
Mindfulness at Methodist—A Prospective Pilot Study of Mindfulness and Stress Resiliency Interventions in Patients at a Tertiary Care Medical Center



Abstract
:1. Background
2. Methods
2.1. Study Objectives and Outcomes
- ⧫
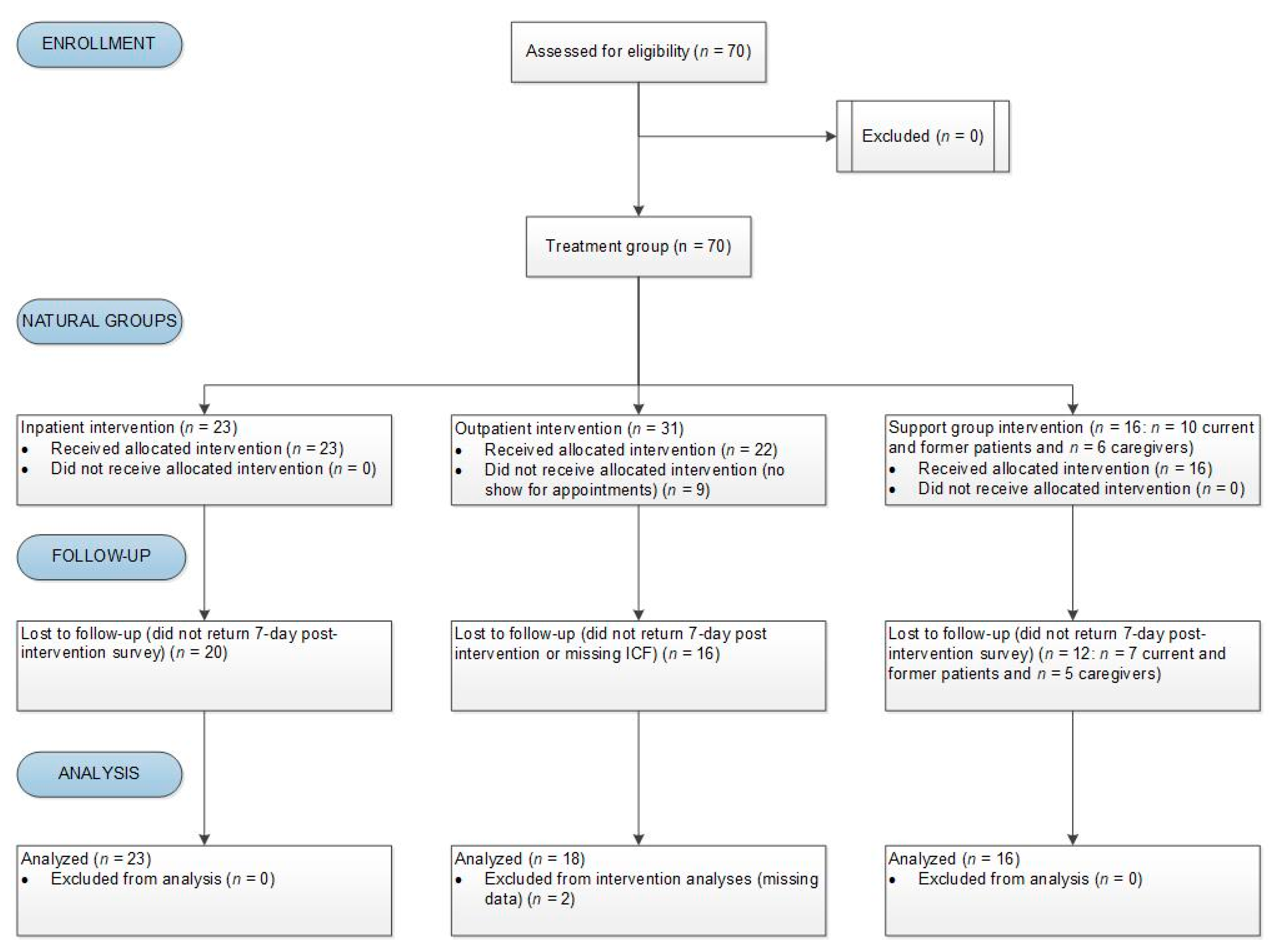
- Cancer inpatients who received the intervention in a one-on-one fashion
- ⧫
- Cancer outpatients who received the intervention in a one-on-one fashion
- ⧫
- Support group participants (i.e., current or former cancer patients and their caregivers) who received the intervention in a group setting
2.2. Feasibility of the Pilot Study Was Ascertained by Intervention Completion and Survey Response Rates. Study Setting and Participants
2.3. Mindful Stress-Reduction Interventions
- Postural (kinesthetic) awareness through guided imagery (somatosensory integration), which is the sense of placement in space and sense of size, shape and texture of things on the bodies surface.
- Postural stability, which is the focus of stability to create safety for a movement. In a stable pose the central nervous system is quieted as fewer signals are sent making external and internal relaxation easier [24].
- Breathing exercises/voluntary breathing, breathing with conscious control that requires focus [25].
- ○
- Abdomino-diaphragmatic breath [26] is at rest inhalation with a passive descent of the respiratory diaphragm, which is critical to normal autonomic function and stress regulation [27]. This works through induction of inhibitory nerve impulses to baroreceptors in the carotid that monitor blood pressure and heart rate. The diaphragmatic descent stimulates slow adapting stretch receptors to down regulate sympathetic tone and the hypothalamic-pituitary-adrenal axis.
- ○
2.4. Stress Intervention Assessments
2.4.1. Perceived Stress
2.4.2. Anxiety
2.4.3. Communication
2.4.4. Visual Analog Scale (VAS) Pain Score
2.4.5. Shared Decision-Making
2.5. Statistical Analysis
3. Results
3.1. Intervention-Associated Outcomes
3.2. Intervention-Associated Outcomes by Demographics
3.3. Relationships Between Anxiety, Stress, Communication and Pain
3.4. Shared Decision-Making
4. Discussion
4.1. Review of Findings
4.2. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANOVA | Analysis of variance |
| CONSORT | Consolidated Standards of Reporting Trials |
| MBSR | Mindfulness-based stress reduction |
| MDMC | Methodist Dallas Medical Center |
| PYTI-C | Professional Yoga Therapy Institute certified |
| SAS | Statistical Analysis System |
| VAS | Visual analog scale |
References
- Kochanek, K.D.; Xu, J.Q.; Arias, E. Mortality in the United States, 2019. In NCHS Data Brief, no 395; National Center for Health Statistics: Hyattsville, MD, USA, 2020. [Google Scholar]
- American Cancer Society: Cancer Facts and Figures 2020. 2020. Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2020/cancer-facts-and-figures-2020.pdf (accessed on 15 March 2021).
- Types of Cancer Treatment; 2020. Available online: https://www.cancer.gov/about-cancer/treatment/types (accessed on 15 March 2021).
- The Psychosocial Needs of Cancer Patients. In Cancer Care for the Whole Patient: Meeting Psychosocial Health Needs; Adler, N.E.; Page, A.E.K. (Eds.) National Academies Press (US): Washington, DC, USA, 2008. [Google Scholar]
- Hickman, R.L., Jr.; Douglas, S.L. Impact of chronic critical illness on the psychological outcomes of family members. Aacn Adv Crit Care 2010, 21, 80–91. [Google Scholar] [CrossRef]
- Vivian, E.; Oduor, H.; Lundberg, L.; Vo, A.; Mantry, P.S. A Cross-Sectional Study of Stress and the Perceived Style of Decision-Making in Clinicians and Patients With Cancer. Health Serv. Res. Manag. Epidemiol. 2019, 6. [Google Scholar] [CrossRef] [Green Version]
- Kotrotsiou, E.; Theodosopoulou, E.; Papathanasiou, I.; Gr, D.; Raftopoulos, V.; E, K. How do patients experience stress caused by hospitalization and how do nurses perceive this stress experienced by patients. A comparative study. Icus Nurs. Web J. 2001, 7, 1. [Google Scholar]
- Musazzi, L.; Tornese, P.; Sala, N.; Popoli, M. Acute or Chronic? A Stressful Question. Trends Neurosci. 2017, 40, 525–535. [Google Scholar] [CrossRef]
- Herbert, T.B.; Cohen, S. Stress and immunity in humans: A meta-analytic review. Psychosom. Med. 1993, 55, 364–379. [Google Scholar] [CrossRef]
- Cohen, S.; Miller, G.E.; Rabin, B.S. Psychological stress and antibody response to immunization: A critical review of the human literature. Psychosom. Med. 2001, 63, 7–18. [Google Scholar] [CrossRef]
- Vivian, E.; Manhas, A.; Lee, A.; Deluna, C.; Oduor, H.; Vo, A.; Davis, A.; Worral, S.; Mantry, P. Evaluation of Oncology Patient Experiences and Preferences for Shared Decision Making and Patient-Centered Care. In Proceedings of the Institute for Health Improvement National Forum, Orlando, FL, USA, 12 December 2017. [Google Scholar]
- Hofmann, S.G.; Sawyer, A.T.; Witt, A.A.; Oh, D. The effect of mindfulness-based therapy on anxiety and depression: A meta-analytic review. J. Consult. Clin. Psychol. 2010, 78, 169–183. [Google Scholar] [CrossRef]
- Mackenzie, M.J.; Carlson, L.E.; Munoz, M.; Speca, M. A qualitative study of self-perceived effects of mindfulness-based stress reduction (MBSR) in a psychosocial oncology setting. Stress Health 2007, 23, 59–69. [Google Scholar] [CrossRef]
- Farb, N.A.; Anderson, A.K.; Mayberg, H.; Bean, J.; McKeon, D.; Segal, Z.V. Minding one’s emotions: Mindfulness training alters the neural expression of sadness. Emotion 2010, 10, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Hargus, E.; Crane, C.; Barnhofer, T.; Williams, J.M.G. Effects of mindfulness on meta-awareness and specificity of describing prodromal symptoms in suicidal depression. Emotion 2010, 10, 34–42. [Google Scholar] [CrossRef]
- Jha, A.P.; Stanley, E.A.; Kiyonaga, A.; Wong, L.; Gelfand, L. Examining the protective effects of mindfulness training on working memory capacity and affective experience. Emotion 2010, 10, 54–64. [Google Scholar] [CrossRef]
- Aherne, D.; Farrant, K.; Hickey, L.; Hickey, E.; McGrath, L.; McGrath, D. Mindfulness based stress reduction for medical students: Optimising student satisfaction and engagement. Bmc Med Educ. 2016, 16, 209. [Google Scholar] [CrossRef] [Green Version]
- Moore, A.; Malinowski, P. Meditation, mindfulness and cognitive flexibility. Conscious. Cogn. 2009, 18, 176–186. [Google Scholar] [CrossRef]
- Verweij, H.; van Ravesteijn, H.; van Hooff, M.L.M.; Lagro-Janssen, A.L.M.; Speckens, A.E.M. Mindfulness-Based Stress Reduction for Residents: A Randomized Controlled Trial. J. Gen. Intern. Med. 2018, 33, 429–436. [Google Scholar] [CrossRef] [Green Version]
- Will, A.; Rancea, M.; Monsef, I.; Wöckel, A.; Engert, A.; Skoetz, N. Mindfulness-based stress reduction for women diagnosed with breast cancer. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- 2019 Cancer Patient Experience Survey Results. 2019. Available online: http://ns.advisory.com/OR-Resource-Q319-Cancer-Patient-Preferences?elq_cid=2802921&x_id=003C000002FKhhQIAT&WT.ac=DBArticleAd_OR_Resource_x_x_Cancer-Patient-Preferences_x_2019Sep25_Eloqua-Daily+Briefing?elqTrackId=224f767093d64f30847822bd48fb2353&elq=04160eda97584ff2b7f2cf1a5a57fd13&elqaid=84041&elqat=1&elqCampaignId=40447&elqcst=272&elqcsid=2757 (accessed on 22 March 2021).
- Williams, A. Therapeutic landscapes in holistic medicine. Soc Sci Med 1998, 46, 1193–1203. [Google Scholar] [CrossRef]
- Verderber, S. Dimensions Ofperson-Window Transactionsin the Hospital Environment. Environ Behav 1986, 18, 450–466. [Google Scholar] [CrossRef]
- Garner, G. Medical Therapeutic Yoga: Biopsychosocial Rehabilitation and Wellness Care, 1st ed.; Handspring Publishing Limited: Pencaitland, East Lothian, UK, 2016. [Google Scholar]
- Gallego, J.; Nsegbe, E.; Durand, E. Learning in respiratory control. Behav. Modif. 2001, 25, 495–512. [Google Scholar] [CrossRef]
- Coulter, D.H. Anatomy of Hatha Yoga: A Manual for Students, Teachers, and Practitioners; Body and Breathe, Inc.: Marlboro, VT, USA, 2010. [Google Scholar]
- Porges, S.W. The polyvagal theory: Phylogenetic substrates of a social nervous system. Int. J. Psychophysiol. Off. J. Int. Organ. Psychophysiol. 2001, 42, 123–146. [Google Scholar] [CrossRef]
- Brown, R.P.; Gerbarg, P.L. The Healing Power of the Breath: Simple Techniques to Reduce Stress and Anxiety, Enhance Concentration, and Balance Your Emotions, 1st ed.; Shambhala Publications, Inc.: Boston, MA, USA, 2012. [Google Scholar]
- Vaschillo, E.G.; Vaschillo, B.; Lehrer, P.M. Characteristics of resonance in heart rate variability stimulated by biofeedback. Appl. Psychophysiol. Biofeedback 2006, 31, 129–142. [Google Scholar] [CrossRef] [PubMed]
- Mellin, L. Emotional Brain Training for Treating Obesity, Eating Disorders, and Stress. Scan’s Pulse 2011, 30, 1–4. [Google Scholar]
- Vivian, E.; Oduor, H.; Arceneaux, S.R.; Flores, J.A.; Vo, A.; Madden, B.M. A Cross-Sectional Study of Perceived Stress, Mindfulness, Emotional Self-Regulation, and Self-Care Habits in Registered Nurses at a Tertiary Care Medical Center. Sage Open Nurs. 2019, 5. [Google Scholar] [CrossRef] [Green Version]
- Cella, D.; Lai, J.S.; Nowinski, C.J.; Victorson, D.; Peterman, A.; Miller, D.; Bethoux, F.; Heinemann, A.; Rubin, S.; Cavazos, J.E.; et al. Neuro-QOL: Brief measures of health-related quality of life for clinical research in neurology. Neurology 2012, 78, 1860–1867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gershon, R.C.; Lai, J.S.; Bode, R.; Choi, S.; Moy, C.; Bleck, T.; Miller, D.; Peterman, A.; Cella, D. Neuro-QOL: Quality of life item banks for adults with neurological disorders: Item development and calibrations based upon clinical and general population testing. Qual. Life Res. 2012, 21, 475–486. [Google Scholar] [CrossRef] [Green Version]
- Neuro QoL-Validation. Available online: Healthmeasures.net (accessed on 16 March 2021).
- Cella, D. User Manual for the Quality of Life in Neurological Disorders (Neuro-QoL) Measures; National Institute of Neurological Disorders and Stroke (NINDS): Bethesda, MA, USA, 2015; Volume 2.0.
- McCormack, H.M.; Horne, D.J.; Sheather, S. Clinical applications of visual analogue scales: A critical review. Psychol. Med. 1988, 18, 1007–1019. [Google Scholar] [CrossRef]
- Knop, C.; Oeser, M.; Bastian, L.; Lange, U.; Zdichavsky, M.; Blauth, M. [Development and validation of the Visual Analogue Scale (VAS) Spine Score]. Unfallchirurg 2001, 104, 488–497. [Google Scholar] [CrossRef]
- Melbourne, E.; Sinclair, K.; Durand, M.A.; Legare, F.; Elwyn, G. Developing a dyadic OPTION scale to measure perceptions of shared decision making. Patient Educ. Couns. 2010, 78, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Nicolai, J.; Moshagen, M.; Eich, W.; Bieber, C. The OPTION scale for the assessment of shared decision making (SDM): Methodological issues. Z. Fur EvidenzFortbild. Und Qual. Im Gesundh. 2012, 106, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, C.J.; Ersser, S.J.; Hopkinson, J.B.; Nicholls, P.G.; Harrington, J.E.; Thomas, P.W. Effectiveness of mindfulness-based stress reduction in mood, breast- and endocrine-related quality of life, and well-being in stage 0 to III breast cancer: A randomized, controlled trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 1335–1342. [Google Scholar] [CrossRef]
- Branstrom, R.; Kvillemo, P.; Brandberg, Y.; Moskowitz, J.T. Self-report mindfulness as a mediator of psychological well-being in a stress reduction intervention for cancer patients--a randomized study. Ann. Behav. Med. A Publ. Soc. Behav. Med. 2010, 39, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Vollestad, J.; Sivertsen, B.; Nielsen, G.H. Mindfulness-based stress reduction for patients with anxiety disorders: Evaluation in a randomized controlled trial. Behav. Res. Ther. 2011, 49, 281–288. [Google Scholar] [CrossRef]
- Goldin, P.R.; Gross, J.J. Effects of mindfulness-based stress reduction (MBSR) on emotion regulation in social anxiety disorder. Emotion 2010, 10, 83–91. [Google Scholar] [CrossRef]
- Bahrami, F.; Yousefi, N. Females are more anxious than males: A metacognitive perspective. Iran J. Psychiatry Behav. Sci. 2011, 5, 83–90. [Google Scholar]
- Lindemann, C. Handbook of the Treatment of the Anxiety Disorders; Jason Aronsoninc: London, UK, 1996. [Google Scholar]
- McLean, C.P.; Asnaani, A.; Litz, B.T.; Hofmann, S.G. Gender differences in anxiety disorders: Prevalence, course of illness, comorbidity and burden of illness. J. Psychiatr Res. 2011, 45, 1027–1035. [Google Scholar] [CrossRef] [Green Version]
- Barre, V.P.; Padmaja, G.; Saxena, R.K.; Rana, S. Impact of medical intervention on stress and quality of life in patients with cancer. Indian J. Palliat. Care 2015, 21, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Bultz, B.D.; Carlson, L.E. Emotional distress: The sixth vital sign--future directions in cancer care. Psycho Oncol. 2006, 15, 93–95. [Google Scholar] [CrossRef]
- Li, Q.; Lin, Y.; Xu, Y.; Zhou, H. The impact of depression and anxiety on quality of life in Chinese cancer patient-family caregiver dyads, a cross-sectional study. Health Qual. Life Outcomes 2018, 16, 230. [Google Scholar] [CrossRef] [PubMed]
- Northouse, L.L.; Mood, D.; Templin, T.; Mellon, S.; George, T. Couples’ patterns of adjustment to colon cancer. Soc. Sci. Med. 2000, 50, 271–284. [Google Scholar] [CrossRef]
- Hagedoorn, M.; Sanderman, R.; Bolks, H.N.; Tuinstra, J.; Coyne, J.C. Distress in couples coping with cancer: A meta-analysis and critical review of role and gender effects. Psychol. Bull 2008, 134, 1–30. [Google Scholar] [CrossRef] [Green Version]
- Social Determinants of Mental Health; World Health Organization and Calouste Gulbenkian Foundation: Geneva, Switzerland, 2014.
- Głąbska, D.; Guzek, D.; Groele, B.; Gutkowska, K. Fruit and Vegetable Intake and Mental Health in Adults: A Systematic Review. Nutrients 2020, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pourmotabbed, A.; Moradi, S.; Babaei, A.; Ghavami, A.; Mohammadi, H.; Jalili, C.; Symonds, M.E.; Miraghajani, M. Food insecurity and mental health: A systematic review and meta-analysis. Public Health Nutr. 2020, 23, 1778–1790. [Google Scholar] [CrossRef] [PubMed]
- Mail Surveys. National Public Research 2019. 2020. Available online: https://nationalpublicresearch.com/services/mail-surveys/ (accessed on 16 March 2021).


{kind=link}
| Study Time Point | ||||
|---|---|---|---|---|
| Immediate Pre-Intervention | Immediate Post-Intervention | Immediate Post-Office Visit | 7-Day Post-Intervention | |
| Treatment Group | Instruments Administered | |||
| Cancer inpatients | Perceived Stress, Anxiety, Communication, Pain | Perceived Stress, Pain | n/a | Anxiety, Communication |
| Cancer outpatients | Perceived Stress, Anxiety, Communication | Perceived Stress | n/a | Anxiety, Communication |
| Support group participants | Perceived Stress, Anxiety, Communication | Perceived Stress | Perceived Stress, Dyadic OPTION | Anxiety, Communication |
| Variable | n (%) | Mean (SD) | Median (IQR) |
|---|---|---|---|
| Source | |||
| Inpatient | 23 (39.0) | ||
| Outpatient | 20 (33.9) | ||
| Support Group Participants | 16 (27.1) | ||
| Age | 60.6 (14.6) | 66.5 (71.0–51.0) | |
| 25–44 | 8 (13.6) | ||
| 45–64 | 17 (28.9) | ||
| 65+ | 29 (49.1) | ||
| Gender | |||
| Female | 34 (60.7) | ||
| Male | 22 (39.3) | ||
| Race | |||
| Black or African American | 17 (30.4) | ||
| White | 33 (58.9) | ||
| Other | 6 (10.7) | ||
| Ethnicity | |||
| Mexican, Mexican American, or Chicano/a | 2 (3.6) | ||
| Not Hispanic, Latino/a, or Spanish origin | 45 (81.8) | ||
| Other Hispanic, Latino/a, or Spanish origin | 6 (10.9) | ||
| Unknown | 2 (3.6) | ||
| Diagnosis | |||
| Breast Cancer | 14 (23.7) | ||
| Liver Cancer | 4 (6.8) | ||
| Pancreas Cancer | 18 (30.5) | ||
| Unknown/Other | 23 (39.0) |
| Perceived Stress Level | Pre-Intervention n (%) | Post-Intervention n (%) | Post MD Visit * n (%) |
|---|---|---|---|
| 1 = Feeling great! | 4 (7.0) | 18 (33.3) | 2 (18.2) |
| 2 = Feeling good | 11 (19.3) | 26 (48.1) | 7 (63.6) |
| 3 = A little stressed | 23 (40.3) | 10 (18.5) | 2 (18.2) |
| 4 = Definitely stressed | 14 (24.6) | 0 (0.0) | 0 (0.0) |
| 5 = Stressed out! | 5 (8.8) | 0 (0.0) | 0 (0.0) |
| Study Instrument | Pre-Intervention | Post-7 Day Intervention | Paired t-test |
|---|---|---|---|
| Anxiety Scale Raw Score | |||
| n | 55 | 16 | t(14) = 3.18, p = 0.0067 |
| Mean (SD) | 56.6 (17.7) | 41.2 (11.9) | |
| Median (IQR) | 54.0 (66.0–41.0) | 43.5 (50.0–31.5) | |
| Communication Scale Raw Score | |||
| n | 55 | 16 | t(14) = −2.82, p = 0.0135 |
| Mean (SD) | 81.7 (17.9) | 90.6 (14.0) | |
| Median (IQR) | 85.0 (95.0–70.0) | 95.0 (100.0–87.5) | |
| Pre-Intervention | Post-Intervention | ||
| Pain VAS * | |||
| n | 21 | 21 | t(20) = −12.96, p < 0.0001 |
| Mean (SD) | 7.0 (2.5) | 2.8 (2.8) | |
| Median (IQR) | 7.0 (8.0–6.0) | 2.0 (5.0–1.0) | |
| Pre-Intervention Perceived Stress Levels | Average Pre-Intervention Anxiety Raw Scores | ANOVA |
|---|---|---|
| Feeling great! | 50.3 ± 13.0 | p = 0.0195 |
| Feeling good | 48.6 ± 14.4 | |
| A little stressed | 52.8 ± 16.5 | |
| Definitely stressed | 64.8 ± 16.3 | |
| Stressed out! | 73.6 ± 21.3 |
| Study Time Period by Instrument Used | Pre-Intervention Anxiety | Post-7-Day Intervention Anxiety | Pre-Intervention Communication | Post-7- Day Intervention Communication | Pre-Intervention VAS | Post-Intervention VAS | |
|---|---|---|---|---|---|---|---|
| Pre-Intervention Anxiety | Correlation | 1 | −0.49428 | −0.26405 | 0.32497 | 0.26735 | |
| p | - | 0.0002 | 0.3416 | 0.1506 | 0.2414 | ||
| Post-7-day Intervention Anxiety | Correlation | 1 | −0.28904 | −0.53468 | −0.27735 | 0.93677 | |
| p | - | 0.2961 | 0.0329 | 0.8211 | 0.2276 | ||
| Pre-Intervention Communication | Correlation | −0.49428 | −0.28904 | 1 | 0.17066 | −0.41255 | |
| p | 0.0002 | 0.2961 | - | 0.8908 | 0.0631 | ||
| Post-7-day Intervention Communication | Correlation | −0.26405 | −0.53468 | 1 | 0.17066 | −0.89290 | |
| p | 0.3416 | 0.0329 | - | 0.8908 | 0.2973 | ||
| Pre-Intervention VAS | Correlation | 0.32497 | −0.27735 | −0.10710 | 0.17066 | 1 | |
| p | 0.1506 | 0.8211 | 0.6440 | 0.8908 | - | ||
| Post-Intervention VAS | Correlation | 0.26735 | 0.93677 | −0.41255 | −0.89290 | ||
| p | 0.2414 | 0.2276 | 0.0631 | 0.2973 | |||
| Item | Question | Response | Patient n = 11 | Physician n = 8 |
|---|---|---|---|---|
| Item 1 | A health problem was identified, where it was made clear that a decision was needed | Strongly agree/agree | 10 | 8 |
| Disagree/strongly disagree | 1 | 0 | ||
| Item 2 | More than way to manage the health problem was described | Strongly agree/agree | 10 | 8 |
| Disagree/strongly disagree | 1 | 0 | ||
| Item 3 | Different sources of information (e.g., leaflets, websites, contact with other people) to help make the decisions were offered | Strongly agree/agree | 9 | 8 |
| Disagree/strongly disagree | 2 | 0 | ||
| Item 4 | Different options (including the possibility of doing nothing) were discussed | Strongly agree/agree | 9 | 8 |
| Disagree/strongly disagree | 2 | 0 | ||
| Item 5 | The advantages, disadvantages and possible outcomes of options were discussed | Strongly agree/agree | 10 | 8 |
| Disagree/strongly disagree | 1 | 0 | ||
| Item 6 | Ideas or expectations about managing the health problem were discussed | Strongly agree/agree | 10 | 8 |
| Disagree/strongly disagree | 1 | 0 | ||
| Item 7 | Concerns or worries about managing the health problem were discussed | Strongly agree/agree | 8 | 8 |
| Disagree/strongly disagree | 3 | 0 | ||
| Item 8 | It was made sure that information had been understood | Strongly agree/agree | 11 | 8 |
| Disagree/strongly disagree | 0 | 0 | ||
| Item 9 | There were opportunities to ask questions | Strongly agree/agree | 10 | 8 |
| Disagree/strongly disagree | 1 | 0 | ||
| Item 10 | The preference to take part in the decision (or not) was respected | Strongly agree/agree | 11 | 8 |
| Disagree/strongly disagree | 0 | 0 | ||
| Item 11 | During the consultation, a decision was made; or there was an agreement to postpone making the decision | Strongly agree/agree | 10 | 8 |
| Disagree/strongly disagree | 1 | 0 | ||
| Item 12 | The possibility of coming back to the decision was discussed | Strongly agree/agree | 9 | 8 |
| Disagree/strongly disagree | 2 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vivian, E.; Oduor, H.; Girisha, P.; Mantry, P. Mindfulness at Methodist—A Prospective Pilot Study of Mindfulness and Stress Resiliency Interventions in Patients at a Tertiary Care Medical Center. Int. J. Environ. Res. Public Health 2021, 18, 4034. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084034
Vivian E, Oduor H, Girisha P, Mantry P. Mindfulness at Methodist—A Prospective Pilot Study of Mindfulness and Stress Resiliency Interventions in Patients at a Tertiary Care Medical Center. International Journal of Environmental Research and Public Health. 2021; 18(8):4034. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084034
Chicago/Turabian StyleVivian, Elaina, Hellen Oduor, Preeti Girisha, and Parvez Mantry. 2021. "Mindfulness at Methodist—A Prospective Pilot Study of Mindfulness and Stress Resiliency Interventions in Patients at a Tertiary Care Medical Center" International Journal of Environmental Research and Public Health 18, no. 8: 4034. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084034