
Aggressive Driving Behaviours in Cannabis Users. The Influence of Consumer Characteristics


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Visual Function
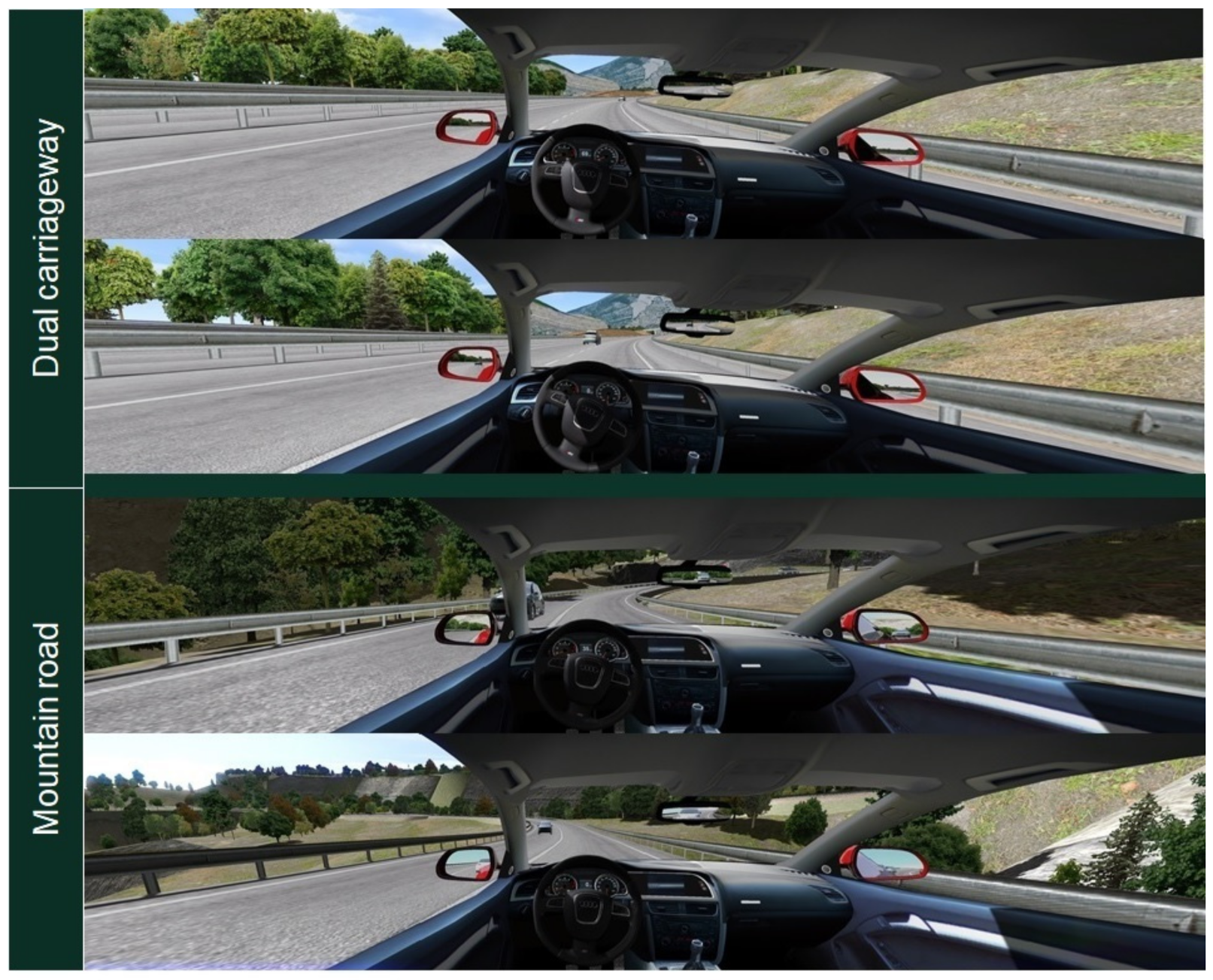
2.3. Driving Simulator
2.4. Self-Reported Data: Demographics and DDDI Questionnaire
2.5. Procedure
2.6. Data Analysis
3. Results
3.1. Visual Assessment
3.2. Risky Driving: Speed Management
3.3. Driving under the Influence of Cannabis (DUIC): Self-Perceived Risk and Behaviour
3.3.1. General Profile of Use and Perception of Risk in Driving
3.3.2. Dula Dangerous Driving Index
3.3.3. Correlations between Visual Outcomes, Speed Management, and Self-Reported Data
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). European Drug Report 2020: Trends and Developments; Publications Office of the European Union: Luxembourg, 2020. [Google Scholar]
- Gjerde, H.; Strand, M.C.; Mørland, J. Driving Under the Influence of Non-Alcohol Drugs—An Update Part I: Epidemiological Studies. Forensic Sci. Rev. 2015, 27, 89–113. [Google Scholar] [PubMed]
- Hartman, R.L.; Huestis, M.A. Cannabis Effects on Driving Skills. Clin. Chem. 2013, 59, 478–492. [Google Scholar] [CrossRef] [PubMed]
- Asbridge, M.; Hayden, J.A.; Cartwright, J.L. Acute cannabis consumption and motor vehicle collision risk: Systematic review of observational studies and meta-analysis. BMJ 2012, 344, e536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gjerde, H.; Mørland, J. Risk for involvement in road traffic crash during acute cannabis intoxication. Addiction 2016, 111, 1492–1495. [Google Scholar] [CrossRef] [Green Version]
- Romano, E.; Voas, R.B.; Camp, B. Cannabis and crash responsibility while driving below the alcohol per se legal limit. Accid. Anal. Prev. 2017, 108, 37–43. [Google Scholar] [CrossRef]
- Bondallaz, P.; Favrat, B.; Chtioui, H.; Fornari, E.; Maeder, P.; Giroud, C. Cannabis and its effects on driving skills. Forensic Sci. Int. 2016, 268, 92–102. [Google Scholar] [CrossRef]
- Alvarez, L.; Colonna, R.; Kim, S.; Chen, C.; Chippure, K.; Grewal, J.; Kimm, C.; Randell, T.; Leung, V. Young and under the influence: A systematic literature review of the impact of cannabis on the driving performance of youth. Accid. Anal. Prev. 2021, 151, 105961. [Google Scholar] [CrossRef]
- Ramaekers, J.G. Driving Under the Influence of Cannabis. JAMA 2018, 319, 1433–1434. [Google Scholar] [CrossRef]
- Hartman, R.L.; Brown, T.L.; Milavetz, G.; Spurgin, A.; Pierce, R.S.; Gorelick, D.A.; Gaffney, G.; Huestis, M.A. Cannabis Effects on Driving Lateral Control with and without Alcohol. Drug Alcohol Depend. 2015, 154, 25–37. [Google Scholar] [CrossRef] [Green Version]
- Hartman, R.L.; Brown, T.L.; Milavetz, G.; Spurgin, A.; Pierce, R.S.; Gorelick, D.A.; Gaffney, G.; Huestis, M.A. Cannabis effects on driving longitudinal control with and without alcohol. J. Appl. Toxicol. 2016, 36, 1418–1429. [Google Scholar] [CrossRef]
- Ortiz-Peregrina, S.; Ortiz, C.; Castro-Torres, J.J.; Jiménez, J.R.; Anera, R.G. Effects of Smoking Cannabis on Visual Function and Driving Performance. A Driving-Simulator Based Study. Int. J. Environ. Res. Public Health 2020, 17, 9033. [Google Scholar] [CrossRef]
- Bolla, K.I.; Brown, K.; Eldreth, D.; Tate, K.; Cadet, J.L. Dose-related neurocognitive effects of marijuana use. Neurology 2002, 59, 1337–1343. [Google Scholar] [CrossRef] [Green Version]
- Meier, M.H.; Caspi, A.; Ambler, A.; Harrington, H.L.; Houts, R.; Keefe, R.S.E.; McDonald, K.; Ward, A.; Poulton, R.; Moffitt, T.E. Persistent cannabis users show neuropsychological decline from childhood to midlife. Proc. Natl. Acad. Sci. USA 2012, 109, E2657–E2664. [Google Scholar] [CrossRef] [Green Version]
- Verdejo-García, A.; Rivas-Pérez, C.; López-Torrecillas, F.; Pérez-García, M. Differential impact of severity of drug use on frontal behavioral symptoms. Addict. Behav. 2006, 31, 1373–1382. [Google Scholar] [CrossRef]
- Solowij, N. Do cognitive impairments recover following cessation of cannabis use? Life Sci. 1995, 56, 2119–2126. [Google Scholar] [CrossRef]
- Ortiz-Peregrina, S.; Ortiz, C.; Casares-López, M.; Jiménez, J.R.; Anera, R.G. Effects of cannabis on visual function and self-perceived visual quality. Sci. Rep. 2021, 11, 1655. [Google Scholar] [CrossRef]
- Wood, J.M. 2015 Glenn A. Fry Award Lecture: Driving toward a New Vision: Understanding the Role of Vision in Driving. Optom. Vis. Sci. 2019, 96, 626–636. [Google Scholar] [CrossRef]
- Dasilva, M.; Grieve, K.L.; Rivadulla, C. Cannabis, Endocannabinoid CB1 Receptors, and the Neuropathology of Vision. In Neuropathology of Drug Addictions and Substance Misuse; Elsevier: Cham, Switzerland, 2016; pp. 738–748. ISBN 9780128002131. [Google Scholar]
- Schwitzer, T.; Schwan, R.; Angioi-Duprez, K.; Ingster-Moati, I.; Lalanne, L.; Giersch, A.; Laprevote, V. The cannabinoid system and visual processing: A review on experimental findings and clinical presumptions. Eur. Neuropsychopharmacol. 2015, 25, 100–112. [Google Scholar] [CrossRef]
- Dawson, W.W.; Jiménez-Antillon, C.F.; Perez, J.M.; Zeskind, J.A. Marijuana and vision-after ten years’ use in Costa Rica. Investig. Ophthalmol. Vis. Sci. 1977, 16, 689–699. [Google Scholar]
- Adams, A.J.; Brown, B.; Haegerstrom-Portnoy, G.; Flom, M.C.; Jones, R.T. Marijuana, Alcohol, and Combined Drug Effects on the Time Course of Glare Recovery. Psychopharmacology 1978, 56, 81–86. [Google Scholar] [CrossRef]
- Huestegge, L.; Radach, R.; Kunert, H.J. Long-term effects of cannabis on oculomotor function in humans. J. Psychopharmacol. 2009, 23, 714–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lalanne, L.; Ferrand-Devouge, E.; Kirchherr, S.; Rauch, L.; Koning, E.; Speeg, C.; Laprevote, V.; Giersch, A. Impaired contrast sensitivity at low spatial frequency in cannabis users with early onset. Eur. Neuropsychopharmacol. 2017, 27, 1289–1297. [Google Scholar] [CrossRef] [PubMed]
- Mikulskaya, E.; Martin, F.H. Contrast sensitivity and motion discrimination in cannabis users. Psychopharmacology 2018, 235, 2459–2469. [Google Scholar] [CrossRef] [PubMed]
- Agramunt, S.; Meuleners, L.B.; Fraser, M.L.; Chow, K.C.; Ng, J.Q.; Raja, V. First and second eye cataract surgery and driver self-regulation among older drivers with bilateral cataract: A prospective cohort study. BMC Geriatr. 2018, 18, 51. [Google Scholar] [CrossRef] [Green Version]
- Agramunt, S.; Meuleners, L.B.; Fraser, M.L.; Chow, K.C.; Ng, J.Q.; Raja, V.; Morlet, N. Do older drivers with bilateral cataract self-regulate their driving while waiting for first eye cataract surgery? Clin. Interv. Aging 2017, 12, 1911–1920. [Google Scholar] [CrossRef] [Green Version]
- Fraser, M.; Meuleners, L.; Ng, J.; Morlet, N. Driver self-regulation and depressive symptoms in cataract patients awaiting surgery: A cross-sectional study. BMC Ophthalmol. 2013, 13, 45. [Google Scholar] [CrossRef] [Green Version]
- Ortiz-Peregrina, S.; Ortiz, C.; Salas, C.; Casares-López, M.; Soler, M.; Anera, R.G. Intraocular scattering as a predictor of driving performance in older adults with cataracts. PLoS ONE 2020, 15, e0227892. [Google Scholar] [CrossRef]
- Vassallo, S.; Smart, D.; Sanson, A.; Cockfield, S.; Harris, A.; McIntyre, A.; Harrison, W. Risky driving among young Australian drivers II: Co-occurrence with other problem behaviours. Accid. Anal. Prev. 2008, 40, 376–386. [Google Scholar] [CrossRef]
- Richer, I.; Bergeron, J. Driving under the influence of cannabis: Links with dangerous driving, psychological predictors, and accident involvement. Accid. Anal. Prev. 2009, 41, 299–307. [Google Scholar] [CrossRef]
- Bergeron, J.; Paquette, M. Relationships between frequency of driving under the influence of cannabis, self-reported reckless driving and risk-taking behavior observed in a driving simulator. J. Saf. Res. 2014. [Google Scholar] [CrossRef]
- Lenné, M.G.; Dietze, P.M.; Triggs, T.J.; Walmsley, S.; Murphy, B.; Redman, J.R. The effects of cannabis and alcohol on simulated arterial driving: Influences of driving experience and task demand. Accid. Anal. Prev. 2010, 42, 859–866. [Google Scholar] [CrossRef]
- Ronen, A.; Chassidim, H.S.; Gershon, P.; Parmet, Y.; Rabinovich, A.; Bar-Hamburger, R.; Cassuto, Y.; Shinar, D. The effect of alcohol, THC and their combination on perceived effects, willingness to drive and performance of driving and non-driving tasks. Accid. Anal. Prev. 2010, 42, 1855–1865. [Google Scholar] [CrossRef]
- Babor, T.F.; Higgins-Biddle, J.C.; Saunders, J.B.; Monteiro, M.G. The Alcohol Use Disorders Identification Test Guidelines for Use in Primary Care; Department of Mental Health and Substance Dependence, World Health Organization: Geneva, Switzerland, 2001.
- Adamson, S.J.; Kay-Lambkin, F.J.; Baker, A.L.; Lewin, T.J.; Thornton, L.; Kelly, B.J.; Sellman, J.D. An improved brief measure of cannabis misuse: The Cannabis Use Disorders Identification Test-Revised (CUDIT-R). Drug Alcohol Depend. 2010, 110, 137–143. [Google Scholar] [CrossRef]
- Bron, A.M.; Viswanathan, A.C.; Thelen, U.; de Natale, R.; Ferreras, A.; Gundgaard, J.; Schwartz, G.; Buchholz, P. International vision requirements for driver licensing and disability pensions: Using a milestone approach in characterization of progressive eye disease. Clin. Ophthalmol. 2010, 4, 1361–1369. [Google Scholar] [CrossRef] [Green Version]
- Owsley, C.; Mcgwin, G. Vision and Driving. Vis. Res. 2010, 50, 2348–2361. [Google Scholar] [CrossRef] [Green Version]
- Wood, J.; Carberry, T.P. Bilateral cataract surgery and driving performance. Br. J. Ophthalmol. 2006, 90, 1277–1280. [Google Scholar] [CrossRef] [Green Version]
- Casares-López, M.; Castro-Torres, J.J.; Martino, F.; Ortiz-Peregrina, S.; Ortiz, C.; Anera, R.G. Contrast sensitivity and retinal straylight after alcohol consumption: Effects on driving performance. Sci. Rep. 2020, 10, 13599. [Google Scholar] [CrossRef]
- Ortiz, C.; Ortiz-Peregrina, S.; Castro, J.J.; Casares-López, M.; Salas, C. Driver distraction by smartphone use (WhatsApp) in different age groups. Accid. Anal. Prev. 2018, 117, 239–249. [Google Scholar] [CrossRef]
- Ortiz-Peregrina, S.; Oviedo-Trespalacios, O.; Ortiz, C.; Casares-López, M.; Salas, C.; Anera, R.G. Factors determining speed management during distracted driving (WhatsApp messaging). Sci. Rep. 2020, 10, 13263. [Google Scholar] [CrossRef]
- Ortiz-Peregrina, S.; Ortiz, C.; Casares-López, M.; Castro-Torres, J.J.; Jiménez Del Barco, L.; Anera, R.G. Impact of Age-Related Vision Changes on Driving. Int. J. Environ. Res. Public Health 2020, 17, 7416. [Google Scholar] [CrossRef]
- Sexton, B.F.; Tunbridge, R.J.; Brook-Carter, N.; Jackson, P.G.; Wright, K.; Stark, M.M.; Englehart, K. The Influence of Cannabis on Driving; Road Safety Division, Department of the Environment, Transport and the Regions: London, UK, 2000.
- Dula, C.S.; Ballard, M.E. Development and Evaluation of a Measure of Dangerous, Aggressive, Negative Emotional, and Risky Driving1. J. Appl. Soc. Psychol. 2003, 33, 263–282. [Google Scholar] [CrossRef]
- Willemsen, J.; Dula, C.S.; Declercq, F. The Dula Dangerous Driving Index: An Investigation of Reliability and Validity across Cultures. Accid. Anal. Prev. 2008, 40, 798–806. [Google Scholar] [CrossRef] [Green Version]
- Grotenhermen, F. Pharmacokinetics and Pharmacodynamics of Cannabinoids. Clin. Pharmacokinet. 2003, 42, 327–360. [Google Scholar] [CrossRef]
- Desrosiers, N.A.; Milman, G.; Mendu, D.R.; Lee, D.; Barnes, A.J.; Gorelick, D.A.; Huestis, M.A. Cannabinoids in oral fluid by on-site immunoassay and by GC-MS using two different oral fluid collection devices. Anal. Bioanal. Chem. 2014, 406, 4117–4128. [Google Scholar] [CrossRef]
- Scherer, J.N.; Schuch, J.B.; Rabelo-da-Ponte, F.D.; Silvestrin, R.; Ornell, R.; Sousa, T.; Limberger, R.P.; Pechansky, F. Analytical reliability of four oral fluid point-of-collection testing devices for drug detection in drivers. Forensic Sci. Int. 2020, 315, 110434. [Google Scholar] [CrossRef] [PubMed]
- Wood, J. Age and visual impairment decrease driving performance as measured on a closed-road circuit. Hum. Factors 2002, 44, 482–494. [Google Scholar] [CrossRef]
- Noyes, R.; Brunk, S.F.; Avery, D.H.; Canter, A. The analgesic properties of delta-9-tetrahydrocannabinol and codeine. Clin. Pharmacol. Ther. 1975, 18, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Adams, A.; Brown, B.; Flom, M.; Jones, R.; Jampolsky, A. Alcohol and marijuana effects on static visual acuity. Am. J. Optom. Physiol. Opt. 1975, 52, 729–735. [Google Scholar] [CrossRef]
- Brown, B.; Adams, A.; Haegerstrom-Portnoy, G.; Jones, R.; Flom, M. Effects of alcohol and marijuana on dynamic visual acuity: I. Threshold measurements. Percept. Psychophys. 1975, 18, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Wood, J.M.; Black, A.A. Ocular disease and driving. Clin. Exp. Optom. 2016, 99, 395–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emrich, H.M.; Weber, M.M.; Wendl, A.; Zihl, J.; Von Meyer, L.; Hanisch, W. Reduced binocular depth inversion as an indicator of cannabis-induced censorship impairment. Pharmacol. Biochem. Behav. 1991, 40, 689–690. [Google Scholar] [CrossRef]
- Semple, D.M.; Ramsden, F.; McIntosh, A.M. Reduced binocular depth inversion in regular cannabis users. Pharmacol. Biochem. Behav. 2003, 75, 789–793. [Google Scholar] [CrossRef]
- Yellott, J.I. Binocular depth inversion. Sci. Am. 1981, 245, 148–159. [Google Scholar] [CrossRef] [Green Version]
- Brands, B.; Mann, R.E.; Wickens, C.M.; Sproule, B.; Stoduto, G.; Sayer, G.S.; Burston, J.; Pan, J.F.; Matheson, J.; Stefan, C.; et al. Acute and residual effects of smoked cannabis: Impact on driving speed and lateral control, heart rate, and self-reported drug effects. Drug Alcohol Depend. 2019, 205, 107641. [Google Scholar] [CrossRef]
- Berning, A.; Compton, R.; Wochinger, K. Results of the 2013–2014 National Roadside Survey of Alcohol and Drug Use by Drivers; Department of Transportation, National Highway Traffic Safety Administration: Washington, DC, USA, 2015.
- Fergusson, D.M.; Horwood, L.J.; Boden, J.M. Is driving under the influence of cannabis becoming a greater risk to driver safety than drink driving? Findings from a longitudinal study. Accid. Anal. Prev. 2008, 40, 1345–1350. [Google Scholar] [CrossRef]
- Ortiz, C.; Castro, J.J.; Alarcón, A.; Soler, M.; Anera, R.G. Quantifying age-related differences in visual-discrimination capacity: Drivers with and without visual impairment. Appl. Ergon. 2013, 44, 523–531. [Google Scholar] [CrossRef]
- Anderson, B.M.; Rizzo, M.; Block, R.I.; Pearlson, G.D.; O’Leary, D.S. Sex differences in the effects of marijuana on simulated driving performance. J. Psychoact. Drugs 2010, 42, 19–30. [Google Scholar] [CrossRef]
- Zhang, Q.; Ge, Y.; Qu, W.; Zhang, K.; Sun, X. The traffic climate in China: The mediating effect of traffic safety climate between personality and dangerous driving behavior. Accid. Anal. Prev. 2018, 113, 213–223. [Google Scholar] [CrossRef]
- Calakos, K.C.; Bhatt, S.; Foster, D.W.; Cosgrove, K.P. Mechanisms Underlying Sex Differences in Cannabis Use. Curr. Addict. Rep. 2017, 4, 439–453. [Google Scholar] [CrossRef]
- Rhodes, N.; Pivik, K. Age and gender differences in risky driving: The roles of positive affect and risk perception. Accid. Anal. Prev. 2011, 43, 923–931. [Google Scholar] [CrossRef]
- Factor, R. An empirical analysis of the characteristics of drivers who are ticketed for traffic offences. Transp. Res. Part F Traffic Psychol. Behav. 2018, 53, 1–13. [Google Scholar] [CrossRef]
- Bédard, M.; Dubois, S.; Weaver, B. The impact of cannabis on driving. Can. J. Public Health 2007, 98, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Chai, J.; Qu, W.; Sun, X.; Zhang, K.; Ge, Y. Negativity Bias in Dangerous Drivers. PLoS ONE 2016, 11, e0147083. [Google Scholar] [CrossRef] [Green Version]
- Bédard, M.; Parkkari, M.; Weaver, B.; Riendeau, J.; Dahlquist, M. Assessment of driving performance using a simulator protocol: Validity and reproducibility. Am. J. Occup. Ther. 2010, 64, 336–340. [Google Scholar] [CrossRef] [Green Version]
- Meuleners, L.; Fraser, M. A validation study of driving errors using a driving simulator. Transp. Res. Part F Traffic Psychol. Behav. 2015, 29, 14–21. [Google Scholar] [CrossRef]
- Micallef, J.; Dupouey, J.; Jouve, E.; Truillet, R.; Lacarelle, B.; Taillard, J.; Daurat, A.; Authié, C.; Blin, O.; Rascol, O.; et al. Cannabis smoking impairs driving performance on the simulator and real driving: A randomized, double-blind, placebo-controlled, crossover trial. Fundam. Clin. Pharmacol. 2018, 32, 558–570. [Google Scholar] [CrossRef]
- Hunault, C.C.; Mensinga, T.T.; De Vries, I.; Kelholt-Dijkman, H.H.; Hoek, J.; Kruidenier, M.; Leenders, M.E.C.; Meulenbelt, J. Delta-9-tetrahydrocannabinol (THC) serum concentrations and pharmacological effects in males after smoking a combination of tobacco and cannabis containing up to 69 mg THC. Psychopharmacology 2008, 201, 171–181. [Google Scholar] [CrossRef]
- Brown, S.; Vanlaar, W.G.M.; Robertson, R.D. Marijuana Use among Drivers in Canada, 2000–2016; Traffic Injury Research Foundation: Ottawa, ON, Canada, 2019. [Google Scholar]
- Robertson, R.D.; Mainegra Hing, M.; Pashley, C.R.; Brown, S.W.; Vanlaar, W.G.M. Prevalence and trends of drugged driving in Canada. Accid. Anal. Prev. 2017, 99, 236–241. [Google Scholar] [CrossRef]
- Lloyd, S.L.; Lopez-Quintero, C.; Striley, C.W. Sex differences in driving under the influence of cannabis: The role of medical and recreational cannabis use. Addict. Behav. 2020, 110, 106525. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Speed Limit (km/h) | Length (km) | Other Traffic and Road Users | Road Configuration/Layout | |
|---|---|---|---|---|
| Dual carriageway | 120 | 4.5 | Moderate Same direction | Two lanes in each direction Straight and gentle curves |
| Mountain road | 40/90 | 6 | Moderate Oncoming and same direction | One single lane carriageway Straight, slight bends, sharp bends, ascending and descending slopes |
| Baseline Condition (Mean (SD)/Median (IQR)) | THC Condition Mean (SD)/Median (IQR)) | t/Z | p-Value | ||
|---|---|---|---|---|---|
| Dual Carriageway | Max acceleration force * | 0.72 (0.62–1.00) | 0.89 (0.71–1.00) | −2.179 | 0.029 |
| Max braking force * | 0.17 (0–0.41) | 0.02 (0–0.75) | −0.974 | 0.330 | |
| Max speed (km/h) * | 130.52 (126.10–138.36) | 130.69 (127.26–138.40) | −0.597 | 0.550 | |
| Speed adaptation (km/h) | −4.13 (6.60) | −1.73 (10.98) | −1.235 | 0.232 | |
| Mountain Road | Max acceleration force * | 0.96 (0.80–1.00) | 1.00 (1.00–1.00) | −2.314 | 0.021 |
| Max braking force * | 1.00 (1.00–1.00) | 1.00 (1.00–1.00) | −1.000 | 0.317 | |
| Max speed (km/h) | 105.58 (8.15) | 103.20 (6.62) | 1.123 | 0.275 | |
| Speed adaptation (km/h) | −17.20 (2.15) | −15.91 (1.95) | −2.142 | 0.045 | |
| Total circuit | Speeding Index | −0.18 (0.40) | 0.11 (0.43) | −2.831 | 0.011 |
| Dula Dangerous Driving Index (DDDI) | 1 = Never | 2 | 3 | 4 | 5 = Always | Mean (SD) | |
|---|---|---|---|---|---|---|---|
| NCE1 | I drive when I am angry or upset. | 30% | 15% | 20% | 15% | 20% | 2.80 (1.54) |
| NCE2 | I lose my temper when driving. | 60% | 35% | 5% | 0% | 0% | 1.45 (0.61) |
| NCE3 | I consider the actions of other drivers to be inappropriate or “stupid”. | 5% | 15% | 70% | 10% | 0% | 2.85 (0.67) |
| AD4 | I flash my headlights when I am annoyed by another driver. | 85% | 10% | 0% | 5% | 0% | 1.25 (0.72) |
| AD5 | I make rude gestures (e.g., giving “the finger”; yelling curse words) toward drivers who annoy me. | 75% | 25% | 0% | 0% | 0% | 1.25 (0.44) |
| AD6 | I verbally insult drivers who annoy me. | 45% | 30% | 15% | 5% | 5% | 1.95 (1.15) |
| AD7 | I deliberately use my car/truck to block drivers who tailgate me. | 80% | 15% | 5% | 0% | 0% | 1.25 (0.55) |
| AD8 | I would tailgate a driver who annoys me. | 95% | 0% | 5% | 0% | 0% | 1.10 (0.45) |
| RD9 | I “drag race” other drivers at stop lights to get out in front. | 95% | 5% | 0% | 0% | 0% | 1.05 (0.22) |
| RD10 | I will illegally pass a car/truck that is going too slowly. | 30% | 45% | 25% | 0% | 0% | 1.95 (0.76) |
| AD11 | I feel it is my right to strike back in some way, if I feel another driver has been aggressive toward me. | 30% | 50% | 15% | 5% | 0% | 1.95 (0.83) |
| NCE12 | When I get stuck in a traffic jam, I get very irritated. | 45% | 35% | 10% | 10% | 0% | 1.85 (0.99) |
| RD13 | I will race a slow-moving train to a railroad crossing. | 95% | 0% | 5% | 0% | 0% | 1.10 (0.45) |
| RD14 | I will weave in and out of slower traffic. | 25% | 40% | 20% | 10% | 5% | 2.30 (1.13) |
| RD15 | I will drive if I am only mildly intoxicated or buzzed. | 45% | 35% | 20% | 0% | 0% | 1.75 (0.79) |
| AD16 | When someone cuts me off, I feel I should punish him/her. | 90% | 0% | 10% | 0% | 0% | 1.20 (0.62) |
| NCE17 | I get impatient and/or upset when I fall behind schedule when I am driving. | 10% | 45% | 35% | 5% | 5% | 2.50 (0.95) |
| NCE18 | Passengers in my car/truck tell me to calm down. | 80% | 20% | 0% | 0% | 0% | 1.20 (0.41) |
| NCE19 | I get irritated when a car/truck in front of me slows down for no reason. | 15% | 45% | 25% | 10% | 5% | 2.45 (1.10) |
| RD20 | I will cross double yellow lines to see if I can pass a slow-moving car/truck. | 50% | 40% | 10% | 0% | 0% | 1.60 (0.68) |
| RD21 | I feel it is my right to get where I need to go as quickly as possible. | 65% | 25% | 10% | 0% | 0% | 1.45 (0.69) |
| NCE22 | I feel that passive drivers should learn how to drive or stay home. | 45% | 40% | 5% | 5% | 5% | 1.85 (1.01) |
| RD23 | I will drive on the shoulder or median strip to get around a traffic jam. | 100% | 0% | 0% | 0% | 0% | 1.00 (0.00) |
| RD24 | When passing a car/truck on a 2-lane road, I will barely miss on-coming cars. | 70% | 20% | 10% | 0% | 0% | 1.40 (0.68) |
| RD25 | I will drive when I am drunk. | 70% | 25% | 0% | 5% | 0% | 1.40 (0.75) |
| NCE26 | I feel that I may lose my temper if I have to confront another driver. | 45% | 40% | 10% | 5% | 0% | 1.75 (0.85) |
| RD27 | I consider myself to be a risk-taker. | 40% | 25% | 25% | 5% | 5% | 2.10 (1.17) |
| RD28 | I feel that most traffic “laws” could be considered suggestions. | 50% | 45% | 5% | 0% | 0% | 1.55 (0.61) |
| TOTAL SCORE | 47.70 (10.04) | ||||||
| NCE SCORE (Negative Cognitive/Emotional Driving) | 14.30 (3.92) | ||||||
| AD SCORE (Aggressive Driving) | 9.95 (3.10) | ||||||
| RD SCORE (Risky Driving) | 19.05 (3.53) | ||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Age | - | ||||||||||||||
| 2 | Gender | −0.113 | - | |||||||||||||
| 3 | Cannabis use (monthly) | −0.214 | −0.509 * | - | ||||||||||||
| 4 | Years driving | 0.909 ** | −0.020 | −0.242 | - | |||||||||||
| 5 | Driving frequency (monthly) | −0.188 | 0.138 | 0.029 | −0.219 | - | ||||||||||
| 6 | Frequencyof DUIC | 0.052 | −0.213 | 0.559 * | 0.060 | 0.481 * | ||||||||||
| 7 | AUDIT | −0.177 | −0.071 | 0.332 | −0.038 | −0.459 * | −0.250 | - | ||||||||
| 8 | CUDIT-R | 0.054 | −0.447 * | 0.735 ** | 0.001 | −0.233 | 0.295 | 0.549 * | - | |||||||
| 9 | Accidents (past year) | 0.099 | −0.243 | 0.101 | 0.122 | −0.219 | −0.142 | 0.135 | 0.012 | - | ||||||
| 10 | DDDI score | −0.074 | −0.241 | 0.591 ** | −0.063 | −0.199 | −0.024 | 0.553 * | 0.674 ** | 0.377 | - | |||||
| 11 | NCDE score | −0.131 | −0.344 | 0.591 ** | −0.154 | −0.313 | −0.044 | 0.369 | 0.524 * | 0.356 | 0.644 ** | - | ||||
| 12 | AD score | −0.006 | −0.031 | 0.278 | 0.107 | 0.024 | −0.046 | 0.248 | 0.289 | 0.469 * | 0.611 ** | 0.293 | - | |||
| 13 | RD score | −0.127 | −0.131 | 0.371 | −0.009 | −0.255 | −0.097 | 0.670 ** | 0.476 * | 0.392 | 0.852 ** | 0.415 | 0.540 * | - | ||
| 14 | Overall Visual Change Index | −0.077 | −0.349 | 0.310 | −0.081 | 0.085 | −0.059 | 0.015 | 0.094 | −0.313 | −0.032 | 0.023 | 0.050 | −0.164 | - | |
| 15 | Speeding Index | 0.176 | −0.502 * | 0.649 ** | 0.129 | −0.148 | 0.138 | 0.171 | 0.366 | 0.026 | 0.112 | 0.141 | −0.012 | 0.039 | 0.133 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortiz-Peregrina, S.; Ortiz, C.; Anera, R.G. Aggressive Driving Behaviours in Cannabis Users. The Influence of Consumer Characteristics. Int. J. Environ. Res. Public Health 2021, 18, 3911. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083911
Ortiz-Peregrina S, Ortiz C, Anera RG. Aggressive Driving Behaviours in Cannabis Users. The Influence of Consumer Characteristics. International Journal of Environmental Research and Public Health. 2021; 18(8):3911. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083911
Chicago/Turabian StyleOrtiz-Peregrina, Sonia, Carolina Ortiz, and Rosario G. Anera. 2021. "Aggressive Driving Behaviours in Cannabis Users. The Influence of Consumer Characteristics" International Journal of Environmental Research and Public Health 18, no. 8: 3911. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083911