
LEAP Motion Technology and Psychology: A Mini-Review on Hand Movements Sensing for Neurodevelopmental and Neurocognitive Disorders


 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Methods
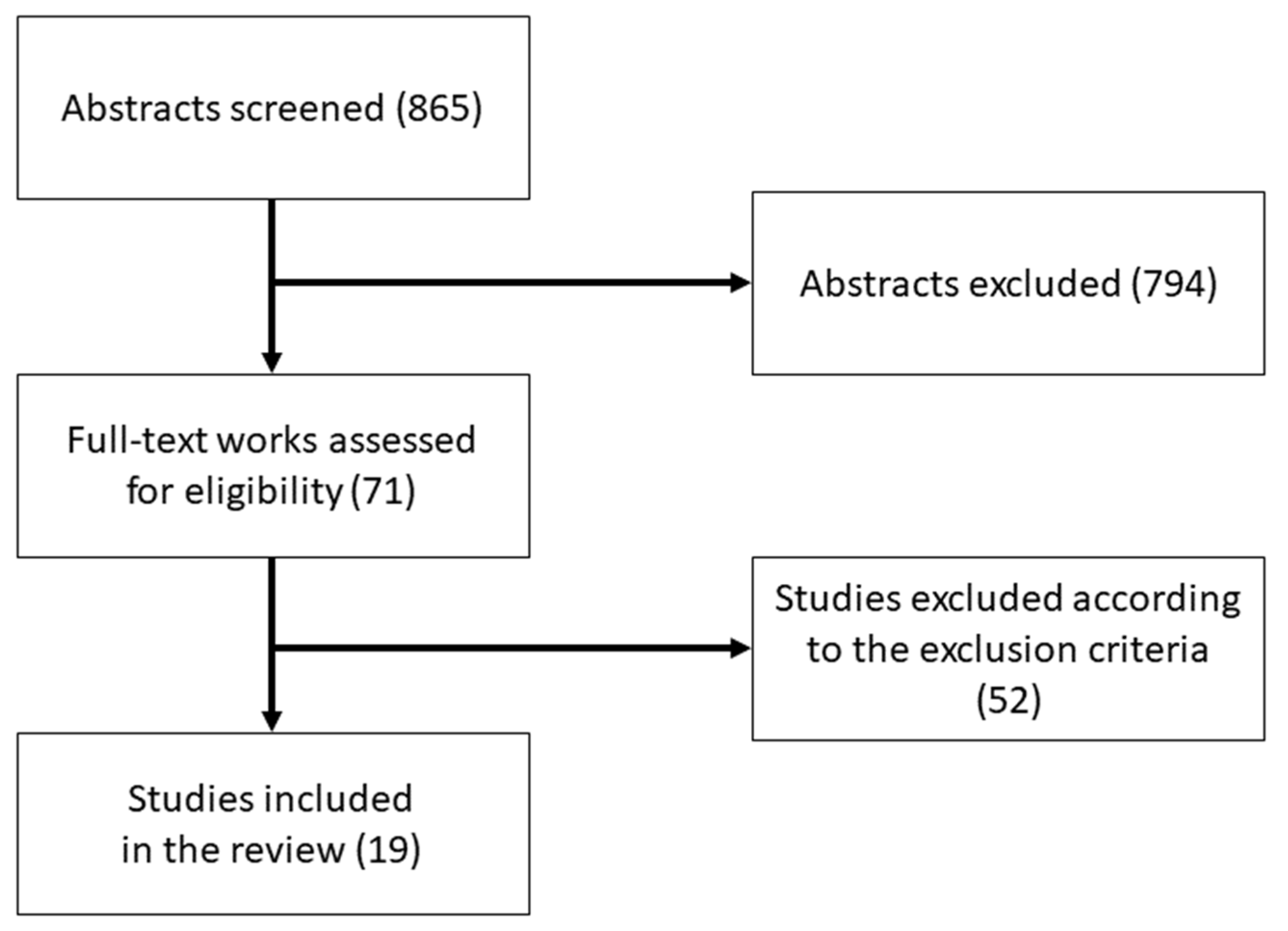
Search and Selection Strategy
3. Results
3.1. Characteristics of the Studies
3.2. Study Results
3.3. Risk of Bias
4. Discussion
4.1. Distribution of Studies on LEAP Motion Applications in the Various Domains
4.2. Objectives of LEAP-Motion-Based Interventions
4.3. Protocols of LEAP-Motion-Based Interventions
4.4. Protocols in Neurocognitive Disorders: Dementia and MCI
4.5. Background for LEAP-Motion-Based Interventions
4.6. Technology Weaknesses and Future Challenges
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Ref. | Sample Size | Groups | Gender Distribution | Age Range and Mean Age (SD) | Sample Characteristics | Task Information (and Duration if Available) |
|---|---|---|---|---|---|---|
| [14] | 3 | 1 experimental group | NR | NR | Children with diagnosis of autism | Labyrinth game: item manipulation task |
| [15] | 12 |
2 groups Control group: 6 participants organized in 3 TD/TD couples Experimental group: 6 participants organized in 3 ASD/TD couples | 83% male |
Range = NR Control group: Mage = 9.99 (0.87) Experimental group: Mage ASD = 11.70 (2.24); Mage TD = 11.09 (1.19) | Children with ASD and typically developing children | Collaborative games: puzzle, collection, delivery games (5 min playtime in pre-test; less than 5 min in post-test) |
| [16] | 24 |
2 groups Control group: 6 ASD/TD couples Experimental group: 6 ASD/TD couples | NR |
Control group: Range = NR Mage ASD = 12.38 (2.60); Mage TD = 12.60 (2.66); Experimental group: Mage ASD = 12.12 (3.59); Mage TD = 13.15 (3.77) | Children with ASD and typically developing children | Collaborative games: puzzle, collection, delivery games |
| [23] | 60 |
2 groups Control group: 37 cognitively intact participants; Experimental group: 23 cognitively impaired participants |
Control group: 70.3% female; Experimental group: 65.2% female |
Range = 65–85; Group 1: Mage = 70.7 (3.6); Group 2: Mage = 73.2 (5.4) | Elderly with and without cognitive impairment from a public primary care clinic in Singapore |
Activities of daily living: opening door with correct key and passcode number; making a phone call recalling a number; identifying items from different categories in a newspaper; sorting things in a room; picking appropriate outfit for occasion; withdrawing cash from automated teller machine; shopping at provision shop (Average time to complete the task of 19.1 min (3.6) in control group; average time of 20.4 (3.4) time in experimental group) |
| [34] | 20 |
2 groups Control group: 10 healthy children Experimental group: 10 children with ADHD |
Group 1: 60% male; Group 2: 60% male |
Range = 7–12; Mage = NR | Children with and without ADHD |
Matching game: color-matching association of geometric figures and boxes (Three attempts in a week, average time of 16.56 min in experimental group; average time of 13.54 min in control group) |
| [35] | 3 | (Multiple probe design across participants) | 100% male |
Range = 6–7 Mage = NR | First-grade students diagnosed with ASD (1 in mild and 2 in moderate range) from an elementary school in Beijing |
Match-to-sample task (20 pre-experimental training trials per session every day, 10–15 min each session. Five seconds to provide response in the intervention phase) |
| [36] | 4 |
1 experimental group (Adapted alternating treatment design. Two conditions—CAI and TII—were alternated with each student each day) | 75% male |
Range = 9–11; Mage = NR | Fourth-grade students with different diagnosis (2 severe autism and mild intellectual disability, 1 Down’s syndrome and mild intellectual disability, 1 moderate intellectual disability) from a Chinese special education school |
Match-to-sample task (20 pre-experimental training trials for each condition, 10–15 min each session. Five seconds to provide response in the intervention phase) |
| [37] | 3 | (Single subject research design) | 66.66% male |
Range = 9–11; Mage = NR | Students with severe autism from a special needs school in Beijing |
Matching game: color-matching balls to boxes and fruits to sticks (Three-week experiment, half an hour a day for five days a week) |
| [38] | 2 | Single subject research design | 50% male |
Range = 9–10; Mage = NR | Third-grade students with severe autism from a special school in Beijing |
Matching game: color-matching balls to boxes and fruits to sticks (30 min every day) |
| [39] |
Study 1: 5 (+ parents) Study 2: 5 (+ teachers) | 1 experimental group for each of the two studies | 100% male | Range = NR; Study 1: Mage = 4.8 (1.8); Study 2: Range = NR; Mage = 6.3 (2.4) |
Study 1: Children with diagnosis of autism and their family members; Study 2: Children with diagnosis of autism; They all came from a Chinese Children’s Educational Development Center |
Drawing game (playtime of 15 min); Word-image pairing in zoo and home interactive game |
| [40] |
Study 1: 5 (+ parents) Study 2: 5 (+ teachers) Study 3: 9 | 1 experimental group for each of the two studies |
Study 1, 2 = 100% male Study 3: 55.5% male | Range = NR; Study 1: Mage = 4.8 (1.8); Study 2: Range = NR; Mage = 6.3 (2.4); Study 3: Mage = 8.1 (3.4) |
Study 1: Children with diagnosis of autism and their family members; Study 2: Children with diagnosis of autism; Study 3: Children with diagnosis of autism (1 also with ADHD, 5 with highly functioning ASD, 4 with low functioning ASD) |
Drawing game (15 min of play); Word-image pairing in zoo and home interactive game; Drum playing game |
| [41] | 2 | 2 groups Experimental group 1: 1 Experimental group 2: 1 | NR | NR | Participants with similar characteristics as children with autism (1 with better motor skills but focus issues; 1 with motor impairment) |
Matching games; Sign recognition task; Eye gazing task (Three sessions of training for each game) |
| [42] | NR | 1 experimental group | NR |
Range = 9–12; Mage = NR | Typically developing children |
Avatar greeting task (Two sessions, 20 min per session) |
| [43] | 10 | 1 experimental group (Virtual-based and performance-based assessment were done on each participant in parallel) | NR | NR | Healthy adults without diagnosis of cognitive impairment | Lunch box packing task |
| [44] | 16 | 1 experimental group | 68.7% male | Range = 65–72 Mage = 68 (2.76) | Elderly without experience in playing video games from a University Hospital in Tokyo (NR diagnosis) | Table preparation task |
| [45] | NR | NR | NR | NR | NR | Shopping task |
| [46] | 223 |
Control group: 71 Experimental group 1: 65 Experimental group 2: 42 Experimental group 3: 45 | 56% female |
Range = NR; Mage = 72.73 (6.89) | Elderly people from two Alzheimer day clinics in Greece (71 healthy elderly, 65 elderly with amnestic single-domain MCI, 42 elderly with amnestic multi-domain MCI, 45 elderly with mild Alzheimer’s dementia) |
Finger-tapping test in in a fire evacuation task (As fast as user could for 15 s) |
| [47] | 205 |
Control group: 72 Experimental group 1: 65 Experimental group 2: 68 | 57% female |
Range = NR Mage = 72.73 (6.89) | Elderly people from two Alzheimer day clinics in Greece (72 healthy elderly, 65 elderly with amnestic MCI, 68 elderly with mild Alzheimer’s disease) |
Finger-tapping test in a fire evacuation task (As fast as user could for 15 s) |
| [48] | 19 | 1 experimental group | 66.7% male |
Range = NR Mage = 10.88 (3.14) | Children (NR diagnosis) | Mathematical operations |
| Reference | Main Findings | Study Limitations | Risk of Biases |
|---|---|---|---|
| [14] | The application was deemed able to train children’s focus with a high percentage of agreement among expert therapists. |
Limited generalizability due to small sample size; shortcomings of participants’ demographic information. | Sampling bias due to lack of sampling criteria explication; bias due to unspecified blinding. |
| [15] | Participants with ASD were more satisfied with performance and showed relatively deep interest in the game. Mean playtime decreased, mean collaborative operations efficiency increased. Control group had a higher collaborative efficiency, both groups had a similar increase trend in level of communication. |
Limited generalizability due to small sample size; the majority of sample were male. | Sampling bias due to lack of sampling criteria explication; bias due to tool technical issues. |
| [16] | Cooperation performance and communication improved in the experimental group. Participants with ASD spoke more words per minute. Offline spontaneous communication was encouraged. | Limited generalizability due to small sample size. | Sampling bias due to lack of sampling criteria explication. |
| [23] | Total performance scores had a moderate positive correlation with three validated cognitive screening tools (Abbreviated Mental Test, Mini-Mental State Examination, and MoCA). A moderately significant relationship was found between total performance scores and presence of cognitive impairment. |
Limited
generalizability due to small sample size; significant difference in the education level between the groups;
limited representativeness of the population at risk of cognitive impairment due to the sample recruitment carried out only at one location with multiple exclusion criteria and classification based only on MoCA scores. |
Sampling bias due to the classification of the study population relying solely on MoCA scores, which is not considered diagnostic of cognitive impairment; Measurement bias due to using an assessment module that was originally used for rehabilitation and then adapted for cognitive screening. |
| [34] | Children’s relaxation, motivation, and concentration improved. Average time of less than 20 min was equivalent to 10.67% improvement in both groups. | Limited generalizability due to small sample size. | Sampling bias due to lack of sampling criteria explication; bias due to unspecified blinding. |
| [35] | A functional relationship was found between the gesture-based instruction via Leap-Motion-aided VR technology and the response accuracy and task engagement of students with ASD. Maintenance of the acquired skills was found at a high level up to 12 weeks. | Limited generalizability due to small sample, segregate setting of intervention (individual training room), and lack of female participants. | Sampling bias due to recruitment of a male-only sample. |
| [36] |
CAI and TII were both effective in teaching visual matching skills, but CAI was more effective for the two students with ASD. CAI was more efficient than TII, since it required a lower number of prompts and a shorter instructional time. CAI promoted more task engagement than TII. Generalization to similar untaught skills and maintenance were found at a high level for up to 5 weeks under both CAI and TII. |
Limited generalizability due to small sample size; the vast majority of sample was male; exclusion of younger students due to sensibility issues of small hand-gestures recognition. | Bias due to exclusion of younger students for technical issues. |
| [37] |
Participant’s recognition and fine motor skills improved considerably, reaching performance accuracy of 100%. Skills such as looking at the hands and objects and moving the gaze with them were increased by the game. Transfer of learned rules and skills was found. | Limited generalizability due to small sample size and use of a single subject research AB design; participants’ improvement may be a mixed result of various factors (i.e., better emotional control that affected concentration; better understanding of the rules of the games; better skills of operating Leap Motion controller; improvement due to rote learning); participants’ different level of experience in using technology devices. | Bias due to use of single subject research design. |
| [38] | Fine motors skills and cognition of colors and fruits were improved, reaching accuracy of 100%. | Limited generalizability due to small sample size. | Bias due to use of single subject research design. |
| [39] | High levels of engagement, sustained attention, and independent manipulation were found in children. High satisfaction was found in families. | Limited generalizability due to small sample size and lack of female participants. | Sampling bias due to recruitment of a male-only sample and lack of sampling criteria explication; bias due to no blinding of participants and nonprobability sampling techniques. |
| [40] | High levels of engagement and sustained attention were found in children. High satisfaction was found in families. Children’s independence and natural manipulation increased. | Limited generalizability due to small sample size. | Sampling bias due to lack of sampling criteria explication; bias due to no blinding of participants and nonprobability sampling techniques. |
| [41] | Participants’ accuracy increased and time needed to complete the task decreased. The eye gazing game confused the children because of item distances issues. | Limited generalizability due to small sample size and lack of inclusion of sample with target diagnosis; shortcomings of participants’ demographic information. | Sampling bias due to lack of sampling criteria explication and lack of inclusion of sample with target diagnosis; bias due to unspecified blinding. |
| [42] | High level of satisfaction was found. Learning curve stabilized around an average response time of 20–30 s for the first training session. Immersive Virtual Reality interface showed efficacy in improving communication performance. |
Limited generalizability due to lack of clinical sample;
shortcomings of participants’ demographic information. | Sampling bias due to lack of clinical sample. |
| [43] | Clusters formed by using acceleration data seemed reasonably analogous to performance measures (i.e., type and number of occurred errors). | Limited generalizability due to small sample size and including non-clinical sample; shortcomings of participants’ demographic information. | Sampling bias due to lack of clinical sample; bias due to unspecified blinding. |
| [44] |
Participants’ satisfaction was shown for LEAP Motion. Natural movements were represented well by LEAP Motion. The tool exhibited promising results for virtual rehabilitation. |
Limited generalizability due to small sample size; the majority of sample were male. | Sampling bias due to lack of sampling criteria explication; bias due to lack of sample diagnosis specification. |
| [45] | LEAP Motion lost accuracy and was influenced by light. | NA | NA |
| [46] | LEAP-Motion-aided VR technology measures of functional abilities showed consistent functional impairment in mild Alzheimer’s disease, amnestic single and multiple domain MCI in comparison with healthy subjects. Total performance scores showed significant discrimination power. | Limited generalizability due to exclusion of elderly with technophobia. | Sampling bias due to exclusion of technophobic participants; statistical bias due to the use of statistical models with a limited number of covariates. |
| [47] | LEAP-Motion-aided VR technology measures of functional abilities was strongly correlated with standard cognitive and functional measurements as Mini-Mental State Examination and Bristol Activities of Daily Living scale scores. Total virtual measures of functional abilities showed consistent functional impairment in mild Alzheimer’s disease and amnestic MCI in comparison with healthy participants. Assessment module showed moderately good psychometric properties in discriminating healthy from pre-dementia and mild dementia patients. | Limited generalizability due to exclusion of elderly with technophobia. | Sampling bias due to exclusion of technophobic participants; statistical bias due to use of statistical models with limited number of covariates. |
| [48] | Users’ learning caused by the system and the interface obtained a considerably high punctuation. Meaningful correlations were found between interface and learning outcomes and information and learning outcomes. The hand–eye coordination exercise helped improve attention. | Limited generalizability due to small sample size and unspecified diagnosis of participants | Sampling bias due to lack of sampling criteria explication; bias due to lack of sample diagnosis specification; bias due to unspecified blinding. |
References
- Carpenter-Song, E. Promoting Meaningful Recovery with Digital Mental Health Care. Epidemiol. Psychiatr. Sci. 2020, 29. [Google Scholar] [CrossRef] [Green Version]
- Lustgarten, S.D.; Elhai, J.D. Technology Use in Mental Health Practice and Research: Legal and Ethical Risks. Clin. Psychol. Sci. Pract. 2018, 25, e12234. [Google Scholar] [CrossRef]
- Weichert, F.; Bachmann, D.; Rudak, B.; Fisseler, D. Analysis of the Accuracy and Robustness of the Leap Motion Controller. Sensors 2013, 13, 6380–6393. [Google Scholar] [CrossRef] [Green Version]
- Wozniak, P.; Vauderwange, O.; Mandal, A.; Javahiraly, N.; Curticapean, D. Possible Applications of the LEAP Motion Controller for More Interactive Simulated Experiments in Augmented or Virtual Reality. In Proceedings of the Optics Education and Outreach IV, San Diego, CA, USA, 27 September 2016; International Society for Optics and Photonics: Bellingham, WA, USA, 2016; Volume 9946. [Google Scholar]
- Kurschl, W.; Augstein, M.; Burger, T.; Pointner, C. User Modeling for People with Special Needs. Int. J. Pervasive Comput. Commun. 2014, 10, 313–336. [Google Scholar] [CrossRef]
- Braun, M.; Wölfel, M.; Renner, G.; Menschik, C. Accessibility of Different Natural User Interfaces for People with Intellectual Disabilities. In Proceedings of the 2020 International Conference on Cyberworlds (CW), Caen, France, 19 September–1 October 2020; pp. 211–218. [Google Scholar]
- Sharma, S.; Varkey, B.; Achary, K.; Hakulinen, J.; Turunen, M.; Heimonen, T.; Srivastava, S.; Rajput, N. Designing Gesture-Based Applications for Individuals with Developmental Disabilities: Guidelines from User Studies in India. ACM Trans. Access. Comput. 2018, 11, 1–27. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.-J.; Chen, S.-F.; Huang, J.-D. A Kinect-Based System for Physical Rehabilitation: A Pilot Study for Young Adults with Motor Disabilities. Res. Dev. Disabil. 2011, 32, 2566–2570. [Google Scholar] [CrossRef]
- Webster, D.; Celik, O. Systematic Review of Kinect Applications in Elderly Care and Stroke Rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 108. [Google Scholar] [CrossRef] [Green Version]
- Boutsika, E. Kinect in Education: A Proposal for Children with Autism. Procedia Comput. Sci. 2014, 27, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Retalis, S.; Korpa, T.; Skaloumpakas, C.; Boloudakis, M.; Kourakli, M.; Altanis, I.; Siameri, F.; Papadopoulou, P.; Lytra, F.; Pervanidou, P. Empowering Children With ADHD Learning Disabilities With the Kinems Kinect Learning Games. In Proceedings of the European Conference on Games Based Learning, Berlin, Germany, 9–10 October 2014; Volume 2, p. 469. [Google Scholar]
- Perhakaran, G.; Yusof, A.M.; Rusli, M.E.; Yusoff, M.Z.M.; Mahidin, E.M.M.; Mahalil, I.; Zainuddin, A.R.R. SnoezelenCAVE: Virtual Reality CAVE Snoezelen Framework for Autism Spectrum Disorders. In Advances in Visual Informatics; Badioze Zaman, H., Robinson, P., Smeaton, A.F., Shih, T.K., Velastin, S., Jaafar, A., Mohamad Ali, N., Eds.; Springer International Publishing: Cham, Switzerland, 2015; pp. 443–453. [Google Scholar]
- Schroeder, P.A.; Lohmann, J.; Butz, M.V.; Plewnia, C. Behavioral Bias for Food Reflected in Hand Movements: A Preliminary Study with Healthy Subjects. Cyberpsychol. Behav. Soc. Netw. 2015, 19, 120–126. [Google Scholar] [CrossRef]
- Syahputra, M.F.; Sari, P.P.; Arisandi, D.; Abdullah, D.; Napitupulu, D.; Setiawan, M.I.; Albra, W.; Asnawi; Andayani, U. Implementation of Augmented Reality to Train Focus on Children with s Pecial Needs. J. Phys. Conf. Ser. 2018, 978, 012109. [Google Scholar] [CrossRef]
- Zhao, H.; Swanson, A.; Weitlauf, A.; Warren, Z.; Sarkar, N. A Novel Collaborative Virtual Reality Game for Children with ASD to Foster Social Interaction. In Universal Access in Human-Computer Interaction. Users and Context Diversity; Antona, M., Stephanidis, C., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 276–288. [Google Scholar]
- Zhao, H.; Swanson, A.R.; Weitlauf, A.S.; Warren, Z.E.; Sarkar, N. Hand-in-Hand: A Communication-Enhancement Collaborative Virtual Reality System for Promoting Social Interaction in Children With Autism Spectrum Disorders. IEEE Trans. Hum. Mach. Syst. 2018, 48, 136–148. [Google Scholar] [CrossRef] [PubMed]
- Ebner, M.; Spot, N. Game-Based Learning with the Leap Motion Controller. Handb. Res. Gaming Trends P-12 Educ. 2015, 555–565. [Google Scholar] [CrossRef] [Green Version]
- Kuntz, N.; Adams, J.A.; Zahr, L.; Killen, R.; Cameron, K.; Wasson, H. Therapeutic Play and Bone Marrow Transplantation. J. Pediatr. Nurs. 1996, 11, 359–367. [Google Scholar] [CrossRef]
- O’Connell, S.R. Recreation Therapy: Reducing the Effects of Isolation for the Patient in a Protected Environment. Child. Health Care 1984, 12, 118–121. [Google Scholar] [CrossRef]
- Dumoulin, S.; Bouchard, S.; Ellis, J.; Lavoie, K.L.; Vézina, M.-P.; Charbonneau, P.; Tardif, J.; Hajjar, A. A Randomized Controlled Trial on the Use of Virtual Reality for Needle-Related Procedures in Children and Adolescents in the Emergency Department. Games Health J. 2019, 8, 285–293. [Google Scholar] [CrossRef]
- Indovina, P.; Barone, D.; Gallo, L.; Chirico, A.; De Pietro, G.; Giordano, A. Virtual Reality as a Distraction Intervention to Relieve Pain and Distress During Medical Procedures. Clin. J. Pain 2018, 34, 858–877. [Google Scholar] [CrossRef] [PubMed]
- Piskorz, J.; Czub, M. Effectiveness of a Virtual Reality Intervention to Minimize Pediatric Stress and Pain Intensity during Venipuncture. J. Spec. Pediatr. Nurs. 2018, 23, e12201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chua, S.I.L.; Tan, N.C.; Wong, W.T.; Allen, J.C., Jr.; Quah, J.H.M.; Malhotra, R.; Østbye, T. Virtual Reality for Screening of Cognitive Function in Older Persons: Comparative Study. J. Med. Internet Res. 2019, 21, e14821. [Google Scholar] [CrossRef] [PubMed]
- Harrison, K.E. Sharing a (Cyber)Space: Fostering Relationship Maintenance in Residential Care through Virtual Reality; UC Santa Barbara: California, CA, USA, 2019. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: Dsm-5, 5th ed.; Amer Psychiatric Pub Inc.: Washington, DC, USA, 2013; ISBN 978-0-89042-555-8. [Google Scholar]
- Sachdev, P.S.; Blacker, D.; Blazer, D.G.; Ganguli, M.; Jeste, D.V.; Paulsen, J.S.; Petersen, R.C. Classifying Neurocognitive Disorders: The DSM-5 Approach. Nat. Rev. Neurol. 2014, 10, 634–642. [Google Scholar] [CrossRef]
- de Sousa, L.R.N.; Silveira, I.F. A Framework for the Creation of Leap Motion Gestural Interfaces for Handwriting Education to Children with Development Coordination Disorder. Int. J. Learn. Teach. Educ. Res. 2017, 16, 31–53. [Google Scholar]
- de Sousa, L.R.N.; Silveira, I.F. Developing Handwriting Skills in Children with Dyspraxia: A Gestural User Interface-Based Approach. In Proceedings of the XX International Conference on Human Computer Interaction, New York, NY, USA, 25 June 2019; Association for Computing Machinery: New York, NY, USA, 2019; pp. 1–6. [Google Scholar]
- Nunes, L.R.; Silveira, I.F. Ensino de Caligrafia para Dispráxicos utilizando Tecnologias Gestuais. An. Temporários LACLO 2015 2015, 10, 326. [Google Scholar]
- Oktay, A.B.; Kocer, A. Differential Diagnosis of Parkinson and Essential Tremor with Convolutional LSTM Networks. Biomed. Signal Process. Control 2020, 56, 101683. [Google Scholar] [CrossRef]
- Tarakci, E.; Arman, N.; Tarakci, D.; Kasapcopur, O. Leap Motion Controller–Based Training for Upper Extremity Rehabilitation in Children and Adolescents with Physical Disabilities: A Randomized Controlled Trial. J. Hand Ther. 2020, 33, 220–228. [Google Scholar] [CrossRef]
- Cohen, M.W.; Regazzoni, D. Hand Rehabilitation Assessment System Using Leap Motion Controller. AI Soc. 2020, 35, 581–594. [Google Scholar] [CrossRef]
- Association, A.P. Neurodevelopmental Disorders: DSM-5® Selections; American Psychiatric Pub: Washington, WA, USA, 2015; ISBN 978-1-61537-013-9. [Google Scholar]
- Capelo, D.C.; Sánchez, M.E.; Hurtado, J.S.; Chicaiza, D.B. Multisensory Virtual Game with Use of the Device Leap Motion to Improve the Lack of Attention in Children of 7–12 Years with ADHD. In Proceedings of the International Conference on Information Technology & Systems (ICITS 2018); Rocha, Á., Guarda, T., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 897–906. [Google Scholar]
- Hu, X.; Han, Z.R. Effects of Gesture-Based Match-to-Sample Instruction via Virtual Reality Technology for Chinese Students with Autism Spectrum Disorders. Int. J. Dev. Disabil. 2019, 65, 327–336. [Google Scholar] [CrossRef]
- Hu, X.; Lee, G.T.; Tsai, Y.-T.; Yang, Y.; Cai, S. Comparing Computer-Assisted and Teacher-Implemented Visual Matching Instruction for Children with ASD and/or Other DD. J. Autism Dev. Disord. 2020, 50, 2540–2555. [Google Scholar] [CrossRef]
- Cai, S.; Zhu, G.; Wu, Y.-T.; Liu, E.; Hu, X. A Case Study of Gesture-Based Games in Enhancing the Fine Motor Skills and Recognition of Children with Autism. Interact. Learn. Environ. 2018, 26, 1039–1052. [Google Scholar] [CrossRef]
- Zhu, G.; Cai, S.; Ma, Y.; Liu, E. A Series of Leap Motion-Based Matching Games for Enhancing the Fine Motor Skills of Children with Autism. In Proceedings of the 2015 IEEE 15th International Conference on Advanced Learning Technologies, Hualien, Taiwan, 6–9 July 2015; pp. 430–431. [Google Scholar]
- Tang, T.Y.; Falzarano, M.; Morreale, P.A. Engaging Chinese Children with Autism to Interact with Portable Hand- and Finger-Gesture Based Applications: Experiment and Reflections. In Learning and Collaboration Technologies; Zaphiris, P., Ioannou, A., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 562–572. [Google Scholar]
- Tang, T.Y.; Falzarano, M.; Morreale, P.A. Assessment of the Utility of Gesture-Based Applications for the Engagement of Chinese Children with Autism. Univers. Access Inf. Soc. 2018, 17, 275–290. [Google Scholar] [CrossRef]
- Rahmadiva, M.; Arifin, A.; Fatoni, M.H.; Baki, S.H.; Watanabe, T. A Design of Multipurpose Virtual Reality Game for Children with Autism Spectrum Disorder. In Proceedings of the 2019 International Biomedical Instrumentation and Technology Conference (IBITeC), Piscataway, NJ, USA, 23–24 October 2019; Volume 1, pp. 1–6. [Google Scholar]
- Halabi, O.; Elseoud, S.A.; Alja’am, J.M.; Alpona, H.; Al-Hemadi, M.; Al-Hassan, D. Immersive Virtual Reality in Improving Communication Skills in Children with Autism. Int. J. Interact. Mob. Technol. IJIM 2017, 11, 146–158. [Google Scholar] [CrossRef] [Green Version]
- Martono, N.P.; Yamaguchi, T.; Ohwada, H. Utilizing Finger Movement Data to Cluster Patients with Everyday Action Impairment. In Proceedings of the 2016 IEEE 15th International Conference on Cognitive Informatics Cognitive Computing (ICCI*CC), Palo Alto, CA, USA, 22–23 August 2016; pp. 459–464. [Google Scholar]
- Vallejo, V.; Tarnanas, I.; Yamaguchi, T.; Tsukagoshi, T.; Yasuda, R.; Müri, R.M.; Mosimann, U.P.; Nef, T. Usability Assessment of Natural User Interfaces during Serious Games: Adjustments for Dementia Intervention. J. Pain Manag. 2015, 9, 333–339. [Google Scholar]
- Sacco, M.; Redaelli, C.; Zangiacomi, A.; Greci, L.; Di Santo, S.; Leone, A.; Vezzoli, A. GOJI an Advanced Virtual Environment Supporting Training of Physical and Cognitive Activities to Prevent Dementia Occurrence in Elderly with Minor Cognitive Disorders. In Ambient Assisted Living: Italian Forum 2014; Andò, B., Siciliano, P., Marletta, V., Monteriù, A., Eds.; Biosystems & Biorobotics; Springer International Publishing: Cham, Switzerland, 2015; pp. 429–437. ISBN 978-3-319-18374-9. [Google Scholar]
- Tarnanas, I.; Mouzakidis, C.; Schlee, W. Functional Impairment in Virtual-Reality-Daily-Living-Activities as a Defining Feature of Amnestic MCI: Cognitive and Psychomotor Correlates. In Proceedings of the 2013 International Conference on Virtual Rehabilitation (ICVR), Piscataway, NJ, USA, 26–29 August 2013; pp. 27–34. [Google Scholar]
- Tarnanas, I.; Schlee, W.; Tsolaki, M.; Müri, R.; Mosimann, U.; Nef, T. Ecological Validity of Virtual Reality Daily Living Activities Screening for Early Dementia: Longitudinal Study. JMIR Serious Games 2013, 1, e2778. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Zapirain, B.; de la Torre Díez, I.; López-Coronado, M. Dual System for Enhancing Cognitive Abilities of Children with ADHD Using Leap Motion and Eye-Tracking Technologies. J. Med. Syst. 2017, 41, 111. [Google Scholar] [CrossRef]
- Ganguli, M. Can the DSM-5 Framework Enhance the Diagnosis of MCI? Neurology 2013, 81, 2045–2050. [Google Scholar] [CrossRef] [Green Version]
- Maglione, M.A.; Gans, D.; Das, L.; Timbie, J.; Kasari, C.; The Technical Expert Panel; HRSA Autism Intervention Research—Behavioral (AIR-B) Network. Nonmedical Interventions for Children With ASD: Recommended Guidelines and Further Research Needs. Pediatrics 2012, 130, S169–S178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinkler, M.; Sochor, J. Integrating Motion Tracking Sensors to Human-Computer Interaction with Respect to Specific User Needs. In Proceedings of the The 18th Central European Seminar on Computer Graphics, Smolenice, Slovakia, 25–27 May 2014; Volume 26, p. 2014. [Google Scholar]
- Bartoli, L.; Corradi, C.; Garzotto, F.; Valoriani, M. Exploring Motion-Based Touchless Games for Autistic Children’s Learning. In Proceedings of the 12th International Conference on Interaction Design and Children, New York, NY, USA, 24 June 2013; Association for Computing Machinery: New York, NY, USA, 2013; pp. 102–111. [Google Scholar]
- Pennington, R.C. Computer-Assisted Instruction for Teaching Academic Skills to Students With Autism Spectrum Disorders: A Review of Literature. Focus Autism Dev. Disabil. 2010, 25, 239–248. [Google Scholar] [CrossRef]
- Salter, T.; Davey, N.; Michaud, F. Designing Developing QueBall, a Robotic Device for Autism Therapy. In Proceedings of the The 23rd IEEE International Symposium on Robot and Human Interactive Communication, Edinburgh, UK, 25–29 August 2014; pp. 574–579. [Google Scholar]
- Sansosti, F.J.; Doolan, M.L.; Remaklus, B.; Krupko, A.; Sansosti, J.M. Computer-Assisted Interventions for Students with Autism Spectrum Disorders within School-Based Contexts: A Quantitative Meta-Analysis of Single-Subject Research. Rev. J. Autism Dev. Disord. 2014, 2, 128–140. [Google Scholar] [CrossRef] [Green Version]
- Shane, H.C.; Albert, P.D. Electronic Screen Media for Persons with Autism Spectrum Disorders: Results of a Survey. J. Autism Dev. Disord. 2008, 38, 1499–1508. [Google Scholar] [CrossRef]
- Parsons, S.; Cobb, S. State-of-the-Art of Virtual Reality Technologies for Children on the Autism Spectrum. Eur. J. Spec. Needs Educ. 2011, 26, 355–366. [Google Scholar] [CrossRef]
- Strickland, D. Virtual Reality for the Treatment of Autism. Stud. Health Technol. Inform. 1997, 44, 81–86. [Google Scholar] [PubMed]
- Cesa, G.L.; Manzoni, G.M.; Bacchetta, M.; Castelnuovo, G.; Conti, S.; Gaggioli, A.; Mantovani, F.; Molinari, E.; Cárdenas-López, G.; Riva, G. Virtual Reality for Enhancing the Cognitive Behavioral Treatment of Obesity With Binge Eating Disorder: Randomized Controlled Study With One-Year Follow-Up. J. Med. Internet Res. 2013, 15, e113. [Google Scholar] [CrossRef]
- Rizzo, A.A.; Buckwalter, J.G. Virtual Reality and Cognitive Assessment and Rehabilitation: The State of the Art. Stud. Health Technol. Inform. 1997, 44, 123–145. [Google Scholar] [PubMed]
- Cullen, B.; O’Neill, B.; Evans, J.J.; Coen, R.F.; Lawlor, B.A. A Review of Screening Tests for Cognitive Impairment. J. Neurol. Neurosurg. Psychiatry 2007, 78, 790–799. [Google Scholar] [CrossRef] [Green Version]
- Thielbar, K.; Spencer, N.; Tsoupikova, D.; Ghassemi, M.; Kamper, D. Utilizing Multi-User Virtual Reality to Bring Clinical Therapy into Stroke Survivors’ Homes. J. Hand Ther. 2020, 33, 246–253. [Google Scholar] [CrossRef]
- Thielbar, K.O.; Triandafilou, K.M.; Barry, A.J.; Yuan, N.; Nishimoto, A.; Johnson, J.; Stoykov, M.E.; Tsoupikova, D.; Kamper, D.G. Home-Based Upper Extremity Stroke Therapy Using a Multiuser Virtual Reality Environment: A Randomized Trial. Arch. Phys. Med. Rehabil. 2020, 101, 196–203. [Google Scholar] [CrossRef]
- Schröder, J.; van Criekinge, T.; Embrechts, E.; Celis, X.; Schuppen, J.V.; Truijen, S.; Saeys, W. Combining the Benefits of Tele-Rehabilitation and Virtual Reality-Based Balance Training: A Systematic Review on Feasibility and Effectiveness. Disabil. Rehabil. Assist. Technol. 2019, 14, 2–11. [Google Scholar] [CrossRef]
- Fiest, K.M.; McIntosh, C.J.; Demiantschuk, D.; Leigh, J.P.; Stelfox, H.T. Translating Evidence to Patient Care through Caregivers: A Systematic Review of Caregiver-Mediated Interventions. BMC Med. 2018, 16, 105. [Google Scholar] [CrossRef] [PubMed]
- Loades, M.E.; Chatburn, E.; Higson-Sweeney, N.; Reynolds, S.; Shafran, R.; Brigden, A.; Linney, C.; McManus, M.N.; Borwick, C.; Crawley, E. Rapid Systematic Review: The Impact of Social Isolation and Loneliness on the Mental Health of Children and Adolescents in the Context of COVID-19. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 1218–1239.e3. [Google Scholar] [CrossRef]
- Plagg, B.; Engl, A.; Piccoliori, G.; Eisendle, K. Prolonged Social Isolation of the Elderly during COVID-19: Between Benefit and Damage. Arch. Gerontol. Geriatr. 2020, 89, 104086. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colombini, G.; Duradoni, M.; Carpi, F.; Vagnoli, L.; Guazzini, A. LEAP Motion Technology and Psychology: A Mini-Review on Hand Movements Sensing for Neurodevelopmental and Neurocognitive Disorders. Int. J. Environ. Res. Public Health 2021, 18, 4006. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084006
Colombini G, Duradoni M, Carpi F, Vagnoli L, Guazzini A. LEAP Motion Technology and Psychology: A Mini-Review on Hand Movements Sensing for Neurodevelopmental and Neurocognitive Disorders. International Journal of Environmental Research and Public Health. 2021; 18(8):4006. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084006
Chicago/Turabian StyleColombini, Giulia, Mirko Duradoni, Federico Carpi, Laura Vagnoli, and Andrea Guazzini. 2021. "LEAP Motion Technology and Psychology: A Mini-Review on Hand Movements Sensing for Neurodevelopmental and Neurocognitive Disorders" International Journal of Environmental Research and Public Health 18, no. 8: 4006. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084006