
Feasibility and Acceptability of a Tailored Infant Safe Sleep Coaching Intervention for African American Families



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. My Baby’s Sleep Family Intervention
- A structured workbook;
- An appendix of information sheets explaining and citing research on various topics including supine sleep position, calming a fussy baby, establishing sleep routines, infant sleep patterns, and maternal self-care;
- a local resource guide [43];
- brochures from the National Institute for Child Health and Human Development (NICHD) Safe to Sleep® campaign [9]
2.3.1. Social Network Engagement
2.3.2. Client-Centered
2.3.3. Tailored Information
2.3.4. Risk Reduction Approach
2.3.5. Home Visits
2.4. Procedures
2.5. Measures
2.5.1. Feasibility
2.5.2. Intervention Acceptability
2.6. Data Analysis
3. Results
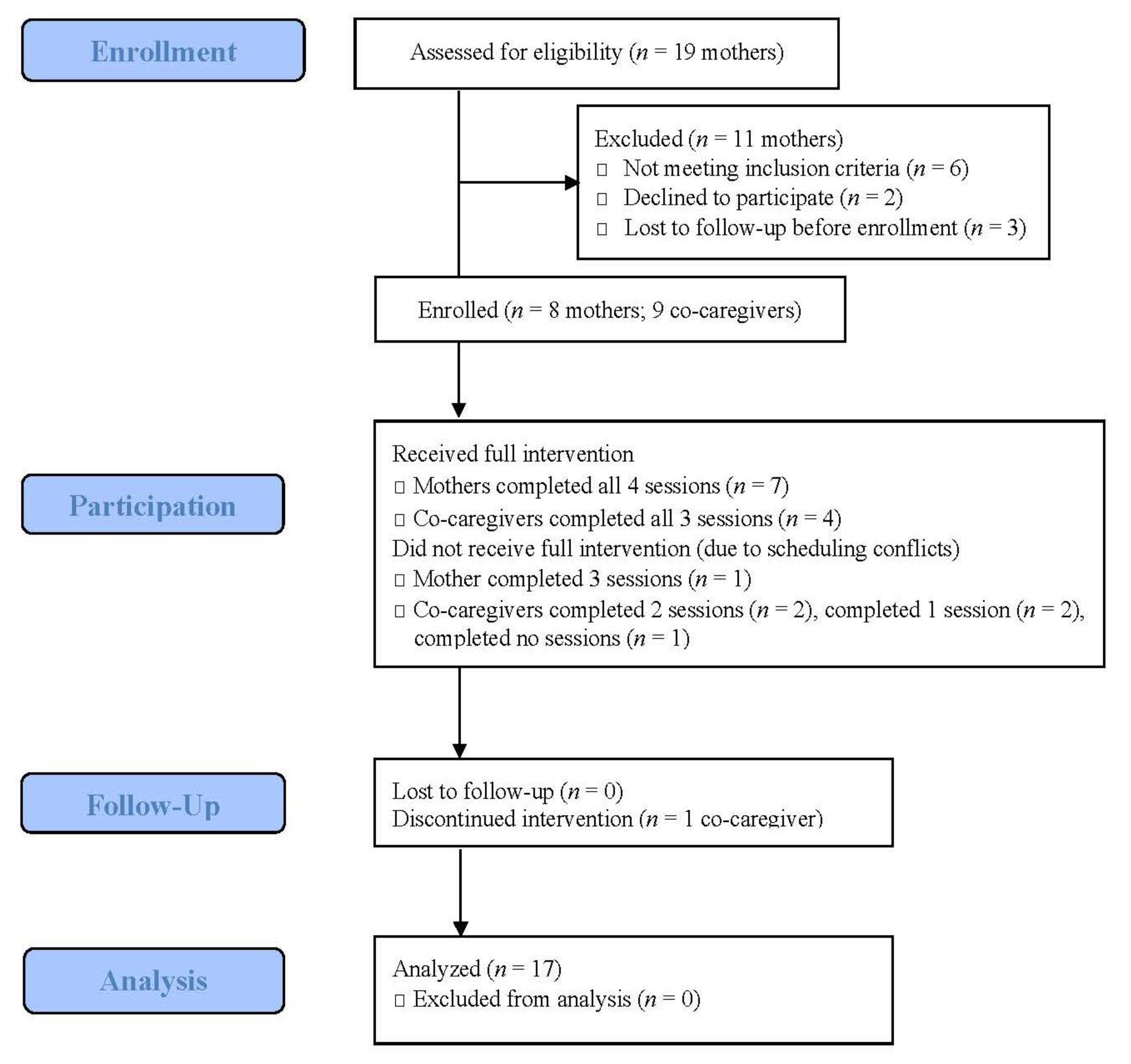
3.1. Participants
3.2. Feasibility
- One session was shortened for a mother experiencing a family emergency;
- Content from two sessions was combined when a session was missed due to mother’s household move;
- Several sessions were modified because a co-caregiver was not present.
- Enthusiastic buy-in and assistance from community partners, for example, adding recruitment flyers to prenatal care “welcome” packets and placing flyers in the waiting area;
- Parental interest in participating, including strong engagement with coaches—for example, many families texted the coach within a few days of the infant’s birth, and three mothers referred friends to the study;
- Study cellphones with text messaging capability facilitated communication (most participants preferred text messaging over phone calls) and provided mobile hotspots to play videos at home visits;
- Offering weekend and evening visits allowed more scheduling flexibility, especially for co-caregivers.
3.3. Acceptability
3.3.1. Positive Aspects of MBS
- Safe sleep information and resources provided (eight families). Families noted the safe sleep information was helpful, including coaches discussing the reasoning behind recommendations. One mother noted, “just the constant reminder of why it’s important to put the baby on a flat surface”. Among families who had older children, several commented MBS was a helpful reminder, especially as some recommendations had changed over time: “no matter how close your kids are (in age), you always lose some type of information.” A few participants also reported using riskier practices with previous children (i.e., stomach sleeping, bed-sharing) that they did not want to repeat with their new infant. Families reported coaches connected them with needed resources: “She helped me with different resources as far as living-wise. She helped me find a house with 2-1-1 (an information and referral line)”. Families also noted the videos and interactive card sort exercise were useful in processing and summarizing the recommendations;
- Binder/workbook (eight families). Although only about half of the families wrote on workbook pages during sessions, all reported referring back to the workbook and informational handouts between sessions. In particular, participants reported referring to handouts on infant sleep patterns, calming a fussy baby, and maternal self-care. One mother noted: “that’s when I had a hard time, when they are fussy. Like how can I calm them down? In the book it got a lot of options when you can calm them down.” Others noted the local resource booklet [43] and Safe to Sleep® grandparent brochure [9] were helpful;
- Educational support tools (eight families). All families commented positively on the educational support tools. All but one mother reported using the travel bassinet for infant sleep at least once per week. Three mothers used the travel bassinet as an alternative to bed-sharing, and several mothers used it when visiting other homes. All eight mothers reported the safe sleep board book [44] was helpful in reminding them of safe sleep recommendations; seven read the board book to their baby at least once. Two families noted an older sibling “read” the board book to the infant. Four families reported the pacifiers were useful; others did not use them;
- Timing of visits (eight families). All families commented positively on having visits during pregnancy to help with planning for the new baby, for example, “I was nervous, because I didn’t know what to do when she get here”. Several noted visits during pregnancy were helpful to get on the “same page” with co-caregivers: “You helped us prepare for them...you helped us get together, help us get in the mind frame, like, it’s coming, the stuff that’s needed”. Visits after baby was born were also helpful to address challenges to following recommendations. One mother noted: “When you get ready to prepare for him, you think you’re going to be able to follow the steps and have baby the safe way. Then when you have him, you actually see what it’s like”;
- Home visits (eight families). Families noted that home visits were helpful for several reasons, including avoiding transportation and childcare issues, not wanting to take a young infant outside of the house, and the inconvenience of trying to ready an infant and other children for travelling;
- Co-caregiver involvement (five families). Families noted that sharing information with co-caregivers was helpful, as well as helping mother think about who will be involved with infant care. One mother noted: “She (infant’s grandmother) said, ‘oh, I like that. I never had this before’. I think that was very helpful to give the co-caregivers (information), so the mother don’t feel so overwhelmed, like she’s the only one that’s getting all the information when it’s obviously going to be other people watching the baby, too”.
3.3.2. Suggestions for Improvement
- More interactive activities (five families). Families suggested adding more interactive activities such as the interactive card sort activity. One father suggested “doing a little (crib) display setup, (asking) ‘how would you set this up?’ seeing how people would set it up...just see where their head is at”. His partner added, “because the doctor, they don’t really show you...but having someone to come in and actually show you how...that would be really helpful”. Another mother suggested physical demonstration could better illustrate suffocation hazards, “show them the dangers of like having the blanket and what that stuff can do or having toys in there”.
- Offering televisits (five families). Several families suggested video calls to add even more scheduling flexibility and to engage co-caregivers with limited availability. Families suggested having some in-person visits (for example, having the first visit in-person and then offering video calls for later sessions (while still offering in-person visits for those who preferred that option).
- Additional content suggestions (three families). Families suggested more detailed content on the following topics: tummy time while awake, specific suggestions for getting baby to sleep when not in physical contact with mother, and pointers for transitioning infants who prefer to sleep on their stomachs away from stomach-sleeping.
- Actively involve siblings (two families). Families also noted that often older siblings are involved in infant care and suggested engaging them in the intervention, for example, “keep the kids involved, the siblings...we say go get the bottle, go grab his diaper...we try to give everybody roles”. Interactive activities such as the crib display could be geared towards siblings “to teach them don’t shake the crib, don’t put toys in there with the baby, don’t put blankets on them”.
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. About Sudden Unexpected Infant Death and Sudden Infant Death Syndrome. Available online: http://www.cdc.gov/sids/about (accessed on 21 February 2021).
- Goldwater, P.N. SIDS, prone sleep position and infection: An overlooked epidemiological link in current SIDS research? Key evidence for the “Infection Hypothesis”. Med. Hypotheses 2020, 144, 110114. [Google Scholar] [CrossRef]
- Spinelli, J.; Collins-Praino, L.; Heuvel, C.V.D.; Byard, R.W. Evolution and significance of the triple risk model in sudden infant death syndrome. J. Paediatr. Child Health 2016, 53, 112–115. [Google Scholar] [CrossRef] [PubMed]
- Filiano, J.J.; Kinney, H.C. A Perspective on Neuropathologic Findings in Victims of the Sudden Infant Death Syndrome: The Triple-Risk Model. Neonatololgy 1994, 65, 194–197. [Google Scholar] [CrossRef]
- Carlin, R.F.; Moon, R.Y. Risk Factors, Protective Factors, and Current Recommendations to Reduce Sudden Infant Death Syndrome. JAMA Pediatr. 2017, 171, 175–180. [Google Scholar] [CrossRef]
- Fleming, P.J.; Blair, P.S.; Pease, A. Sudden unexpected death in infancy: Aetiology, pathophysiology, epidemiology and prevention in 2015. Arch. Dis. Child. 2015, 100, 984–988. [Google Scholar] [CrossRef] [PubMed]
- Moon, R.Y.; Hauck, F.R.; Abbass-Dick, J.; Stern, S.B.; Nelson, L.E.; Watson, W.; Dennis, C.-L. Hazardous Bedding in Infants’ Sleep Environment Is Still Common and a Cause for Concern. Pediatrics 2014, 135, 178–179. [Google Scholar] [CrossRef] [Green Version]
- Syndrome, T.F.O.S.I.D. SIDS and Other Sleep-Related Infant Deaths: Updated 2016 Recommendations for a Safe Infant Sleeping Environment. Pediatrics 2016, 138, e20162938. [Google Scholar] [CrossRef]
- National Institute of Child Health and Human. Safe to Sleep® Campaign Materials. Available online: https://safetosleep.nichd.nih.gov/materials (accessed on 21 February 2021).
- Chu, T.; Hackett, M.; Kaur, N. Housing influences among sleep-related infant injury deaths in the USA. Health Promot. Int. 2015, 31, 396–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathews, A.; Oden, R.; Joyner, B.; He, J.; McCarter, R.; Moon, R.Y. Differences in African–American Maternal Self-Efficacy Regarding Practices Impacting Risk for Sudden Infant Death. J. Community Health 2015, 41, 244–249. [Google Scholar] [CrossRef] [Green Version]
- Moon, R.Y.; Mathews, A.; Joyner, B.L.; Oden, R.P.; He, J.; McCarter, R. Health Messaging and African–American Infant Sleep Location: A Randomized Controlled Trial. J. Community Health 2016, 42, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ajao, T.I.; Oden, R.P.; Joyner, B.L.; Moon, R.Y. Decisions of Black Parents About Infant Bedding and Sleep Surfaces: A Qualitative Study. Pediatrics 2011, 128, 494–502. [Google Scholar] [CrossRef] [Green Version]
- Chu, T.; Hackett, M.; Kaur, N. Exploring Caregiver Behavior and Knowledge About Unsafe Sleep Surfaces in Infant Injury Death Cases. Health Educ. Behav. 2015, 42, 293–301. [Google Scholar] [CrossRef]
- Gaydos, L.M.; Blake, S.C.; Gazmararian, J.A.; Woodruff, W.; Thompson, W.W.; Dalmida, S.G. Revisiting Safe Sleep Recommendations for African-American Infants: Why Current Counseling is Insufficient. Matern. Child Health J. 2015, 19, 496–503. [Google Scholar] [CrossRef]
- Hackett, M.; Simons, H. Parental Adherence to Infant Sleep Safety Recommendations. J. Community Med. Health Educ. 2016, 3, 219–225. [Google Scholar] [CrossRef] [Green Version]
- Herman, S.; Adkins, M.; Moon, R.Y. Knowledge and Beliefs of African-American and American Indian Parents and Supporters About Infant Safe Sleep. J. Community Health 2014, 40, 12–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathews, A.A.; Joyner, B.L.; Oden, R.P.; Alamo, I.; Moon, R.Y. Comparison of Infant Sleep Practices in African-American and US Hispanic Families: Implications for Sleep-Related Infant Death. J. Immigr. Minor. Health 2014, 17, 834–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, T.C.S.; Doering, J.J. Application of a Socio-Ecological Model to Mother–Infant Bed-Sharing. Health Educ. Behav. 2014, 41, 577–589. [Google Scholar] [CrossRef] [PubMed]
- Ward, T.C.S.; Ngui, E.M. Factors Associated with Bed-Sharing for African American and White Mothers in Wisconsin. Matern. Child Health J. 2014, 19, 720–732. [Google Scholar] [CrossRef] [PubMed]
- Ward, T.C.S.; Balfour, G.M. Infant Safe Sleep Interventions, 1990–2015: A Review. J. Community Health 2016, 41, 180–196. [Google Scholar] [CrossRef] [PubMed]
- Ward, T.C.S.; Robb, S.W.; Kanu, F.A. Prevalence and Characteristics of Bed-Sharing Among Black and White Infants in Georgia. Matern. Child Health J. 2015, 20, 347–362. [Google Scholar] [CrossRef]
- Hwang, S.S.; Corwin, M.J. Safe Infant Sleep Practices: Parental Engagement, Education, and Behavior Change. Pediatr. Ann. 2017, 46, e291–e296. [Google Scholar] [CrossRef]
- Moon, R.Y.; Hauck, F.R.; Colson, E.R. Safe Infant Sleep Interventions: What is the Evidence for Successful Behavior Change? Curr. Pediatr. Rev. 2016, 12, 67–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauck, F.R.; Tanabe, K.O.; McMurry, T.; Moon, R.Y. Evaluation of bedtime basics for babies: A national crib distribution program to reduce the risk of sleep-related sudden infant deaths. J. Community Health 2014, 40, 457–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooker, E.; Ball, H.L.; Kelly, P.J. Sleeping like a baby: Attitudes and experiences of bedsharing in Northeast England. Med. Anthr. 2001, 19, 203–222. [Google Scholar] [CrossRef]
- Kellams, A.; Hauck, F.R.; Moon, R.Y.; Kerr, S.M.; Heeren, T.; Corwin, M.J.; Colson, E. Factors Associated With Choice of Infant Sleep Location. Pediatrics 2020, 145, e20191523. [Google Scholar] [CrossRef] [PubMed]
- Ward, T.C.S. Reasons for Mother–Infant Bed-Sharing: A Systematic Narrative Synthesis of the Literature and Implications for Future Research. Matern. Child Health J. 2014, 19, 675–690. [Google Scholar] [CrossRef]
- Tully, K.P.; Holditch-Davis, D.; Brandon, D. The Relationship Between Planned and Reported Home Infant Sleep Locations Among Mothers of Late Preterm and Term Infants. Matern. Child Health J. 2015, 19, 1616–1623. [Google Scholar] [CrossRef] [PubMed]
- Altfeld, S.; Peacock, N.; Rowe, H.L.; Massino, J.; Garland, C.; Smith, S.; Wishart, M. Moving Beyond “Abstinence-Only” Messaging to Reduce Sleep-Related Infant Deaths. J. Pediatr. 2017, 189, 207–212. [Google Scholar] [CrossRef]
- Verbiest, S.; Tully, K.; Simpson, M.; Stuebe, A. Elevating mothers’ voices: Recommendations for improved patient-centered postpartum. J. Behav. Med. 2018, 41, 577–590. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDierR) checklist and guide. BMJ 2014, 348, 1687. [Google Scholar] [CrossRef] [Green Version]
- Lancaster, G.A.; Thabane, L. Guidelines for reporting non-randomised pilot and feasibility studies. Pilot Feasibility Stud. 2019, 5, 1–6. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Ecology of the family as a context for human development: Research perspectives. Dev. Psychol. 1986, 22, 723–742. [Google Scholar] [CrossRef]
- Moon, R.Y.; Corwin, M.J.; Kerr, S.; Heeren, T.; Colson, E.; Kellams, A.; Geller, N.L.; Drake, E.; Tanabe, K.; Hauck, F.R. Mediators of Improved Adherence to Infant Safe Sleep Using a Mobile Health Intervention. Pediatrics 2019, 143, e20182799. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Mathews, A.; Joyner, B.L.; Oden, R.P.; He, J.; McCarter, R.; Moon, R.Y. Messaging Affects the Behavior of African American Parents with Regards to Soft Bedding in the Infant Sleep Environment: A Randomized Controlled Trial. J. Pediatr. 2016, 175, 79.e2–85.e2. [Google Scholar] [CrossRef]
- Colson, E.R.; Geller, N.L.; Heeren, T.; Corwin, M.J. Factors Associated With Choice of Infant Sleep Position. Pediatrics 2017, 140, e20170596. [Google Scholar] [CrossRef] [Green Version]
- Ward, T.C.S.; McClellan, M.M.; Miller, T.J.; Brown, S. Evaluation of a Crib Distribution and Safe Sleep Educational Program to Reduce Risk of Sleep-Related Infant Death. J. Community Health 2018, 43, 848–855. [Google Scholar] [CrossRef] [PubMed]
- Carlin, R.F.; Abrams, A.; Mathews, A.; Joyner, B.L.; Oden, R.; McCarter, R.; Moon, R.Y. The Impact of Health Messages on Maternal Decisions About Infant Sleep Position: A Randomized Controlled Trial. J. Community Health 2018, 43, 977–985. [Google Scholar] [CrossRef]
- Hwang, S.S.; Rybin, D.V.; Heeren, T.C.; Colson, E.R.; Corwin, M.J. Trust in Sources of Advice about Infant Care Practices: The SAFE Study. Matern. Child Health J. 2016, 20, 1956–1964. [Google Scholar] [CrossRef]
- Oden, R.P.; Joyner, B.L.; Ajao, T.I.; Moon, R.Y. Factors influencing African American mothers’ decisions about sleep position: A qualitative study. J. Natl. Med Assoc. 2010, 102, 870–880. [Google Scholar] [CrossRef]
- Mental Health America of Wisconsin. Mental Health & Wellness Resource Guide for Milwaukee County; Mental Health America of Wisconsin: Milwaukee, WI, USA, 2017; Available online: http://www.mhawisconsin.org/print-guide.aspx (accessed on 21 February 2021).
- Hutton, J. Sleep Baby, Safe and Snug; Blue Manatee Press: Cincinnati, OH, USA, 2016. [Google Scholar]
- Hutton, J.S.; Gupta, R.; Gruber, R.; Berndsen, J.; DeWitt, T.; Ollberding, N.J.; Van Ginkel, J.B.; Ammerman, R.T. Randomized Trial of a Children’s Book Versus Brochures for Safe Sleep Knowledge and Adherence in a High-Risk Population. Acad. Pediatr. 2017, 17, 879–886. [Google Scholar] [CrossRef]
- Bronheim, S. Building on Campaigns with Conversations: An Individualized Approach to Helping Families Embrace Safe Sleep and Breastfeeding; National Center for Education in Maternal and Child Health: Washington, DC, USA, 2017. [Google Scholar]
- Carlin, R.F.; Mathews, A.; Oden, R.; Moon, R.Y. The Influence of Social Networks and Norms on Breastfeeding in African American and Caucasian Mothers: A Qualitative Study. Breastfeed. Med. 2019, 14, 640–647. [Google Scholar] [CrossRef]
- Moon, R.Y.; Mathews, A.; Oden, R.; Carlin, R. A Qualitative Analysis of How Mothers’ Social Networks Are Established and Used to Make Infant Care Decisions. Clin. Pediatr. 2019, 58, 985–992. [Google Scholar] [CrossRef]
- Barry, M.J.; Edgman-Levitan, S. Shared Decision Making—The Pinnacle of Patient-Centered Care. N. Engl. J. Med. 2012, 366, 780–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gray, B.; Coker, T.R. When shared decision-making and evidence based practice clash: Infant sleep practices. J. Paediatr. Child Health 2019, 55, 1009–1012. [Google Scholar] [CrossRef] [Green Version]
- Shipstone, R.A.; Young, J.; Kearney, L.; Thompson, J.M.D. Applying a Social Exclusion Framework to Explore the Relationship Between Sudden Unexpected Deaths in Infancy (SUDI) and Social Vulnerability. Front. Public Health 2020, 8, 563573. [Google Scholar] [CrossRef] [PubMed]
- Ball, H.L.; Volpe, L.E. Sudden Infant Death Syndrome (SIDS) risk reduction and infant sleep location—Moving the discussion forward. Soc. Sci. Med. 2013, 79, 84–91. [Google Scholar] [CrossRef] [Green Version]
- Blair, P.S.; Ball, H.L.; McKenna, J.J.; Feldman-Winter, L.; Marinelli, K.A.; Bartick, M.C.; Young, M.; Noble, L.; Calhoun, S.; Elliott-Rudder, M.; et al. Bedsharing and Breastfeeding: The Academy of Breastfeeding Medicine Protocol #6, Revision 2019. Breastfeed. Med. 2020, 15, 5–16. [Google Scholar] [CrossRef] [Green Version]
- Peacock, N.R.; Altfeld, S.; Rosenthal, A.L.; Garland, C.E.; Massino, J.M.; Smith, S.L.; Rowe, H.L.; Wagener, S.E. Qualitative Analysis of Infant Safe Sleep Public Campaign Messaging. Health Promot. Pract. 2017, 19, 203–212. [Google Scholar] [CrossRef]
- Pease, A.; Blair, P.S.; Ingram, J.; Fleming, P. Conversations with families about reducing the risk of sudden infant death syndrome. J. Health Visit. 2019, 7, 226–231. [Google Scholar] [CrossRef] [Green Version]
- Doering, J.J.; Lim, P.S.; Ward, T.C.S.; Davies, W.H. Prevalence of unintentional infant bedsharing. Appl. Nurs. Res. 2019, 46, 28–30. [Google Scholar] [CrossRef] [PubMed]
- Kendall–Tackett, K.; Cong, Z.; Hale, T.W. Mother–Infant Sleep Locations and Nighttime Feeding Behavior: U.S. Data from the Survey of Mothers’ Sleep and Fatigue. Clin. Lact. 2010, 1, 27–31. [Google Scholar] [CrossRef]
- Kendrick, D.; A Mulvaney, C.; Ye, L.; Stevens, T.; A Mytton, J.; Stewart-Brown, S. Parenting interventions for the prevention of unintentional injuries in childhood. Cochrane Database Syst. Rev. 2013, 3, CD006020. [Google Scholar] [CrossRef]
- Peacock, S.; Konrad, S.; Watson, E.; Nickel, D.; Muhajarine, N. Effectiveness of home visiting programs on child outcomes: A systematic review. BMC Public Health 2013, 13, 17. [Google Scholar] [CrossRef] [Green Version]
- Horvath, A.O.; Greenberg, L.S. Development and validation of the Working Alliance Inventory. J. Couns. Psychol. 1989, 36, 223–233. [Google Scholar] [CrossRef]
- Tracey, T.J.; Kokotovic, A.M. Factor structure of the Working Alliance Inventory. Psychol. Assess. 1989, 1, 207–210. [Google Scholar] [CrossRef]
- Doering, J.J.; Dogan, S. A Postpartum Sleep and Fatigue Intervention Feasibility Pilot Study. Behav. Sleep Med. 2018, 16, 185–201. [Google Scholar] [CrossRef]
- Alio, A.P.; Richman, A.R.; Clayton, H.B.; Jeffers, D.F.; Wathington, D.J.; Salihu, H.M. An ecological approach to understanding black-white disparities in perinatal mortality. Matern. Child Health J. 2010, 14, 557–566. [Google Scholar] [CrossRef]


{kind=link}
| Session Number/Timing | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 7–8th Month of Pregnancy | 8–9th Month of Pregnancy | 2–4 Weeks of Age | 2–3 Months of Age | |
| Format | Mother only | Mother + Co-Caregivers | Mother + Co-Caregivers | Mother + Co-Caregivers |
| Session Focus | Engagement Assessment Goal setting | Engagement Assessment Goal setting | Assessment of sleep safety Skill-building Consensus-building Problem-solving Anticipatory guidance | |
| Session Activities | My goals and hopes for baby My worries and concerns My support system Planning baby’s sleep Handling stress | Our new arrival Supporting mom Baby sleep recommendations How we put it all together | Our baby sleep challenges Making realistic plans together Supporting mom and baby Common sleep challenges Baby sleep patterns Sleep tips for mom | |
| Characteristic | Number | Percent | |
|---|---|---|---|
| Maternal Demographics (n = 8) | |||
| Age (average, in years) | 26.1 (18–32) | ||
| Race | African American | 7 | 87.5 |
| Bi-racial (African American and White) | 1 | 12.5 | |
| Ethnicity | Not Hispanic | 7 | 87.5 |
| Hispanic | 1 | 12.5 | |
| Education | Some high school | 2 | 25 |
| High school grad/GED | 3 | 37.5 | |
| Some college/technical/vocational | 2 | 25 | |
| Technical/vocational graduate | 0 | 0 | |
| 4-year college graduate | 1 | 12.5 | |
| Marital status | Living with partner/married | 5 | 62.5 |
| Single | 3 | 37.5 | |
| Insurance type | Private, employer | 1 | 12.5 |
| Income-contingent state health plan | 4 | 50 | |
| Medicaid | 3 | 37.5 | |
| Co-Caregiver Demographics (n = 9) | |||
| Relationship to infant | Father | 6 | 66.7 |
| Grandmother | 2 | 22.2 | |
| Aunt | 1 | 11.1 | |
| Age (average, in years) | 31.1 (18–58) | ||
| Race | African American | 8 | 88.9 |
| Bi-racial (not specified) | 1 | 11.1 | |
| Ethnicity | Not Hispanic | 7 | 77.8 |
| Hispanic | 2 | 22.2 | |
| Education | Some high school | 5 | 55.6 |
| High school grad/GED | 2 | 22.2 | |
| Some college/technical/vocational | 1 | 11.1 | |
| Technical/vocational graduate | 1 | 11.1 | |
| Item 1 | Session 1 (n = 8) | Session 2 (n = 8) | Session 3 (n = 7) | Session 4 (n = 8) | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Intervention Helpfulness | ||||||||
| Today’s visit was helpful. | 3.0 | 0 | 2.9 | 0.4 | 2.9 | 0.4 | 3.0 | 0 |
| I would recommend this visit to my friends. | 2.9 | 0.4 | 3.0 | 0 | 2.9 | 0.4 | 3.0 | 0 |
| I learned a lot from this visit. | 2.9 | 0.4 | 2.9 | 0.4 | 2.7 | 0.5 | 2.9 | 0.4 |
| Coach Engagement | ||||||||
| I liked my coach. | 3.0 | 0 | 3.0 | 0 | 3.0 | 0 | 3.0 | 0 |
| My coach was helpful to me. | 3.0 | 0 | 3.0 | 0 | 3.0 | 0 | 3.0 | 0 |
| My coach cares about me as a person. | 3.0 | 0 | 3.0 | 0 | 3.0 | 0 | 3.0 | 0 |
| My coach respects me. | 3.0 | 0 | 3.0 | 0 | 3.0 | 0 | 3.0 | 0 |
| My coach listens to me. | 3.0 | 0 | 3.0 | 0 | 3.0 | 0 | 3.0 | 0 |
| My coach had useful recommendations. | 3.0 | 0 | 3.0 | 0 | 3.0 | 0 | 3.0 | 0 |
| My coach understands me and my life. | 3.0 | 0 | 3.0 | 0 | 2.9 | 0.4 | 3.0 | 0 |
| Item 2 | Session 2 (n = 7) | Session 3 (n = 5) | Session 4 (n = 5) | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Intervention Helpfulness | ||||||
| Today’s visit was helpful. | 3.0 | 0 | 3.0 | 0 | 2.8 | 0.5 |
| I would recommend this visit to my friends. | 3.0 | 0 | 3.0 | 0 | 2.8 | 0.5 |
| I learned a lot from this visit. | 2.9 | 0.4 | 2.8 | 0.5 | 2.8 | 0.5 |
| Coach Engagement | ||||||
| I liked my coach. | 2.7 | 0.5 | 3.0 | 0 | 2.8 | 0.5 |
| My coach was helpful to me. | 3.0 | 0 | 3.0 | 0 | 2.8 | 0.5 |
| My coach cares about me as a person. | 2.7 | 0.5 | 2.8 | 0.5 | 2.6 | 0.6 |
| My coach respects me. | 3.0 | 0 | 3.0 | 0 | 3.0 | 0 |
| My coach listens to me. | 3.0 | 0 | 3.0 | 0 | 3.0 | 0 |
| My coach had useful recommendations. | 2.9 | 0.4 | 3.0 | 0 | 2.8 | 0.5 |
| My coach understands me and my life. | 2.7 | 0.5 | 2.8 | 0.5 | 2.6 | 0.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salm Ward, T.C.; McPherson, J.; Kogan, S.M. Feasibility and Acceptability of a Tailored Infant Safe Sleep Coaching Intervention for African American Families. Int. J. Environ. Res. Public Health 2021, 18, 4133. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084133
Salm Ward TC, McPherson J, Kogan SM. Feasibility and Acceptability of a Tailored Infant Safe Sleep Coaching Intervention for African American Families. International Journal of Environmental Research and Public Health. 2021; 18(8):4133. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084133
Chicago/Turabian StyleSalm Ward, Trina C., Jane McPherson, and Steven M. Kogan. 2021. "Feasibility and Acceptability of a Tailored Infant Safe Sleep Coaching Intervention for African American Families" International Journal of Environmental Research and Public Health 18, no. 8: 4133. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084133