
Twenty-Four-Year Trends in Family and Regional Disparities in Fruit, Vegetable and Sugar-Sweetened Beverage Consumption among Adolescents in Belgium

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study
2.2. Sampling
2.3. Measures
2.4. Statistical Analyses
2.4.1. Reprocessing Data
2.4.2. Modeling
3. Results
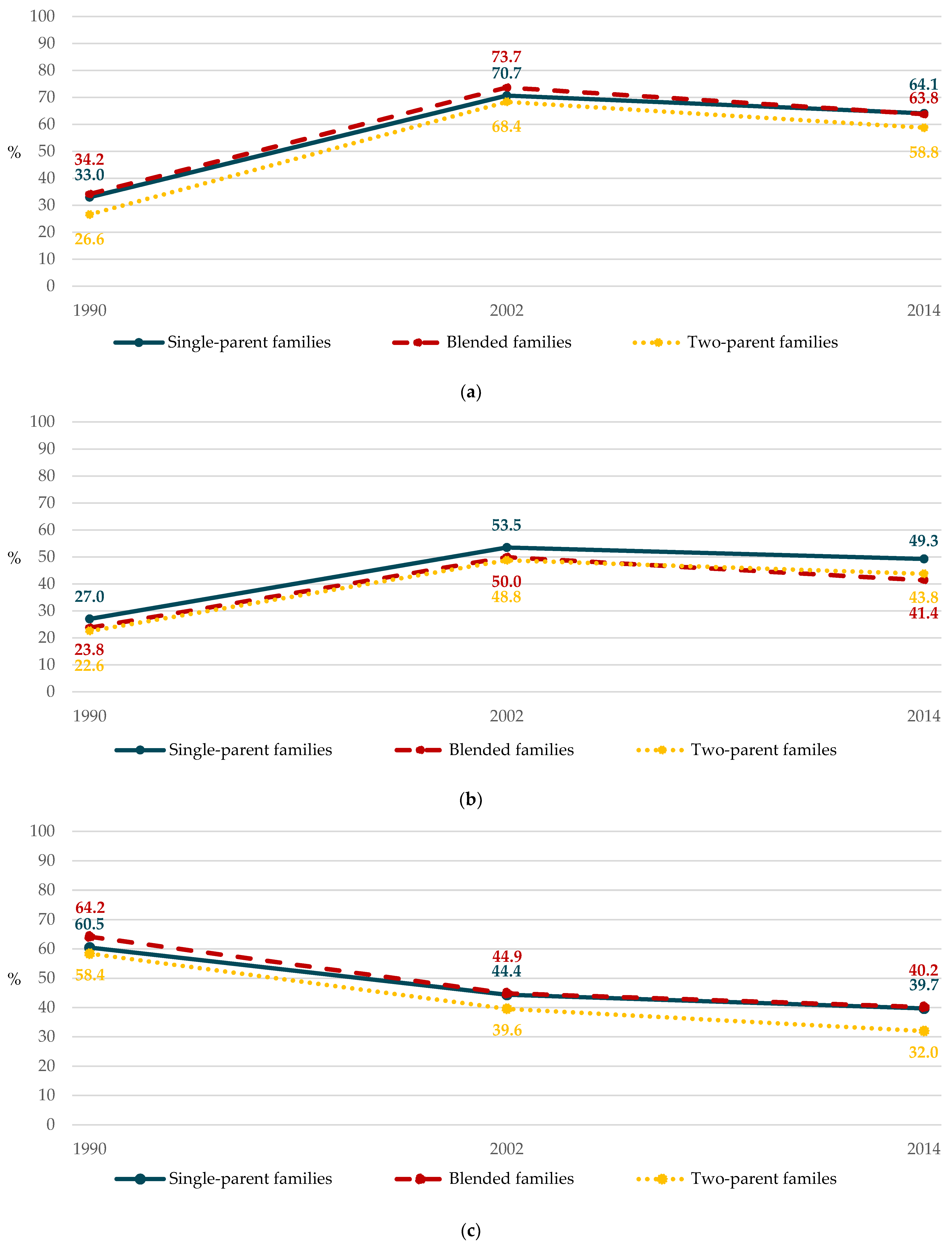
3.1. Disparities Related to the Family Structure
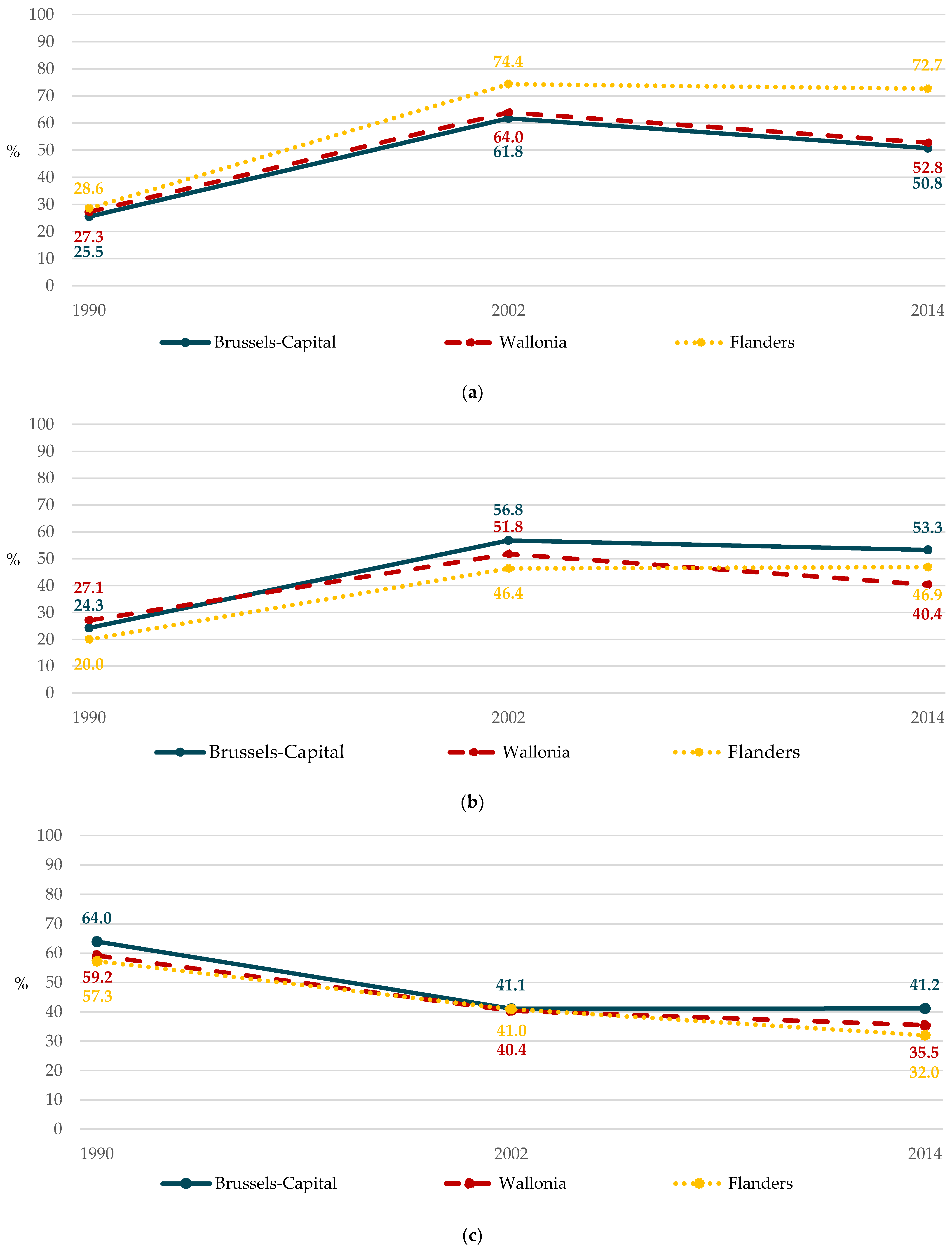
3.2. Disparities Related to the School Region
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dahlgren, G.; Whitehead, M. Policies and Strategies to Promote Social Equity in Health: Background Document to WHO—Strategy Paper for Europe; Institute for Futures Studies: Stockholm, Sweden, 1991; ISBN 978-91-85619-18-4. [Google Scholar]
- Baek, Y.J.; Paik, H.Y.; Shim, J.E. Association between family structure and food group intake in children. Nutr. Res. Pract. 2014, 8, 463–468. [Google Scholar] [CrossRef] [Green Version]
- Desbouys, L.; de Ridder, K.; Rouche, M.; Castetbon, K. Food consumption in adolescents and young adults: Age-specific socio-economic and cultural disparities (Belgian Food Consumption survey 2014). Nutrients 2019, 11, 1520. [Google Scholar] [CrossRef] [Green Version]
- Desbouys, L.; Méjean, C.; de Henauw, S.; Castetbon, K. Socio-economic and cultural disparities in diet among adolescents and young adults: A systematic review. Public Health Nutr. 2020, 23, 843–860. [Google Scholar] [CrossRef] [Green Version]
- Stewart, S.D.; Menning, C.L. Family structure, nonresident father involvement, and adolescent eating patterns. J. Adolesc. Health 2009, 45, 193–201. [Google Scholar] [CrossRef]
- Morris, M.A.; Hulme, C.; Clarke, G.P.; Edwards, K.L.; Cade, J.E. What is the cost of a healthy diet? Using diet data from the UK Women’s Cohort Study. J. Epidemiol. Community Health 2014, 68, 1043–1049. [Google Scholar] [CrossRef] [Green Version]
- Rouche, M.; de Clercq, B.; Lebacq, T.; Dierckens, M.; Moreau, N.; Desbouys, L.; Godin, I.; Castetbon, K. Socioeconomic disparities in diet vary according to migration status among adolescents in Belgium. Nutrients 2019, 11, 812. [Google Scholar] [CrossRef] [Green Version]
- Chatelan, A.; Beer-Borst, S.; Randriamiharisoa, A.; Pasquier, J.; Blanco, J.M.; Siegenthaler, S.; Paccaud, F.; Slimani, N.; Nicolas, G.; Camenzind-Frey, E.; et al. Major differences in diet across three linguistic regions of Switzerland: Results from the first national nutrition survey menuCH. Nutrients 2017, 9, 1163. [Google Scholar] [CrossRef] [PubMed]
- Census/Statbel. Population Par Lieu de Résidence (Province), sexe, Position Dans le Ménage (C), État Civil, Situation sur le Marché de L’emploi (A) et Lieu de Naissance (A) [Internet]. Available online: http://census2011.fgov.be/censusselection/selectionFR.html (accessed on 5 September 2019).
- Observatoire de la Santé et du Social de Bruxelles-Capitale. Baromètre Social 2018: Rapport Bruxellois Sur L’état de la Pauvreté, Bruxelles. Available online: https://www.ccc-ggc.brussels/sites/default/files/documents/graphics/rapport-pauvrete/barometre_social_2018.pdf (accessed on 5 September 2019).
- Lasater, G.; Piernas, C.; Popkin, B.M. Beverage patterns and trends among school-aged children in the US, 1989–2008. Nutr. J. 2011, 10, 103. [Google Scholar] [CrossRef] [Green Version]
- Mendez, M.A.; Miles, D.R.; Poti, J.M.; Sotres-Alvarez, D.; Popkin, B.M. Persistent disparities over time in the distribution of sugar-sweetened beverage intake among children in the United States. Am. J. Clin. Nutr. 2019, 109, 79–89. [Google Scholar] [CrossRef] [Green Version]
- Rose, G.A. The Strategy of Preventive Medicine; Oxford University Press: Oxford, UK, 1992; ISBN 0-19-262125-4. [Google Scholar]
- Lalonde, M. Nouvelle Perspective de la Santé des Canadiens: Un Document de Travail; Government of Canada: Ottawa, ON, Canada, 1974. Available online: http://www.phac-aspc.gc.ca/ph-sp/pdf/perspect-fra.pdf (accessed on 3 October 2019).
- Marmot, M.G.; Allen, J.; Goldblatt, P.; Boyce, T.; McNeish, D.; Grady, M.; Geddes, I. Fair Society, Healthy Lives: The Marmot Review; University College London: London, UK, 2010; ISBN 978-0-9564870-0-1. [Google Scholar]
- Organisation for Economic Co-operation and Development. Doing Better for Families; OECD Publishing: Paris, France, 2011; ISBN 978-92-64-09872-5. [Google Scholar]
- Health Behaviour in School-Aged Children. Fact Sheet—The HBSC Network. Available online: http://www.hbsc.org/publications/factsheets/Info%20sheet%202013-14%20(English).pdf (accessed on 6 December 2019).
- Vereecken, C.A.; Maes, L. A Belgian study on the reliability and relative validity of the Health Behaviour in School-Aged Children food-frequency questionnaire. Public Health Nutr. 2003, 6, 581–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Superior Health Council. Dietary Guidelines for the Belgian Adult Population; SHC: Brussels, Belgium, 2019; Available online: https://www.health.belgium.be/sites/default/files/uploads/fields/fpshealth_theme_file/20190902_shc-9284_fbdg_vweb.pdf (accessed on 19 June 2020).
- Uwawunkonye, E.G.; Anaene, O.I.C. A comparative study between ridit and modified ridit analysis. AJTAS 2013, 2, 248–254. [Google Scholar] [CrossRef]
- Sergeant, J.C.; Firth, D. Relative index of inequality: Definition, estimation, and inference. Biostatistics 2006, 7, 213–224. [Google Scholar] [CrossRef] [Green Version]
- Mackenbach, J.P.; Kunst, A.E. Measuring the magnitude of socio-economic inequalities in health: An overview of available measures illustrated with two examples from Europe. Soc. Sci. Med. 1997, 44, 757–771. [Google Scholar] [CrossRef]
- Moreno-Betancur, M.; Latouche, A.; Menvielle, G.; Kunst, A.E.; Rey, G. Relative index of inequality and slope index of inequality: A structured regression framework for estimation. Epidemiology 2015, 26, 518–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barros, A.J.D.; Hirakata, V.N. Alternatives for logistic regression in cross-sectional studies: An empirical comparison of models that directly estimate the prevalence ratio. BMC Med. Res. Methodol. 2003, 3, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ernstsen, L.; Strand, B.H.; Nilsen, S.M.; Espnes, G.A.; Krokstad, S. Trends in absolute and relative educational inequalities in four modifiable ischaemic heart disease risk factors: Repeated cross-sectional surveys from the Nord-Trøndelag Health Study (HUNT) 1984-2008. BMC Public Health 2012, 12, 266. [Google Scholar] [CrossRef] [Green Version]
- Kit, B.K.; Fakhouri, T.H.I.; Park, S.; Nielsen, S.J.; Ogden, C.L. Trends in sugar-sweetened beverage consumption among youth and adults in the United States: 1999–2010. Am. J. Clin. Nutr. 2013, 98, 180–188. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, M.; Krølner, R.; Svastisalee, C.M.; Due, P.; Holstein, B.E. Secular trends in fruit intake among Danish schoolchildren, 1988 to 2006: Changing habits or methodological artefacts? Int. J. Behav. Nutr. Phys. Act. 2008, 5, 6. [Google Scholar] [CrossRef] [Green Version]
- French, S.A.; Lin, B.-H.; Guthrie, J.F. National trends in soft drink consumption among children and adolescents age 6 to 17 years: Prevalence, amounts, and sources, 1977/1978 to 1994/1998. J. Am. Diet Assoc. 2003, 103, 1326–1331. [Google Scholar] [CrossRef]
- King, A.; Wold, B.; Tudor-Smith, C.; Harel, Y. The Health of Youth: A Cross-National Survey: A Report of the 1993-94 Survey Results of Health Behaviour in School-Aged Children; WHO Regional Publications; European Series; World Health Organization: Copenhague, Denmark, 1996; Available online: http://www.hbsc.org/documents/The%20Health%20of%20Youth%20A%20cross-national%20survey.pdf (accessed on 2 July 2019).
- Currie, C.; Roberts, C.; Morgan, A.; Smith, R.; Settertobulte, W.; Samdal, O.; Rasmussen, V.B. Young People’s Health in Context. Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2001/2002 Survey; Health Policy for Children and Adolescents No. 4; World Health Organization: Copenhaguen, Denmark, 2004; Available online: http://www.euro.who.int/__data/assets/pdf_file/0008/110231/e82923.pdf?ua=1 (accessed on 2 July 2019).
- Inchley, J.; Currie, D.; Young, T.; Samdal, O.; Torsheim, T.; Augustson, L.; Mathison, F.; Aleman-Diaz, A.Y.; Molcho, M.; Weber, M.W.; et al. Growing up Unequal: Gender and Socioeconomic Differences in Young People’s Health and Well-Being Health Behaviour in School-Aged Children (HBSC) Study International Report from the 2013/2014 Survey; Health Policy for Children and Adolescents; World Health Organization: Copenhagen, Denmark, 2016; Available online: http://www.euro.who.int/en/health-topics/Life-stages/child-and-adolescent-health/health-behaviour-in-school-aged-children-hbsc/hbsc-international-reports/growing-up-unequal.-hbsc-2016-study-20132014-survey (accessed on 2 July 2019).
- Krølner, R.; Rasmussen, M.; Brug, J.; Klepp, K.-I.; Wind, M.; Due, P. Determinants of fruit and vegetable consumption among children and adolescents: A review of the literature. Part II: Qualitative studies. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 112. [Google Scholar] [CrossRef] [Green Version]
- Ashfield-Watt, P.A.L.; Welch, A.A.; Godward, S.; Bingham, S.A. Effect of a pilot community intervention on fruit and vegetable intakes: Use of FACET (Five-a-day Community Evaluation Tool). Public Health Nutr. 2007, 10, 671–680. [Google Scholar] [CrossRef] [Green Version]
- Currie, C.; Hurrelmann, K.; Settertobulte, W.; Smith, R.; Todd, J. Health and Health Behaviour among Young People; Health Policy for Children and Adolescents No. 1; World Health Organization: Copenhagen, Denmark, 2000; Available online: http://www.euro.who.int/__data/assets/pdf_file/0006/119571/E67880.pdf (accessed on 2 July 2019).
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Lampousi, A.-M.; Knuppel, S.; Iqbal, K.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of all-cause mortality: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2017, 105, 1462–1473. [Google Scholar] [CrossRef] [Green Version]
- Imamura, F.; O’Connor, L.; Ye, Z.; Mursu, J.; Hayashino, Y.; Bhupathiraju, S.N.; Forouhi, N.G. Consumption of sugar sweetened beverages, artificially sweetened beverages, and fruit juice and incidence of type 2 diabetes: Systematic review, meta-analysis, and estimation of population attributable fraction. BMJ 2015, 351, h3576. [Google Scholar] [CrossRef] [Green Version]
- Bolt-Evensen, K.; Vik, F.N.; Stea, T.H.; Klepp, K.-I.; Bere, E. Consumption of sugar-sweetened beverages and artificially sweetened beverages from childhood to adulthood in relation to socioeconomic status—15 years follow-up in Norway. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torsheim, T.; Cavallo, F.; Levin, K.A.; Schnohr, C.; Mazur, J.; Niclasen, B.; Currie, C. Psychometric validation of the revised family affluence scale: A latent variable approach. Child Indic. Res. 2016, 9, 771–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkpatrick, S.I.; Dodd, K.W.; Reedy, J.; Krebs-Smith, S.M. Income and race/ethnicity are associated with adherence to food-based dietary guidance among US adults and children. J. Acad. Nutr. Diet 2012, 112, 624–635.e6. [Google Scholar] [CrossRef] [Green Version]
- Leider, J.; Powell, L.M. Sugar-sweetened beverage prices: Variations by beverage, food store, and neighborhood characteristics, 2017. Prev. Med. Rep. 2019, 15, 100883. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Family Structure | 1990 | 2002 | 2014 | P for Trend |
|---|---|---|---|---|
| Non-daily fruit consumption | ||||
| Single-parent family (%) | 33.0 | 70.7 | 64.1 | |
| Blended family (%) | 34.2 | 73.7 | 63.8 | |
| Two parents (%) | 26.6 | 68.4 | 58.8 | |
| cRII-F (95% CI) 1 | 1.56 (1.32–1.86) | 1.10 (1.06–1.14) | 1.17 (1.13–1.23) | 0.43 a |
| aRII-F (95% CI) 2 | 1.58 (1.33–1.88) | 1.15 (1.11–1.19) | 1.18 (1.13–1.23) | 0.007 a |
| cSII-F (95% CI) 1 | 13.37 (7.82–18.92) | 6.56 (4.10–9.02) | 9.91 (7.26–12.55) | <0.001 b |
| aSII-F (95% CI) 2 | 13.14 (7.59–18.70) | 9.53 (7.04–12.03) | 10.40 (7.72–13.08) | <0.001 b |
| Non-daily vegetable consumption | ||||
| Single-parent family (%) | 27.0 | 53.5 | 49.3 | |
| Blended family (%) | 23.8 | 50.0 | 41.4 | |
| Two parents (%) | 22.6 | 48.8 | 43.8 | |
| cRII-F (95% CI) 1 | 1.35 (1.10–1.66) | 1.14 (1.09–1.21) | 1.15 (1.08–1.22) | 0.26 a |
| aRII-F (95% CI) 2 | 1.30 (1.06–1.60) | 1.11 (1.06–1.17) | 1.16 (1.09–1.23) | 0.32 a |
| cSII-F (95% CI) 1 | 7.30 (2.08–12.51) | 6.80 (4.11–9.50) | 6.10 (3.42–8.78) | 0.68 a |
| aSII-F (95% CI) 2 | 6.74 (1.54–11.94) | 5.56 (2.84–8.28) | 6.81 (4.11–9.50) | 0.76 a |
| Daily sugar-sweetened beverage consumption | ||||
| Single-parent family (%) | 60.5 | 44.4 | 39.7 | |
| Blended family (%) | 64.2 | 44.9 | 40.2 | |
| Two parents (%) | 58.4 | 39.6 | 32.0 | |
| cRII-F (95% CI) 1 | 1.10 (1.00–1.21) | 1.26 (1.18–1.34) | 1.51 (1.41–1.62) | <0.001 a |
| aRII-F (95% CI) 2 | 1.08 (0.98–1.19) | 1.27 (1.19–1.35) | 1.47 (1.37–1.58) | <0.001 a |
| cSII-F (95% CI) 1 | 5.87 (0.00–11.74) | 9.70 (7.00–12.40) | 15.05 (12.39–17.72) | 0.001 a |
| aSII-F (95% CI) 2 | 4.80 (−1.11–10.70) | 10.10 (7.41–12.80) | 14.34 (11.68–17.00) | 0.002 a |
| School Region | 1990 | 2002 | 2014 | P for Trend |
|---|---|---|---|---|
| Non-daily fruit consumption | ||||
| Brussels-Capital (%) | 25.5 | 61.8 | 50.8 | |
| Wallonia (%) | 27.3 | 64.0 | 52.8 | |
| Flanders (%) | 28.6 | 74.4 | 72.7 | |
| cRII-F (95% CI) 1 | 0.87 (0.76–0.99) | 0.74 (0.71–0.76) | 0.54 (0.52–0.57) | <0.001 a |
| aRII-F (95% CI) 2 | 0.83 (0.73–0.96) | 0.73 (0.71–0.76) | 0.55 (0.52–0.57) | <0.001 a |
| cSII-F (95% CI) 1 | −3.92 (−7.67–−0.17) | −20.75 (−22.76–−18.73) | −34.84 (−37.15–−32.53) | <0.001 a |
| aSII-F (95% CI) 2 | −4.19 (−7.94–−0.45) | −20.71 (−22.76–−18.67) | −34.68 (−37.03–−32.33) | <0.001 a |
| Non-daily vegetable consumption | ||||
| Brussels-Capital (%) | 24.3 | 56.8 | 53.3 | |
| Wallonia (%) | 27.1 | 51.8 | 40.4 | |
| Flanders (%) | 20.0 | 46.4 | 46.9 | |
| cRII-F (95% CI) 1 | 1.57 (1.35–1.82) | 1.31 (1.25–1.37) | 0.97 (0.91–1.02) | <0.001 a |
| aRII-F (95% CI) 2 | 1.55 (1.33–1.80) | 1.29 (1.23–1.34) | 0.99 (0.93–1.05) | <0.001 a |
| cSII-F (95% CI) 1 | 11.07 (7.39–14.76) | 13.43 (11.24–15.62) | −1.44 (−3.79–0.91) | <0.001 a |
| aSII-F (95% CI) 2 | 11.38 (7.65–15.10) | 12.65 (10.44–14.87) | −0.38 (−2.75–1.98) | <0.001 a |
| Daily sugar-sweetened beverage consumption | ||||
| Brussels-Capital (%) | 64.0 | 41.1 | 41.2 | |
| Wallonia (%) | 59.2 | 40.4 | 35.5 | |
| Flanders (%) | 57.3 | 41.0 | 32.0 | |
| cRII-F (95% CI) 1 | 1.13 (1.06–1.22) | 0.99 (0.94–1.04) | 1.35 (1.26–1.45) | <0.001 b |
| aRII-F (95% CI) 2 | 1.15 (1.07–1.23) | 0.99 (0.94–1.04) | 1.37 (1.28–1.47) | <0.001 b |
| cSII-F (95% CI) 1 | 7.41 (3.32–11.49) | −0.55 (−2.72–1.62) | 10.27 (7.89–12.66) | <0.001 b |
| aSII-F (95% CI) 2 | 8.13 (4.00–12.26) | 1.13 (−1.05–3.31) | 11.03 (8.65–13.40) | <0.001 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rouche, M.; Dierckens, M.; Desbouys, L.; Pedroni, C.; Lebacq, T.; Godin, I.; Deforche, B.; Castetbon, K. Twenty-Four-Year Trends in Family and Regional Disparities in Fruit, Vegetable and Sugar-Sweetened Beverage Consumption among Adolescents in Belgium. Int. J. Environ. Res. Public Health 2021, 18, 4408. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094408
Rouche M, Dierckens M, Desbouys L, Pedroni C, Lebacq T, Godin I, Deforche B, Castetbon K. Twenty-Four-Year Trends in Family and Regional Disparities in Fruit, Vegetable and Sugar-Sweetened Beverage Consumption among Adolescents in Belgium. International Journal of Environmental Research and Public Health. 2021; 18(9):4408. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094408
Chicago/Turabian StyleRouche, Manon, Maxim Dierckens, Lucille Desbouys, Camille Pedroni, Thérésa Lebacq, Isabelle Godin, Benedicte Deforche, and Katia Castetbon. 2021. "Twenty-Four-Year Trends in Family and Regional Disparities in Fruit, Vegetable and Sugar-Sweetened Beverage Consumption among Adolescents in Belgium" International Journal of Environmental Research and Public Health 18, no. 9: 4408. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094408