
A Qualitative Study of the Health Perceptions in the Venezuelan Immigrant Population in Medellín (Colombia) and Its Conditioning Factors

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
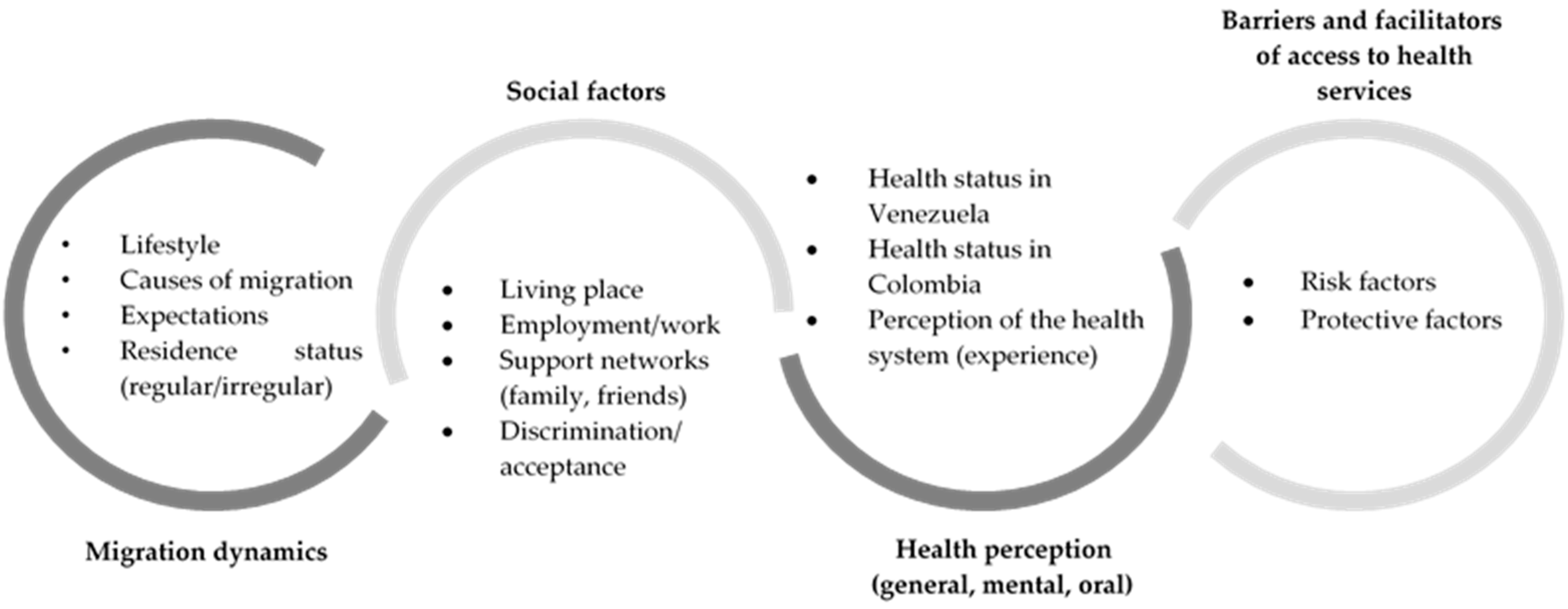
2.1. Approach and Design
2.2. Participants
- Venezuelan immigrants: The study included 17 Venezuelan immigrants of legal age (≥18 years old); men and women with a minimum stay of six months in Colombia and a minimum labor experience of one month were included. Only Venezuelan nationals were considered. In this participation criterion, those who did not have a Colombian citizenship identification card and who had less opportunity for access to various social and health services were taken into account. Those who were Colombian nationals or children of Colombians did not participate. There were no restrictions on immigration status (regular or irregular) for participating. For the selection of participants, theoretical and/or intentional sampling strategies, including snowball sampling and referrals, were used, and patients included those who consulted the emergency service of the Faculty of Dentistry, University of Antioquia, and other institutions that were in contact with the immigrant population. In each case, the voluntary nature of participation was regarded. The final number of participants was determined via saturation, that is, verifying that no new data for the objectives of the study emerged [31]. The sociodemographic characteristics of the Venezuelan participants are summarized in Table 1.
- Key informants: Four health professionals (one medical doctor, one psychologist, and two dentists) from two institutions that were consulted by the immigrant population participated, offering their experiences when assisting the Venezuelan population in Medellín.
- Dental staff: Dentists (n = 6) and dental students (n = 5) from the University of Antioquia participated in two focus groups (FGs) to identify the social and contextual determinants of the immigrant population from the perspective of the people who served this population type in public and private health institutions. These FGs were enough to collect information from the dental staff’s perspectives according to the research objectives.
2.3. Techniques and Instruments of Information Gathering
2.4. Data Analysis
2.5. Ethics Approval and Consent to Participate
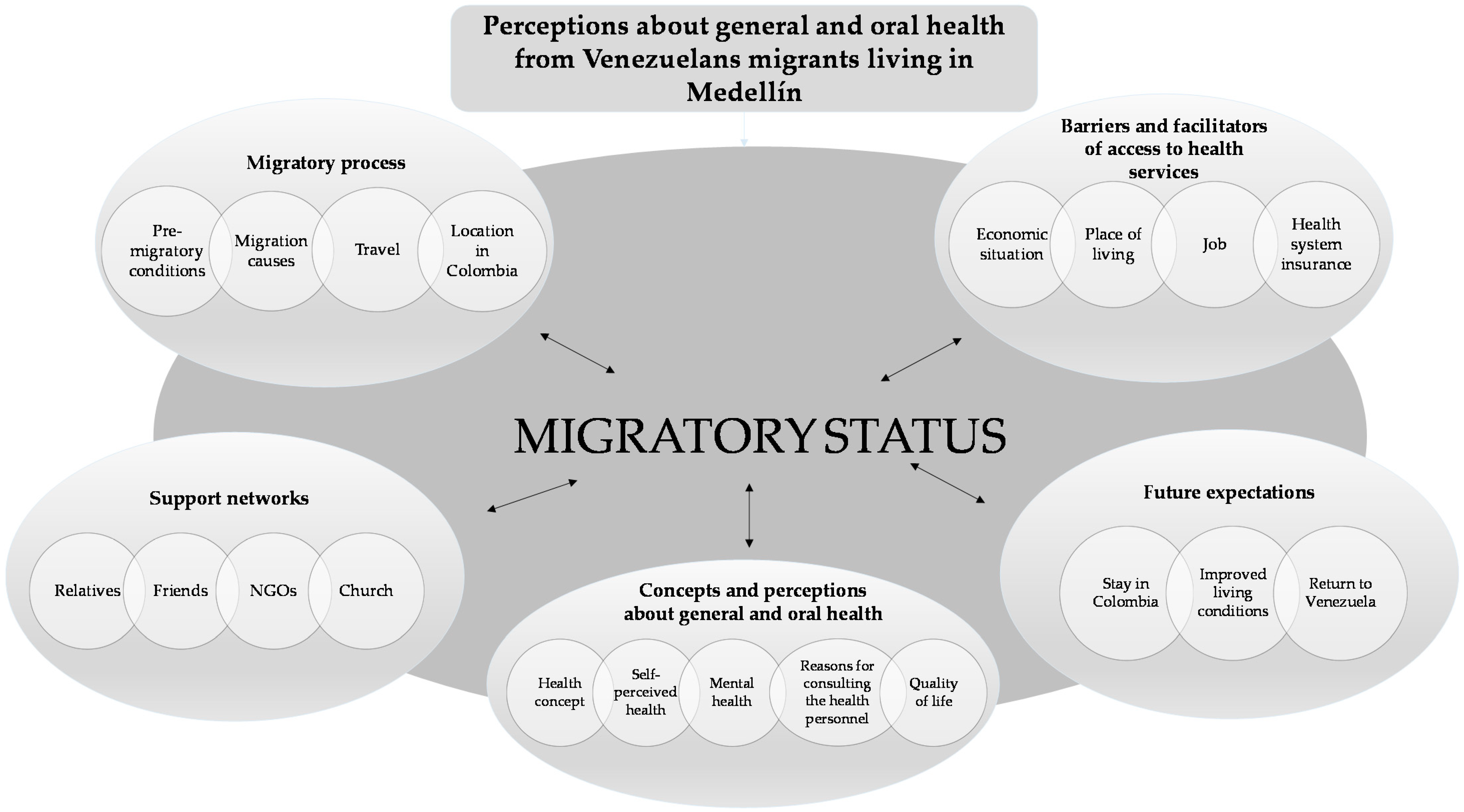
3. Results
3.1. Migratory Process
3.2. Health
3.3. Barriers and Facilitators of Access to Health Services
3.4. Support Networks
3.5. Expectations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- United Nations Department of Economic and Social Affairs, Population Division. International Migration 2020 Highlights; United Nations: New York, NY, USA, 2021. [Google Scholar]
- Crasto, T.C.; Álvarez, M.R. Perceptions of Venezuelan migration: Causes, Spain as a destination, return expectations. [Perceptions of Venezuelan migration: Causes, Spain as a destination, return expectations]. Migraciones 2017, 41, 133–163. [Google Scholar]
- United Nations High Commissioner for Refugees (UNHCR); International Organization for Migration (IOM). Coordination Platform for Refugees and Migrants from Venezuela. Available online: https://r4v.info/en/situations/platform (accessed on 19 February 2021).
- Ministerio de Relaciones Exteriores [Ministry of Foreign Affairs]. Migración Colombia. Radiografía Venezolanos en Colombia. Corte a 30 de Junio [Migration Colombia. Venezuelans Radiography in Colombia. Cut to June 30]. Available online: https://www.migracioncolombia.gov.co/infografias/venezolanos-en-colombia-corte-a-31-de-mayo-de-2020 (accessed on 19 February 2021).
- Fernández-Niño, J.A.; Luna-Orozco, K.; Navarro-Lechuga, E.; Flórez-García, V.; Acosta-Reyes, J.; Solano, A.; Bravo, E.; Goenaga, E. Necesidades percibidas de salud por los migrantes desde Venezuela en el asentamiento de Villa Caracas—Barranquilla, 2018: Reporte de caso en salud pública. Rev. Univ. Ind. Santander. Salud 2018, 50, 269–276. [Google Scholar] [CrossRef]
- Fernández-Niño, J.A.; Vásquez-Rodríguez, A.B.; Florez-García, V.A.; Rojas-Botero, M.L.; Luna-Orozco, K.; Navarro-Lechuga, E.; Acosta-Reyes, J.L.; Rodríguez-Perez, D.A. Modos de vida y estado de salud de migrantes en un asentamiento de Barranquilla, 2018. Rev. Salud Pública 2018, 20, 530–538. [Google Scholar] [CrossRef]
- Agudelo-Suárez, A.A.; Vargas-Valencia, M.Y.; Vahos-Arias, J.; Ariza-Sosa, G.; Rojas-Gutiérrez, W.J.; Ronda-Pérez, E. Precarious employment and health: A qualitative study in Venezuelan immigrant population in Colombia. J. Migr. Health 2020, 1–2, 100009. [Google Scholar] [CrossRef]
- Hargreaves, S.; Rustage, K.; Nellums, L.B.; McAlpine, A.; Pocock, N.; Devakumar, D.; Aldridge, R.W.; Abubakar, I.; Kristensen, K.L.; Himmels, J.W.; et al. Occupational health outcomes among international migrant workers: A systematic review and meta-analysis. Lancet Glob. Health 2019, 7, e872–e882. [Google Scholar] [CrossRef] [Green Version]
- Arici, C.; Ronda-Pérez, E.; Tamhid, T.; Absekava, K.; Porru, S. Occupational Health and Safety of Immigrant Workers in Italy and Spain: A Scoping Review. Int. J. Environ. Res. Public Health 2019, 16, 4416. [Google Scholar] [CrossRef] [Green Version]
- Bas-Sarmiento, P.; Saucedo-Moreno, M.J.; Fernández-Gutiérrez, M.; Poza-Méndez, M. Mental Health in Immigrants Versus Native Population: A Systematic Review of the Literature. Arch. Psychiatr. Nurs. 2017, 31, 111–121. [Google Scholar] [CrossRef]
- Blukacz, A.; Cabieses, B.; Markkula, N. Inequities in mental health and mental healthcare between international immigrants and locals in Chile: A narrative review. Int. J. Equity Health 2020, 19, 1–15. [Google Scholar] [CrossRef]
- Metusela, C.; Ussher, J.; Perz, J.; Hawkey, A.; Morrow, M.; Narchal, R.; Estoesta, J.; Monteiro, M. “In My Culture, We Don’t Know Anything About That”: Sexual and Reproductive Health of Migrant and Refugee Women. Int. J. Behav. Med. 2017, 24, 836–845. [Google Scholar] [CrossRef]
- Klein, J.; Knesebeck, O.V.D. Inequalities in health care utilization among migrants and non-migrants in Germany: A systematic review. Int. J. Equity Health 2018, 17, 160. [Google Scholar] [CrossRef] [Green Version]
- Gil-González, D.; Carrasco-Portiño, M.; Vives-Cases, C.; Agudelo-Suárez, A.A.; Bolea, R.C.; Ronda-Pérez, E. Is health a right for all? An umbrella review of the barriers to health care access faced by migrants. Ethn. Health 2015, 20, 523–541. [Google Scholar] [CrossRef]
- Delgado-Angulo, E.K.; Marcenes, W.; Harding, S.; Bernabé, E. Ethnicity, migration status and dental caries experience among adults in East London. Community Dent. Oral Epidemiol. 2018, 46, 392–399. [Google Scholar] [CrossRef]
- Pabbla, A.; Duijster, D.; Grasveld, A.; Sekundo, C.; Agyemang, C.; van der Heijden, G. Oral Health Status, Oral Health Behaviours and Oral Health Care Utilisation Among Migrants Residing in Europe: A Systematic Review. J. Immigr. Minor. Health 2021, 23, 373–388. [Google Scholar] [CrossRef]
- Agudelo-Suárez, A.A.; Vivares-Builes, A.M.; Muñoz-Pino, N.; Martínez-Martínez, J.M.; Reid, A.; Ronda-Pérez, E. Oral Health-Related Quality of Life in Native and Immigrant Populations in the PELFI Study in Spain. Int. J. Environ. Res. Public Health 2019, 16, 1796. [Google Scholar] [CrossRef] [Green Version]
- Reda, S.F.; Reda, S.M.; Thomson, W.M.; Schwendicke, F. Inequality in Utilization of Dental Services: A Systematic Review and Meta-analysis. Am. J. Public Health 2018, 108, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- Agudelo-Suárez, A.A.; Muñoz-Pino, N.; Vivares-Builes, A.M.; Ronda-Pérez, E. Oral Health and Oral Health Service Utilization in Native and Immigrant Population: A Cross-Sectional Analysis from the PELFI Cohort in Spain. J. Immigr. Minor. Health 2020, 22, 484–493. [Google Scholar] [CrossRef] [PubMed]
- Dahlan, R.; Badri, P.; Saltaji, H.; Amin, M. Impact of acculturation on oral health among immigrants and ethnic minorities: A systematic review. PLoS ONE 2019, 14, e0212891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xhihani, B.; Rainchuso, L.; Smallidge, D.; Dominick, C. Oral Health Beliefs, Attitudes, and Practices of Albanian Immigrants in the United States. J. Community Health 2016, 42, 235–241. [Google Scholar] [CrossRef]
- Gao, X.; Chan, C.W.; Mak, S.L.; Ng, Z.; Kwong, W.H.; Kot, C.C.S. Oral Health of Foreign Domestic Workers: Exploring the Social Determinants. J. Immigr. Minor. Health 2013, 16, 926–933. [Google Scholar] [CrossRef]
- de Diego-Cordero, R.; Romero-Saldaña, M.; Jigato-Calero, A.; Badanta, B.; Lucchetti, G.; Vega-Escaño, J. “Looking for Better (Job) Opportunities”: A Qualitative Analysis of the Occupational Health of Immigrants in Southern Spain. Work. Health Saf. 2021. [Google Scholar] [CrossRef]
- Nedungalaparambil, N.M.; Kumar, R.; Mohanan, N. Emergency and primary care collaboration during COVID-19 pandemic: A quick systematic review of reviews. J. Fam. Med. Prim. Care 2020, 9, 3856–3862. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Niño, J.A.; Cubillos-Novella, A.; Bojórquez, I.; Rodríguez, M. Recommendations for the response against COVID-19 in migratory contexts under a closed border: The case of Colombia. Biomédica 2020, 40, 68–72. [Google Scholar] [CrossRef]
- Chai, H.; Gao, S.; Chen, K.; Duangthip, D.; Lo, E.; Chu, C. A Concise Review on Qualitative Research in Dentistry. Int. J. Environ. Res. Public Health 2021, 18, 942. [Google Scholar] [CrossRef] [PubMed]
- Isaacs, A.N. An overview of qualitative research methodology for public health researchers. Int. J. Med. Public Health 2014, 4, 318. [Google Scholar] [CrossRef] [Green Version]
- Murillo-Pedrozo, A.M.; Agudelo-Suárez, A.A. La migración sur/sur como un determinante social de impacto en las desigualdades e inequidades en salud bucal en Latinoamérica. Rev. Peru. Med. Exp. Salud Pública 2019, 36, 692–699. [Google Scholar] [CrossRef] [Green Version]
- Savage, J. Ethnography and health care. BMJ 2000, 321, 1400–1402. [Google Scholar] [CrossRef] [Green Version]
- Higginbottom, G.M.; Pillay, J.J.; Boadu, N.Y. Guidance on Performing Focused Ethnographies with an Emphasis on Healthcare Research. Qual. Rep. 2013, 18, 1–16. [Google Scholar]
- Saunders, B.; Sim, J.; Kingstone, T.; Baker, S.; Waterfield, J.; Bartlam, B.; Burroughs, H.; Jinks, C. Saturation in qualitative research: Exploring its conceptualization and operationalization. Qual. Quant. 2018, 52, 1893–1907. [Google Scholar] [CrossRef]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aruj, R.S. Causas, consecuencias, efectos e impacto de las migraciones en Latinoamérica [Causes, consequences, effects and impact of the migrations in Latin America]. Pap. Poblac. 2008, 14, 95–116. [Google Scholar]
- Agudelo Suarez, A.A.; Ronda Perez, E.; Benavides, F.G. Occupational Health. In Migration and Health in the European Union; Rechel, B., Mladovsky, P., Devillé, W., Rijks, B., Petrova-Benedict, R., Mckee, M., Eds.; McGraw Hill-Open University Press: Glasgow, UK, 2011; pp. 155–168. [Google Scholar]
- Lee, H.; Seo, S.; Kang, R.; Kim, Y.; Hyun, H.-K. Increasing access to oral healthcare for marriage-immigrant women in South Korea: Programme design to policy recommendation. Int. Dent. J. 2019, 69, 354–360. [Google Scholar] [CrossRef]
- Gallegos-Juárez, I.; Ponce-Samaniego, Y.; Sempere-Selva, M.; Ramos-Rincón, J. Estilos de vida, salud autopercibida y utilización de los servicios sanitarios en inmigrantes de Paraguay y Bolivia residentes en la ciudad de Elche. SEMERGEN Med. Fam. 2012, 38, 432–438. [Google Scholar] [CrossRef]
- Helgesson, M.; Johansson, B.; Nordquist, T.; Vingård, E.; Svartengren, M. Healthy migrant effect in the Swedish context: A register-based, longitudinal cohort study. BMJ Open 2019, 9, e026972. [Google Scholar] [CrossRef] [PubMed]
- Sivakumar, V.; Jain, J.; Battur, H.; Patil, P.U.; Lingaraj, S.; Palliyal, S. Exploring Oral Health Beliefs and Behaviour Among Tibetan Immigrants of Bylakkupe. Oral Health Prev. Dent. 2016, 14, 111–116. [Google Scholar]
- Bianucci, R.; Charlier, P.; Perciaccante, A.; Lippi, D.; Appenzeller, O. The “Ulysses syndrome”: An eponym identifies a psychosomatic disorder in modern migrants. Eur. J. Intern. Med. 2017, 41, 30–32. [Google Scholar] [CrossRef]
- Sanchez, M.; Diez, S.; Fava, N.M.; Cyrus, E.; Ravelo, G.; Rojas, P.; Li, T.; Cano, M.A.; De La Rosa, M. Immigration Stress among Recent Latino Immigrants: The Protective Role of Social Support and Religious Social Capital. Soc. Work. Public Health 2019, 34, 279–292. [Google Scholar] [CrossRef] [PubMed]
- Urzúa, A.; Caqueo-Urízar, A.; Carvajal, C.C.; Páez, L.R. ¿El apoyo social mediatiza el efecto negativo del estrés por aculturación en la salud? un estudio en colombianos y peruanos inmigrantes en el norte de Chile [Does social support mediate the negative effect of stress on acculturation in health? A study in immigrant Colombians and Peruvians in northern Chile]. Interciencia 2017, 42, 818–822. [Google Scholar]
- Urzúa, A.; Heredia, O.; Caqueo-Urízar, A. Salud mental y estrés por aculturación en inmigrantes sudamericanos en el norte de Chile [Mental health and stress by acculturation in immigrants from South America in northern Chile]. Rev. Med. Chile 2016, 144, 563–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abadía Barrero, C.E.; Oviedo Manrique, D.G. Itinerarios burocráticos de la salud en Colombia: La burocracia neoliberal, su estado y la ciudadanía en salud [Health care related bureaucratic itineraries in Colombia: The neoliberal bureaucracy, its condition and the citizenry regarding health]. Rev. Gerenc Políticas Salud 2010, 9, 86–102. [Google Scholar]
- Tanahashi, T. Health service coverage and its evaluation. Bull. World Health Organ. 1978, 56, 295–303. [Google Scholar]
- Adauy, M.H.; Angulo, L.P.; Sepúlveda, A.M.J.; Sanhueza, X.A.; Becerra, I.D.; Morales, J.V. Barreras y facilitadores de acceso a la atención de salud: Una revisión sistemática cualitativa. Rev. Panam. Salud Pública 2013, 33, 223–229. [Google Scholar] [CrossRef] [Green Version]
- Hart, J.T. The Inverse Care Law. Lancet 1971, 297, 405–412. [Google Scholar] [CrossRef] [Green Version]
- Grabovschi, C.; Loignon, C.; Fortin, M. Mapping the concept of vulnerability related to health care disparities: A scoping review. BMC Health Serv. Res. 2013, 13, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galon, T.; Briones-Vozmediano, E.; Od, A.A.A.; Felt, E.B.; Benavides, F.G.; Ronda-Pérez, E. Understanding sickness presenteeism through the experience of immigrant workers in a context of economic crisis. Am. J. Ind. Med. 2014, 57, 950–959. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Boccuzzi, M.; Pold, A.; Krsek, M. The alarming burden of non-communicable diseases in COVID-19 new normal: Implications on oral health. Oral Dis. 2021, 27, 791–792. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | n (%) |
|---|---|
| Sex | |
| Male | 8 (47) |
| Female | 9 (53) |
| Zone | |
| Urban (cities and municipalities) | 14 (82) |
| Rural (sidewalks, villages, little towns) | 3 (18) |
| Age (years), mean (range) | 37 (19–56) |
| Time of residence in Colombia (months), mean (range) | 24 (9–60) |
| Medical antecedents in Venezuela | |
| Yes | 3 (18) |
| No | 14 (82) |
| Employment situation | |
| Yes | 7 (41) |
| No | 10 (59) |
| Presence of work contract | |
| Yes | 3 (18) |
| No | 14 (82) |
| Health insurance | |
| Yes | 6 (35) |
| No | 11 (65) |
| Marital status | |
| Single | 6 (35) |
| Married/cohabitated | 10 (59) |
| Widow | 2 (12) |
| Education | |
| Primary | 1 (6) |
| Incomplete secondary | 1 (6) |
| Complete secondary | 5 (29.4) |
| Technical studies | 5 (29.4) |
| University | 5 (29.4) |
| Categories | Keywords | Verbatim Extracts form Participants’ Discourses |
|---|---|---|
| (1) Migratory process | Motivations | (a) “[I am] seeking a better future for my family and my babies.” (I-12, female, 23 years old) |
| (b) “Because in Venezuela there was no food, there was no medicine, there was nothing, looking for a better one here.” (I-6, female, 46 years old) | ||
| (c) “Because of the situation in the country, because of the circumstances that all Venezuelans are going through, because of this government, a dictatorship.” (I-3, male, 29 years old) | ||
| The trip | (d) “In a chirrinchera [typical Venezuelan word] … a chirrinchera is a truck that has rails on the sides, and there, one comes standing. For all that is La Guajira [Colombian region], grabbing the trails of Maicao [Colombian municipality].” (I-9, female, 56 years old) | |
| (e) “Along the trails and that day, a family member drowned because it was in the rain, and a family member drowned when crossing the river. We passed … Well, that was horrible.” (I-6, female, 46 years old) | ||
| Destination choice | (f) “It is the closest place we have. Even though Brazil is also close to Venezuela, the closest is Colombia.” (I-8, female, 37 years old) | |
| (g) “Here in Medellín [Colombia], we had an acquaintance. He was a comadre [relative] of my wife, who was here in Medellín. She received us for three days.” (I-7, male, 33 years old) | ||
| (2) Health | Health concept | (a) “For me, health is the physical and mental state that people have and that must be guaranteed and supported by a system.” (I-4, male, 35 years old) |
| (b) “To have a better quality of life, being in health, because if one does not have good health, how can one have a better quality of life to work, to do other things, to take care of even the family.” (I-14, female, 44 years old) | ||
| Perception of current health status | (c) “Well, thank God. Since I got here, I have never had a difficulty such as telling you that I have been in bed. Thank God, no.” (I-16, male, 34 years old) | |
| (d) “Today, I feel a little bad, from the colon, and I don’t sleep. Sometimes I don’t sleep because sometimes it won’t let me sleep [due to] a lot of pain.” (I-2, male, 45 years old) | ||
| (e) “Right now, it has improved because here, at least you can get the right medicine for hypertension both for me and my dad.” (I-13, male, 45 years old) | ||
| Oral health status | (f) “I came from Venezuela. I had work done on my tooth [molar], but only halfway—that is, I could not finish it.” (I-11, male, 40 years old) | |
| (g) “I consider that much of this burden of diseases came from Venezuela, which obviously worsened. Yes, [due to] cavities not attended here, that come from there and are not treated here [and] the difficult access here, they became worse. That’s the reason for the emergency care for them.” (KI, dentist, female, public health professional, public sector) | ||
| (h) “Main reasons for [dental] consultation (...) they [Venezuelans] always come for many root tips of teeth, many dental caries, many pulpitis …” (FG-1, dentist, public and private sectors) | ||
| Mental health | (i) “I am currently consulting with a psychologist because I manage a very high level of anxiety and stress.” (I-4, male, 35 years old) | |
| (j) “The most frequent, precisely that one, [is] that of problems in cultural adaptation, and that is one of those that prevail within these reasons for consultation and that there is a pattern that is repetitive and that one would not only believe that occurs in adults. No, it really occurs in all types of populations.” (KI, psychologist, female, NGO) | ||
| (k) “My house [Venezuela], of course. I was also in my comfort zone, my house, my job, where I lived, what was normal, my routine, my family, my dad [referring to the family in Venezuela]” (I-15, female, 42 years old) | ||
| (3) Barriers and facilitators of access to health services | Special Permission for Residence (PEP) | (a) “As we do not have passports, right now, they [the government] are taking out the PEP, unlike those people who have stamped their passports. Since we do not have passports because we cannot get it, we would have to wait for Colombian migration to take a day to get PEP.” (I-8, female, 37 years old) |
| (b) “The first barrier is the link. If Venezuelans do not have the temporary or special permit, they cannot link as they want. For me, that is the first barrier. Once they have permission, they can be linked.” (FG-1, dentist, public and private sectors) | ||
| Cost | (c) “No, but here, I have not even been able to go to a dentist due to the same situation that, here, everything is very expensive.” (I-1, female, 45 years old) | |
| Employment/working conditions | (d) “I was working in Parque Berrío [a main square in the city], in a sewing workshop. They make sheets, cut sheets, make quilts, and all that.” (I-17, male, 31 years old) | |
| (e) “I work daily selling manillas [a kind of souvenir] on buses. I live with my wife [and] my two daughters. My wife works the same way, selling manillas.” (I-7, male, 33 years old) | ||
| (f) “They [Venezuelans] are afraid of losing their jobs … In order not to miss their job, they don’t want an appointment on a Saturday because they don’t work on Sunday. So, they don’t want to use the sick leave because they don’t want to miss their job because if they miss job, they get fired.” (FG-1, dentist, public and private sector) | ||
| Housing | (g) “Here, to rent a house they don’t allow you with a PEP; you have to have real property, you have to have a guarantor. You have to have all those kinds of documents, and if you don’t have a document to support you, they don’t give you anything. So, it is very difficult to be from one place to another.” (I-17, male, 31 years old) | |
| (h) “We are in a very little room—how to say, three by three practically … we are eight: she [sister] with her three daughters and I with my family. (I-13, male, 45 years old) | ||
| Affiliation to the General Social Security System (health insurance) | (i) “My mother and grandmother did enter with border permits. They do not have PEP—that is, since they have not taken a census again, I have not been able to get them out. If my mother had the permit, I would already have it affiliated with the EPS [Acronym in Spanish for Empresas Promotoras de Salud, in English means: health maintenance organization]. That is the limitation that I have.” (I-11, male, 40 years old) | |
| (j) “I am very calm in the aspect of health because I already have my wife and my daughter linked to the EPS—that is, that tranquility that if I need a consultation, I [can] easily ask for it.” (I-11, male, 40 years old) | ||
| (4) Support networks | Family | (a) “Well, since he [a friend] has his family here, here, where we have rented, is family. The man above is his cousin.” (EI-1, female, 45 years old) |
| Nongovernmental organizations (NGOs) | (b) “The UNHCR [NGO with an office in Medellín] gave me the appointment by phone and told me that I had an appointment here [Famicove, an NGO located in Medellín]. I didn’t even know where it was, even the lady who is seeing herself right now came and was the one who accompanied me to look for the address of Famicove.” (I-E09, female, 56 years old) | |
| Church | (c) “Those from the church also arrived, how do I say, well, those who work in the rectory also arrived, saw me, [health staff] took my blood pressure. Almost every day, they went to the house, they took my blood pressure, they [health staff] gave me the pill.” (I-6, female, 45 years old) | |
| (5) Expectations | Short term | (a) “Our plans right now … [are] to get something more comfortable for ourselves because since … we are five people who live here and, well, we are very, very small, but we have … plans to go to something bigger.” (I-1, female, 45 years old) |
| (b) “Stay as we are right now, look for a good job, why do we do, without a job we can’t do anything else...” (I-17, male, 31 years old) | ||
| Medium term | (c) “My plans for the future [are to] validate my career [and] practice my profession here. I want to do another specialization, but I want to do it here and nothing else. [I want to] get a job in my area.” (I-4, male, 35 years old) | |
| Long term | (d) “Right now, in the situation we are in [all migrants], we wanted to return, but right now in Venezuela, things are much worse than when we came.” (I-7, male, 33 years old) | |
| (e) “The truth is, yes, I would like…, but right now, the only way for me to return is not to stay but to go visit, let the government fall, visit the family again, which is what one misses the most.” (I-16, male, 34 years old) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murillo-Pedrozo, A.M.; Martínez-Herrera, E.; Ronda-Pérez, E.; Agudelo-Suárez, A.A. A Qualitative Study of the Health Perceptions in the Venezuelan Immigrant Population in Medellín (Colombia) and Its Conditioning Factors. Int. J. Environ. Res. Public Health 2021, 18, 3897. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083897
Murillo-Pedrozo AM, Martínez-Herrera E, Ronda-Pérez E, Agudelo-Suárez AA. A Qualitative Study of the Health Perceptions in the Venezuelan Immigrant Population in Medellín (Colombia) and Its Conditioning Factors. International Journal of Environmental Research and Public Health. 2021; 18(8):3897. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083897
Chicago/Turabian StyleMurillo-Pedrozo, Andrés M., Eliana Martínez-Herrera, Elena Ronda-Pérez, and Andrés A. Agudelo-Suárez. 2021. "A Qualitative Study of the Health Perceptions in the Venezuelan Immigrant Population in Medellín (Colombia) and Its Conditioning Factors" International Journal of Environmental Research and Public Health 18, no. 8: 3897. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083897