
The Association between Migraine and Abdominal Aortic Aneurysms: A Nationwide Population-Based Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
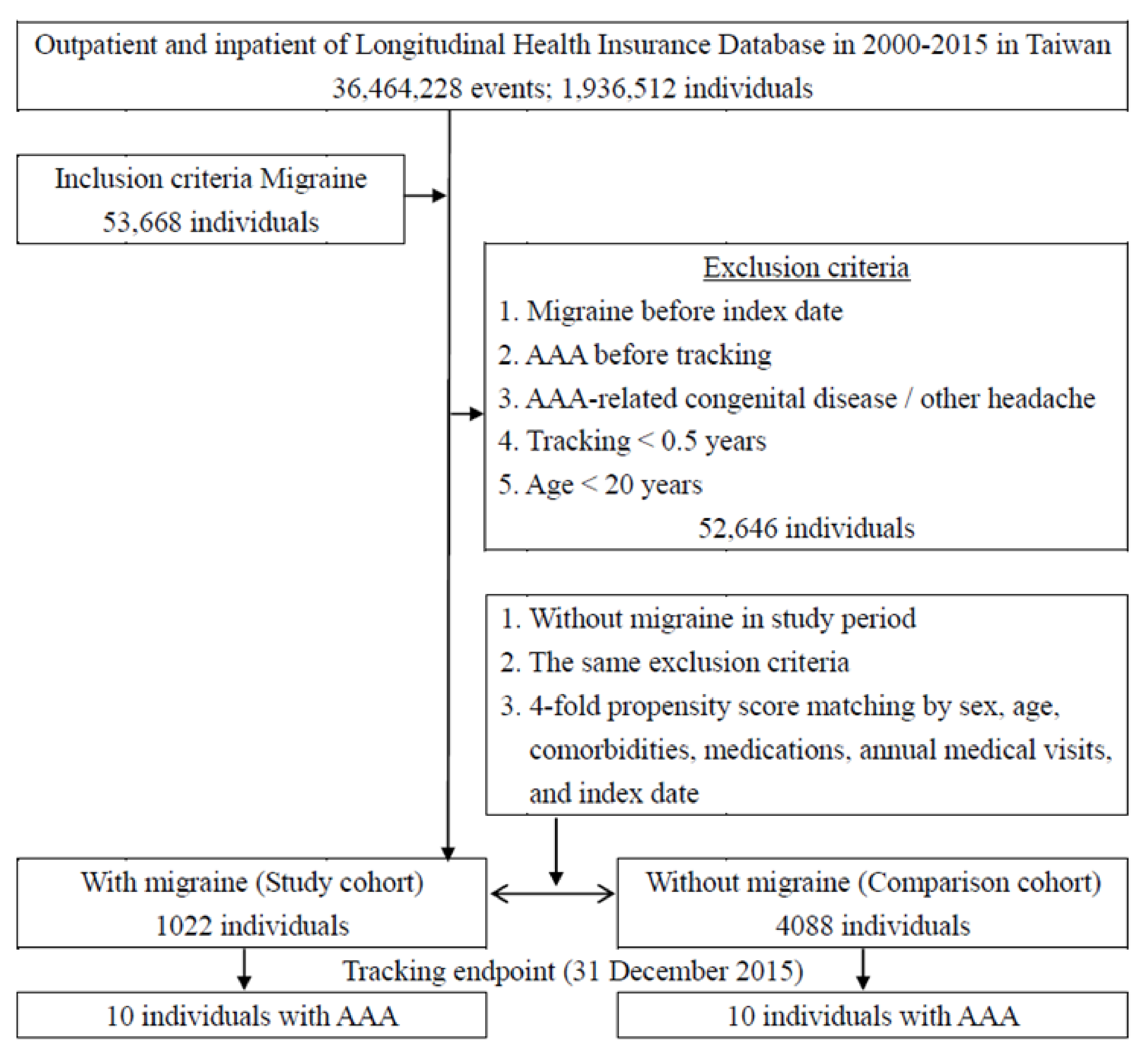
2.2. Sampled Patients
2.3. Patient and Public Involvement
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Kruit, M.C.; van Buchem, M.A.; Hofman, P.A.; Bakkers, J.T.; Terwindt, G.M.; Ferrari, M.D.; Launer, L.J. Migraine as a risk factor for subclinical brain lesions. JAMA 2004, 291, 427–434. [Google Scholar] [CrossRef] [Green Version]
- Agostoni, E.C.; Longoni, M. Migraine and cerebrovascular disease: Still a dangerous connection? Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2018, 39, 33–37. [Google Scholar] [CrossRef]
- Zarcone, D.; Corbetta, S. Shared mechanisms of epilepsy, migraine and affective disorders. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2017, 38, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Scher, A.I.; Terwindt, G.M.; Picavet, H.S.; Verschuren, W.M.; Ferrari, M.D.; Launer, L.J. Cardiovascular risk factors and migraine: The GEM population-based study. Neurology 2005, 64, 614–620. [Google Scholar] [CrossRef]
- López-Mesonero, L.; Márquez, S.; Parra, P.; Gámez-Leyva, G.; Muñoz, P.; Pascual, J. Smoking as a precipitating factor for migraine: A survey in medical students. J. Headache Pain 2009, 10, 101–103. [Google Scholar] [CrossRef] [Green Version]
- Rist, P.M.; Tzourio, C.; Kurth, T. Associations between lipid levels and migraine: Cross-sectional analysis in the epidemiology of vascular ageing study. Cephalalgia Int. J. Headache 2011, 31, 1459–1465. [Google Scholar] [CrossRef] [Green Version]
- Giannini, G.; Cevoli, S.; Sambati, L.; Cortelli, P. Migraine: Risk factor and comorbidity. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2012, 33 (Suppl. 1), S37–S41. [Google Scholar] [CrossRef]
- Kent, K.C. Abdominal Aortic Aneurysms. N. Engl. J. Med. 2014, 371, 2101–2108. [Google Scholar] [CrossRef]
- Allison, M.A.; Kwan, K.; DiTomasso, D.; Wright, C.M.; Criqui, M.H. The epidemiology of abdominal aortic diameter. J. Vasc. Surg. 2008, 48, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Neri, M.; Frustaci, A.; Milic, M.; Valdiglesias, V.; Fini, M.; Bonassi, S.; Barbanti, P. A meta-analysis of biomarkers related to oxidative stress and nitric oxide pathway in migraine. Cephalalgia Int. J. Headache 2015, 35, 931–937. [Google Scholar] [CrossRef]
- Tietjen, G.E.; Khubchandani, J.; Herial, N.; Palm-Meinders, I.H.; Koppen, H.; Terwindt, G.M.; van Buchem, M.A.; Launer, L.J.; Ferrari, M.D.; Kruit, M.C. Migraine and vascular disease biomarkers: A population-based case-control study. Cephalalgia Int. J. Headache 2018, 38, 511–518. [Google Scholar] [CrossRef]
- Tietjen, G.E.; Collins, S.A. Hypercoagulability and Migraine. Headache 2018, 58, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.H.; Wang, J.C.; Liao, W.I.; Hsu, Y.J.; Lin, C.Y.; Liao, M.T.; Huang, P.H.; Lin, S.J. Fucoidan attenuates angiotensin II-induced abdominal aortic aneurysms through the inhibition of c-Jun N-terminal kinase and nuclear factor kappaB activation. J. Vasc. Surg. 2018, 68, 72S–81S.e71. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.L.; Kao, Y.H.; Lin, S.J.; Lee, C.H.; Lai, M.L. Validation of the National Health Insurance Research Database with ischemic stroke cases in Taiwan. Pharmacoepidemiol. Drug Saf. 2011, 20, 236–242. [Google Scholar] [CrossRef]
- Lee, C.C.; Lee, M.T.; Chen, Y.S.; Lee, S.H.; Chen, Y.S.; Chen, S.C.; Chang, S.C. Risk of Aortic Dissection and Aortic Aneurysm in Patients Taking Oral Fluoroquinolone. JAMA Intern. Med. 2015, 175, 1839–1847. [Google Scholar] [CrossRef]
- Hsieh, C.Y.; Su, C.C.; Shao, S.C.; Sung, S.F.; Lin, S.J.; Kao Yang, Y.H.; Lai, E.C. Taiwan’s National Health Insurance Research Database: Past and future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.J.; Fuh, J.L.; Huang, S.Y.; Yang, S.S.; Wu, Z.A.; Hsu, C.H.; Wang, C.H.; Yu, H.Y.; Wang, P.J. Diagnosis and development of screening items for migraine in neurological practice in Taiwan. J. Formos. Med. Assoc. 2008, 107, 485–494. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.P.; Hsieh, M.L.; Chiang, J.H.; Chang, H.Y.; Hsieh, V.C. Migraine and risk of narcolepsy in children: A nationwide longitudinal study. PLoS ONE 2017, 12, e0189231. [Google Scholar] [CrossRef]
- Schwedt, T.J. Chronic migraine. BMJ 2014, 348, g1416. [Google Scholar] [CrossRef] [Green Version]
- Baykan, B.; Ertas, M.; Karlı, N.; Uluduz, D.; Uygunoglu, U.; Ekizoglu, E.; Kocasoy Orhan, E.; Saip, S.; Zarifoglu, M.; Siva, A. Migraine incidence in 5 years: A population-based prospective longitudinal study in Turkey. J. Headache Pain 2015, 16, 103. [Google Scholar] [CrossRef] [Green Version]
- Lu, S.R.; Fuh, J.L.; Chen, W.T.; Juang, K.D.; Wang, S.J. Chronic daily headache in Taipei, Taiwan: Prevalence, follow-up and outcome predictors. Cephalalgia Int. J. Headache 2001, 21, 980–986. [Google Scholar] [CrossRef]
- Wang, S.J.; Fuh, J.L.; Lu, S.R.; Liu, C.Y.; Hsu, L.C.; Wang, P.N.; Liu, H.C. Chronic daily headache in Chinese elderly: Prevalence, risk factors, and biannual follow-up. Neurology 2000, 54, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Kent, K.C.; Zwolak, R.M.; Egorova, N.N.; Riles, T.S.; Manganaro, A.; Moskowitz, A.J.; Gelijns, A.C.; Greco, G. Analysis of risk factors for abdominal aortic aneurysm in a cohort of more than 3 million individuals. J. Vasc. Surg. 2010, 52, 539–548. [Google Scholar] [CrossRef] [Green Version]
- Ashton, H.A.; Gao, L.; Kim, L.G.; Druce, P.S.; Thompson, S.G.; Scott, R.A.P. Fifteen-year follow-up of a randomized clinical trial of ultrasonographic screening for abdominal aortic aneurysms. Br. J. Surg. 2007, 94, 696–701. [Google Scholar] [CrossRef] [PubMed]
- Fagherazzi, G.; El Fatouhi, D.; Fournier, A.; Gusto, G.; Mancini, F.R.; Balkau, B.; Boutron-Ruault, M.C.; Kurth, T.; Bonnet, F. Associations between Migraine and Type 2 Diabetes in Women: Findings from the E3N Cohort Study. JAMA Neurol. 2019, 76, 257–263. [Google Scholar] [CrossRef]
- Pafili, K.; Gouni-Berthold, I.; Papanas, N.; Mikhailidis, D.P. Abdominal aortic aneurysms and diabetes mellitus. J. Diabetes Complicat. 2015, 29, 1330–1336. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Schulz, U.G.; Kuker, W.; Rothwell, P.M.; Oxford Vascular, S. Age-specific association of migraine with cryptogenic TIA and stroke: Population-based study. Neurology 2015, 85, 1444–1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eikermann-Haerter, K.; Lee, J.H.; Yuzawa, I.; Liu, C.H.; Zhou, Z.; Shin, H.K.; Zheng, Y.; Qin, T.; Kurth, T.; Waeber, C.; et al. Migraine mutations increase stroke vulnerability by facilitating ischemic depolarizations. Circulation 2012, 125, 335–345. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.C.; Chien, W.C.; Wang, J.C.; Chung, C.H.; Liao, W.I.; Lin, W.S.; Lin, C.S.; Tsai, S.H. Association between Atrial Fibrillation and Aortic Aneurysms: A Population-Based Cohort Study. J. Vasc. Res. 2018, 55, 299–307. [Google Scholar] [CrossRef]
- Sen, S.; Androulakis, X.M.; Duda, V.; Alonso, A.; Chen, L.Y.; Soliman, E.Z.; Magnani, J.; Trivedi, T.; Merchant, A.T.; Gottesman, R.F.; et al. Migraine with visual aura is a risk factor for incident atrial fibrillation: A cohort study. Neurology 2018, 91, e2202–e2210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adelborg, K.; Szepligeti, S.K.; Holland-Bill, L.; Ehrenstein, V.; Horvath-Puho, E.; Henderson, V.W.; Sorensen, H.T. Migraine and risk of cardiovascular diseases: Danish population based matched cohort study. BMJ 2018, 360, k96. [Google Scholar] [CrossRef] [Green Version]
- Witvoet, E.H.; Pelzer, N.; Terwindt, G.M.; Rinkel, G.J.E.; Vlak, M.H.M.; Algra, A.; Wermer, M.J.H. Migraine prevalence in patients with unruptured intracranial aneurysms: A case-control study. Brain Behav. 2017, 7, e00662. [Google Scholar] [CrossRef]
- Lebedeva, E.R.; Gurary, N.M.; Sakovich, V.P.; Olesen, J. Migraine before rupture of intracranial aneurysms. J. Headache Pain 2013, 14, 15. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.C.; Chien, W.C.; Chung, C.H.; Lin, C.Y.; Chen, Y.H.; Liao, M.T.; Liao, W.I.; Hsu, C.C.; Tsai, S.H. Association between surgical repair of aortic aneurysms and the diagnosis of intracranial aneurysms. J. Vasc. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Al-Kawaz, M.; Kamel, H.; Murthy, S.B.; Merkler, A.E. Association of Aortic Aneurysms and Dissections with Subarachnoid Hemorrhage. J. Am. Heart Assoc. 2019, 8, e013456. [Google Scholar] [CrossRef]
- Magalhaes, J.E.; Barros, I.M.L.; Pedrosa, R.P.; Sampaio Rocha-Filho, P.A. Migraine and Markers of Carotid Atherosclerosis in Middle-Aged Women: A Cross-Sectional Study. Headache 2019, 59, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Sacco, S.; Ornello, R.; Ripa, P.; Tiseo, C.; Degan, D.; Pistoia, F.; Carolei, A. Migraine and risk of ischaemic heart disease: A systematic review and meta-analysis of observational studies. Eur. J. Neurol. 2015, 22, 1001–1011. [Google Scholar] [CrossRef]
- Spector, J.T.; Kahn, S.R.; Jones, M.R.; Jayakumar, M.; Dalal, D.; Nazarian, S. Migraine headache and ischemic stroke risk: An updated meta-analysis. Am. J. Med. 2010, 123, 612–624. [Google Scholar] [CrossRef] [Green Version]
- Schurks, M.; Rist, P.M.; Shapiro, R.E.; Kurth, T. Migraine and mortality: A systematic review and meta-analysis. Cephalalgia Int. J. Headache 2011, 31, 1301–1314. [Google Scholar] [CrossRef] [Green Version]
- Bigal, M.E.; Kurth, T.; Hu, H.; Santanello, N.; Lipton, R.B. Migraine and cardiovascular disease: Possible mechanisms of interaction. Neurology 2009, 72, 1864–1871. [Google Scholar] [CrossRef] [Green Version]
- Koshty, A.; Bork, M.; Boning, A.; Gunduz, D.; Pleger, S.P. Coronary Artery Disease as a Relevant Risk Factor in Screening of Abdominal Aortic Ectasia and Aneurysm. Thorac. Cardiovasc. Surg. 2018. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.C.; Chien, W.C.; Chung, C.H.; Liao, W.I.; Tsao, C.H.; Wu, Y.F.; Tsai, S.H. Increased risk of malignancy in patients with an aortic aneurysm: A nationwide population-based retrospective study. Oncotarget 2018, 9, 2829–2837. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.-C.; Chien, W.-C.; Chung, C.-H.; Lin, C.-Y.; Hsu, C.-W.; Lin, C.-S.; Tsai, S.-H. Association between surgical repair of aortic aneurysms and the diagnosis of subsequent cardiovascular diseases. J. Cardiol. 2019. [Google Scholar] [CrossRef]
- Kok, S.N.; Hayes, S.N.; Cutrer, F.M.; Raphael, C.E.; Gulati, R.; Best, P.J.M.; Tweet, M.S. Prevalence and Clinical Factors of Migraine in Patients With Spontaneous Coronary Artery Dissection. J. Am. Heart Assoc. 2018, 7, e010140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, M.; Christiansen, C.F.; Mehnert, F.; Rothman, K.J.; Sorensen, H.T. Non-steroidal anti-inflammatory drug use and risk of atrial fibrillation or flutter: Population based case-control study. BMJ 2011, 343, d3450. [Google Scholar] [CrossRef] [Green Version]
- Cooper, C.; Chapurlat, R.; Al-Daghri, N.; Herrero-Beaumont, G.; Bruyere, O.; Rannou, F.; Roth, R.; Uebelhart, D.; Reginster, J.Y. Safety of Oral Non-Selective Non-Steroidal Anti-Inflammatory Drugs in Osteoarthritis: What Does the Literature Say? Drugs Aging 2019, 36, 15–24. [Google Scholar] [CrossRef] [Green Version]
- Ungprasert, P.; Srivali, N.; Wijarnpreecha, K.; Charoenpong, P.; Knight, E.L. Non-steroidal anti-inflammatory drugs and risk of venous thromboembolism: A systematic review and meta-analysis. Rheumatology 2015, 54, 736–742. [Google Scholar] [CrossRef] [Green Version]
- Lin, K.H.; Chu, C.M.; Lin, Y.K.; Chiao, H.Y.; Pu, T.W.; Tsai, Y.M.; Chen, Y.Y.; Huang, H.K.; Chang, H.; Lee, S.C.; et al. The abbreviated burn severity index as a predictor of acute respiratory distress syndrome in young individuals with severe flammable starch-based powder burn. Burn. J. Int. Soc. Burn Inj. 2018. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, A.T.; Haskal, Z.J.; Hertzer, N.R.; Bakal, C.W.; Creager, M.A.; Halperin, J.L.; Hiratzka, L.F.; Murphy, W.R.; Olin, J.W.; Puschett, J.B.; et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): A collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients with Peripheral Arterial Disease): Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation 2006, 113, e463–e654. [Google Scholar] [CrossRef] [Green Version]
- McGloughlin, T.M.; Doyle, B.J. New approaches to abdominal aortic aneurysm rupture risk assessment: Engineering insights with clinical gain. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 1687–1694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, T.M.; Chuang, Y.W.; Yu, M.C.; Chen, C.H.; Yang, C.K.; Huang, S.T.; Lin, C.L.; Shu, K.H.; Kao, C.H. Risk of cancer in patients with polycystic kidney disease: A propensity-score matched analysis of a nationwide, population-based cohort study. Lancet Oncol. 2016, 17, 1419–1425. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total | With Migraine | Without Migraine | p-Value | |
|---|---|---|---|---|
| N (%) | N (%) | N (%) | ||
| Total | 5110 | 1022 (20%) | 4088 (80%) | |
| Sex | 0.999 | |||
| Male | 1640 (32.09%) | 328 (32.09%) | 1312 (32.09%) | |
| Female | 3470 (67.91%) | 694 (67.91%) | 2776 (67.91%) | |
| Age (years) | 47.12 ± 16.86 | 46.92 ± 16.46 | 47.17 ± 16.96 | 0.674 |
| Hypertension | 488 (9.55%) | 109 (10.67%) | 379 (9.27%) | 0.190 |
| Hyperlipidemia | 180 (3.52%) | 40 (3.91%) | 140 (3.42%) | 0.448 |
| DM | 390 (7.63%) | 64 (6.26%) | 326 (7.97%) | 0.065 |
| Ischemic stroke | 112 (2.19%) | 22 (2.15%) | 90 (2.20%) | 0.924 |
| Intracerebral hemorrhage | 25 (0.49%) | 6 (0.59%) | 19 (0.46%) | 0.617 |
| CAD | 298 (5.83%) | 72 (7.05%) | 226 (5.53%) | 0.073 |
| AF | 39 (0.76%) | 4 (0.39%) | 35 (0.86%) | 0.159 |
| HF | 75 (1.47%) | 14 (1.37%) | 61 (1.49%) | 0.885 |
| COPD | 462 (9.04%) | 88 (8.61%) | 374 (9.15%) | 0.592 |
| CKD | 137 (2.68%) | 23 (2.25%) | 114 (2.79%) | 0.387 |
| Malignancy | 118 (2.31%) | 21 (2.05%) | 97 (2.37%) | 0.545 |
| Annual medical visiting | 7.82 ± 6.83 | 7.65 ± 6.79 | 7.86 ± 6.84 | 0.379 |
| Total | With Migraine | Without Migraine | p-Value | |
|---|---|---|---|---|
| N (%) | N (%) | N (%) | ||
| Total | 5110 | 1022 (20.00%) | 4088 (80.00%) | |
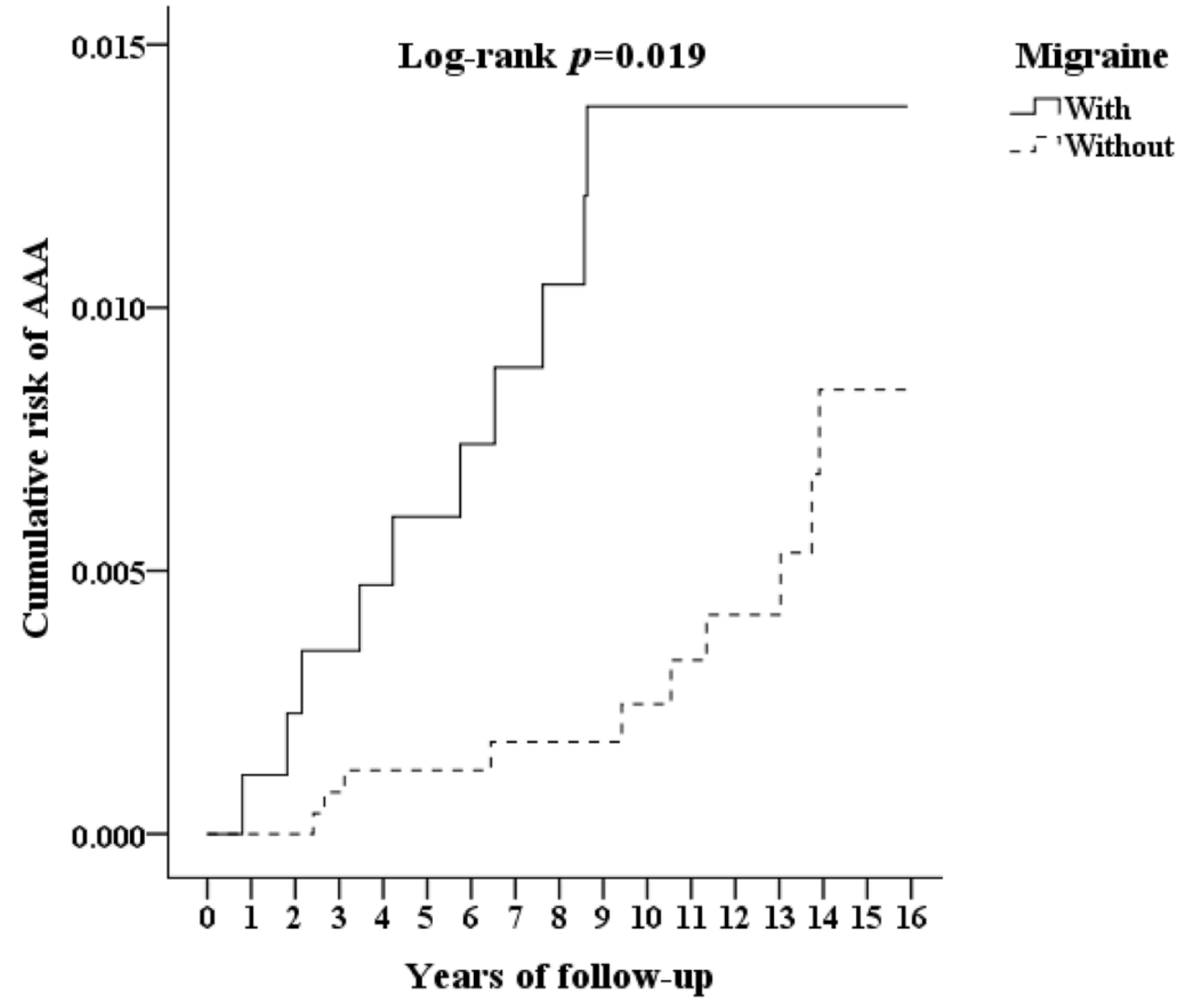
| AAA | 20 (0.39%) | 10 (0.98%) | 10 (0.24%) | 0.003 * |
| Sex | 0.999 | |||
| Male | 1640 (32.09%) | 328 (32.09%) | 1312 (32.09%) | |
| Female | 3470 (67.91%) | 694(67.91%) | 2776 (67.91%) | |
| Age (years) | 54.02 ± 18.39 | 56.02 ± 17.70 | 53.52 ± 18.53 | <0.001 * |
| Hypertension | 797 (15.60%) | 200 (19.57%) | 597 (14.60%) | <0.001 * |
| DM | 643 (12.58%) | 147 (14.38%) | 496 (12.13%) | 0.058 |
| Hyperlipidemia | 121 (2.37%) | 37 (3.62%) | 84 (2.05%) | 0.005 * |
| Ischemic stroke | 130 (2.54%) | 30 (2.94%) | 100 (2.45%) | 0.375 |
| Intracerebral hemorrhage | 52 (1.02%) | 14 (1.37%) | 38 (0.93%) | 0.222 |
| CAD | 336(6.58%) | 80 (7.83%) | 256 (6.26%) | 0.078 |
| AF | 71(1.39%) | 14 (1.37%) | 57 (1.39%) | 0.952 |
| HF | 176 (3.44%) | 36 (3.52%) | 140 (3.42%) | 0.848 |
| COPD | 310 (6.07%) | 81 (7.93%) | 229 (5.60%) | 0.007 * |
| CKD | 287 (5.62%) | 56 (5.48%) | 231 (5.65%) | 0.879 |
| Malignancy | 540 (9.86%) | 74 (7.24%) | 430 (10.52%) | 0.002 * |
| Variables | Crude HR | 95% CI | p | Adjusted HR | 95% CI | p-Value | ||
|---|---|---|---|---|---|---|---|---|
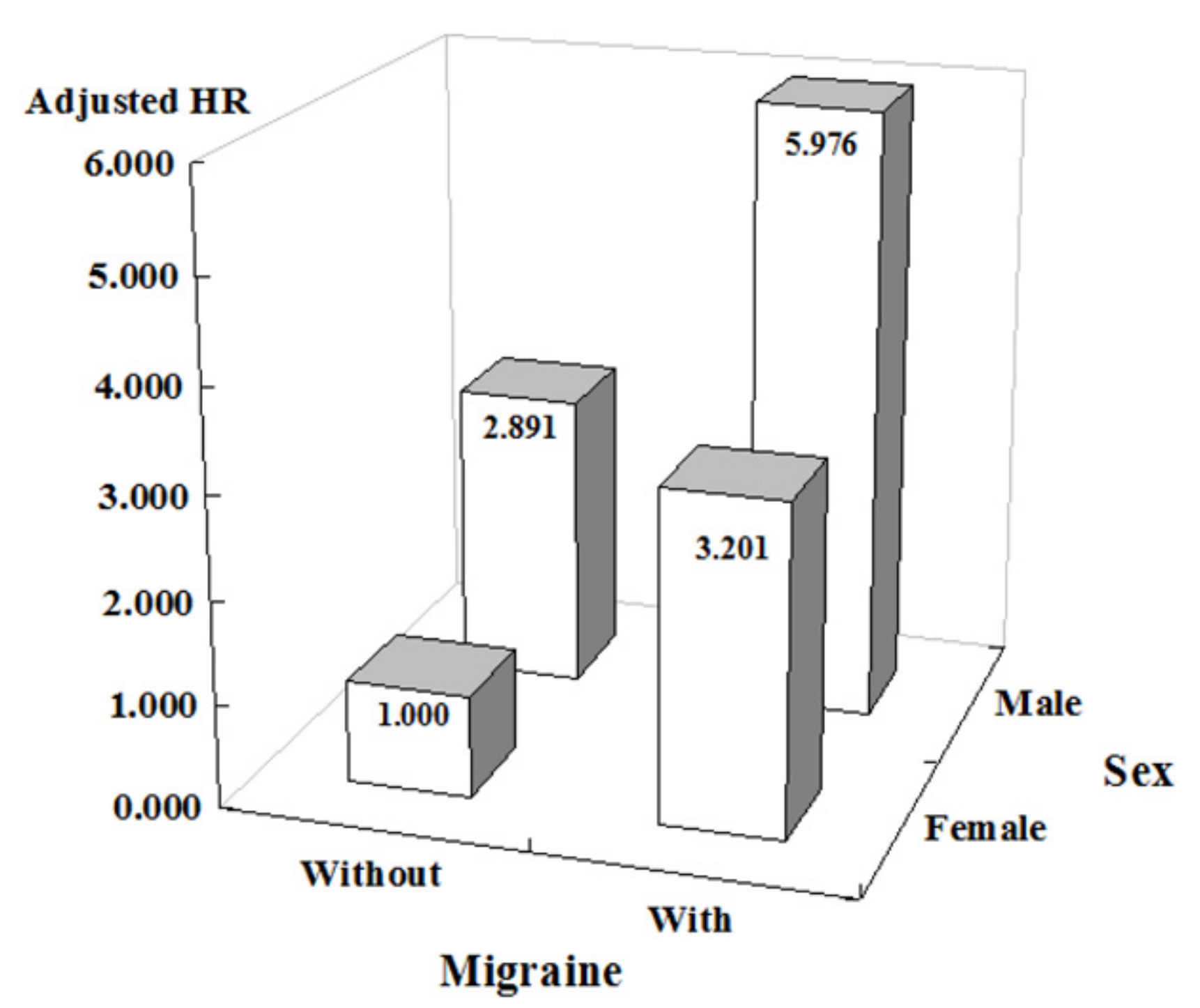
| Migraine | 2.757 | 1.146 | 6.632 | 0.024 | 3.558 | 1.439 | 8.799 | 0.006 * |
| Male | 3.192 | 1.301 | 7.833 | 0.011 | 3.008 | 1.132 | 7.998 | 0.027 * |
| Age (years) | 1.011 | 0.983 | 1.039 | 0.452 | 0.993 | 0.961 | 1.026 | 0.684 |
| Hypertension | 1.012 | 0.149 | 1.754 | 0.287 | 1.422 | 0.115 | 1.550 | 0.194 |
| DM | 1.504 | 0.117 | 2.174 | 0.358 | 1.487 | 0.108 | 2.209 | 0.351 |
| Hyperlipidemia | ||||||||
| Ischemic stroke | 4.266 | 0.989 | 18.406 | 0.052 | 4.462 | 0.952 | 20.900 | 0.058 |
| Intracerebral hemorrhage | 13.009 | 2.968 | 57.021 | 0.001 | 22.406 | 4.476 | 112.235 | <0.001 * |
| CAD | 2.757 | 0.921 | 8.252 | 0.070 | 4.402 | 1.189 | 13.738 | 0.025 * |
| AF | ||||||||
| HF | 2.962 | 0.678 | 12.941 | 0.149 | 1.985 | 0.388 | 10.144 | 0.410 |
| COPD | 2.245 | 0.656 | 7.679 | 0.198 | 1.897 | 0.501 | 7.176 | 0.346 |
| CKD | 1.934 | 0.123 | 7.100 | 0.948 | 1.662 | 0.084 | 5.214 | 0.695 |
| Malignancy | 2.550 | 0.841 | 7.732 | 0.098 | 3.848 | 1.190 | 12.438 | 0.024 * |
| Competing Risk in the Model | ||||||
|---|---|---|---|---|---|---|
| Sensitivity Test | Migraine Subgroups | Adjusted HR | 95% CI | p-Value | ||
| Overall | Without migraine | Reference | ||||
| With migraine | 3.558 | 1.439 | 8.799 | 0.006 | ||
| With aura | 5.426 | 2.201 | 16.984 | <0.001 | ||
| Without aura | 1.502 | 0.906 | 2.978 | 0.211 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, J.-Y.; Tung, C.-S.; Wang, J.-C.; Chien, W.-C.; Chung, C.-H.; Lin, C.-Y.; Tsai, S.-H. The Association between Migraine and Abdominal Aortic Aneurysms: A Nationwide Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 4389. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084389
Lin J-Y, Tung C-S, Wang J-C, Chien W-C, Chung C-H, Lin C-Y, Tsai S-H. The Association between Migraine and Abdominal Aortic Aneurysms: A Nationwide Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(8):4389. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084389
Chicago/Turabian StyleLin, Jou-Yu, Che-Se Tung, Jen-Chun Wang, Wu-Chien Chien, Chi-Hsiang Chung, Chih-Yuan Lin, and Shih-Hung Tsai. 2021. "The Association between Migraine and Abdominal Aortic Aneurysms: A Nationwide Population-Based Cohort Study" International Journal of Environmental Research and Public Health 18, no. 8: 4389. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084389