
Mini-Implant-Retained Overdentures for the Rehabilitation of Completely Edentulous Maxillae: A Systematic Review and Meta-Analysis

 and
and
Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Screening and Selection
2.3. Data Extraction
2.4. Risk of Bias and Quality of Evidence
2.5. Statistical Analysis
3. Results
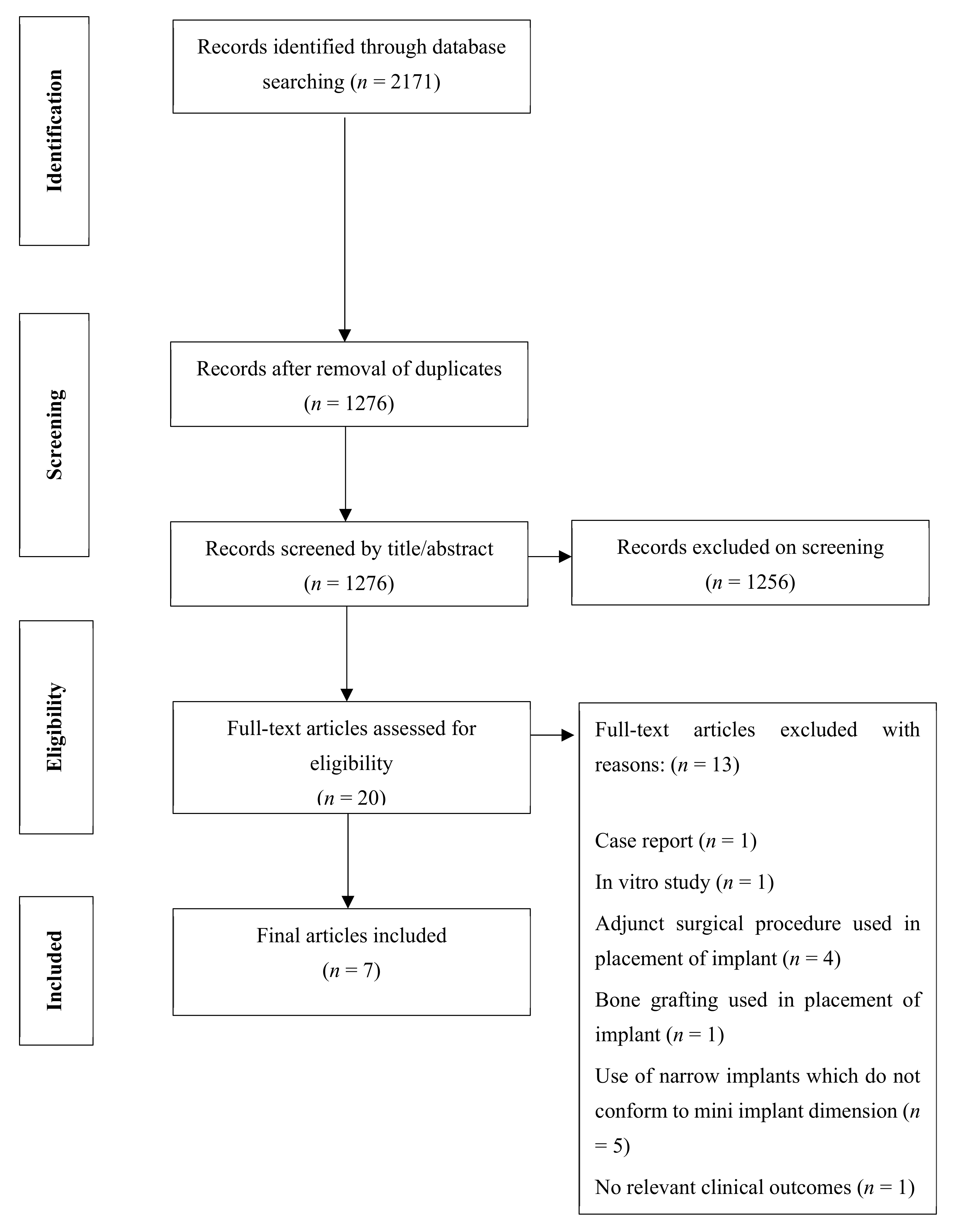
3.1. Literature Search
3.2. Study Characteristics
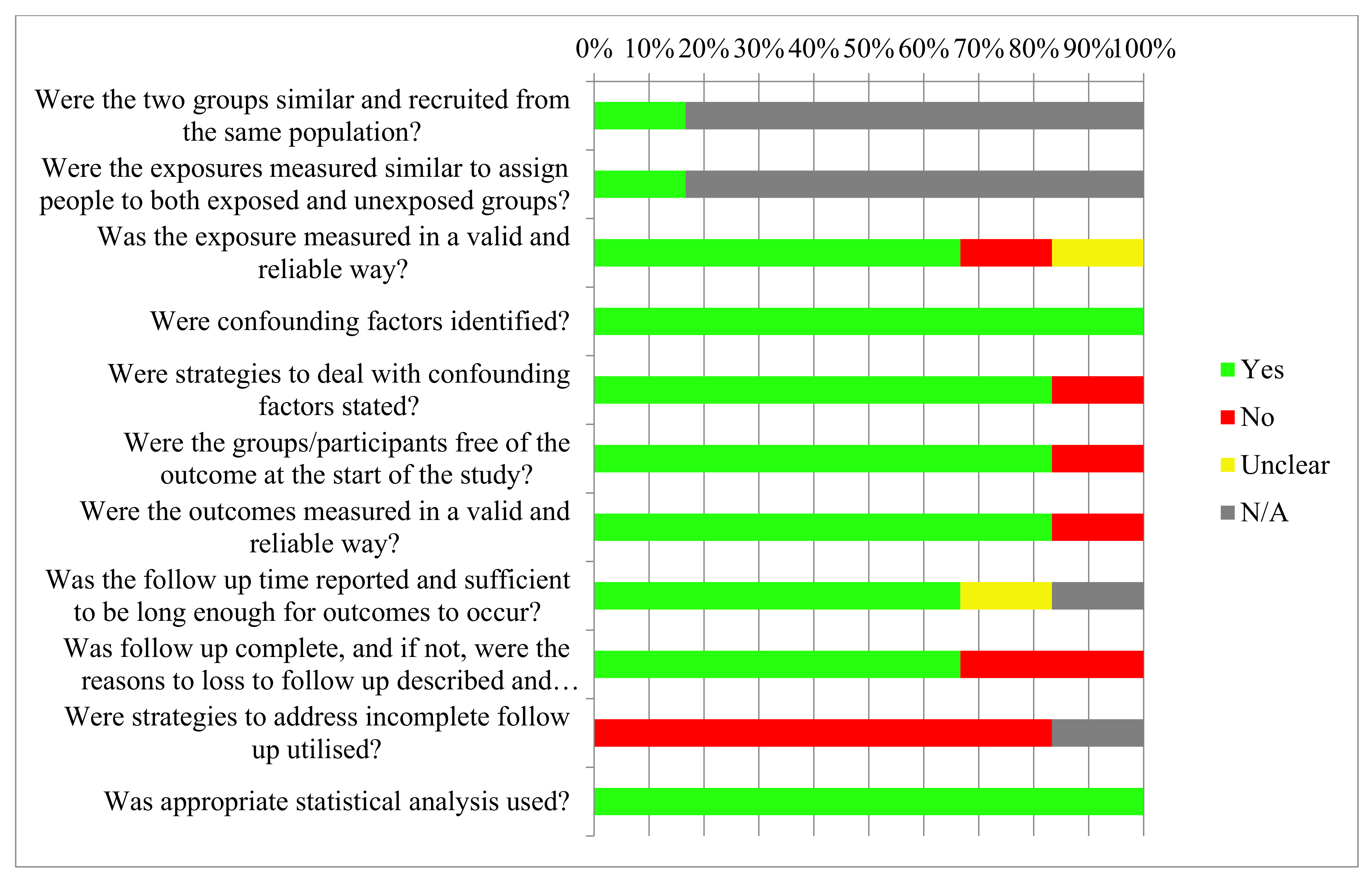
3.3. Risk of Bias
3.4. Effect of MDIs on Biological Outcomes
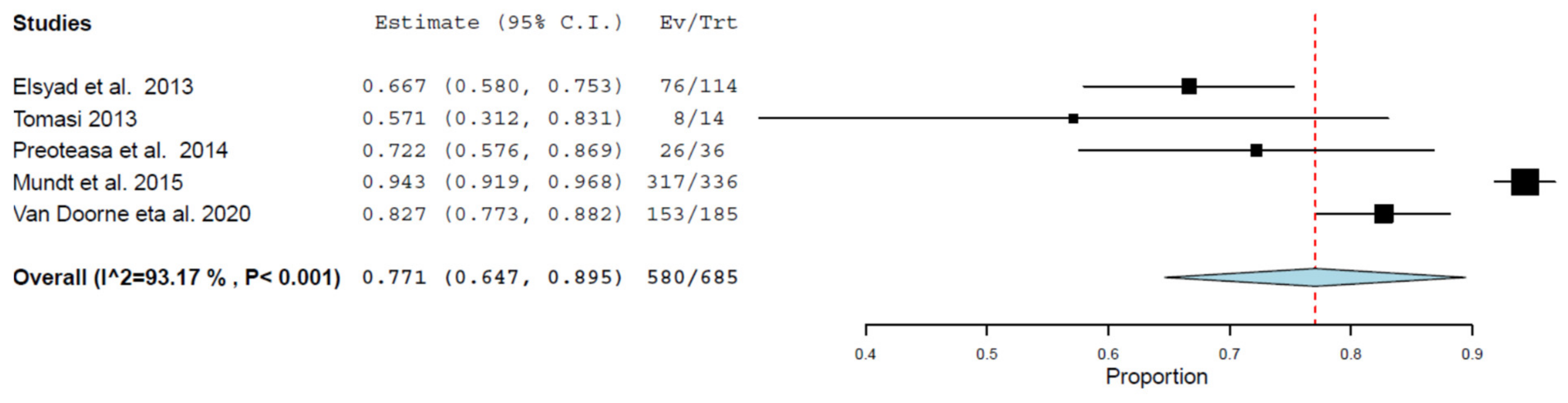
3.5. Effect of MDIs on Implant Survival
3.6. Effect of MDIs on Prosthesis Survival
3.7. Effect of MDIs on Patient Satisfaction and OHRQoL
3.8. Association of Confounding Variables and MDI Success
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bernabé, E.; Marcenes, W.; Hernandez, C.R.; Bailey, J.; Abreu, L.G.; Alipour, V.; Amini, S.; Arabloo, J.; Arefi, Z.; Arora, A.; et al. Global, Regional, and National Levels and Trends in Burden of Oral Conditions from 1990 to 2017: A Systematic Analysis for the Global Burden of Disease 2017 Study. J. Dent. Res. 2020, 99, 362–373. [Google Scholar] [CrossRef]
- Misch, C. Dental Implants Prosthetics, 2nd ed.; Elsevier: Mosby, Norway, 2005. [Google Scholar]
- Laurito, D.; Lamazza, L.; Spink, M.J.; De Biase, A. Tissue-supported dental implant prosthesis (overdenture): The search for the ideal protocol. A literature review. Ann. Stomatol. 2012, 3, 2–10. [Google Scholar]
- Goodacre, C.J. Implant overdentures: Their benefits for patients. Saudi J. Med. Med. Sci. 2018, 6, 1. [Google Scholar] [CrossRef]
- Sivaramakrishnan, G.; Sridharan, K. Comparison of patient satisfaction with mini-implant versus standard diameter implant overdentures: A systematic review and meta-analysis of randomized controlled trials. Int. J. Implants Dent. 2017, 3, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemos, C.A.A.; Verri, F.R.; Batista, V.E.D.S.; Júnior, J.F.S.; Mello, C.C.; Pellizzer, E.P. Complete overdentures retained by mini implants: A systematic review. J. Dent. 2017, 57, 4–13. [Google Scholar] [CrossRef] [Green Version]
- Upendran, A.; Gupta, N.; Salisbury, H. Dental, Mini-Implants; StatPearls Publishing LLC: Treasure Islands, FL, USA, 2019. [Google Scholar]
- Šćepanović, M.; Calvo-Guirado, J.L.; Marković, A.; Delgado-Ruiz, R.; Todorović, A.; Miličić, B.; Mišić, A.T. A 1-year prospective cohort study on mandibular overdentures retained by mini dental implants. Eur. J. Oral Implantol. 2012, 5, 367–379. [Google Scholar] [PubMed]
- Abou-Ayash, S.; Enkling, N.; Srinivasan, M.; Haueter, M.; Worni, A.; Schimmel, M. Evolution of in vivo assessed retention forces in one-piece mini dental implant-retained mandibular overdentures: 5-Year follow-up of a prospective clinical trial. Clin. Implants Dent. Relat. Res. 2019, 21, 968–976. [Google Scholar] [CrossRef] [PubMed]
- Ahn, M.-R.; An, K.-M.; Choi, J.-H.; Sohn, D.-S. Immediate Loading with Mini Dental Implants in the Fully Edentulous Mandible. Implant. Dent. 2004, 13, 367–372. [Google Scholar] [CrossRef]
- Singh, R.D.; Ramashanker, P.C. Management of atrophic mandibular ridge with mini dental implant system. Natl. J. Maxillofac. Surg. 2010, 1, 176–178. [Google Scholar] [CrossRef]
- Aunmeungtong, W.; Kumchai, T.; Strietzel, F.P.; Reichart, P.A.; Khongkhunthian, P. Comparative Clinical Study of Conventional Dental Implants and Mini Dental Implants for Mandibular Overdentures: A Randomized Clinical Trial. Clin. Implant. Dent. Relat. Res. 2017, 19, 328–340. [Google Scholar] [CrossRef]
- Elsyad, M.A.; Ghoneem, N.E.; El-Sharkawy, H. Marginal bone loss around unsplinted mini-implants supporting maxillary overdentures: A preliminary comparative study between partial and full palatal coverage. Quintessence Int. 2013, 44, 45–52. [Google Scholar]
- Kabbua, P.; Aunmeungtong, W.; Khongkhunthian, P. Computerised occlusal analysis of mini-dental implant-retained mandibular overdentures: A 1-year prospective clinical study. J. Oral Rehabil. 2020, 47, 757–765. [Google Scholar] [CrossRef]
- Slot, W.; Raghoebar, G.M.; Vissink, A.; Slater, J.J.H.; Meijer, H.J. A systematic review of implant-supported maxillary overdentures after a mean observation period of at least 1 year. J. Clin. Periodontol. 2010, 37, 98–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadowsky, S.J. Treatment considerations for maxillary implant overdentures: A systematic review. J. Prosthet. Dent. 2007, 97, 340–348. [Google Scholar] [CrossRef]
- Mericske-Stern, R. Treatment outcomes with implant-supported overdentures: Clinical considerations. J. Prosthet. Dent. 1998, 79, 66–73. [Google Scholar] [CrossRef]
- Mericske-Stern, R.D.; Taylor, T.D.; Belser, U. Management of the edentulous patient. Clin. Oral Implant. Res. 2000, 11, 108–125. [Google Scholar] [CrossRef]
- Kiener, P.; Oetterli, M.; Mericske, E.; Mericske-Stern, R. Effectiveness of maxillary overdentures supported by implants: Maintenance and prosthetic complications. Int. J. Prosthodont. 2002, 14, 133–140. [Google Scholar]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R. Chapter 7: Systematic Reviews of Etiology and Risk. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2017; Available online: https://reviewersmanual.joannabriggs.org (accessed on 20 July 2020).
- Wallace, B.C.; Dahabreh, I.J.; Trikalinos, T.A.; Lau, J.; Trow, P.; Schmid, C.H. Closing the Gap between Methodologists and End-Users: R as a Com-putational Back-End. J. Stat. Softw. 2012, 49, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Fonteyne, E.; Van Doorne, L.; Becue, L.; Matthys, C.; Bronckhorst, E.; De Bruyn, H. Speech evaluation during maxillary mini-dental implant overdenture treatment: A prospective study. J. Oral Rehabil. 2019, 46, 1151–1160. [Google Scholar] [CrossRef]
- Preoteasa, E.; Imre, M.; Preoteasa, C. A 3-Year Follow-up Study of Overdentures Retained by Mini–Dental Implants. Int. J. Oral Maxillofac. Implant 2014, 29, 1170–1176. [Google Scholar] [CrossRef] [Green Version]
- Van Doorne, L.; De Kock, L.; De Moor, A.; Shtino, R.; Bronkhorst, E.; Meijer, G.; De Bruyn, H. Flaplessly placed 2.4-mm mini-implants for maxillary overdentures: A prospective multicentre clinical cohort study. Int. J. Oral Maxillofac. Surg. 2020, 49, 384–391. [Google Scholar] [CrossRef]
- Mundt, T.; Schwahn, C.; Biffar, R.; Heinemann, F. Changes in Bone Levels around Mini-Implants in Edentulous Arches. Int. J. Oral Maxillofac. Implant. 2015, 30, 1149–1155. [Google Scholar] [CrossRef] [Green Version]
- Mundt, T.; Schwahn, C.; Stark, T.; Biffar, R. Clinical response of edentulous people treated with mini dental implants in nine dental practices. Gerodontology 2015, 32, 179–187. [Google Scholar] [CrossRef]
- Fergusson, D.; Aaron, S.D.; Guyatt, G.; Hébert, P. Post-randomisation exclusions: The intention to treat principle and exclud-ing patients from analysis. BMJ 2002, 325, 652–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kristman, V.; Manno, M.; Côté, P. Loss to Follow-Up in Cohort Studies: How Much is Too Much? Eur. J. Epidemiol. 2003, 19, 751–760. [Google Scholar] [CrossRef] [PubMed]
- Tomasi, C.; Idmyr, B.-O.; Wennström, J.L. Patient satisfaction with mini-implant stabilised full dentures. A 1-year prospective study. J. Oral Rehabil. 2013, 40, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Bidra, A.S.; Almas, K. Mini implants for definitive prosthodontic treatment: A systematic review. J. Prosthet. Dent. 2013, 109, 156–164. [Google Scholar] [CrossRef]
- Raghoebar, G.M.; Meijer, H.J.; Slot, W.; Slater, J.J.; Vissink, A. A systematic review of implant-supported overdentures in the edentulous maxilla, compared to the mandible: How many implants? Eur. J. Oral Implantol. 2014, 7 (Suppl. 2), S191–S201. [Google Scholar]
- Allum, S.R.; Tomlinson, R.A.; Joshi, R. The impact of loads on standard diameter, small diameter and mini implants: A comparative laboratory study. Clin. Oral Implant. Res. 2008, 19, 553–559. [Google Scholar] [CrossRef] [Green Version]
- Di Francesco, F.; De Marco, G.; Carnevale, U.A.G.; Lanza, M.; Lanza, A. The number of implants required to support a maxillary overdenture: A systematic review and meta-analysis. J. Prosthodont. Res. 2019, 63, 15–24. [Google Scholar] [CrossRef]
- Takahashi, T.; Gonda, T.; Maeda, Y. Effects of Reinforcement on Denture Strain in Maxillary Implant Overdentures: An In Vitro Study under Various Implant Configurations. Int. J. Oral Maxillofac. Implant. 2016, 31, e162–e167. [Google Scholar] [CrossRef] [Green Version]
- Pommer, B.; Krainhöfner, M.; Watzek, G.; Tepper, G.; Dintsios, C.-M. Relevance of Variations in the Opposing Dentition for the Functionality of Fixed and Removable Partial Dentures: A Systematic Review. Int. J. Dent. 2012, 2012, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Ando, T.; Maeda, Y.; Wada, M.; Gonda, T. Contribution of the palate to denture base support: An in vivo study. Int. J. Prosthodont. 2014, 27, 228–230. [Google Scholar] [CrossRef] [PubMed]
- Molly, L.; Nackaerts, O.; Vandewiele, K.; Manders, E.; Van Steenberghe, D.; Jacobs, R. Speech adaptation after treatment of full edentulism through immediate-loaded implant protocols. Clin. Oral Implant. Res. 2007, 19, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Pommer, B.; Frantal, S.; Willer, J.; Posch, M.; Watzek, G.; Tepper, G. Impact of dental implant length on early failure rates: A meta-analysis of observational studies. J. Clin. Periodontol. 2011, 38, 856–863. [Google Scholar] [CrossRef] [PubMed]
- Manor, Y.; Oubaid, S.; Mardinger, O.; Chaushu, G.; Nissan, J. Characteristics of Early Versus Late Implant Failure: A Retrospective Study. J. Oral Maxillofac. Surg. 2009, 67, 2649–2652. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| # | Search Term |
|---|---|
| #1 | Maxilla [MeSH term] OR Maxilla [All Fields] |
| #2 | Maxillary [All Fields] |
| #3 | (#1 OR #2) |
| #4 | Mini dental implant* [All Fields] |
| #5 | Narrow dental implant * [All Fields] |
| #6 | Mini implant* [All Fields] |
| #7 | Narrow implant* [All Fields] |
| #8 | Mini implant overdenture* [All Fields] |
| #9 | Narrow implant overdenture* [All Fields] |
| #10 | Mini implant supported overdenture* [All Fields] |
| #11 | Narrow implant supported overdenture* [All Fields] |
| #12 | Mini implant supported denture* [All Fields] |
| #13 | Narrow implant supported denture [All Fields] |
| #14 | Mini implant overlay denture* [All Fields] |
| #15 | Narrow implant overlay denture* [All Fields] |
| #16 | Mini implant supported overlay denture* [All Fields] |
| #17 | Narrow implant supported overlay denture* [All Fields] |
| #18 | Full mouth rehabilitation [All Fields] |
| #19 | (#4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18) |
| Final Search | #3 AND #19 |
| Selection Criteria | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Language type | English | Non-English |
| Study type | Empirical studies including randomised controlled trials, nonrandomised clinical trials, cohort studies, case series | Review studies including narrative reviews, systematic reviews, literature reviews |
| Study Features | Flapless placement of implants Implant diameter up to and including 2.4 mm Mini implant-retained overdentures Maxillary cases Partial and complete edentulism | Adjunct surgical procedures used for implant placement Implant diameter of 2.4 mm and more Overdentures retained via other means Fixed partial dentures Mandibular cases |
| Analysis of clinical outcomes | At least one of the following parameters: Patient satisfaction and perception in regard to treatment Success and survival rate | Studies focusing on participants pre-treatment characteristics |
| Publication date | Publications from 2010 to present | Publications prior to 2010 |
| Population | Human studies (all ages) | In vitro studies Animal studies |
| Selection criteria | Inclusion Criteria | Exclusion Criteria |
| Author (Year) | Design | Study Setting | Sample Size and Dropout Rates | Mean Age and Gender (M:F) | Opposing Dentition | Implant System | Number of Implants Placed Per Patient in Maxilla | Denture Design | Loading Period | Number of Follow-Ups | Length of Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Fonteyne (2019) | Prospective cohort study | University Clinic Ghent and General Hospital AZ ZENO Knokke-Blankenberge, Belgium | 25; 21.9% | 62.6; 17:13 | Natural teeth and combination of natural teeth and partial prosthesis | ILZ Southern Implant Inc. | 5 to 6 | Complete denture with partial palatal coverage | 6 months | Two: At provisional loading and final connection | 6 months |
| Elsyad (2013) | Prospective cohort study | Mansoura University, Mansoura, Egypt | 19; 0.0% | 63.8; 11:8 | All patients were given new mandibular dentures | MAX Thread, Sendaxs MDI, IMTECT | 6 | Group I—Full palatal coverage Group II—Partial palatal coverage | Immediate- same day | Three: 6, 12, and 24 months after insertion | 24 months |
| Van Doorne (2020) | Prospective cohort study | University Clinic Ghent and General Hospital AZ ZENO Knokke-Blankenberge, Belgium | 31; 6.5% | 62.3; 17:14 | Natural teeth and combination of natural teeth and partial prosthesis | ILZ Southern Implants Inc. | 6 | Complete denture with horseshoe design | 6 months | Six: 1 week, followed by 1, 3, 6, 12, and 24 months | 24 months |
| Mundt (2013, 2015) | Retrospective study | Nine private practices in Germany | 54; 26.9% | 71.2; 54:79 | Not specified | 3M ESPE | 4, 5, 6, 7, 8, or 10 | Complete dentures with complete and partial palatal coverage | Immediate or delayed with 3 to 4 months | Not specified | 27.1 ± 12.8 months |
| Preoteasa (2014) | Prospective cohort study | University of Medicine and Pharmacy, Bucharest, Romania | 23; 4.2% | 62.0; 10:13 | Natural teeth or fixed prosthetic restoration | IMTEC/3M ESPE | 5 or 6 | Complete denture with complete palatal coverage | Not specified | Six: Weekly during 1st month post-surgery,3 and 6 months, and 1, 2, and 3 years post-surgery | 36 months |
| Tomasi (2013) | Prospective cohort study | University of Gothenburg, Gothenburg and private practice, Mjolby, Sweden | 21; 8.7% | 71.0; 9:12 | Not specified | Dentatus Atlas | 2 and 4 | All complete dentures with full palatal coverage | Not specified | One: 12 months post-treatment | 12 months |
| Were the Two Groups Similar and Recruited from the Same Population? | Were the Exposures Measured Similar to Assign People to both Exposed and Unexposed Groups? | Was the Exposure Measured in a Valid and Reliable Way? | Were Confounding Factors Identified? | Were Strategies to Deal with Confounding Factors Stated? | Were the Groups/Participants Free of the Outcome at the Start of the Study? | Were the Outcomes Measured in a Valid and Reliable Way? | Was the Follow-Up Time Reported and Sufficient to be Long Enough for Outcomes to Occur? | Was the Follow-up Complete, and If Not, Were the Reasons for Loss to Follow-Up Described and Explored? | Were Strategies to Address Incomplete Follow-Up Utilised? | Was Appropriate Statistical Analysis Used? | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Fonteyne, E., et al. (2019) |  | |  |  |  | | | | | | |
| Elsyad, L., et al. (2013) | | | | | | | | | | | |
| Mundt, T., et al. (2013 and 2015) | | | | | | | | | | | |
| Preoteasa, E., et al. (2014) | | | | | | | | | | | |
| Tomasi, C., et al. (2013) | | | | | | | | | | | |
| Van Doorne, L., et al. (2020) | | | | | | | | | | | |
 —Not applicable;
—Not applicable;  —Yes;
—Yes;  —No;
—No;  —Unclear.
—Unclear.| Author (Year) | Outcomes Reported | Data Collection Method | Length of Follow-Up | Biological Outcomes | Implant Survival and Success Rates | Patient Satisfaction and Oral Health-Related Quality of Life (OHRQoL) |
|---|---|---|---|---|---|---|
| Fonteyne (2019) | -Articulation - Oromyofunctional behaviour - Patient satisfaction - Quality of life | Articulation: Digitally with video camera Oromyofunction: 3-point rating scale Patient satisfaction: with oral health and speech via 10 cm VAS scale OHRQoL: OHIP-14 | 6 months | Not specified. | Not specified. | Satisfaction with oral health: increased from 67% to 83% Satisfaction with speech: increased from 77% to 84% OHRQoL: improved- OHIP score decreased from 21.97 to 8.23. |
| Elsyad (2013) | - Peri-implant bone loss around MI - Mobility - Patient satisfaction - Survival rate of MI | Peri-implant bone loss: Radiographically Mobility: Periotest instrument Patient satisfaction: with retention and chewing measured via 10 cm VAS scale Survival rate: Kaplan–Meier life table analysis | 24 months | Mean vertical bone loss: Group I- 5.38 ± 1.65 mm Group II- 6.29 ± 2.33 mm Mobility: increased over time in both groups. Mobility of Group II > Group I at T2 and T3 | Survival rate: Group I—78.4% Group II—53.8% (significant difference) | Patient satisfaction with retention: Group I-2.5 ± 0.84; Group II—1.0 ± 0.99 (no significant difference) Patient satisfaction with chewing: Group I- 7.9 ± 0.73; Group II- 8.22 ± 0.97 (significant improvement in both groups). |
| Van Doorne (2020) | - Implant stability at surgery - Patient’s perception of pain - Patient satisfaction - Survival rate - Success rate | Implant stability: Torque wrench Perception of pain: Numeric rating scale of 1 to 10 Patient satisfaction: ‘yes’/ ‘no’ questionnaire Survival rate: Kaplan–Meier life table analysis Success rate: When >5 MDIs are lost. | 24 months | Not specified. | Survival rate: 82.3% Success rate: 93.5% Initial MDI failure rate: 17.3%. All MDI failures occurred in initial healing phase. | Average final patient satisfaction score was 8.6 ± 1.7. 96% of the patients would recommend this treatment to others. |
| Mundt (2013, 2015) | - Surgical and prosthetic complications - OHRQoL- Implant and prosthetic status Changes in bone level | Surgical and prosthetic complications: Data from patient records, oral examinations, and questionnaires. OHRQoL: OHIP-14 scale Implant and prosthetic status: Compared with participants records Changes in bone level: Radiographically | 27.1 ± 12.8 months 2.2 ± 1 years | 10.3% MDIs TBL of >2 mm 3.3% MDIs TBL of >3 mm | Survival rate: 94.3% 15 maxillary implants lost after insertion. | Significant improvements for all participants in all single questions regarding OHRQoL Retention rated very high in 9 (16.7%), fair in 44 (81.5%), and low in one denture. |
| Preoteasa (2014) | -MDI status - Overdenture status - Patient’s perception regarding treatment | MDI Status: Radiographically, clinical evaluation, self-reported peri-implant bleeding. Overdenture status: Self-reported Patient perception: Self-reported | 36 months | 11 MDIs presented with bone loss >1 thread. | MDI health status: 8 failed | Patients generally satisfied with aesthetics, retention, function (mastication and phonation). Complaints mainly associated with occasional pain to soft tissue supporting overdenture. |
| Tomasi (2013) | - Patient satisfaction - Clinical assessments - Survival rate | Patient satisfaction: 10 cm VAS scale and ‘yes’/‘no’ questionnaire Clinical assessment: Plaque score, BoP, and implant stability judged by percussion | 12 months | Mean plaque score of 20% for maxillary and mandibular MDIs. Mean BoP score of 30%. Mean pocket probing depth was 2.3 mm with a range from 1 to 6 mm. | Implant failure rate was significantly higher in maxilla than the mandible, 43% and 15%, respectively. 6 out of 14 implants failed | All patients said ‘yes’ when asked if they were satisfied with their denture. Patient satisfaction with chewing ability increased from 4.5 to 9.0 Patient satisfaction with speech increased from 5.8 to 9.3 Patient overall denture satisfaction increased from 3.3 to 9.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vi, S.; Pham, D.; Du, Y.Y.M.; Arora, H.; Tadakamadla, S.K. Mini-Implant-Retained Overdentures for the Rehabilitation of Completely Edentulous Maxillae: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 4377. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084377
Vi S, Pham D, Du YYM, Arora H, Tadakamadla SK. Mini-Implant-Retained Overdentures for the Rehabilitation of Completely Edentulous Maxillae: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(8):4377. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084377
Chicago/Turabian StyleVi, Serena, Damon Pham, Yu Yian Marina Du, Himanshu Arora, and Santosh Kumar Tadakamadla. 2021. "Mini-Implant-Retained Overdentures for the Rehabilitation of Completely Edentulous Maxillae: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 8: 4377. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084377