
Interventions Preventing Vaginitis, Vaginal Atrophy after Brachytherapy or Radiotherapy Due to Malignant Tumors of the Female Reproductive Organs—A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
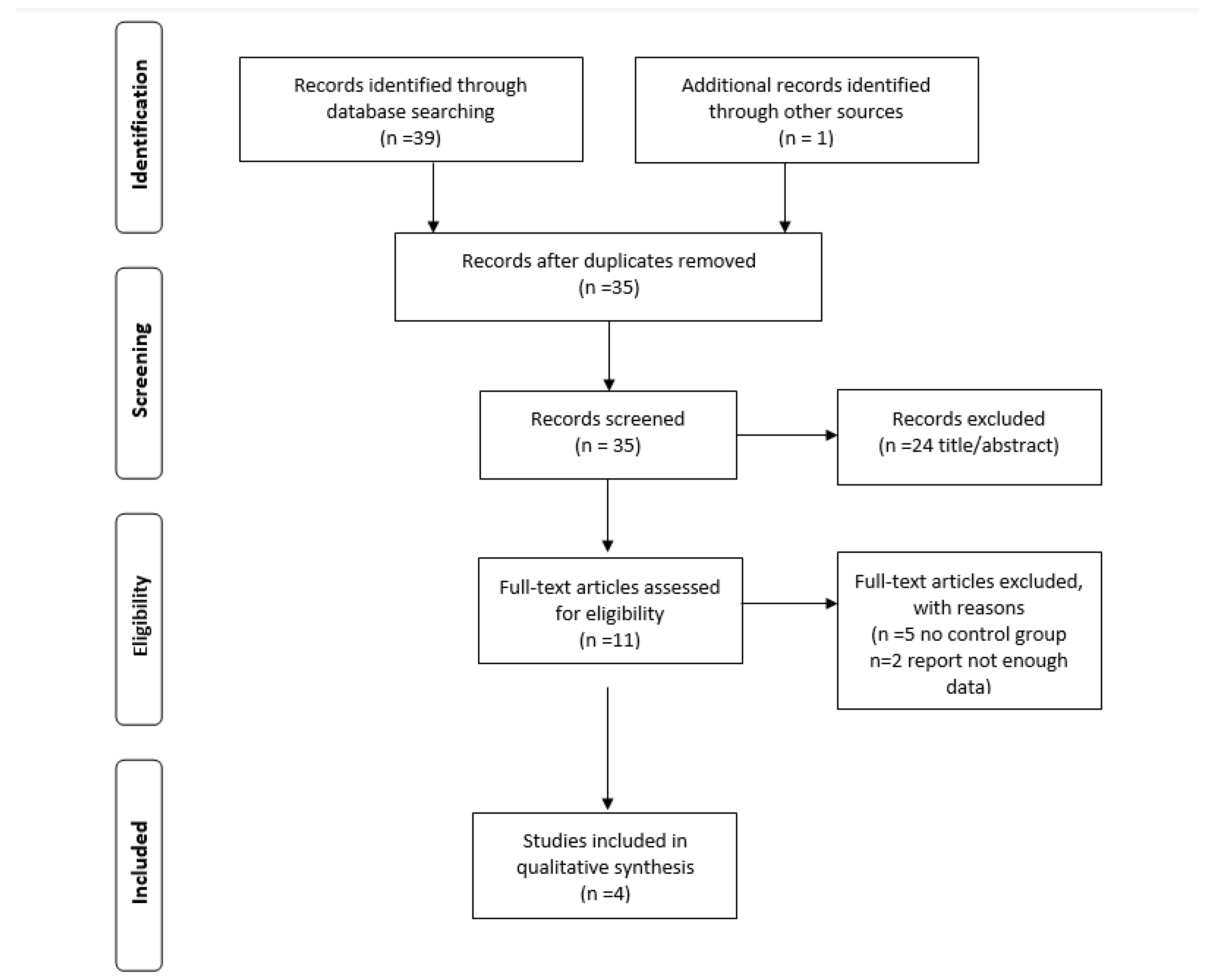
2.1. Search Strategy and Study Selection
2.2. Data Extraction
2.3. Outcomes and Measures
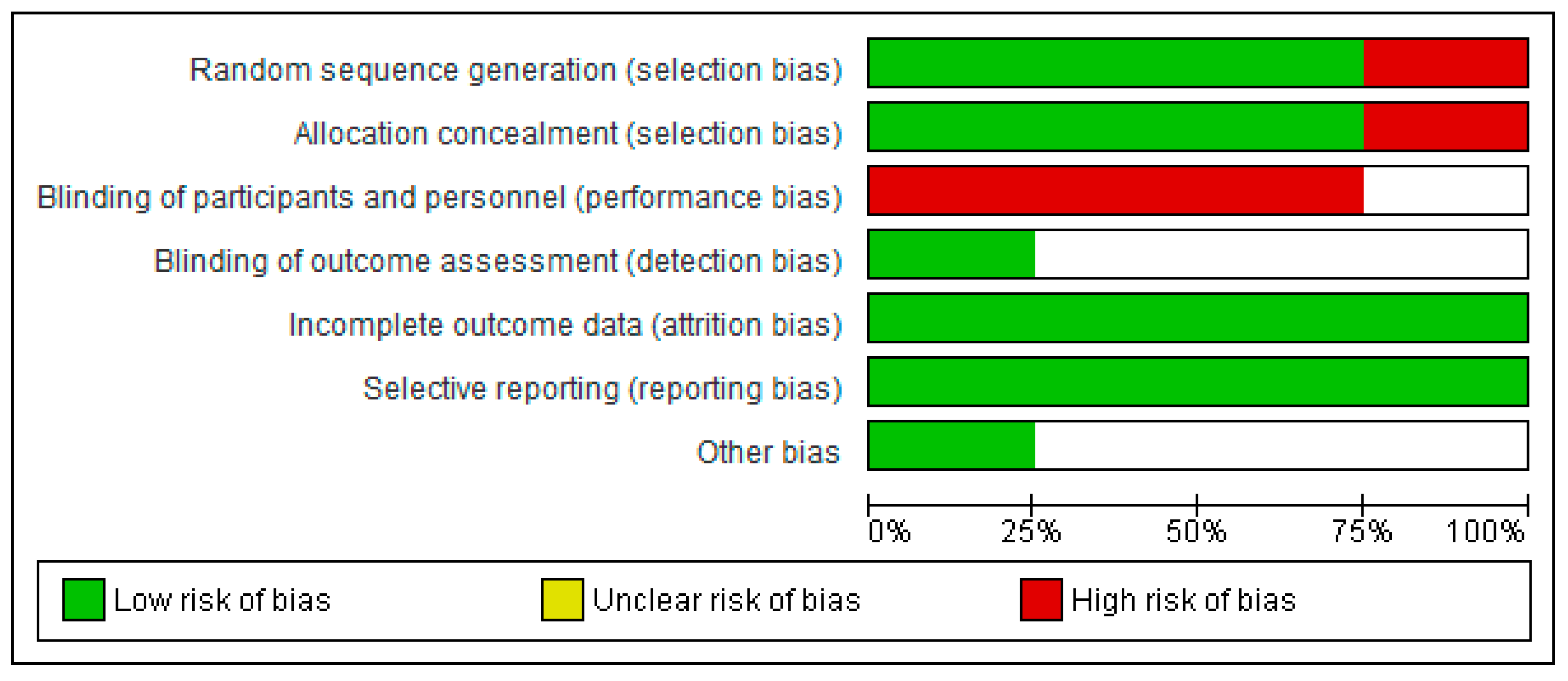
2.4. Risk of Bias Tool
2.5. Statistical Analysis
3. Results
3.1. Study Selection and Characteristics of the Study Population
3.2. Effect of Topical Interventions on Vaginal Changes and Clinical Outcomes
4. Discussion
4.1. Characteristics of the Study
4.2. Biological Properties of Vaginal Suppositories
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Naumova, I.; Castelo-Branco, C. Current Treatment Options for Postmenopausal Vaginal Atrophy. Int. J. Womens Health 2018, 10, 387–395. [Google Scholar] [CrossRef] [Green Version]
- Vaginitis: Diagnosis and Treatment-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/29671516/ (accessed on 10 February 2021).
- Definition of Vaginal Atrophy-NCI Dictionary of Cancer Terms-National Cancer Institute. Available online: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/vaginal-atrophy (accessed on 10 February 2021).
- Wilmoth, M.C.; Spinelli, A. Sexual Implications of Gynecologic Cancer Treatments. J. Obstet. Gynecol. Neonatal. Nurs. 2000, 29, 413–421. [Google Scholar] [CrossRef]
- Sathyanarana Rao, T.; Nagaraj, A.K. Female Sexuality. Indian J. Psychiatry 2015, 57, 296. [Google Scholar] [CrossRef]
- Ganz, P.A. Quality of Life in Long-Term, Disease-Free Survivors of Breast Cancer: A Follow-up Study. Cancer Spectrum Knowl. Environ. 2002, 94, 39–49. [Google Scholar] [CrossRef]
- Chargari, C.; Deutsch, E.; Blanchard, P.; Gouy, S.; Martelli, H.; Guérin, F.; Dumas, I.; Bossi, A.; Morice, P.; Viswanathan, A.N.; et al. Brachytherapy: An Overview for Clinicians. CA Cancer J. Clin. 2019, 69, 386–401. [Google Scholar] [CrossRef] [Green Version]
- Shankar, A.; Prasad, N.; Roy, S.; Chakraborty, A.; Sharma Biswas, A.; Patil, J.; Rath, G.K. Sexual Dysfunction in Females after Cancer Treatment: An Unresolved Issue. Asian Pac. J. Cancer Prev. 2017, 18, 1177–1182. [Google Scholar] [CrossRef]
- Andrews, S.; von Gruenigen, V.E. Management of the Late Effects of Treatments for Gynecological Cancer. Curr. Opin. Oncol. 2013, 25, 566–570. [Google Scholar] [CrossRef]
- Edwards, D.; Panay, N. Treating Vulvovaginal Atrophy/Genitourinary Syndrome of Menopause: How Important Is Vaginal Lubricant and Moisturizer Composition? Climacteric 2016, 19, 151–161. [Google Scholar] [CrossRef] [Green Version]
- Tayyeb, M.; Gupta, V. Dyspareunia. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Information for Mucosal Inflammation. Available online: http://sideeffects.embl.de/se/C0333355/pt (accessed on 25 March 2021).
- Vaginal Dryness: Causes, Symptoms, and More. Available online: https://www.healthline.com/health/vaginal-dryness (accessed on 25 March 2021).
- Vaginal Bleeding-Mayo Clinic. Available online: https://www.mayoclinic.org/symptoms/vaginal-bleeding/basics/definition/sym-20050756 (accessed on 25 March 2021).
- VAGINAL-FIBROSIS. Available online: http://www.ugr.es/~oncoterm/csdata/VAGINAL-FIBROSIS.html (accessed on 25 March 2021).
- Shuster, J.J. Review: Cochrane Handbook for Systematic Reviews for Interventions. Res. Synth. Methods 2011, 2, 126–130. [Google Scholar] [CrossRef]
- Delia, P.; Sansotta, G.; Pontoriero, A.; Iati, G.; De Salvo, S.; Pisana, M.; Potami, A.; Lopes, S.; Messina, G.; Pergolizzi, S. Clinical Evaluation of Low-Molecular-Weight Hyaluronic Acid-Based Treatment on Onset of Acute Side Effects in Women Receiving Adjuvant Radiotherapy after Cervical Surgery: A Randomized Clinical Trial. Oncol. Res. Treat. 2019, 42, 217–223. [Google Scholar] [CrossRef]
- Galuppi, A.; Perrone, A.M.; La Macchia, M.; Santini, D.; Medoro, S.; Maccarini, L.R.; Strada, I.; Pozzati, F.; Rossi, M.; De Iaco, P. Local α-Tocopherol for Acute and Short-Term Vaginal Toxicity Prevention in Patients Treated with Radiotherapy for Gynecologic Tumors. Int. J. Gynecol. Cancer 2011, 21, 1708–1711. [Google Scholar] [CrossRef]
- Pitkin, R.M.; VanVoorhis, L.W. Postirradiation Vaginitis: An Evaluation of Prophylaxis with Topical Estrogen. Radiology 1971, 99, 417–421. [Google Scholar] [CrossRef] [Green Version]
- Hyaluronic Acid and Vitamins Are Effective in Reducing Vaginal Atrophy in Women Receiving Radiotherapy-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/26788875/ (accessed on 12 January 2021).
- Douple, E.B.; Richmond, R.C. A Review of Platinum Complex Biochemistry Suggests a Rationale for Combined Platinum-Radiotherapy. Int. J. Radiat. Oncol. 1979, 5, 1335–1339. [Google Scholar] [CrossRef]
- Vaginal Stenosis Following Irradiation Therapy for Carcinoma of the Cervix Uteri-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/5051667/ (accessed on 25 January 2021).
- Emamverdikhan, A.; Golmakani, N.; Tabassi, S.; Hassanzadeh, M.; Sharifi, N.; Shakeri, M. A Survey of the Therapeutic Effects of Vitamin E Suppositories on Vaginal Atrophy in Postmenopausal Women. Iran. J. Nurs. Midwifery Res. 2016, 21, 475. [Google Scholar] [CrossRef]
- Dos Santos, C.C.M.; Uggioni, M.L.R.; Colonetti, T.; Colonetti, L.; Grande, A.J.; Da Rosa, M.I. Hyaluronic Acid in Postmenopause Vaginal Atrophy: A Systematic Review. J. Sex. Med. 2021, 18, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Mazloomdoost, D.; Westermann, L.B.; Mutema, G.; Crisp, C.C.; Kleeman, S.D.; Pauls, R.N. Histologic Anatomy of the Anterior Vagina and Urethra. Female Pelvic Med. Reconstr. Surg. 2017, 23, 329–335. [Google Scholar] [CrossRef]
- Wilkinson, E.M.; Łaniewski, P.; Herbst-Kralovetz, M.M.; Brotman, R.M. Personal and Clinical Vaginal Lubricants: Impact on Local Vaginal Microenvironment and Implications for Epithelial Cell Host Response and Barrier Function. J. Infect. Dis. 2019, 220, 2009–2018. [Google Scholar] [CrossRef]
- Iżycki, D.; Woźniak, K.; Iżycka, N. Consequences of Gynecological Cancer in Patients and Their Partners from the Sexual and Psychological Perspective. Menopausal Rev. 2016, 2, 112–116. [Google Scholar] [CrossRef] [Green Version]
- Hofsjö, A.; Bohm-Starke, N.; Blomgren, B.; Jahren, H.; Steineck, G.; Bergmark, K. Radiotherapy-Induced Vaginal Fibrosis in Cervical Cancer Survivors. Acta Oncol. 2017, 56, 661–666. [Google Scholar] [CrossRef] [Green Version]
- Stinesen Kollberg, K.; Waldenström, A.-C.; Bergmark, K.; Dunberger, G.; Rossander, A.; Wilderäng, U.; Åvall-Lundqvist, E.; Steineck, G. Reduced Vaginal Elasticity, Reduced Lubrication, and Deep and Superficial Dyspareunia in Irradiated Gynecological Cancer Survivors. Acta Oncol. 2015, 54, 772–779. [Google Scholar] [CrossRef]
- Effectiveness and Safety of Vaginal Suppositories for the Treatment of the Vaginal Atrophy in Postmenopausal Women: An Open, Non-Controlled Clinical Trial-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/19146203/ (accessed on 24 January 2021).
- McLaren, H.C. Vitamin E in the Menopause. BMJ 1949, 2, 1378–1382. [Google Scholar] [CrossRef]
- Karanth, S.; Yu, W.H.; Mastronardi, C.A.; McCann, S.M. Vitamin E Stimulates Luteinizing Hormone-Releasing Hormone and Ascorbic Acid Release from Medial Basal Hypothalami of Adult Male Rats. Exp. Biol. Med. 2003, 228, 779–785. [Google Scholar] [CrossRef]
- Pessina, M.A.; Hoyt, R.F.; Goldstein, I.; Traish, A.M. Differential Effects of Estradiol, Progesterone, and Testosterone on Vaginal Structural Integrity. Endocrinology 2006, 147, 61–69. [Google Scholar] [CrossRef]
- Keshavarzi, Z.; Janghorban, R.; Alipour, S.; Tahmasebi, S.; Jokar, A. The Effect of Vitamin D and E Vaginal Suppositories on Tamoxifen-Induced Vaginal Atrophy in Women with Breast Cancer. Support. Care Cancer 2019, 27, 1325–1334. [Google Scholar] [CrossRef]
- Morali, G.; Polatti, F.; Metelitsa, E.; Mascarucci, P.; Magnani, P.; Brunenghi Marrè, G. Open, Non-Controlled Clinical Studies to Assess the Efficacy and Safety of a Medical Device in Form of Gel Topically and Intravaginally Used in Postmenopausal Women with Genital Atrophy. Arzneimittelforschung 2011, 56, 230–238. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.-B.; Liu, S.-L.; Gan, X.-L.; Zhou, Q.; Hu, L.-N. The Effects of Hyaluronic Acid Vaginal Gel on the Vaginal Epithelium of Ovariectomized Rats. Gynecol. Endocrinol. 2015, 31, 208–213. [Google Scholar] [CrossRef]
- Dimmeler, S.; Zeiher, A.M. Akt Takes Center Stage in Angiogenesis Signaling. Circ. Res. 2000, 86, 4–5. [Google Scholar] [CrossRef] [Green Version]
- Peattie, R.A.; Nayate, A.P.; Firpo, M.A.; Shelby, J.; Fisher, R.J.; Prestwich, G.D. Stimulation of in Vivo Angiogenesis by Cytokine-Loaded Hyaluronic Acid Hydrogel Implants. Biomaterials 2004, 25, 2789–2798. [Google Scholar] [CrossRef]
- Yosipovitch, G. Dry Skin and Impairment of Barrier Function Associated with Itch—New Insights. Int. J. Cosmet. Sci. 2004, 26, 1–7. [Google Scholar] [CrossRef]
- Role of High Molecular Weight Hyaluronic Acid in Postmenopausal Vaginal Discomfort-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/22728576/ (accessed on 25 January 2021).
- Efficacy and Safety of Hyaluronic Acid (Cikatridina)(R)) in the Treatment of Hormone or Chemotherapy Induced Vaginal Atrophy in Patients with Breast Cancer. Available online: https://www.researchgate.net/publication/298279312_Efficacy_and_safety_of_hyaluronic_acid_CikatridinaR_in_the_treatment_of_hormone_or_chemotherapy_induced_vaginal_atrophy_in_patients_with_breast_cancer (accessed on 9 February 2021).
- Rahn, D.D.; Carberry, C.; Sanses, T.V.; Mamik, M.M.; Ward, R.M.; Meriwether, K.V.; Olivera, C.K.; Abed, H.; Balk, E.M.; Murphy, M. Vaginal Estrogen for Genitourinary Syndrome of Menopause: A Systematic Review. Obstet. Gynecol. 2014, 124, 1147–1156. [Google Scholar] [CrossRef] [Green Version]
- Weber, M.A.; Kleijn, M.H.; Langendam, M.; Limpens, J.; Heineman, M.J.; Roovers, J.P. Local Oestrogen for Pelvic Floor Disorders: A Systematic Review. PLoS ONE 2015, 10, e0136265. [Google Scholar] [CrossRef] [Green Version]
- Tanmahasamut, P.; Jirasawas, T.; Laiwejpithaya, S.; Areeswate, C.; Dangrat, C.; Silprasit, K. Effect of Estradiol Vaginal Gel on Vaginal Atrophy in Postmenopausal Women: A Randomized Double-blind Controlled Trial. J. Obstet. Gynaecol. Res. 2020, 46, 1425–1435. [Google Scholar] [CrossRef]
- Donders, G.; Neven, P.; Moegele, M.; Lintermans, A.; Bellen, G.; Prasauskas, V.; Grob, P.; Ortmann, O.; Buchholz, S. Ultra-Low-Dose Estriol and Lactobacillus Acidophilus Vaginal Tablets (Gynoflor®) for Vaginal Atrophy in Postmenopausal Breast Cancer Patients on Aromatase Inhibitors: Pharmacokinetic, Safety, and Efficacy Phase I Clinical Study. Breast Cancer Res. Treat. 2014, 145, 371–379. [Google Scholar] [CrossRef] [Green Version]
- Wills, S.; Ravipati, A.; Venuturumilli, P.; Kresge, C.; Folkerd, E.; Dowsett, M.; Hayes, D.F.; Decker, D.A. Effects of Vaginal Estrogens on Serum Estradiol Levels in Postmenopausal Breast Cancer Survivors and Women at Risk of Breast Cancer Taking an Aromatase Inhibitor or a Selective Estrogen Receptor Modulator. J. Oncol. Pract. 2012, 8, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-S.; Kim, S.-O.; Ahn, K.; Park, K. All-Trans Retinoic Acid Increases Aquaporin 3 Expression in Human Vaginal Epithelial Cells. Sex. Med. 2016, 4, e249–e254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCullough, F.S.W.; Northrop-Clewes, C.A.; Thurnham, D.I. The Effect of Vitamin A on Epithelial Integrity. Proc. Nutr. Soc. 1999, 58, 289–293. [Google Scholar] [CrossRef] [Green Version]
- Polcz, M.E.; Barbul, A. The Role of Vitamin A in Wound Healing. Nutr. Clin. Pract. 2019, 34, 695–700. [Google Scholar] [CrossRef]
- Kim, S.; Oh, K.J.; Lee, H.S.; Ahn, K.; Kim, S.W.; Park, K. Expression of Aquaporin Water Channels in the Vagina in Premenopausal Women. J. Sex. Med. 2011, 8, 1925–1930. [Google Scholar] [CrossRef]
- Tammi, R.; Ripellino, J.A.; Margolis, R.U.; Maibach, H.I.; Tammi, M. Hyaluronate Accumulation in Human Epidermis Treated with Retinoic Acid in Skin Organ Culture. J. Investig. Dermatol. 1989, 92, 326–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burton, G.W.; Joyce, A.; Ingold, K.U. Is Vitamin E the Only Lipid-Soluble, Chain-Breaking Antioxidant in Human Blood Plasma and Erythrocyte Membranes? Arch. Biochem. Biophys. 1983, 221, 281–290. [Google Scholar] [CrossRef]
- Kaileh, M.; Sen, R. Role of NF-ΚB in the Anti-Inflammatory Effects of Tocotrienols. J. Am. Coll. Nutr. 2010, 29, 334S–339S. [Google Scholar] [CrossRef]
- Suzuki, Y.J.; Tsuchiya, M.; Wassall, S.R.; Choo, Y.M.; Govil, G.; Kagan, V.E.; Packer, L. Structural and Dynamic Membrane Properties of .Alpha.-Tocopherol and .Alpha.-Tocotrienol: Implication to the Molecular Mechanism of Their Antioxidant Potency. Biochemistry 1993, 32, 10692–10699. [Google Scholar] [CrossRef]
- Lewis, E.D.; Meydani, S.N.; Wu, D. Regulatory Role of Vitamin E in the Immune System and Inflammation: Regulatory Role of Vitamin E. IUBMB Life 2019, 71, 487–494. [Google Scholar] [CrossRef]
- Fraser, J.R.E.; Laurent, T.C.; Laurent, U.B.G. Hyaluronan: Its Nature, Distribution, Functions and Turnover. J. Intern. Med. 1997, 242, 27–33. [Google Scholar] [CrossRef]
- Ashcroft, G.S.; Dodsworth, J.; Boxtel, E.V.; Tarnuzzer, R.W.; Horan, M.A.; Schultz, G.S.; Ferguson, M.W.J. Estrogen Accelerates Cutaneous Wound Healing Associated with an Increase in TGF-Β1 Levels. Nat. Med. 1997, 3, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Grosman, N.; Hvidberg, E.; Schou, J. The Effect of Oestrogenic Treatment on the Acid Mucopolysaccharide Pattern in Skin of Mice. Acta Pharmacol. Toxicol. 2009, 30, 458–464. [Google Scholar] [CrossRef]
- Skin Disorders during Menopause-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/26919507/ (accessed on 11 February 2021).
- Athanasiou, S.; Pitsouni, E.; Grigoriadis, T.; Michailidis, G.; Tsiveleka, A.; Rodolakis, A.; Loutradis, D. A Study Protocol of Vaginal Laser Therapy in Gynecological Cancer Survivors. Climacteric 2020, 23, 53–58. [Google Scholar] [CrossRef]
- Perrone, A.M.; Tesei, M.; Ferioli, M.; De Terlizzi, F.; Della Gatta, A.N.; Boussedra, S.; Dondi, G.; Galuppi, A.; Morganti, A.G.; De Iaco, P. Results of a Phase I-II Study on Laser Therapy for Vaginal Side Effects after Radiotherapy for Cancer of Uterine Cervix or Endometrium. Cancers 2020, 12, 1639. [Google Scholar] [CrossRef]
- Law, E.; Kelvin, J.F.; Thom, B.; Riedel, E.; Tom, A.; Carter, J.; Alektiar, K.M.; Goodman, K.A. Prospective Study of Vaginal Dilator Use Adherence and Efficacy Following Radiotherapy. Radiother. Oncol. 2015, 116, 149–155. [Google Scholar] [CrossRef] [Green Version]
- Cerentini, T.M.; Schlöttgen, J.; Viana da Rosa, P.; La Rosa, V.L.; Vitale, S.G.; Giampaolino, P.; Valenti, G.; Cianci, S.; Macagnan, F.E. Clinical and Psychological Outcomes of the Use of Vaginal Dilators after Gynaecological Brachytherapy: A Randomized Clinical Trial. Adv. Ther. 2019, 36, 1936–1949. [Google Scholar] [CrossRef] [Green Version]
- Hanlon, A.; Small, W.; Strauss, J.; Lin, L.L.; Hanisch, L.; Huang, L.; Bai, J.; Wells, J.; Bruner, D.W. Dilator Use After Vaginal Brachytherapy for Endometrial Cancer: A Randomized Feasibility and Adherence Study. Cancer Nurs. 2018, 41, 200–209. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Source, Year | Country | Trial Type | Sample Size (n) | Age (Years) Mean ± SD | Type of Cancer | Staging * | |||
|---|---|---|---|---|---|---|---|---|---|
| Control Group | Intervention Group | Control Group | Intervention Group | Control Group | Intervention Group | ||||
| Delia et al. 2018 [17] | Italy | RCT | 89 | 88 | 50.3 ± 10.3 | 49.7 ± 9.2 | Cervical cancer | CC IB–IIA | CC IB–IIA |
| Dinicola et al. 2015 [20] | Italy | PRS | 23 | 22 | 38 ± 6 | 38 ± 6 | Cervical cancer | CC IIB–IIIB | CC IIB–IIIB |
| Galuppi et al. 2011 [18] | Italy | RCT | 29 | 33 | 66 ± 13.6 | 67 ± 12.3 | Endometrial cancerCervical cancer | EC IC 11 | EC IC 9 |
| EC IIB 3 | EC IIB 4 | ||||||||
| EC III 1 | EC III 1 | ||||||||
| CC IB 18 | CC IB 15 | ||||||||
| Pitkin et al. 1971 [19] | USA | RCT | 49 | 43 | 49.87 ± 13.73 | 50.04 ± 13.66 | Cervical cancer | CC I 9 | CC I 10 |
| CC II 14 | CC II 12 | ||||||||
| CC III 26 | CC III 21 | ||||||||
| CC IV 1 | |||||||||
| Study Included | Intervention Time (weeks) | Intervention Dose (mg) | Used Intervention | Method of Evaluation | Key Results |
|---|---|---|---|---|---|
| Delia et al. 2018 [17] | 5 | 5 | HA | gynecological inspection, Adverse Event Reporting Questions, VAS | ↓ vaginal dryness ↓ dyspareunia ↓ mucosal inflammation |
| 1 | Vitamin E | ||||
| 1 | Vitamin A | ||||
| Dinicola et al. 2015 [20] | 16 | 5 | HA | biopsy of the vaginal vault, VAS, anamnestic interview, medical examination | ↓ dyspareunia ↓ mucosal inflammation ↓ bleeding ↓ fibrosis ↓ cellular atypia |
| 1 | Vitamin E | ||||
| 1 | Vitamin A | ||||
| Galuppi et al. 2011 [18] | 14–17 | 500 | alpha-tocopherol acetate | punch biopsy, RTOGSS, VAS, microscopical assessment using histological criteria | ↓ mucosal inflammation ↑ vaginal acanthosis |
| Pitkin et al. 1971 [19] | 20–40 | 7.8 | dienestrol | gynecological inspection, historical information | ↓ dyspareunia ↓ vaginal caliber ↓ bleeding |
| Source, Year | Dyspareunia | p-Value | Dryness | p-Value | Inflammation | p-Value | |||
|---|---|---|---|---|---|---|---|---|---|
| Intervention after | Control after | Intervention after | Control after | Intervention after | Control after | ||||
| Delia et al. 2018 [17] | 2.46 ± 0.50 | 0.74 ± 0.43 | p < 0.001 | 0.63 ± 0.33 | 2.43 ± 0.50 | p < 0.001 | 0.77 ± 0.25 | 2.47 ± 0.50 | p < 0.001 |
| Dinicola et al. 2015 [20] | 23% | 69% | p < 0.05 | n/a | n/a | n/a | 23% | 75% | p < 0.05 |
| Galuppi et al. 2011 [18] | 1.33 ± 1.55 | 2.07 ± 1.77 | p = 0.09 | 1.17 ± 0.80 | 0.62 ± 0.62 | p > 0.05 | 1.64 ± 0.65 | 2.21 ± 0.80 * | p < 0.05 |
| Pitkin et al. 1971 [19] | 23.1% | 44.4% | p < 0.05 | n/a | n/a | n/a | n/a | n/a | n/a |
| Source, Year | Bleeding | p-Value | Fibrosis | p-Value | ||
|---|---|---|---|---|---|---|
| Intervention after | Control after | Intervention after | Control after | |||
| Delia et al. 2018 [17] | n/a | n/a | n/a | n/a | n/a | n/a |
| Dinicola et al. 2015 [20] | 9% | 43% | p < 0.05 | 18% | 56% | p < 0.05 |
| Galuppi et al. 2011 [18] | n/a | n/a | n/a | 2.00 ± 1.15 | 2.50 ± 0.52 | p > 0.05 |
| Pitkin et al. 1971 [19] | 79.6% | 27% | p > 0.05 | n/a | n/a | n/a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wierzbicka, A.; Mańkowska-Wierzbicka, D.; Cieślewicz, S.; Stelmach-Mardas, M.; Mardas, M. Interventions Preventing Vaginitis, Vaginal Atrophy after Brachytherapy or Radiotherapy Due to Malignant Tumors of the Female Reproductive Organs—A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 3932. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083932
Wierzbicka A, Mańkowska-Wierzbicka D, Cieślewicz S, Stelmach-Mardas M, Mardas M. Interventions Preventing Vaginitis, Vaginal Atrophy after Brachytherapy or Radiotherapy Due to Malignant Tumors of the Female Reproductive Organs—A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(8):3932. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083932
Chicago/Turabian StyleWierzbicka, Adrianna, Dorota Mańkowska-Wierzbicka, Stanisław Cieślewicz, Marta Stelmach-Mardas, and Marcin Mardas. 2021. "Interventions Preventing Vaginitis, Vaginal Atrophy after Brachytherapy or Radiotherapy Due to Malignant Tumors of the Female Reproductive Organs—A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 8: 3932. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083932