 9. [Google Scholar] [CrossRef] [Green Version]
- Swor, R.; Khan, I.; Domeier, R.; Honeycutt, L.; Chu, K.; Compton, S. CPR training and CPR performance: Do CPR-trained bystanders perform CPR? Acad. Emerg. Med. 2006, 13, 596–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawlins, L.; Woollard, M.; Williams, J.; Hallam, P. Effect of listening to Nellie the Elephant during CPR training on performance of chest compressions by lay people: Randomised crossover trial. BMJ 2009, 339, b4707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeung, J.; Meeks, R.; Edelson, D.; Gao, F.; Soar, J.; Perkins, G.D. The use of CPR feedback/prompt devices during training and CPR performance: A systematic review. Resuscitation 2009, 80, 743–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, K.Y.; Ko, Y.C.; Hsieh, M.J.; Chiang, W.C.; Ma, M.H. Interventions to improve the quality of bystander cardiopulmonary resuscitation: A systematic review. PLoS ONE 2019, 14, e0211792. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.Y.; Chiang, W.C.; Hsieh, M.J.; Sun, J.T.; Chang, Y.C.; Ma, M.H. Quality of audio-assisted versus video-assisted dispatcher-instructed bystander cardiopulmonary resuscitation: A systematic review and meta-analysis. Resuscitation 2018, 123, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Suet, G.; Blanie, A.; De Montblanc, J.; Roulleau, P.; Benhamou, D. External Cardiac Massage Training of Medical Students: A Randomized Comparison of Two Feedback Methods to Standard Training. J. Emerg. Med. 2020, 59, 270–277. [Google Scholar] [CrossRef]
- Havel, C.; Schreiber, W.; Trimmel, H.; Malzer, R.; Haugk, M.; Richling, N.; Riedmüller, E.; Sterz, F.; Herkner, H. Quality of closed chest compression on a manikin in ambulance vehicles and flying helicopters with a real time automated feedback. Resuscitation 2010, 81, 59–64. [Google Scholar] [CrossRef]
- Cheng, A.; Brown, L.L.; Duff, J.P.; Davidson, J.; Overly, F.; Tofil, N.M.; Peterson, D.T.; White, M.L.; Bhanji, F.; Bank, I.; et al. Improving Cardiopulmonary Resuscitation with a CPR Feedback Device and Refresher Simulations (CPR CARES Study). JAMA Pediatr. 2015, 169, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Soar, J.; Nolan, J.P.; Böttiger, B.W.; Perkins, G.D.; Lott, C.; Carli, P.; Pellis, T.; Sandroni, C.; Skrifvars, M.B.; Smith, G.B.; et al. European resuscitation council guidelines for resuscitation 2015: Section 3. Adult advanced life support. Resuscitation 2015, 95, 100–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamzeh, J.; Kaur, N.; Bush, P.; Hudon, C.; Schuster, T.; Vedel, I.; Hong, Q.N.; Pluye, P. Towards a comprehensive Questionnaire Origin and Development Appraisal tool: A literature review and a modified nominal group. Educ. Inf. 2019, 35, 7–20. [Google Scholar] [CrossRef]
- World Health Organization. Summary Report of Systematic Reviews for Public Health Emergency Operations Centres: Plans and Procedures; Communication Technology and Infrastructure: Minimum Datasets and Standards; Training and Exercises; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Goniewicz, K.; Goniewicz, M.; Włoszczak-Szubzda, A.; Burkle, F.M.; Hertelendy, A.J.; Al-Wathinani, A.; Molloy, M.S.; Khorram-Manesh, A. The Importance of Pre-Training Gap Analyses and the Identification of Competencies and Skill Requirements of Medical Personnel for Mass Casualty Incidents and Disaster Training. BMC Public Health 2021, 21, 114. [Google Scholar] [CrossRef]
- Medford-Davis, L.N.; Kapur, G.B. Preparing for effective communications during disasters: Lessons from a World Health Organization quality improvement project. Int. J. Emerg. Med. 2014, 7, 15. [Google Scholar] [CrossRef] [Green Version]
- Burkle, F.M.; Bradt, D.A.; Ryan, B.J. Global Public Health Database Support to Population-Based Management of Pandemics and Global Public Health Crises, Part I: The Concept. Prehospital Disaster Med. 2021, 36, 95–104. [Google Scholar] [CrossRef]
- Khorram-Manesh, A. Flexible surge capacity—public health, public education, and disaster management. Heal. Promot. Perspect. 2020, 10, 175–179. [Google Scholar] [CrossRef]
- Kudenchuk, P.J.; Redshaw, J.D.; Stubbs, B.A.; Fahrenbruch, C.E.; Dumas, F.; Phelps, R.; Blackwood, J.; Rea, T.D.; Eisenberg, M.S. Impact of Changes in Resuscitation Practice on Survival and Neurological Outcome After Out-of-Hospital Cardiac Arrest Resulting from Nonshockable Arrhythmias. Circulation 2012, 125, 1787–1794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinberg, M.T.; Olsen, J.A.; Brunborg, C.; Persse, D.; Sterz, F.; Lozano, M., Jr.; Brouwer, M.A.; Westfall, M.; Souders, C.M.; van Grunsven, P.M.; et al. Minimizing pre-shock chest compression pauses in a cardiopulmonary resuscitation cycle by performing an earlier rhythm analysis. Resuscitation 2015, 87, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Goniewicz, K.; Goniewicz, M.; Burkle, F.M.; Khorram-Manesh, A. Cohort research analysis of disaster experience, preparedness, and competency-based training among nurses. PLoS ONE. 2021, 16, e0244488. [Google Scholar] [CrossRef] [PubMed]
- Goniewicz, K.; Goniewicz, M.; Burkle, F.M.; Khorram-Manesh, A. The Impact of Experience, Length of Service, and Workplace Preparedness in Physicians’ Readiness in the Response to Disasters. J. Clin. Med. 2020, 9, 3328. [Google Scholar] [CrossRef] [PubMed]
- Misztal-Okońska, P.; Goniewicz, K.; Hertelendy, A.J.; Khorram-Manesh, A.; Al-Wathinani, A.; Alhazmi, R.A.; Goniewicz, M. How Medical Studies in Poland Prepare Future Healthcare Managers for Crises and Disasters: Results of a Pilot Study. Healthcare 2020, 8, 202. [Google Scholar] [CrossRef] [PubMed]
- Girau, E.; Mura, F.; Bazurro, S.; Casadio, M.; Chirico, M.; Solari, F.; Chessa, M. A mixed reality system for the simulation of emergency and first-aid scenarios. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 5690–5695. [Google Scholar]
- Sharma, S. Improving Emergency Response Training and Decision Making Using a Collaborative Virtual Reality Environment for Building Evacuation. In Proceedings of the International Conference on Human-Computer Interaction 2020, Copenhagen, Denmark, 19–24 July 2020; Springer: Cham, Switzerland, 2020; pp. 213–224. [Google Scholar]
- Biggs, J.B. Teaching for Quality Learning at University: What the Student Does; McGraw-Hill Education: London, UK, 2011. [Google Scholar]
- Hattie, J. The applicability of Visible Learning to higher education. Scholarsh. Teach. Learn. Psychol. 2015, 1, 79. [Google Scholar] [CrossRef] [Green Version]
- Denton, P.; Madden, J.; Roberts, M.; Rowe, P. Students’ response to traditional and computer-assisted formative feedback: A comparative case study. Br. J. Educ. Technol. 2008, 39, 486–500. [Google Scholar] [CrossRef]
- Jordan, S.; Mitchell, T. e-Assessment for learning? The potential of short-answer free-text questions with tailored feedback. Br. J. Educ. Technol. 2009, 40, 371–385. [Google Scholar] [CrossRef] [Green Version]
- Narciss, S.; Huth, K. Fostering achievement and motivation with bug-related tutoring feedback in a computer-based training for written subtraction. Learn. Instr. 2006, 16, 310–322. [Google Scholar] [CrossRef]
- Eshel, R.; Wacht, O.; Schwartz, D. Real-Time Audiovisual Feedback Training Improves Cardiopulmonary Resuscitation Performance: A Controlled Study. Simul. Healthc. 2019, 14, 359–365. [Google Scholar] [CrossRef]
- Lu, T.-C.; Chang, Y.-T.; Ho, T.-W.; Chen, Y.; Lee, Y.-T.; Wang, Y.-S.; Chen, Y.-P.; Tsai, C.-L.; Ma, M.H.-M.; Fang, C.-C.; et al. Using a smartwatch with real-time feedback improves the delivery of high-quality cardiopulmonary resuscitation by healthcare professionals. Resuscitation 2019, 140, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Liu, X.; Steckelberg, A.L. Assessor or assessee: How student learning improves by giving and receiving peer feedback. Br. J. Educ. Technol. 2010, 41, 525–536. [Google Scholar] [CrossRef]
- Tanaka, S.; Tsukigase, K.; Hara, T.; Sagisaka, R.; Myklebust, H.; Birkenes, T.S.; Takahashi, H.; Iwata, A.; Kidokoro, Y.; Yamada, M.; et al. Effect of real-time visual feedback device ‘Quality Cardiopulmonary Resuscitation (QCPR) Classroom’with a metronome sound on layperson CPR training in Japan: A cluster randomized control trial. BMJ Open 2019, 9, e026140. [Google Scholar] [CrossRef] [Green Version]
- Lakomek, F.; Lukas, R.P.; Brinkrolf, P.; Mennewisch, A.; Steinsiek, N.; Gutendorf, P.; Sudowe, H.; Heller, M.; Kwiecien, R.; Zarbock, A.; et al. Real-time feedback improves chest compression quality in out-of-hospital cardiac arrest: A prospective cohort study. PLoS ONE 2020, 15, e0229431. [Google Scholar] [CrossRef] [Green Version]
- Buléon, C.; Parienti, J.J.; Morilland-Lecoq, E.; Halbout, L.; Cesaréo, E.; Dubien, P.Y.; Jardel, B.; Boyer, C.; Husson, K.; Andriamirado, F.; et al. Impacts of chest compression cycle length and real-time feedback with a CPRmeter® on chest compression quality in out-of-hospital cardiac arrest: Study protocol for a multicenter randomized controlled factorial plan trial. Trials 2020, 21, 627. [Google Scholar] [CrossRef]
- Nolan, J.P.; Monsieurs, K.G.; Bossaert, L.; Böttiger, B.W.; Greif, R.; Lott, C.; Madar, J.; Olasveengen, T.M.; Roehr, C.C.; Semeraro, F.; et al. European Resuscitation Council COVID-19 guidelines executive summary. Resuscitation 2020, 153, 45–55. [Google Scholar] [CrossRef]
- Lund-Kordahl, I.; Mathiassen, M.; Melau, J.; Olasveengen, T.M.; Sunde, K.; Fredriksen, K. Relationship between level of CPR training, self-reported skills, and actual manikin test performance—An observational study. Int. J. Emerg. Med. 2019, 12, 2. [Google Scholar] [CrossRef]
- Stiell, I.G.; Brown, S.P.; Nichol, G.; Cheskes, S.; Vaillancourt, C.; Callaway, C.W.; Morrison, L.J.; Christenson, J.; Aufderheide, T.P.; Davis, D.P.; et al. What is the optimal chest compression depth during out-of-hospital cardiac arrest resuscitation of adult patients? Circulation 2014, 130, 1962–1970. [Google Scholar] [CrossRef] [Green Version]
- Monsieurs, K.G.; Nolan, J.P.; Bossaert, L.L.; Greif, R.; Maconochie, I.K.; Nikolaou, N.I.; Perkins, G.D.; Soar, J.; Truhlář, A.; Wyllie, J.; et al. European resuscitation council guidelines for resuscitation 2015: Section 1. Executive summary. Resuscitation 2015, 95, 1–80. [Google Scholar] [CrossRef] [PubMed]
- Niles, D.E.; Sutton, R.M.; Nadkarni, V.M.; Glatz, A.; Zuercher, M.; Maltese, M.R.; Eilevstjønn, J.; Abella, B.S.; Becker, L.B.; Berg, R.A. Prevalence and hemodynamic effects of leaning during CPR. Resuscitation 2011, 82, S23–S26. [Google Scholar] [CrossRef] [Green Version]
- Hansen, C.; Bang, C.; Stærk, M.; Krogh, K.; Løfgren, B. Certified Basic Life Support Instructors Identify Improper Cardiopulmonary Resuscitation Skills Poorly: Instructor Assessments Versus Resuscitation Manikin Data. Simul. Healthc. 2019, 14, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Brennan, E.E.; McGraw, R.C.; Brooks, S.C. Accuracy of instructor assessment of chest compression quality during simulated resuscitation. Can. J. Emerg. Med. 2016, 18, 276–282. [Google Scholar] [CrossRef] [Green Version]
- Baldi, E.; Cornara, S.; Contri, E.; Epis, F.; Fina, D.; Zelaschi, B.; Dossena, C.; Fichtner, F.; Tonani, M.; Di Maggio, M.; et al. Real-time visual feedback during training improves laypersons’ CPR quality: A randomized controlled manikin study. Can. J. Emerg. Med. 2017, 19, 480–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naylor, K.; Torres, K. Transitioning to Online Learning in Basic Life Support Due to the Covid-19 Pandemic, to Battle the Fear of Out of Hospital Cardiac Arrest; a Presentation of Novel Methods. J. Med. Internet Res. 2021, 27108, in press. [Google Scholar] [CrossRef]
- Kim, S.S.; Roh, Y.S. Status of cardiopulmonary resuscitation curricula for nursing students: A questionnaire study. Nurs. Health Sci. 2016, 18, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, J.; Roberge, J.; Bacani, J.; Welsford, M.; Mondoux, S. Implementation of Chest Compression Feedback Technology to Improve the Quality of Cardiopulmonary Resuscitation in the Emergency Department: A Quality Initiative Test-of-change Study. Cureus 2019, 11, e5523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abolfotouh, M.A.; Alnasser, M.A.; Berhanu, A.N.; Al-Turaif, D.A.; Alfayez, A.I. Impact of basic life-support training on the attitudes of health-care workers toward cardiopulmonary resuscitation and defibrillation. BMC Health Serv. Res. 2017, 17, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Faculty | n | % | M (%) | Female | Male |
|---|---|---|---|---|---|
| Dietetics II year | 136 | 20 | 21.33 | 124 | 12 |
| Dietetics IV year | 30 | 4 | 23.12 | 29 | 1 |
| Pharmacy I year | 105 | 15 | 20.08 | 87 | 18 |
| Pharmacy IV year | 41 | 6 | 23.04 | 29 | 12 |
| Physiotherapy I year | 118 | 17 | 19.48 | 76 | 42 |
| Cosmetology I year | 132 | 19 | 19.19 | 132 | 0 |
| Public Health II year | 51 | 7 | 20.29 | 43 | 8 |
| Medical Rescue I year | 81 | 12 | 20.67 | 26 | 55 |
| Total | 694 | 100 | 20.89 | 552 | 157 |
| Feedback Type | Faculty | M | n | Me | Pharmacy IV Year | Dietetics IV Year | Dietetics II Year | Medical Rescue I Year | Physiotherapy I Year | Public Health II Year | Pharmacy I Year |
|---|---|---|---|---|---|---|---|---|---|---|---|
| basic | Cosmetology I year | 372.33 | 132 | 7 | 2404.5 | 1761.0 | 8152.5 | 5286.5 | 6328.5 | 3154.5 | 5147.5 * |
| Pharmacy IV year | 335.59 | 41 | 7 | 469.0 | 2529.5 | 1475.5 | 2191.0 | 853.0 | 1785.5 | ||
| Dietetics IV year | 412.63 | 30 | 8 | 1746.0 | 1113.0 | 1225.0 | 730.0 | 962.0 * | |||
| Dietetics II year | 365.82 | 136 | 7 | 5340.0 | 6607.5 | 3165.5 | 5336.5 * | ||||
| Medical Rescue I year | 372.43 | 81 | 7 | 3954.0 | 1962.5 | 3265.0 | |||||
| Physiotherapy I year | 306.33 | 118 | 7 | 2242.5 | 5813.0 | ||||||
| Public Health II year | 395.00 | 51 | 7 | 1796.0 ** | |||||||
| Pharmacy I year | 282.58 | 105 | 7 | ||||||||
| detailed | Cosmetology I year | 333.42 | 132 | 10 | 2266.0 | 1782.5 | 8402.5 | 4994.0 | 7374.5 | 2985.5 | 5844.5 |
| Pharmacy IV year | 278.71 | 41 | 10 | 461.5 | 2160.5 | 1513.0 | 1905.5 | 766.5 | 1493.0 ** | ||
| Dietetics IV year | 367.92 | 30 | 10 | 1960.5 | 1023.5 | 1685.0 | 755.5 | 1490.0 | |||
| Dietetics II year | 355.14 | 136 | 10 | 4811.0 | 7942.0 | 3290.5 | 6456.5 | ||||
| Medical Rescue I year | 311.65 | 81 | 10 | 4225.5 | 1710.0 | 3351.0 * | |||||
| Physiotherapy I year | 351.60 | 118 | 10 | 2826.0 | 5548.5 | ||||||
| Public Health II year | 372.41 | 51 | 10 | 2563.0 | |||||||
| Pharmacy I year | 387.27 | 105 | 10 |
| Students’ Reaction to Displaying Their Outcomes on a Projector | n | Feedback Preferences | ||
|---|---|---|---|---|
| Basic Feedback | No Preference | Detailed Feedback | ||
| Adverse—embarrassment | n | 2 a | 0 b | 27 b |
| % | 50.00% | 0.00% | 4.22% | |
| Positive—motivation increase | n | 2 a | 43 a | 551 a |
| % | 50.00% | 86.00% | 86.09% | |
| Neutral | n | 0 a | 7 a | 62 a |
| % | 0.00% | 14.00% | 9.69% | |
| Students’ Reaction to Displaying Their Outcomes on a Projector | n | The Belief in the Usefulness of the Given Feedback | |
|---|---|---|---|
| Highest Usefulness of Basic Feedback Device | Highest Usefulness of Detailed Feedback Device | ||
| Adverse—embarrassment | n | 2 a | 27 a |
| % | 5.00% | 4.13% | |
| Positive—motivation increase | n | 33 a | 563 a |
| % | 82.50% | 86.09% | |
| Neutral | n | 5 a | 64 a |
| % | 12.50% | 9.79% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Misztal-Okońska, P.; Goniewicz, K.; Goniewicz, M.; Ranse, J.; Hertelendy, A.J.; Gray, L.; Carlström, E.; Løwe Sørensen, J.; Khorram-Manesh, A. Importance of Immediate Electronic-Based Feedback to Enhance Feedback for First-Time CPR Trainees. Int. J. Environ. Res. Public Health 2021, 18, 3885. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083885
Misztal-Okońska P, Goniewicz K, Goniewicz M, Ranse J, Hertelendy AJ, Gray L, Carlström E, Løwe Sørensen J, Khorram-Manesh A. Importance of Immediate Electronic-Based Feedback to Enhance Feedback for First-Time CPR Trainees. International Journal of Environmental Research and Public Health. 2021; 18(8):3885. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083885
Chicago/Turabian StyleMisztal-Okońska, Patrycja, Krzysztof Goniewicz, Mariusz Goniewicz, Jamie Ranse, Attila J. Hertelendy, Lesley Gray, Eric Carlström, Jarle Løwe Sørensen, and Amir Khorram-Manesh. 2021. "Importance of Immediate Electronic-Based Feedback to Enhance Feedback for First-Time CPR Trainees" International Journal of Environmental Research and Public Health 18, no. 8: 3885. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083885