
The Health Literacy Status and Its Role in Interventions in Iran: A Systematic and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
- What is the HL status of the Iranian population?
- What are the commonly used instruments for measuring HL in Iran?
- Is there an association between individuals’ HL and self-care behaviors, self-efficacy, health promotion behaviors (healthy food and physical activity), medical adherence, knowledge, and communication skills?
- Can HL intervention improve HL skills (includes reading, writing, listening, speaking, numeracy, and critical analysis) and health outcomes?
2.1. Search Strategy
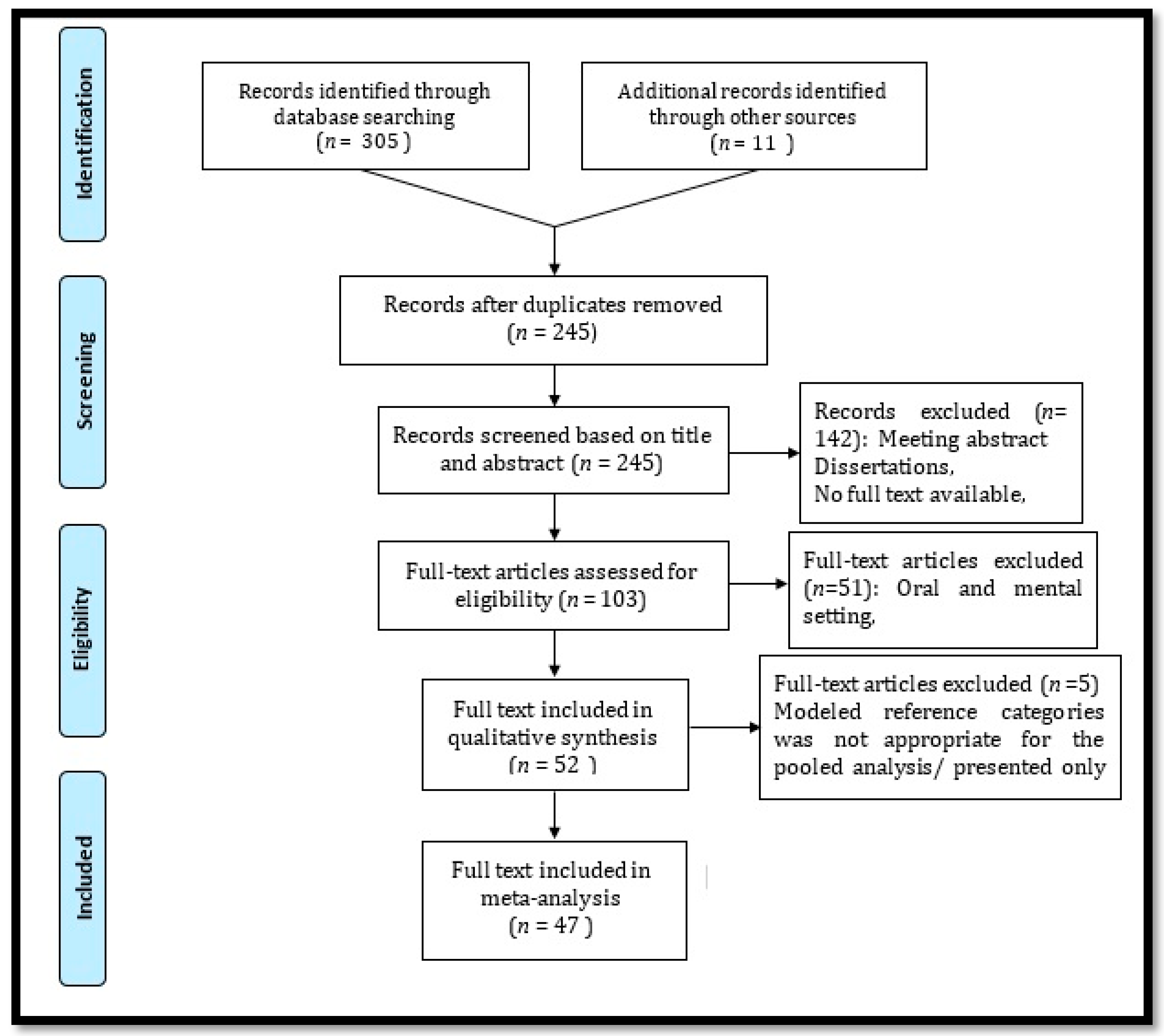
2.2. Article Selections and Screening
2.3. Data Extraction and Quality Assessment
2.4. Meta-Analysis Assessment
3. Results
3.1. Search Outcome
3.2. Study Designs and Populations
3.3. Methodological Quality
3.4. Health Literacy Tools
3.5. Systematic Review
3.6. Meta-Analysis
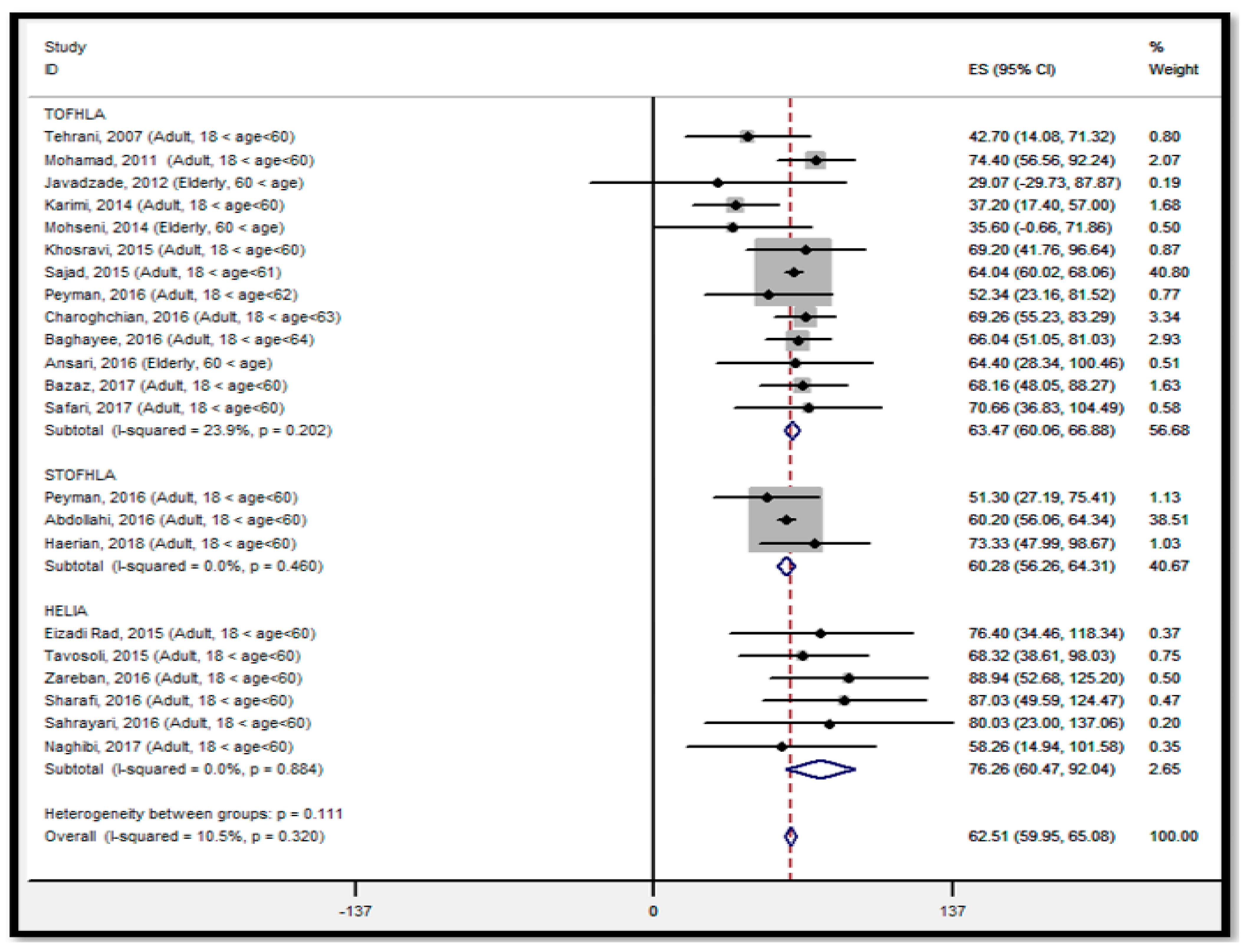
3.6.1. Health Literacy Status
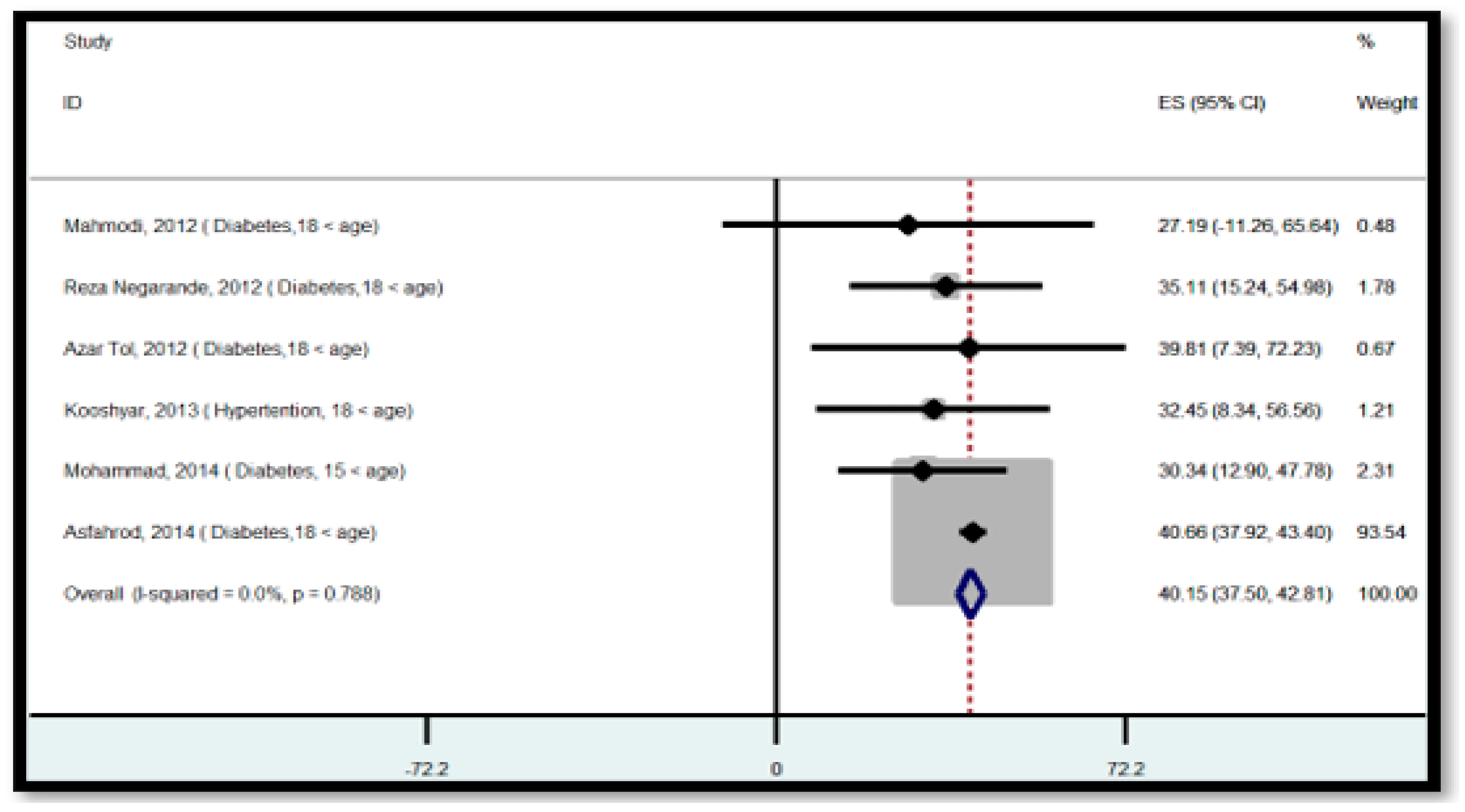
3.6.2. Binary Outcome
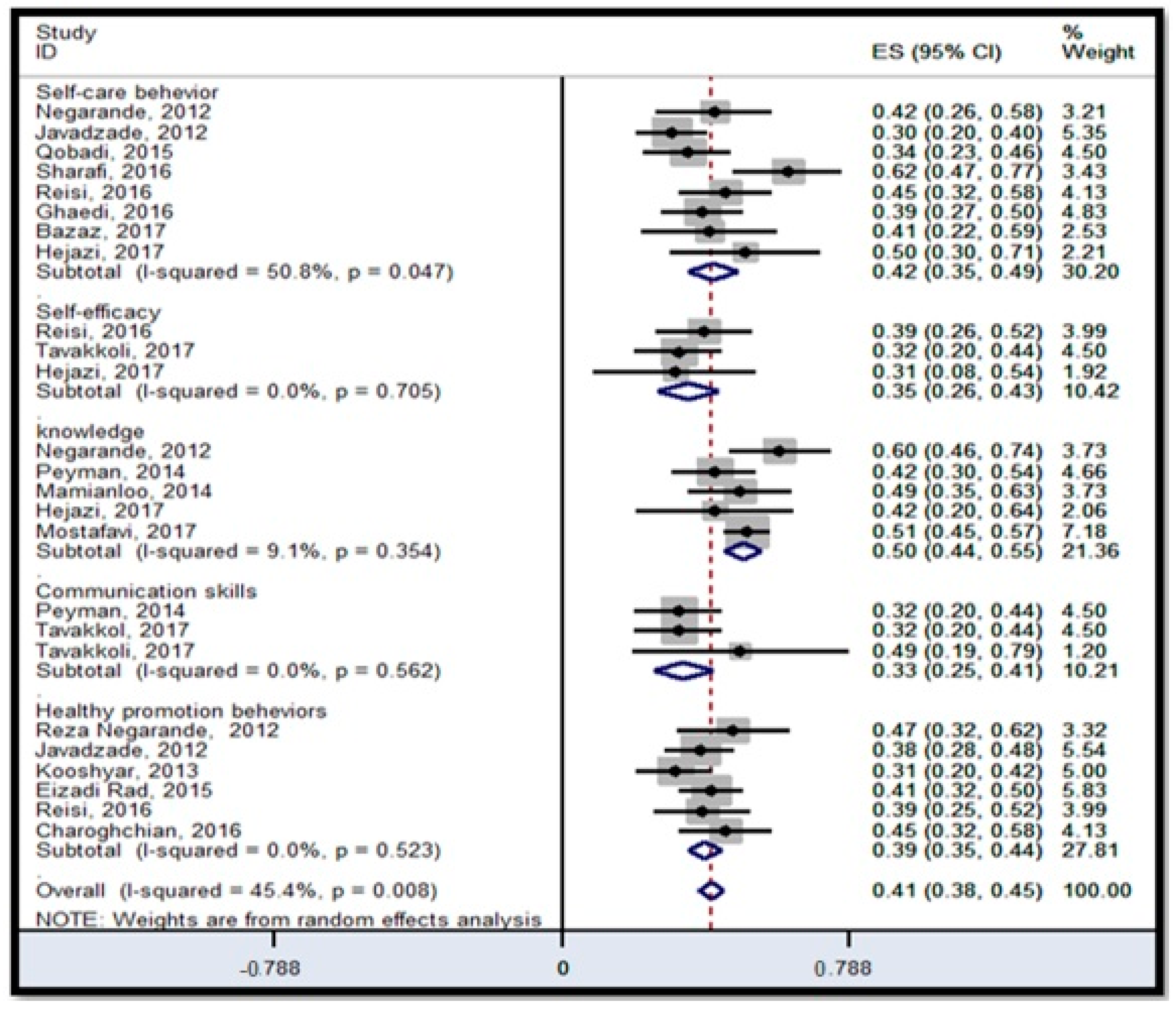
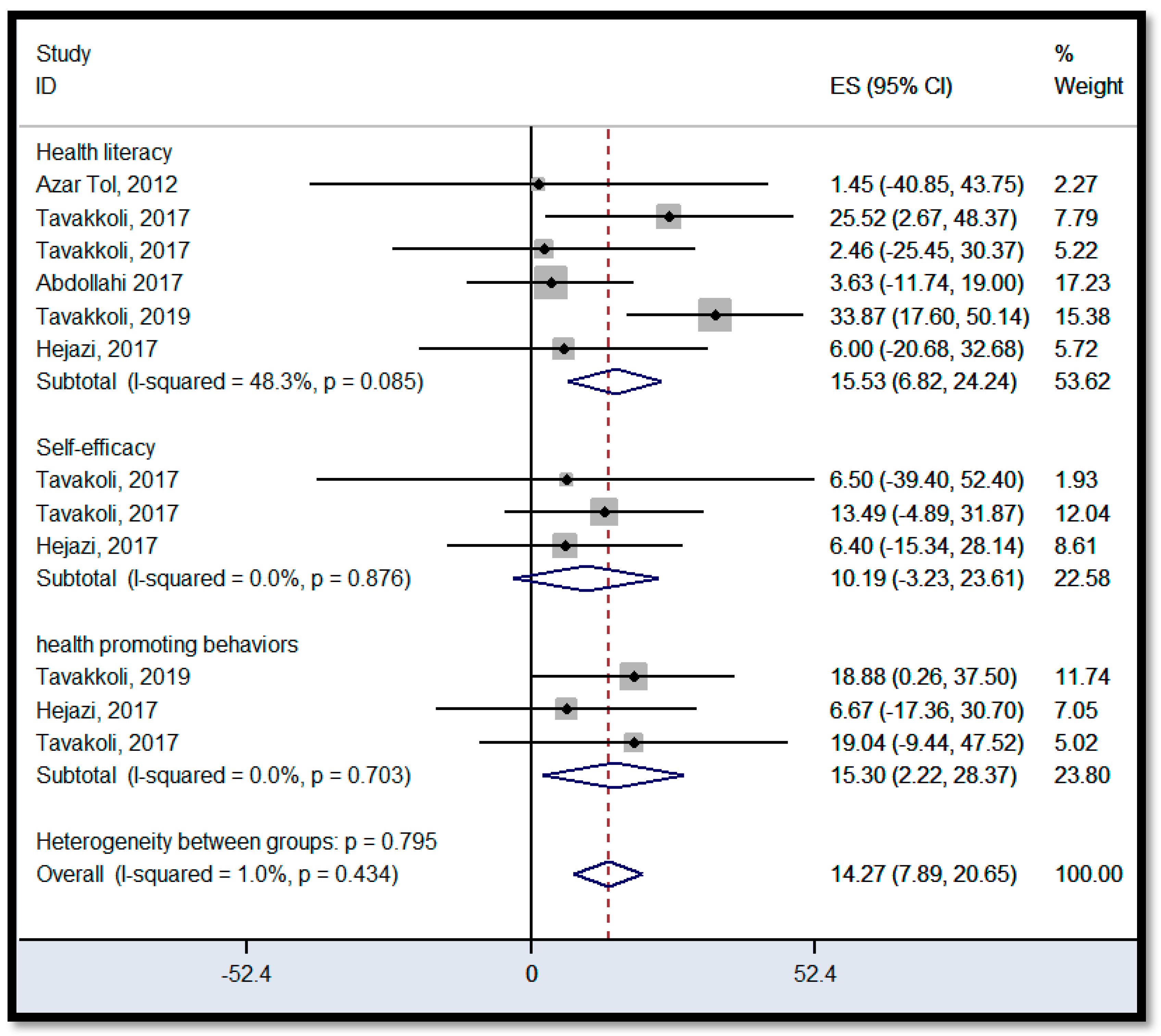
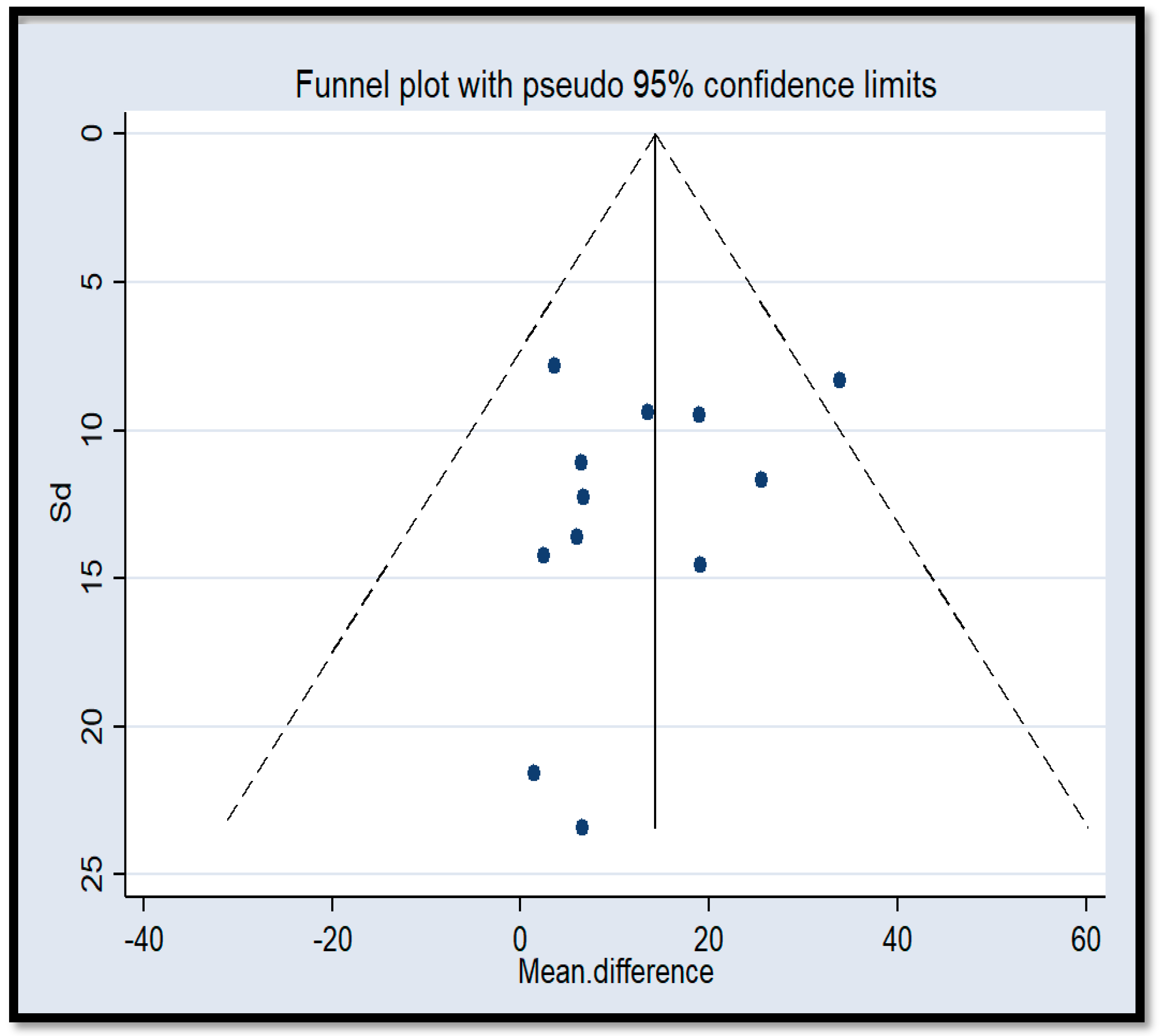
3.6.3. Intervention Outcome
4. Discussion
4.1. Health Literacy Status
4.2. Health Literacy Intervention
4.3. Challenge and Gaps
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Simonds, S.K. Health Education as Social Policy. Health Educ. Monogr. 1974, 2, 1–10. [Google Scholar] [CrossRef]
- Khorasani, E.C.; Sany, S.B.T.; Tehrani, H.; Doosti, H.; Peyman, N. Review of Organizational Health Literacy Practice at Health Care Centers: Outcomes, Barriers and Facilitators. Int. J. Environ. Res. Public Health 2020, 17, 7544. [Google Scholar] [CrossRef]
- Sørensen, K.; Trezona, A.; Levin-Zamir, D.; Kosir, U.; Nutbeam, D.; World Health Organization. Transforming health systems and societies by investing in health literacy policy and strategy. Public Health Panor. 2019, 5, 259–263. [Google Scholar]
- Nutbeam, D. The evolving concept of health literacy. Soc. Sci. Med. 2008, 67, 2072–2078. [Google Scholar] [CrossRef]
- Miller, T.A. Health literacy and adherence to medical treatment in chronic and acute illness: A meta-analysis. Patient Educ. Couns. 2016, 99, 1079–1086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bröder, J.; Okan, O.; Bauer, U.; Bruland, D.; Schlupp, S.; Bollweg, T.M.; Saboga-Nunes, L.; Bond, E.; Sørensen, K.; Bitzer, E.-M.; et al. Health literacy in childhood and youth: A systematic review of definitions and models. BMC Public Health 2017, 17, 361. [Google Scholar] [CrossRef]
- Durand, M.-A.; Carpenter, L.; Dolan, H.; Bravo, P.; Mann, M.; Bunn, F.; Elwyn, G. Do Interventions Designed to Support Shared Decision-Making Reduce Health Inequalities? A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e094670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Tehrani Banihashemi, A.; Amirkhani, M.; Haghdust, A.; Alavian, M.; Asgharifard, H.; Baradaran, H.; Barghmdi, M.; Parsinia, S.; Fathi Ranjbar, S. Health literacy in five provinces of the country and its influencing factors. Strides Dev. Med Educ. 2007, 1, 1–9. [Google Scholar]
- Nekoei, M.M. Health literacy and utilization of health services in Kerman urban area. Tolooebehdasht 2013, 11, 123–134. [Google Scholar]
- Sharifirad, G.; Mostafavi, F.; Hasanzade, A.; Javadzade, S.H.; Radjati, F.; Reisi, M. Relationship between health literacy, health status, and healthy behaviors among older adults in Isfahan, Iran. J. Educ. Health Promot. 2012, 1, 31. [Google Scholar] [CrossRef] [PubMed]
- Keyvanara, M.; Karimi, S.; Khorasani, E.; Jazi, M.J. Experts’ perceptions of the concept of induced demand in healthcare: A qualitative study in Isfahan, Iran. J. Educ. Health Promot. 2014, 3, 3. [Google Scholar]
- Nekoei-Moghadam, M.; Amiresmaili, M. Hospital services quality assessment: Hospitals of Kerman University of Medical Sciences, as a tangible example of a developing country. Int. J. Health Care Qual. Assur. 2011, 24, 57–66. [Google Scholar] [CrossRef]
- Alizadeh, S.; Alizadeh, S.; Mohseni, M.; Khanjani, N.; Momenabadi, V. Correlation between social participation of women and their quality of life in Kerman. J. Health Promot. Manag. 2014, 3, 34–42. [Google Scholar]
- Azimi, F.; Naddafi, K.; Nabizadeh, R.; Hassanvand, M.S.; Alimohammadi, M.; Afhami, S.; Musavi, S.N. Fungal air quality in hospital rooms: A case study in Tehran, Iran. J. Environ. Health Sci. Eng. 2013, 11, 30. [Google Scholar] [CrossRef] [Green Version]
- Javadzade, H.S.G. Health literacy among adults of Isfahan, Iran. Health Syst. Res. 2013, 9, 540–549. [Google Scholar]
- Karimi, P.; Islami, F.; Anandasabapathy, S.; Freedman, N.D.; Kamangar, F. Gastric Cancer: Descriptive Epidemiology, Risk Factors, Screening, and Prevention. Cancer Epidemiol. Biomark. Prev. 2014, 23, 700–713. [Google Scholar] [CrossRef] [Green Version]
- Sajjadi, H.; Hosseinpour, N.; Sharifian Sani, M.; Mahmoodi, Z. Association between health literacy and life style in married rural women in Izeh, Iran. J. Health 2016, 7, 479–489. [Google Scholar]
- Peyman, N.; Samiee Roudi, K. Investigating the status of health literacy among health providers of rural area. J. Health Lit. 2016, 1, 46–52. [Google Scholar]
- Charoghchian Khorasani, E.; Peyman, N.; Esmaily, H. Relations between breastfeeding self-efficacy and maternal health literacy among pregnant women. Evid. Based Care 2017, 6, 18–25. [Google Scholar]
- Baghaei, R.; Najarzadeh, M.; Saei, M.; Mohamadi, N. Functional health literacy in pregnant women in health centers of Urmia city-2015. J. Urmia Nurs. Midwifery Fac. 2017, 15, 368–375. [Google Scholar]
- Ansari, H.; Almasi, Z.; Ansari-Moghaddam, A.; Mohammadi, M.; Peyvand, M.; Hajmohammadi, M.; Bagheri, F. Health Literacy in Older Adults and Its Related Factors: A Cross-Sectional Study in Southeast Iran. Health Scope 2016, 5, e37453. [Google Scholar] [CrossRef]
- Safari Moradabadi, A.; Aghamolaei, T.; Ramezankhani, A.; Dadipoor, S. The health literacy of pregnant women in Bandar Abbas, Iran. Sci. J. Sch. Public Health Inst. Public Health Res. 2017, 10, 123–131. [Google Scholar]
- Peyman, N.; Abdollahi, M. The relationship between health literacy and self-efficacy physical activity in postpartum women. J. Health Lit. 2016, 1, 5–12. [Google Scholar]
- Abdollahi, M.; Peyman, N. The Effect of an Educational Program based on Health Literacy Strategies on Physical Activity in Postpartum Women. J. Midwifery Reprod. Health 2017, 5, 1059–1065. [Google Scholar]
- Izadirad, H.; Zareban, I. The Relationship of Health Literacy with Health Status, Preventive Behaviors and Health Services Utilization in Baluchistan, Iran. J. Educ. Community Health 2015, 2, 43–50. [Google Scholar] [CrossRef] [Green Version]
- Khosravi, A.; Ahmadzadeh, K.H. Investigating health literacy Level of patients referred to Bushehr hospitals and recognizing its effective factors. Iran South Med. J. 2016, 18, 1245–1253. [Google Scholar]
- Zareban, I.; Izadirad, H. Evaluation of health literacy, health status and health services utilization in women in Baluchistan region of Iran. J. Health Lit. 2016, 1, 71–82. [Google Scholar]
- SheikhSharafi, H.; Seyedamini, B. Assessment of health literacy and self-care in heart failure patients. J. Health Lit. 2017, 1, 203–219. [Google Scholar]
- Sahrayi, M.; Panahi, R.; Kazemi, S.S.; GoliRostami, Z.; Rezaie, H.; Jorvand, R. The study of Health Literacy of adults in Karaj. J. Health Lit. 2017, 1, 230–238. [Google Scholar]
- Afshari, M.A.; Teimori, G.H.; Kohnavard, B.; Pour, H.E.; Kangavari, M. Health literacy of workers in the auto parts industry: A cross-sectional study. J. Iran. Job Health 2017, 14, 147–155. [Google Scholar]
- Naghibi, A.; Chaleshgar, M.; Kazemi, A.; Hosseini, M. Evaluation of health literacy level among 18–65 year-old adults in Shahriar, Iran. J. Health Res. Community 2017, 3, 17–25. [Google Scholar]
- Kaboudi, M.; Kianipour, N.; Ziapour, A.; Dehghan, F. A study of health literacy components and their relationships with health-promoting behaviors in students at Kermanshah University of Medical Sciences. Int. J. Pediatrics 2017, 5, 6721–6729. [Google Scholar]
- Kilfoyle, K.A.; Vitko, M.; O’Conor, R.; Bailey, S.C. Health literacy and Women’s reproductive health: A systematic review. J. Women’s Health 2016, 25, 1237–1255. [Google Scholar] [CrossRef]
- Corrarino, J.E. Health literacy and women’s health: Challenges and opportunities. J. Midwifery Women’s Health 2013, 58, 257–264. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Munn, Z.; Moola, S.; Riitano, D.; Lisy, K. The development of a critical appraisal tool for use in systematic reviews addressing questions of prevalence. Int. J. Health Policy Manag. 2014, 3, 123–128. [Google Scholar] [CrossRef] [Green Version]
- Hedges, L.V. Distribution theory for Glass’s estimator of effect size and related estimators. J. Educ. Stat. 1981, 6, 107–128. [Google Scholar] [CrossRef]
- Mahmoodi, H.; Negarandeh, R.; Javaheri, M.; Sharifi, P.; Ghanei, R.; AminPour, A.; Akbari, A.; Kazemi, E.; Mohammadi, Y. Examining the relation of health literacy with outcomes of diabetes among type 2 diabetes patients in Saqez, western Iran, 2011. J. Urmia Nurs. Midwifery Fac. 2014, 12, 56–62. [Google Scholar]
- Negarandeh, R.; Mahmoodi, H.; Noktehdan, H.; Heshmat, R.; Shakibazadeh, E. Teach back and pictorial image educational strategies on knowledge about diabetes and medication/dietary adherence among low health literate patients with type 2 diabetes. Prim. Care Diabetes 2013, 7, 111–118. [Google Scholar] [CrossRef]
- Tol, A.; Pourreza, A.; Foroshani, R.; Tavassoli, E. Assessing the effect of educational program based on small group on promoting knowledge and health literacy among women with type2 diabetes referring to selected hospitals affiliated to Tehran University of Medical Sciences. Razi J. Med. Sci. 2013, 19, 104. [Google Scholar]
- Mamianloo, H.; Tol, A.; Khatibi, N.; Amadi, K.S.; Mohebbi, B. Assessing the effect of small group intervention program on knowledge and health literacy among patients with heart failure. J. Nurs. Educ. 2014, 3, 34–41. [Google Scholar]
- Rahmanian, M.; Ghaffari Targhi, M. A survey on health literacy of referred diabetic patients to Yazd diabetes research center. Tolooebehdasht 2016, 15, 176–186. [Google Scholar]
- Peyman, N.; Behzad, F.; Taghipour, A.; Esmaily, H. Evaluation of communication between healthcare workers and patients with chronic diseases according to their levels of health literacy. J. Res. Health 2014, 4, 599–607. [Google Scholar]
- Miri, A.; Ghanbari, M.A.; Najafi, A. The relationship between health literacy and the recovery rate of cardiovascular patients after bypass surgery. J. Health Lit. 2016, 1, 83–91. [Google Scholar]
- Khorasani, E.C.; Peyman, N.; Sahebkar, M.; Moghzi, M. Investigating health literacy in patients with type2 diabets referring to the health houses of Chenaran in 2016. J. North Khorasan Univ. Med. Sci. 2017, 9, 183–191. [Google Scholar] [CrossRef]
- Reisi, M.; Mostafavi, F.; Javadzade, H.; Mahaki, B.; Tavassoli, E.; Sharifirad, G. Impact of Health Literacy, Self-efficacy, and Outcome Expectations on Adherence to Self-care Behaviors in Iranians with Type 2 Diabetes. Oman Med. J. 2016, 31, 52–59. [Google Scholar] [CrossRef]
- Malekzadeh, S.; Azami, M.; Mirzaei, M.; Motamedi, F. Comparative Investigation of Health Literacy Level of Cardiovascular Patients Hospitalized in Private and Educational Hospitals of Kerman City, Iran. Acta Inform. Med. 2016, 24, 56–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sany, S.B.T.; Peyman, N.; Behzhad, F.; Esmaeily, H.; Taghipoor, A.; Ferns, G. Health providers’ communication skills training affects hypertension outcomes. Med. Teach. 2017, 40, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Hejazi, S.; Peyman, N.; Tajfard, M.; Esmaily, H. The Impact of Education Based on Self-efficacy Theory on Health Literacy, Self-efficacy and Self-care Behaviors in Patients with Type 2 Diabetes. Nian J. Health Educ. Health Promot. 2018, 5, 296–303. [Google Scholar] [CrossRef]
- Masoompour, M.; Tirgari, B.; Ghazanfari, Z. The Relationship between Health Literacy, Self-Efficacy, and Self-Care Behaviors in Diabetic Patients. Evid. Based Care 2017, 7, 17–25. [Google Scholar]
- Khosravi, A.; Ahmadzadeh, K.; Zareivenovel, M. Evaluating the health literacy level among diabetic patients referring to Shiraz health centers. Int. J. Inf. Sci. Manag. 2018, 16, 31–42. [Google Scholar]
- Mollakhalili, H.; Papi, A.; Zare-Farashbandi, F.; Sharifirad, G.; HasanZadeh, A. A survey on health literacy of inpatient’s educational hospitals of Isfahan University of Medical Sciences in 2012. J. Educ. Health Promot. 2014, 4, 3–18. [Google Scholar]
- Qobadi, M.; Besharat, M.A.; Rostami, R.; Rahiminezhad, A.; Pourgholami, M. Health literacy, negative emotional status, and self-care behaviors in dialysis. J. Fundam. Ment. Health 2014, 17, 46–51. [Google Scholar]
- Darvishpour, J.; Omidi, S.; Farmanbar, R. The Relationship between Health Literacy and Hypertension Treatment Control and Follow-up. Casp. J. Health Res. 2016, 2, 1–8. [Google Scholar] [CrossRef]
- Rafiezadeh, G.S.; Tabarsy, B.; Hassanjani, S.; Razavi, M.; Amjady, M.; Hojjati, H. Relationship between the Health Literacy with Selfefficacy of the Diabetic Patient’s Type 2 Referred to Gorgan City Clinic in 2014. J. Diabetes. Nurs. 2015, 3, 31–42. [Google Scholar]
- Haghighi, S.T.; Lamyian, M.; Granpaye, L. Assessment of the level of health literacy among fertile Iranian women with breast cancer. Electron. Physician 2015, 7, 1359–1364. [Google Scholar]
- Ghaedi, M.; Banihashemi, F.; Latifi, M.; Soleymaninejad, M. The relationship between health literacy and self-care among patients with type 2 diabetes residing in the city of Bastak. Iran. J. Endocrinol. Metab. 2016, 18, 90–96. [Google Scholar]
- Naimi, A.J.; Naderiravesh, N.; Bayat, Z.S.; Shakeri, N.; Matbouei, M. Correlation between health literacy and health-related quality of life in patients with hypertension, in Tehran, Iran, 2015–2016. Electron. Physician 2017, 9, 5712–5720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sany, S.B.T.; Peyman, N.; Zadehahmad, Z.; Ferns, G.; Doosti, H. Effect of educational interventions on health literacy in patients with heart failure. Int. J. Health Promot. Educ. 2018, 57, 23–36. [Google Scholar] [CrossRef]
- Peyman, N.; Alipour Anbarani, M. The effect of training diabetes prevention behaviors on promotion of knowledge, attitude and practice of students for prevention of diabetes in Mashhad city. Int. J. Pediatrics 2015, 3, 501–507. [Google Scholar]
- Mohseni, M.; Khanjani, N.; Iranpour, A.; Tabe, R.; Borhaninejad, V.R. The relationship between health literacy and health status among elderly people in Kerman. Iran. J. Ageing 2015, 10, 146–155. [Google Scholar]
- Jafari, Y.; Vahedian-Shahroodi, M.; Tehrani, H.; Haresabadi, M.; Shariati, M. The relationship between caregivers’ health literacy and the behavior of women with multiple sclerosis. Iran. J. Obstet. Gynecol. Infertil. 2018, 21, 64–71. [Google Scholar]
- Diviani, N.; Putte, B.V.D.; Giani, S.; Van Weert, J.C. Low Health Literacy and Evaluation of Online Health Information: A Systematic Review of the Literature. J. Med. Internet Res. 2015, 17, e112. [Google Scholar] [CrossRef] [Green Version]
- Parker, R. Health literacy: A challenge for American patients and their health care providers. Health Promot. Int. 2000, 15, 277–283. [Google Scholar] [CrossRef] [Green Version]
- Cutilli, C.C.; Bennett, I.M. Understanding the Health Literacy of America Results of the National Assessment of Adult Literacy. Orthop. Nurs. Natl. Assoc. Orthop. Nurses 2009, 28, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Walker, J.; Pepa, C.; Gerard, P.S. Assessing the Health Literacy Levels of Patients Using Selected Hospital Services. Clin. Nurse Spéc. 2010, 24, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Shieh, C.; Halstead, J.A. Understanding the impact of health literacy on women’s health. J. Obstet. Gynecol. Neonatal Nurs. 2009, 38, 601–612. [Google Scholar] [CrossRef]
- Nutbeam, D. Building health literacy in Australia. Med. J. Aust. 2009, 191, 525–526. [Google Scholar] [CrossRef]
- Crengle, S.; Luke, J.N.; Lambert, M.; Smylie, J.K.; Reid, S.; Harré-Hindmarsh, J.; Kelaher, M. Effect of a health literacy intervention trial on knowledge about cardiovascular disease medications among Indigenous peoples in Australia, Canada and New Zealand. BMJ Open 2018, 8, e018569. [Google Scholar] [CrossRef] [Green Version]
- Siuki, H.A.; Peyman, N.; Vahedian-Shahroodi, M.; Gholian-Aval, M.; Tehrani, H. Health Education Intervention on HIV/AIDS Prevention Behaviors among Health Volunteers in Healthcare Centers: An Applying the Theory of Planned Behavior. J. Soc. Serv. Res. 2019, 45, 582–588. [Google Scholar] [CrossRef]
- Ghoreishi, M.-S.; Vahedian-Shahroodi, M.; Jafari, A.; Tehranid, H. Self-care behaviors in patients with type 2 diabetes: Education intervention base on social cognitive theory. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2049–2056. [Google Scholar] [CrossRef] [PubMed]
- Poustchi, H.; Eghtesad, S.; Kamangar, F.; Etemadi, A.; Keshtkar, A.-A.; Hekmatdoost, A.; Mohammad, H.S.; Mahmoudi, Z.; Shayanrad, A.; Roozafzai, F.; et al. Prospective Epidemiological Research Studies in Iran (the PERSIAN Cohort Study): Rationale, Objectives, and Design. Am. J. Epidemiol. 2018, 187, 647–655. [Google Scholar] [CrossRef]
- Moradi-Lakeh, M.; Vosoogh-Moghaddam, A. Health Sector Evolution Plan in Iran; Equity and Sustainability Concerns. Int. J. Health Policy Manag. 2015, 4, 637–640. [Google Scholar] [CrossRef] [Green Version]
- Shojaei, S.; Yousefi, M.; Ebrahimipour, H.; Valinejadi, A.; Tabesh, H.; Fazaeli, S. Catastrophic health expenditures and impoverishment in the households receiving expensive interventions before and after health sector evolution plan in Iran: Evidence from a big hospital. Koomesh 2018, 14, 283–290. [Google Scholar]
- Rezaei, S.; Hajizadeh, M.; Bazyar, M.; Karyani, A.K.; Jahani, B.; Matin, B.K. The impact of Health Sector Evolution Plan on the performance of hospitals in Iran: Evidence from the Pabon Lasso model. Int. J. Health Gov. 2018, 23, 111–119. [Google Scholar] [CrossRef]
- LeDoux, J.; Mann, C. Addressing Limitations in Health Literacy: Greater Understanding Promotes Autonomy and Self-Determination. Prof. Case Manag. 2019, 24, 219–221. [Google Scholar] [CrossRef]
- Kobayashi, L.C.; Wardle, J.; Wolf, M.S.; Von Wagner, C. Aging and Functional Health Literacy: A Systematic Review and Meta-Analysis. J. Gerontol. Ser. B 2016, 71, 445–457. [Google Scholar] [CrossRef]
- Marques, S.R.; Lemos, S.M. Health literacy assessment instruments: Literature review. Audiol. Commun. Res. 2017, 22, e1757. [Google Scholar]
- Mantwill, S.; Monestel-Umaña, S.; Schulz, P.J. The Relationship between Health Literacy and Health Disparities: A Systematic Review. PLoS ONE 2015, 10, e0145455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrara, A.; Schulz, P.J. The role of health literacy in predicting adherence to nutritional recommendations: A systematic review. Patient Educ. Couns. 2018, 101, 16–24. [Google Scholar] [CrossRef]
- Montazeri, A.; Tavousi, M.; Rakhshani, F.; Azin, S.A.; Jahangiri, K.; Ebadi, M.; Naderimagham, S.; Solimanian, A.; Sarbandi, F.; Motamedi, A.; et al. Health Literacy for Iranian Adults (HELIA): Development and psychometric properties. Payesh 2014, 2, 112–129. [Google Scholar]
- Tavakolikia, N.; Kheiltash, A.; Shojaeefar, E.; Montazeri, A.; Shariati, M.; Meysamie, A. The most well-known health literacy questionnaires: A narrative review. Soc. Determ. Health 2017, 3, 104–113. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors (Year) | Tool | City | Study Design | N | Participants | Mean H | HL Scores (%) |
|---|---|---|---|---|---|---|---|
| Mahmodi, 2012 [41] | TOFHLA | Saqqez | Cross-sectional | 1563 | Diabetic patient, 65% illiterate, 35% diploma or higher | 27.19± 19.62 | Ad: 6.2, M: 14.8, In: 79 |
| Negarande, 2012 [42] | TOFHLA | Tehran | RCT | 127 | Diabetic patient, 95% under diploma | 35.11 ± 10.14 | |
| Azar Tol, 2012 [43] | TOFHLA | Tehran | RCT | 160 | Diabetic patient, 98.1% married, 65% >diploma, 67.7% moderate or higher income | 39.81 ± 16.54 | |
| Mamianloo, 2014 [44] | NVS | Tehran | Semi-experimental | 150 | Heart failure patient, 41% diploma/40% under diploma, 58% married | 1.77 ± 0.4 | |
| Mohammad, 2014 [63] | TOFHLA | Tehran, | Cross-sectional | 407 | Diabetic patient, 71% illiterate, 35% under diploma | 30.34 ± 8.9 | Ad: 18.2, M: 17.8, In: 70 |
| Reazee 2014 [45] | TOFHLA, | Yazd | Cross-sectional | 432 | Diabetic patient, 99.1% married, 85% moderate or high income, 69% under diploma, 7.4% live in village | 46.66 ± 1.4 | Ad: 22.2, M: 18.5, In: 59.3 |
| Peyman, 2014 [46] | TOFHLA | Mashhad | Cross-sectional | 240 | Hypertensive patient, 75% illiterate or under diploma, 80% low income | 63.3 ± 12.04 | Ad: 50.4, M: 37.9, In: 11.7 |
| Khosravi, 2015 [27] | TOFHLA | Bushehr | Cross-sectional | 250 | Heart failure patient, 75% diploma or under diploma, | 69.2 ± 14 | |
| Miri, 2015 [5] | TOFHLA | Mashhad | Cross-sectional | 75 | Cardiovascular disease, 82% illiterate or under diploma | 64.14 ± 7.19 | Ad: 14.66, M: 38.6, In: 38.67 |
| Charoghcheian, 2015 [48] | TOFHLA | Chenaran | Semi-experimental | 162 | Diabetic patient, 92% under diploma, 68% low income | 53.6 ± 24.03 | Ad: 11, M: 30.5, In: 68.5 |
| Reisi, 2016 [49] | TOFHLA | Isfahan | Cross-sectional | 187 | Diabetic patient, 57% under diploma, 95% married | 60 ± 11, | |
| Malekzadeh, 2016 [50] | TOFHLA | Kerman | Cross-sectional | 200 | Cardiovascular disease, 68% diploma or under diploma, low or moderate income, 98% Married | 61.12± 10.3 | Ad: 29, M: 22, In: 49 |
| Seyedoshohadaee, 2016 [30] | TOFHLA | Tehran | Cross-sectional | 200 | Diabetic patient, 90% married, 92% low or moderate income, 69 diploma or under diploma | 71.09± 14.01 | Ad: 42, M: 24, In: 24 |
| Tavakkoli, 2017 [51] | TOFHLA | Mashhad | RCT, 2 interventions | 240 | Hypertensive patient, 82% Married, 80% under diploma, 79% low income. Two health providers | 63 ± 15 | Ad: 32, M: 28, In: 40 |
| Hejazi, 2017 [52] | TOFHLA | Mashhad | Semi-experimental | 70 | Diabetic patient, 77% diploma or under diploma, 92% low or middle income | 75.3 ± 10.7 | Ad: 37, M: 35, In: 28 |
| Mostafavi, 2017 [29] | TOFHLA | Esfahan | Cross-sectional | 700 | Hypertensive patient, 91% married, 72% under diploma | 60 ± 25 | |
| Masoompour, 2017 [53] | TOFHLA | Kerman | Cross-sectional | 400 | Diabetic patient, 81% married, 84% illiterate or under diploma | 63.6 ± 14.35 | |
| Khosravi 2018 [54] | TOFHLA | Shiraz | Cross-sectional | 400 | Diabetic patient, 75% diploma or under diploma | 65 ± 18, 17–99 | Ad: 41.4, M: 23.6, In: 35 |
| Mollakhalili, 2014 [55] | TOFHLA | Isfahan | Cross-sectional | 384 | Inpatient, 59% diploma or under diploma, 96% low or middle income, 62% married | 63.29± 2.3 | Ad: 33.9, M: 25, In: 41 |
| Kooshyar, 2013 [55] | STOFHLA | Mashhad | Cross-sectional | 300 | Hypertensive patient, 62% diploma or under diploma, 82% married | 32.45± 12.3 | Ad: 15, M: 14, In: 71 |
| Qobadi, 2015 [56] | STOFHLA | Tehran | Cross-sectional | 240 | Dialysis Patient, 59% diploma or under diploma, 71% married | 60.54 ± 10.34 | Ad: 65.2, M: 9.8, In:25 |
| Darvishpour, 2016 [57] | STOFHLA | Rasht | Cross-sectional | 257 | Hypertensive patient, 69% diploma or under diploma | 68.7 ± 16.4 | Ad: 41.62, M: 30, In: 28.4 |
| Rfiehzadeh, 2015 [58] | HELIA | Gorgon | Cross-sectional | 100 | Diabetic patient, 54% diploma or under diploma, 89% married | 86.7± 21.9 | Limited: 79, In: 21 |
| Haghighi, 2015 [59] | HELIA | Tehran | Cross-sectional | 260 | Women with breast cancer, 74% diploma or under diploma | 80.32± 12 | In: 6.9, Ad: 38.3 Limited: 18.8, |
| Ghaedi, 2016 [60] | HELIA | Bastak | Cross-sectional | 265 | Diabetic patient, 80% married, 83% illiterate or under diploma | 90.41 ± 27.18 | In: 51.7, Ad: 48.3 |
| Johari Naimi, 2017 [61] | HELIA | Tehran | Cross-sectional | 400 | Hypertensive patient 73% diploma or under diploma, | 68.66 ± 13.56 | In: 7.8, limited: 55, Ad: 37.2 |
| Tehrani, 2007 [9] | TOFHLA | 5 Province | Cross-sectional | 1086 | 41% illiterate/under diploma, 31% diploma 57% married, 45% low/moderate income, 35% live in village | 42.7± 14.6 | Ad: 28, M: 15.3, In: 56.6 |
| Nekoei-Moghadam, 2011 [10] | TOFHLA | Kerman | Cross-sectional | 1000 | 37% diploma/30% under diploma, 97% low or moderate income | 74.4± 9.1 | Ad: 41.4, M: 53.8, In: 4.8 |
| Javadzade, 2012 [16] | TOFHLA | Esfahan | Cross-sectional | 354 | Elderly, 58% illiterate or under diploma/32% diploma, 77.7% narried, 86% low income | 29.07 ± 30 | Ad: 10.3, M: 23.7, In: 66 |
| Azimi, 2013 [15] | NVS | Tehran | Cross-sectional | 250 | University student, 100% higher diploma, 90% single, | 1.84 ± 1.36 | In: 44.8, limited: 44.4, Ad: 10.8 |
| Tavassoli, 2013 [62] | NVS | Esfahan | Cross-sectional | 525 | - | 2.4± 1.45 | In: 26.5, limited: 36.5, Ad: 38 |
| Karimi, 2014 [17] | TOFHLA | Esfahan | Cross-sectional | 300 | 41% under diploma/30% diploma, 82% married | 37.2 ± 10.1 | |
| Mohseni, 2014 [64] | TOFHLA | Kerman | Cross-sectional | 200 | Elderly, 87% illiterate/under diploma, 92% married | 35.6 ± 18.5 | Ad: 17, M: 31, In: 52.5 |
| Sajjadi, 2015 [18] | TOFHLA | Izeh | Cross-sectional | 240 | Adult women, 42% diploma/50% under diploma, 100% married | 64.04 ± 2.05 | Ad: 38.75, M: 37.91, In: 23.33 |
| Peyman, 2016 [19] | TOFHLA | Khaf | Cross-sectional | 43 | 55% under diploma/40% diploma | 52.34± 14.89 | |
| Charoghchian, 2016 [20] | TOFHLA | Mashhad | Cross-sectional | 185 | Pregnant women, 33% diploma/40% under diploma, 100% married, 79% low income | 69.26 ± 7.16 | Ad: 35.10, M: 39.80, In: 15.1 |
| Baghaei, 2016 [21] | TOFHLA | Orumiyeh | Cross-sectional | 400 | Pregnant women, 46% diploma /52% under diploma, 86% low income, 100% married | 66.04 ± 7.65 | Ad: 51, M: 25, In: 24 |
| Ansari, 2016 [22] | TOFHLA | Zahedan | Cross-sectional | 200 | Elderly, 33% diploma/40% under diploma, 87% married, 78% low/moderate income | 64.4 + 18.4 | Ad: 32.5, M: 29, In: 38.5 |
| Bazaz, 2017 [57] | TOFHLA | Ahvaz | Cross-sectional | 93 | Women population | 68.16 ± 10.26 | Ad: 46, M: 31.8, In: 22.2 |
| Safari, 2017 [23] | TOFHLA | Bandar Abbas | Cross-sectional | 250 | Pregnant women, 24% diploma/32% under diploma, 100% married | 70.66 ± 17.26 | Ad: 52, M: 20.8, In: 27.2 |
| Peyman, 2016 [24] | STOFHLA | Mashhad | Cross-sectional | 120 | Postpartum women, 26.2% diploma/40% under diploma, 60% low income, 100% married | 51.3 ± 12.3 | |
| Abdollahi, 2016 [25] | STOFHLA | Mashhad | Semi-experimental | 80 | Postpartum women, 80% diploma or higher, 60% low income, | 60.2 ± 2.11 | Ad: 25.3, M: 35.1, In: 39.6 |
| Haerian, 2018 | STOFHLA | Yazd | Cross-sectional | 224 | - | 73.33 ± 12.93 | |
| EizadiRad, 2015 [65] | HELIA | Baluchistan | Cross-sectional | 400 | 26% diploma/43% under diploma, 81% low/moderate income | 76.4 ± 21.4 | Ad: 32, limited: 34, In: 34 |
| Tavassoli, 2015 [26] | HELIA | Iran population | Cross-sectional | 20571 | - | 68.3± 15.16 | In: 12, limited: 32.4, Ad: 39.9, Ex: 15.8 |
| Zareban, 2016 [28] | HELIA | Zahedan | Cross-sectional | 247 | Women, 24% diploma/40% under diploma, 85% low middle income, 100% married | 88.9 ± 18.5 | In: 33.2, limited: 34, Ad: 32 |
| Sharafi, 2016 [29] | HELIA | Tehran | Cross-sectional | 105 | 64% illiterate or under diploma/30% diploma 49.5% married | 87.03 ± 19.1 | |
| Sahrayi, 2016 [30] | HELIA | Karaj | Cross-sectional | 525 | 32% diploma/30% under diploma, 53.5% married | 80.03 ± 29.1 | In: 24.2, limited: 23.4, Ad: 37.9, Ex: 14.5 |
| Afshari, 2016 [31] | HELIA | Tehran | Cross-sectional | 157 | 64% illiterate or under diploma/ 22% diploma, 100% low income | 45.32 ± 19.3 | In: 79, limited: 22.09, Ad: 20 |
| Naghibi, 2017 [32] | HELIA | Shahryar | Cross-sectional | 299 | 21.8% diploma/30.54% under diploma | 58.26± 22.1 | In: 36.5, limited: 23.1, Ad: 23.1, Ex: 14.4 |
| Kaboudi, 2017 [33] | HELIA | Kermanshah | Cross-sectional | 420 | University student, 100% higher diploma, 95% single | 40.04 ± 0.43 | |
| Tavakkoli, 2019 [62] | TOFHLA | Kashmar | Semi-experimental | 80 | HF Heart failure patient, 28% diploma or 43% under diploma, 95% married | 42.03 ± 5.37 | Ad: 12.4, In: 87.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tavakoly Sany, S.B.; Doosti, H.; Mahdizadeh, M.; Orooji, A.; Peyman, N. The Health Literacy Status and Its Role in Interventions in Iran: A Systematic and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 4260. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084260
Tavakoly Sany SB, Doosti H, Mahdizadeh M, Orooji A, Peyman N. The Health Literacy Status and Its Role in Interventions in Iran: A Systematic and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(8):4260. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084260
Chicago/Turabian StyleTavakoly Sany, Seyedeh Belin, Hassan Doosti, Mehrsadat Mahdizadeh, Arezoo Orooji, and Nooshin Peyman. 2021. "The Health Literacy Status and Its Role in Interventions in Iran: A Systematic and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 8: 4260. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084260