
Women’s Depressive Symptoms during the COVID-19 Pandemic: The Role of Pregnancy

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Instruments
2.3. Statistical Analysis
3. Results
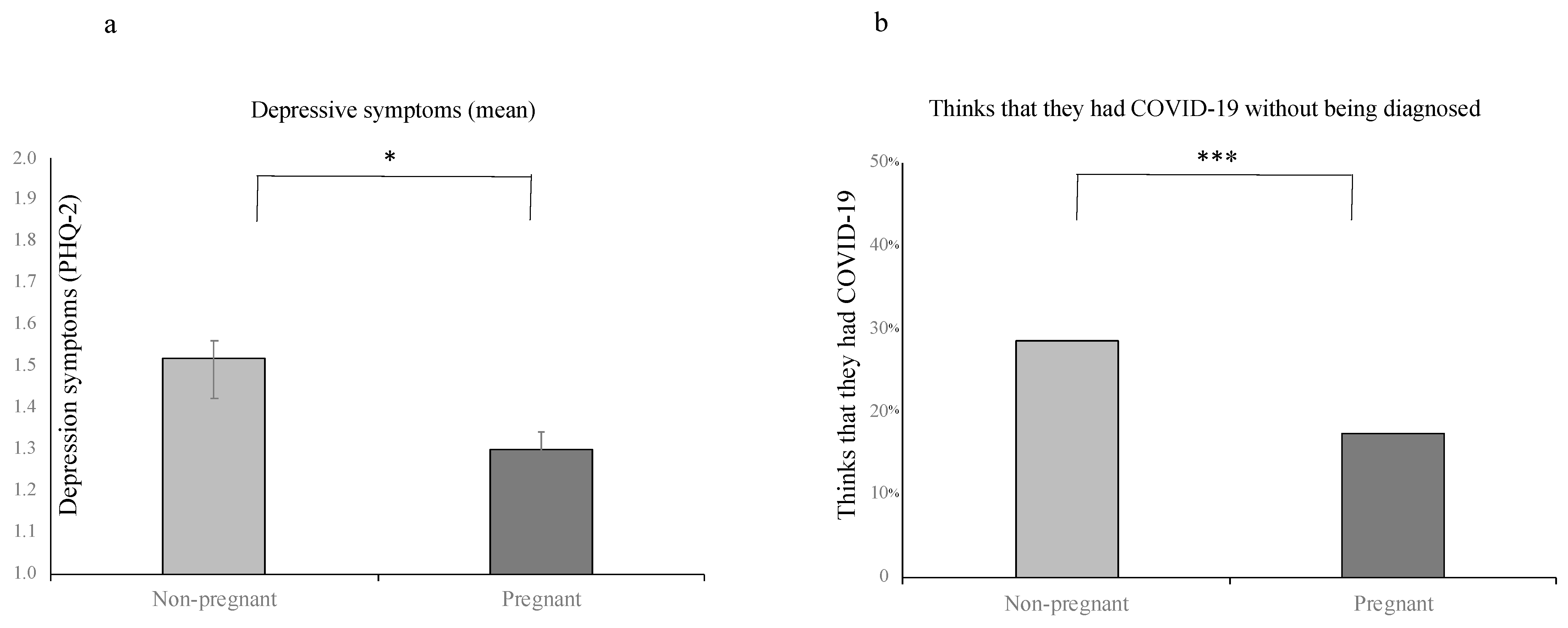
3.1. Group Differences between Pregnant and Non-Pregnant Women
3.2. Multivariate Correlates of Depressive Symptoms among Pregnant and Non-Pregnant Women
3.3. Multivariate Correlates of Depressive Symptoms among Pregnant Women
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020. [Google Scholar] [CrossRef] [PubMed]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Preis, H.; Mahaffey, B.; Heiselman, C.; Lobel, M. Vulnerability and resilience to pandemic-related stress among U.S. women pregnant at the start of the COVID-19 pandemic. Soc. Sci. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Harville, E.; Xiong, X.; Buekens, P. Disasters and Perinatal Health: A Systematic Review. Obstet. Gynecol. Surv. 2010, 65, 713–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Truijens, S.E.M.; Boerekamp, C.A.M.; Spek, V.; Van Son, M.J.M.; Oei, S.G.; Pop, V.J.M. Increased Levels of Depressive Symptoms among Pregnant Women in The Netherlands After the Crash of Flight MH17. Am. J. Epidemiol. 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goto, A.; Bromet, E.J.; Ota, M.; Ohtsuru, A.; Yasumura, S.; Fujimori, K. The Fukushima Nuclear Accident Affected Mothers’ Depression but Not Maternal Confidence. Asia Pac. J. Public Health 2017. [Google Scholar] [CrossRef] [Green Version]
- Brock, R.L.; O’Hara, M.W.; Hart, K.J.; McCabe-Beane, J.E.; Williamson, J.A.; Brunet, A.; Laplante, D.P.; Yu, C.; King, S. Peritraumatic Distress Mediates the Effect of Severity of Disaster Exposure on Perinatal Depression: The Iowa Flood Study. J. Trauma Stress 2015. [Google Scholar] [CrossRef] [Green Version]
- Nishigori, H.; Sugawara, J.; Obara, T.; Nishigori, T.; Sato, K.; Sugiyama, T.; Okamura, K.; Yaegashi, N. Surveys of postpartum depression in Miyagi, Japan, after the Great East Japan Earthquake. Arch. Womens Ment. Health 2014. [Google Scholar] [CrossRef] [Green Version]
- Harville, E.W.; Xiong, X.; Buekens, P.; Pridjian, G.; Elkind-Hirsch, K. Resilience after Hurricane Katrina among pregnant and postpartum women. Womens Health Issues 2011, 20, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Pomer, A.; Buffa, G.; Ayoub, M.-B.; Taleo, F.; Sizemore, J.H.; Tokon, A.; Chan, C.W.; Kaneko, A.; Obed, J.; Iaruel, J.; et al. Psychosocial distress among women following a natural disaster in a low- to middle-income country: “healthy mothers, healthy communities” study in Vanuatu. Arch. Womens Ment. Health 2019. [Google Scholar] [CrossRef] [PubMed]
- Berthelot, N.; Lemieux, R.; Garon-Bissonnette, J.; Drouin-Maziade, C.; Martel, É.; Maziade, M. Uptrend in distress and psychiatric symptomatology in pregnant women during the coronavirus disease 2019 pandemic. Acta Obstet. Gynecol. Scand. 2020, 99, 848–855. [Google Scholar] [CrossRef]
- Wu, Y.; Zhang, C.; Liu, H.; Duan, C.; Li, C.; Fan, J.; Li, H.; Chen, L.; Xu, H.; Li, X.; et al. Perinatal depressive and anxiety symptoms of pregnant women during the coronavirus disease 2019 outbreak in China. Am. J. Obstet. Gynecol. 2020, 21, 1–9. [Google Scholar] [CrossRef]
- Zanardo, V.; Manghina, V.; Giliberti, L.; Vettore, M.; Severino, L.; Straface, G. Psychological impact of COVID-19 quarantine measures in northeastern Italy on mothers in the immediate postpartum period. Int. J. Gynecol. Obstet. 2020. [Google Scholar] [CrossRef]
- Hessami, K.; Romanelli, C.; Chiurazzi, M.; Cozzolino, M. COVID-19 pandemic and maternal mental health: A systematic review and meta-analysis. J. Matern. Neonatal. Med. 2020, 1–8. [Google Scholar] [CrossRef]
- Racine, N.; Hetherington, E.; McArthur, B.A.; McDonald, S.; Edwards, S.; Tough, S.; Madigan, S. Maternal depressive and anxiety symptoms before and during the COVID-19 pandemic in Canada: A longitudinal analysis. Lancet Psychiatry 2021. [Google Scholar] [CrossRef]
- Zhou, Y.; Shi, H.; Liu, Z.; Peng, S.; Wang, R.; Qi, L.; Li, Z.; Yang, J.; Ren, Y.; Song, X.; et al. The prevalence of psychiatric symptoms of pregnant and non-pregnant women during the COVID-19 epidemic. Transl. Psychiatry 2020. [Google Scholar] [CrossRef]
- Hompson, K.A.; Bardone-Cone, A.M. 2019-nCOV distress and depressive, anxiety and OCD-type, and eating disorder symptoms among postpartum and control women. Arch. Women’s Ment. Health 2021, 1–10. [Google Scholar]
- Nelson, B. The positive effects of covid-19. BMJ 2020. [Google Scholar] [CrossRef] [PubMed]
- Denckla, C.A.; Mancini, A.D.; Consedine, N.S.; Milanovic, S.M.; Basu, A.; Seedat, S.; Spies, G.; Henderson, D.C.; Bonanno, G.A.; Koenen, K.C. Distinguishing postpartum and antepartum depressive trajectories in a large population-based cohort: The impact of exposure to adversity and offspring gender. Psychol. Med. 2018. [Google Scholar] [CrossRef] [Green Version]
- Lebel, C.; MacKinnon, A.; Bagshawe, M.; Tomfohr-Madsen, L.; Giesbrecht, G. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J. Affect. Disord. 2020. [Google Scholar] [CrossRef] [PubMed]
- Bloch, M.; Schmidt, P.J.; Danaceau, M.; Murphy, J.; Nieman, L.; Rubinow, D.R. Effects of Gonadal Steroids in Women with a History of Postpartum Depression. Am. J. Psychiatry 2000, 157, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Oates, M. Suicide: The leading cause of maternal death. Br. J. Psychiatry 2003, 183, 279–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Payne, J.L. Depression: Is pregnancy protective? J. Women’s Health 2012, 21, 809–810. [Google Scholar] [CrossRef]
- De Weerth, C.; Buitelaar, J.K. Physiological stress reactivity in human pregnancy—A review. Neurosci. Biobehav. Rev. 2005. [Google Scholar] [CrossRef] [PubMed]
- Christian, L.M. Physiological reactivity to psychological stress in human pregnancy: Current knowledge and future directions. Prog. Neurobiol. 2012. [Google Scholar] [CrossRef] [Green Version]
- Komesaroff, P.A.; Esler, M.D.; Sudhir, K. Estrogen Supplementation Attenuates Glucocorticoid and Catecholamine Responses to Mental Stress in Perimenopausal Women1. J. Clin. Endocrinol. Metab. 1999. [Google Scholar] [CrossRef] [Green Version]
- Herrera, A.Y.; Hodis, H.N.; Mack, W.J.; Mather, M. Estradiol Therapy After Menopause Mitigates Effects of Stress on Cortisol and Working Memory. J. Clin. Endocrinol. Metab. 2017. [Google Scholar] [CrossRef]
- Lobel, M.; Hamilton, J.G.; Cannella, D.T. Psychosocial Perspectives on Pregnancy: Prenatal Maternal Stress and Coping. Soc. Pers. Psychol. Compass 2008. [Google Scholar] [CrossRef]
- Ng, Q.X.; Venkatanarayanan, N.; Loke, W.; Yeo, W.-S.; Lim, D.Y.; Chan, H.W.; Sim, W.-S. A meta-analysis of the effectiveness of yoga-based interventions for maternal depression during pregnancy. Complement. Ther. Clin. Pr. 2019, 34, 8–12. [Google Scholar] [CrossRef]
- Yu, M.; Gong, W.; Taylor, B.; Cai, Y.; Xu, D.R. Coping Styles in Pregnancy, Their Demographic and Psychological Influences, and Their Association with Postpartum Depression: A Longitudinal Study of Women in China. Int. J. Environ. Res. Public Health 2020, 17, 3654. [Google Scholar] [CrossRef] [PubMed]
- López, D.M.L.; Hinojo, C.A.B.; Bernal, J.E.A.; Laiz, M.F.; Santiago, J.A.; Vilches, V.G.; Fernández, M.C.; Moral, A.B.; Perdigones, A.O.; Rodríguez, B.R.; et al. Resilience and psychological distress in pregnant women during quarantine due to the COVID-19 outbreak in Spain: A multicentre cross-sectional online survey. J. Psychosom. Obstet. Gynecol. 2021, 1–8. [Google Scholar] [CrossRef]
- Farewell, C.V.; Jewell, J.; Walls, J.; Leiferman, J.A. A Mixed-Methods Pilot Study of Perinatal Risk and Resilience During COVID-19. J. Prim. Care Community Health 2020. [Google Scholar] [CrossRef]
- Preis, H.; Mahaffey, B.; Heiselman, C.; Lobel, M. Pandemic-related pregnancy stress and anxiety among women pregnant during the COVID-19 pandemic. Am. J. Obstet. Gynecol. 2020, 2, 100155. [Google Scholar]
- Grigoriadis, S.; VonderPorten, E.H.; Mamisashvili, L.; Tomlinson, G.; Dennis, C.-L.; Koren, G.; Steiner, M.; Mousmanis, P.; Cheung, A.; Radford, K.; et al. The Impact of Maternal Depression during Pregnancy on Perinatal Outcomes. J. Clin. Psychiatry 2013. [Google Scholar] [CrossRef]
- Jarde, A.; Morais, M.; Kingston, D.; Giallo, R.; MacQueen, G.M.; Giglia, L.; Beyene, J.; Wang, Y.; McDonald, S.D. Neonatal Outcomes in Women with Untreated Antenatal Depression Compared With Women Without Depression. JAMA Psychiatry 2016. [Google Scholar] [CrossRef]
- Gentile, S. Untreated depression during pregnancy: Short- and long-term effects in offspring. A systematic review. Neuroscience 2017, 342, 154–166. [Google Scholar] [CrossRef] [PubMed]
- Talge, N.M.; Neal, C.; Glover, V. Antenatal maternal stress and long-term effects on child neurodevelopment: How and why? J. Child Psychol. Psychiatry 2007, 48, 245–261. [Google Scholar] [CrossRef] [PubMed]
- Lobel, M.; Cannella, D.L.; Graham, J.E.; DeVincent, C.; Schneider, J.; Meyer, B.A. Pregnancy-specific stress, prenatal health behaviors, and birth outcomes. Health Psychol. 2008, 27, 604–615. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, S.M.; Lobel, M. Conceptualization, measurement, and effects of pregnancy-specific stress: Review of research using the original and revised Prenatal Distress Questionnaire. J. Behav. Med. 2020, 43, 16–33. [Google Scholar] [CrossRef] [PubMed]
- Preis, H.; Mahaffey, B.; Pati, S.; Heiselman, C.; Lobel, M. Adverse Perinatal Outcomes Predicted by Prenatal Maternal Stress among U.S. Women at the COVID-19 Pandemic Onset. Ann. Behav. Med. 2021, 55, 179–191. [Google Scholar] [PubMed]
- Preis, H.; Mahaffey, B.; Lobel, M. Psychometric properties of the Pandemic-Related Pregnancy Stress Scale (PREPS). J. Psychosom. Obstet. Gynecol. 2020, 41, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The Patient Health Questionnaire-2: Validity of a two-item depression screener. Med. Care 2003, 41, 1284–1292. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W. Validation and utility of a self-report version of PRIME-MD: The PHQ Primary Care Study. J. Am. Med. Assoc. 1999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vlenterie, R.; Van Ras, H.W.; Roeleveld, N.; Pop-Purceleanu, M.; Van Gelder, M.M. Epidemiological evaluation of the Patient Health Questionnaire-2 in a pregnant population. J. Psychosom. Res. 2017. [Google Scholar] [CrossRef]
- Weitkamp, K.; Romer, G.; Rosenthal, S.; Wiegand-Grefe, S.; Daniels, J. German Screen for Child Anxiety Related Emotional Disorders (SCARED): Reliability, validity, and cross-informant agreement in a clinical sample. Child. Adolesc. Psychiatry Ment. Health 2010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilska, M.; Kołodziej-Zaleska, A.; Brandt-Salmeri, A.; Preis, H.; Lobel, M. Pandemic-related pregnancy stress assessment–Psychometric properties of the Polish PREPS and its relationship with childbirth fear. Midwifery 2021, 96, 102940. [Google Scholar] [CrossRef]
- Schaal, N.K.; La Marca-Ghaemmaghami, P.; Preis, H.; Mahaffey, B.; Lobel, M.; Castro, R.A. The German version of the pandemic-related pregnancy stress scale: A validation study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder. Arch. Intern. Med. 2006. [Google Scholar] [CrossRef] [Green Version]
- Zhong, Q.-Y.; Gelaye, B.; Zaslavsky, A.M.; Fann, J.R.; Rondon, M.B.; Sanchez, S.E.; Williams, M.A. Diagnostic Validity of the Generalized Anxiety Disorder—7 (GAD-7) among Pregnant Women. PLoS ONE 2015. [Google Scholar] [CrossRef]
- Gong, Y.; Zhou, H.; Zhang, Y.; Zhu, X.; Wang, X.; Shen, B.; Xian, J.; Ding, Y. Validation of the 7-item Generalized Anxiety Disorder scale (GAD-7) as a screening tool for anxiety among pregnant Chinese women. J. Affect. Disord. 2021, 282, 98–103. [Google Scholar] [CrossRef] [PubMed]
- IBM. IBM SPSS Statistics 23. Release Notes 2016. [Google Scholar] [CrossRef]
- Arbuckle, J.L. Amos; IBM SPSS.: Chicago, IL, USA, 2012. [Google Scholar]
- STATA. Stata: Software for Statistics and Data Science; STATA: College Station, TX, USA, 2020. [Google Scholar]
- Jann, B. KMATCH: Stata module for multivariate-distance and propensity-score matching, including entropy balancing, inverse probability weighting, (coarsened) exact matching, and regression adjustment. In Statistical Software Components; IDEAS: Nashville, TN, USA, 2017. [Google Scholar]
- Arrieta, J.; Aguerrebere, M.; Raviola, G.; Flores, H.; Elliott, P.; Espinosa, A.; Reyes, A.; Ortiz-Panozo, E.; Rodriguez-Gutierrez, E.G.; Mukherjee, J.; et al. Validity and Utility of the Patient Health Questionnaire (PHQ)-2 and PHQ-9 for Screening and Diagnosis of Depression in Rural Chiapas, Mexico: A Cross-Sectional Study. J. Clin. Psychol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sade, S.; Sheiner, E.; Wainstock, T.; Hermon, N.; Salem, S.Y.; Kosef, T.; Battat, T.L.; Oron, S.; Pariente, G. Risk for Depressive Symptoms among Hospitalized Women in High-Risk Pregnancy Units during the COVID-19 Pandemic. J. Clin. Med. 2020, 9, 2449. [Google Scholar] [CrossRef]
- O’Hara, M.W.; Swain, A.M. Rates and risk of postpartum depression—A meta-analysis. Int. Rev. Psychiatry 1996. [Google Scholar] [CrossRef]
- Milgrom, J.; Hirshler, Y.; Reece, J.; Holt, C.; Gemmill, A.W. Social Support-A Protective Factor for Depressed Perinatal Women? Int. J. Environ. Res. Public Health 2019, 16, 1426. [Google Scholar] [CrossRef] [Green Version]
- Stapleton, L.R.T.; Schetter, C.D.; Westling, E.; Rini, C.; Glynn, L.M.; Hobel, C.J.; Sandman, C.A. Perceived partner support in pregnancy predicts lower maternal and infant distress. J. Fam. Psychol. 2012. [Google Scholar] [CrossRef] [Green Version]
- Seguin, L.; Potvin, L.; St-Denis, M.; Loiselle, J. Chronic stressors, social support, and depression during pregnancy. Obstet. Gynecol. 1995. [Google Scholar] [CrossRef]
- Lee, D.T.; Sahota, D.; Leung, T.N.; Yip, A.S.; Lee, F.F.; Chung, T.K. Psychological responses of pregnant women to an infectious outbreak: A case-control study of the 2003 SARS outbreak in Hong Kong. J. Psychosom. Res. 2006. [Google Scholar] [CrossRef]
- Brik, M.; Sandonis, M.A.; Fernández, S.; Suy, A.; Parramon-Puig, G.; Maiz, N.; Dip, M.E.; Ramos-Quiroga, J.A.; Carreras, E. Psychological impact and social support in pregnant women during lockdown due to SARS-CoV2 pandemic: A cohort study. Acta Obstet. Gynecol. Scand. 2021. [Google Scholar] [CrossRef]
- Cooney, G.M.; Dwan, K.; Greig, C.A.; Lawlor, D.A.; Rimer, J.; Waugh, F.R.; McMurdo, M.; Mead, G.E. Exercise for depression (Review). Cochrane Libr. 2013. [Google Scholar] [CrossRef]
- Rebar, A.L.; Stanton, R.; Geard, D.; Short, C.; Duncan, M.J.; Vandelanotte, C. A meta-meta-analysis of the effect of physical activity on depression and anxiety in non-clinical adult populations. Health Psychol. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Ashdown-Franks, G.; Sabiston, C.M.; Stubbs, B. The evidence for physical activity in the management of major mental illnesses. Curr. Opin. Psychiatry 2019. [Google Scholar] [CrossRef]
- Davenport, M.H.; McCurdy, A.P.; Mottola, M.F.; Skow, R.J.; Meah, V.L.; Poitras, V.J.; Garcia, A.J.; Gray, E.C.; Barrowman, N.; Riske, L.; et al. Impact of prenatal exercise on both prenatal and postnatal anxiety and depressive symptoms: A systematic review and meta-analysis. Br. J. Sports Med. 2018. [Google Scholar] [CrossRef]
- Davenport, M.H.; Meyer, S.; Meah, V.L.; Strynadka, M.C.; Khurana, R. Moms Are Not OK: COVID-19 and Maternal Mental Health. Front. Glob. Womens Health 2020. [Google Scholar] [CrossRef]
- Niela-Vilén, H.; Auxier, J.; Ekholm, E.; Sarhaddi, F.; Mehrabadi, M.A.; Mahmoudzadeh, A.; Azimi, I.; Liljeberg, P.; Rahmani, A.M.; Axelin, A. Pregnant women’s daily patterns of well-being before and during the COVID-19 pandemic in Finland: Longitudinal monitoring through smartwatch technology. PLoS ONE 2021, 16, e0246494. [Google Scholar] [CrossRef] [PubMed]
- Labor branch—Ministry of Labor, Welfare and Social Services. Maternity Rights in Workplace. Available online: https://www.gov.il/he/Departments/Guides/workers-rights-during-maternity-leave (accessed on 17 August 2020).
- Labor branch—Ministry of Labor, Welfare and Social Services. Workplace Rights of Pregnant Women and Their Spouses. Available online: https://www.gov.il/he/departments/guides/labor-rights-during-pregnancy-and-birthwork (accessed on 17 August 2020).
- Thayer, Z.M.; Gildner, T.E. COVID-19-related financial stress associated with higher likelihood of depression among pregnant women living in the United States. Am. J. Hum. Biol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Biaggi, A.; Conroy, S.; Pawlby, S.; Pariante, C.M. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J. Affect. Disord. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, P.B.; Zambaldi, C.F.; Cantilino, A.; Sougey, E.B. Special features of high-risk pregnancies as factors in development of mental distress: A review. Trends Psychiatry Psychother. 2016, 38, 136–140. [Google Scholar] [CrossRef]
- Okagbue, H.I.; Adamu, P.I.; Bishop, S.A.; Oguntunde, P.E.; Opanuga, A.A.; Akhmetshin, E.M. Systematic Review of Prevalence of Antepartum Depression during the Trimesters of Pregnancy. Open Access Maced. J. Med Sci. 2019. [Google Scholar] [CrossRef] [Green Version]
- Perzow, S.E.; Hennessey, E.-M.P.; Hoffman, M.C.; Grote, N.K.; Davis, E.P.; Hankin, B.L. Mental health of pregnant and postpartum women in response to the COVID-19 pandemic. J. Affect. Disord. Rep. 2021, 4, 100123. [Google Scholar] [CrossRef]
- Prinds, C.; Hvidt, N.C.; Mogensen, O.; Buus, N. Making existential meaning in transition to motherhood—A scoping review. Midwifery 2014. [Google Scholar] [CrossRef]
- Ibrahim, S.M.; Nicoloro-SantaBarbara, J.; Auerbach, M.V.; Rosenthal, L.; Kocis, C.; Busso, C.E.; Lobel, M. Pregnancy-specific coping and changes in emotional distress from mid- to late pregnancy. J. Reprod. Infant Psychol. 2019. [Google Scholar] [CrossRef]
- Giurgescu, C.; Penckofer, S.; Maurer, M.C.; Bryant, F.B. Impact of Uncertainty, Social Support, and Prenatal Coping on the Psychological Well-being of High-risk Pregnant Women. Nurs. Res. 2006. [Google Scholar] [CrossRef]
- Ministry of Health. Israeli Ministry of Health Basket. 2021. Available online: https://www.health.gov.il/hozer/mk03_2018.pdf (accessed on 12 April 2021).
- Hooper, M.W.; Nápoles, A.M.; Pérez-Stable, E.J. COVID-19 and Racial/Ethnic Disparities. JAMA 2020, 323, 2466–2467. [Google Scholar] [CrossRef]
- Matthey, S.; Bilbao, F. A comparison of the PHQ-2 and MGMQ for screening for emotional health difficulties during pregnancy. J. Affect. Disord. 2018. [Google Scholar] [CrossRef]
- Löwe, B.; Kroenke, K.; Gräfe, K. Detecting and monitoring depression with a two-item questionnaire (PHQ-2). J. Psychosom. Res. 2005. [Google Scholar] [CrossRef]
- Ng, Q.X.; Lim, D.Y.; Chee, K.T. Not all trauma is the same. Proc. Natl. Acad. Sci. USA 2020, 117, 25200. [Google Scholar] [CrossRef]


{kind=link}
| Study Variables | Pregnant N = 1114 | Non-Pregnant N = 256 | χ2/t-Test (df), p | Effect Size | ||
|---|---|---|---|---|---|---|
| M/% | S.D. | M/% | S.D. | |||
| Sociodemographic variables | ||||||
| Age | 31.88 | 4.22 | 35.71 | 5.42 | t(1366) = 12.38, p < 0.001 | 0.79 |
| Years of Education | 16.10 | 2.62 | 16.59 | 3.42 | t(1368) = 2.15, p = 0.03 | 0.16 |
| Income (Below average) | 13.2% | 15.6% | X2(1) = 1.03, p = 0.31 | −0.93 | ||
| Relationship status (Married or cohabiting) | 96.5% | 85.9% | X2(1) = 44.87, p < 0.001 | 0.18 | ||
| Current employment status (working) | 85.7% | 85% | X2(1) = 0.07, p = 0.80 | −0.01 | ||
| Number of children under 18 | 1.00 | 1.15 | 1.93 | 1.16 | t(1368) = 11.60, p < 0.001 | 0.80 |
| COVID-19 related variables | ||||||
| Contact with someone diagnosed COVID-19 | 8.5% | 9.4% | X2(1) = 0.18, p = 0.67 | −0.01 | ||
| Think they had COVID-19 without being diagnosed | 17.4% | 28.5% | X2(1) = 16.23, p < 0.001 | −0.11 | ||
| Access to outdoor spaces (whenever) | 84.9% | 85.2% | X2(1) = 0.01, p = 0.91 | 0.003 | ||
| Psychological variables | ||||||
| Family/friends support (1–5) | 3.93 | 1.09 | 3.67 | 1.15 | t(1368) = −3.30, p = 0.001 | 0.23 |
| Partner support (1–5) | 4.48 | 0.78 | 4.21 | 0.89 | t(1329) = −4.19, p < 0.001 | 0.32 |
| Health behaviors (1–5) | 3.27 | 0.99 | 2.92 | 1.10 | t(1368) = −5.09, p < 0.001 | 0.33 |
| Stress (1–5) | 2.91 | 1.01 | 2.86 | 1.05 | t(1368) = −0.64, p = 0.52 | 0.05 |
| Anxiety (GAD-7) | 5.96 | 4.76 | 5.66 | 5.65 | t(1368) = −0.91, p = 0.36 | 0.06 |
| Depression (PHQ-2) | 1.30 | 1.41 | 1.52 | 1.56 | t(1368) = 2.06, p = 0.04 | 0.15 |
| Variables | Step 1 (β) | Step 2 (β) | Step 3 (β) |
|---|---|---|---|
| Step 1: Sociodemographic variables | |||
| Being pregnant | −0.08 * | −0.07 * | −0.06 * |
| Age | −0.03 | −0.02 | −0.03 |
| Years of Education | −0.05 | −0.05 | −0.04 |
| Income (Below average) | 0.16 *** | 0.13 *** | 0.11 ** |
| Relationship status (Married or cohabiting) | 0.06 | 0.06 | 0.05 |
| Current employment status (working) | 0.11 ** | 0.11 ** | 0.10 ** |
| Number of children under 18 | −0.02 | −0.02 | −0.09 * |
| Step 2: COVID-19 related variables | |||
| Contact with someone diagnosed COVID-19 | −0.02 | −0.01 | |
| Think they had COVID-19 without being diagnosed | 0.10 ** | 0.10 ** | |
| Access to outdoor space (whenever) | 0.06 | 0.05 | |
| Step 3: Social support and health behaviors | |||
| Family/friends support (1–5) | −0.04 | ||
| Partner support (1–5) | −0.10 ** | ||
| Health behaviors (1–5) | −0.11 *** | ||
| F | 7.95 *** | 7.16 *** | 8.17 *** |
| R2 | 0.05 | 0.06 | 0.09 |
| ΔR2 | 0.05 *** | 0.01 ** | 0.03 *** |
| Variables | Step 1 (β) | Step 2 (β) | Step 3 (β) | Step 4 (β) | Step 5 (β) |
|---|---|---|---|---|---|
| Step 1: Sociodemographic variables | |||||
| Age | −0.02 | −0.02 | −0.03 | −0.04 | −0.005 |
| Years of Education | −0.05 | −0.06 | −0.04 | −0.03 | −0.03 |
| Income (Below average) | 0.14 *** | 0.13 *** | 0.11 ** | 0.09 * | 0.08 * |
| Relationship status (Married or cohabiting) | 0.06 | 0.06 | 0.05 | 0.04 | 0.03 |
| Current employment status (working) | 0.11 ** | 0.11 ** | 0.10 ** | 0.09 * | 0.09 ** |
| Number of children under 18 | −0.02 | −0.01 | −0.10 ** | −0.10 ** | −0.08 * |
| Step 2: COVID-19 related variables | |||||
| Contact with someone diagnosed COVID-19 | −0.02 | −0.01 | −0.01 | −0.02 | |
| Think they had COVID-19 without being diagnosed | 0.09 ** | 0.08 * | 0.08 * | 0.06 * | |
| Access to outdoor space (whenever) | 0.06 | 0.04 | 0.03 | 0.02 | |
| Step 3: Social support and health behaviors | |||||
| Family/friends support (1–5) | −0.07 | −0.06 | −0.05 | ||
| Partner support (1–5) | −0.09 * | −0.07 * | −0.08 * | ||
| Health behaviors (1–5) | −0.14 *** | −0.13 *** | −0.09 * | ||
| Step 4: Obstetric factors | |||||
| Gestational age (weeks) | −0.06 | −0.09 * | |||
| Prenatal appointment altered/canceled | 0.08 * | 0.02 | |||
| High-risk Pregnancy | 0.10 ** | 0.07 * | |||
| Step 5: Pandemic-Related Pregnancy Stress (PREPS) | |||||
| Preparedness | 0.25 *** | ||||
| Infection | 0.03 | ||||
| Positive Appraisal | −0.07 * | ||||
| F | 7.39 *** | 6.26 *** | 7.85 *** | 7.68 *** | 10.11 *** |
| R2 | 0.05 | 0.06 | 0.10 | 0.12 | 0.18 |
| ΔR2 | 0.05 *** | 0.01 ** | 0.04 *** | 0.03 *** | 0.06 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yirmiya, K.; Yakirevich-Amir, N.; Preis, H.; Lotan, A.; Atzil, S.; Reuveni, I. Women’s Depressive Symptoms during the COVID-19 Pandemic: The Role of Pregnancy. Int. J. Environ. Res. Public Health 2021, 18, 4298. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084298
Yirmiya K, Yakirevich-Amir N, Preis H, Lotan A, Atzil S, Reuveni I. Women’s Depressive Symptoms during the COVID-19 Pandemic: The Role of Pregnancy. International Journal of Environmental Research and Public Health. 2021; 18(8):4298. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084298
Chicago/Turabian StyleYirmiya, Karen, Noa Yakirevich-Amir, Heidi Preis, Amit Lotan, Shir Atzil, and Inbal Reuveni. 2021. "Women’s Depressive Symptoms during the COVID-19 Pandemic: The Role of Pregnancy" International Journal of Environmental Research and Public Health 18, no. 8: 4298. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084298