
Gait Speed as a Predictor for Diabetes Incidence in People with or at Risk of Knee Osteoarthritis: A Longitudinal Analysis from the Osteoarthritis Initiative

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
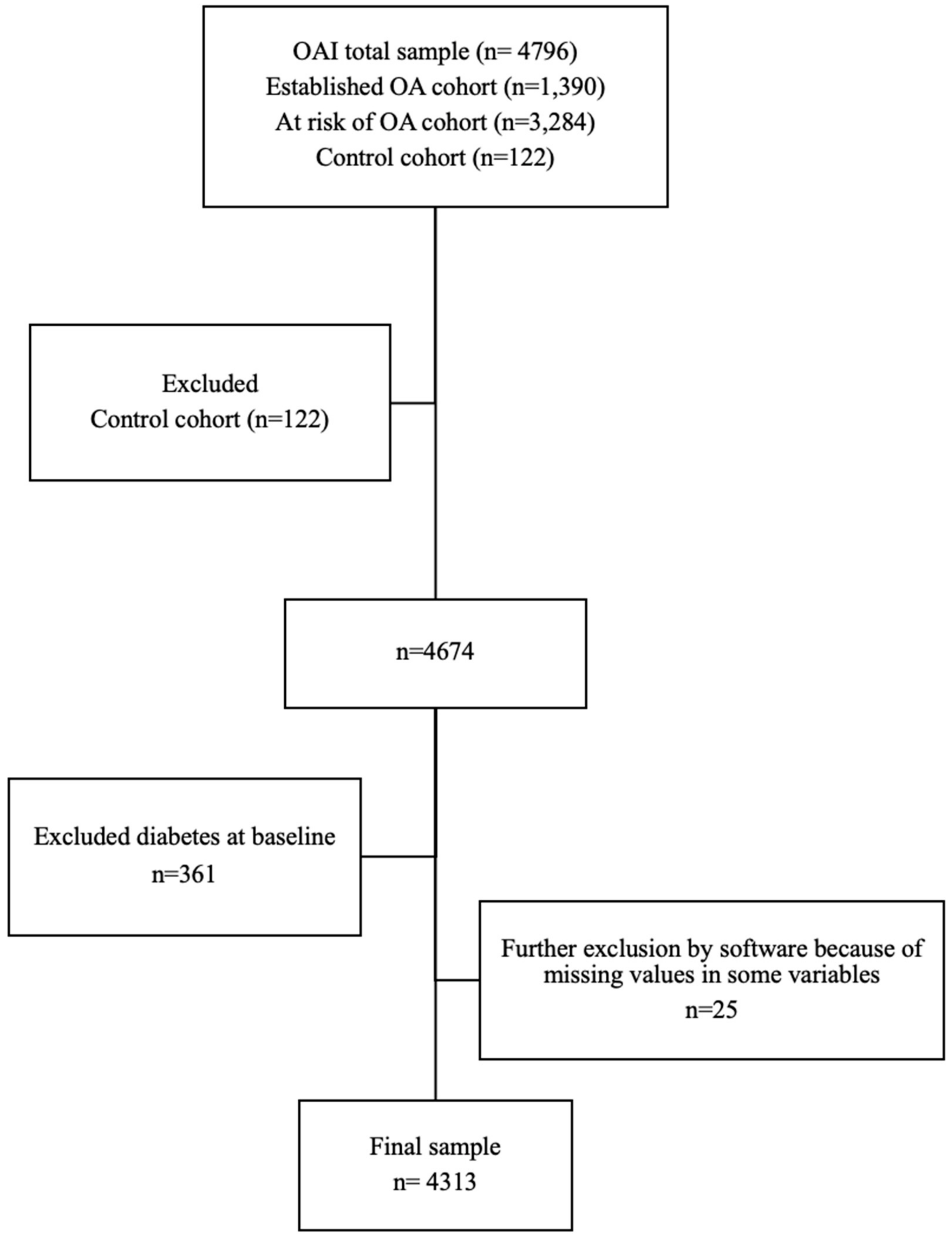
2.1. Cohort Selection
2.2. Outcome Measures
2.3. Exposure Group
2.4. Confounders
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lawrence, R.C.; Felson, D.T.; Helmick, C.G.; Arnold, L.M.; Choi, H.; Deyo, R.A.; Gabriel, S.; Hirsch, R.; Hochberg, M.C.; Hunder, G.G.; et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part II. Arthritis Rheum. 2007, 58, 26–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auchincloss, A.H.; Roux, A.V.D.; Mujahid, M.S.; Shen, M.; Bertoni, A.G.; Carnethon, M.R. Neighborhood resources for physical activity and healthy foods and incidence of type 2 diabetes mellitus: The Multi-Ethnic study of Atherosclerosis. Arch. Intern. Med. 2009, 169, 1698–1704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piva, S.R.; Susko, A.M.; Khoja, S.S.; Josbeno, D.A.; Fitzgerald, G.K.; Toledo, F.G. Links between osteoarthritis and diabetes: Implications for management from a physical activity perspective. Clin. Geriatr. Med. 2015, 3, 67–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolen, J.; Murphy, L.; Greenlund, K.; Helmick, C.G.; Hootman, J.; Brady, T.J.; Langmaid, G.; Keenan, N. Arthritis as a potential barrier to physical activity among adults with heart disease-United States, 2005 and 2007. Morb. Mortal. Wkly. Rep. 2009, 58, 165–169. [Google Scholar]
- Lane, N.E.; Ivanova, J.; Emir, B.; Mobasheri, A.; Jensen, M.G. Characterization of individuals with osteoarthritis in the United States and their use of prescription and over-the-counter supplements. Maturitas 2021, 145, 24–30. [Google Scholar] [CrossRef]
- CDC. New CDC Report: More than 100 Million Americans Have Diabetes or Prediabetes; CDC: Atlanta, GA, USA, 2017.
- Volpato, S.; Maraldi, C.; Fellin, R. Type 2 diabetes and risk for functional decline and disability in older persons. Curr. Diabetes Rev. 2010, 6, 134–143. [Google Scholar] [CrossRef]
- McDaniel, G.; Renner, J.B.; Sloane, R.; Kraus, V.B. Association of knee and ankle osteoarthritis with physical performance. Osteoarthr. Cartil. 2011, 19, 634–638. [Google Scholar] [CrossRef] [Green Version]
- Guralnik, J.M.; Ferrucci, L.; Simonsick, E.M.; Salive, M.E.; Wallace, R.B. Lower-Extremity Function in Persons over the Age of 70 Years as a Predictor of Subsequent Disability. N. Engl. J. Med. 1995, 332, 556–562. [Google Scholar] [CrossRef] [Green Version]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait speed and survival in older adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Yates, T.; Zaccardi, F.; Dhalwani, N.N.; Davies, M.J.; Bakrania, K.; Celis-Morales, C.A.; Gill, J.M.R.; Franks, P.W.; Khunti, K. Association of walking pace and handgrip strength with all-cause, cardiovascular, and cancer mortality: A UK Biobank observational study. Eur. Hearth J. 2017, 38, 3232–3240. [Google Scholar] [CrossRef]
- Fritz, S.; Lusardi, M. White paper: “walking speed: The sixth vital sign”. J. Geriatr. Phys. Ther. 2009, 32, 46–49. [Google Scholar] [CrossRef] [Green Version]
- Castell, M.-V.; Sánchez, M.; Julián, R.; Queipo, R.; Martín, S.; Otero, Á. Frailty prevalence and slow walking speed in persons age 65 and older: Implications for primary care. BMC Fam. Pract. 2013, 14, 86. [Google Scholar] [CrossRef] [Green Version]
- Montero-Odasso, M.; Schapira, M.; Soriano, E.R.; Varela, M.; Kaplan, R.; Camera, L.A.; Mayorga, L.M. Gait Velocity as a Single Predictor of Adverse Events in Healthy Seniors Aged 75 Years and Older. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2005, 60, 1304–1309. [Google Scholar] [CrossRef] [Green Version]
- Inzitari, M.; Newman, A.B.; Yaffe, K.; Boudreau, R.; De Rekeneire, N.; Shorr, R.; Harris, T.B.; Rosano, C. Gait Speed Predicts Decline in Attention and Psychomotor Speed in Older Adults: The Health Aging and Body Composition Study. Neuroepidemiology 2007, 29, 156–162. [Google Scholar] [CrossRef] [Green Version]
- Kera, T.; Kawai, H.; Hirano, H.; Kojima, M.; Watanabe, Y.; Fujiwara, Y.; Ihara, K.; Obuchi, S. Comparison of body composition and physical and cognitive function between older Japanese adults with no diabetes, prediabetes and diabetes: A cross-sectional study in community-dwelling Japanese older people. Geriatr. Gerontol. Int. 2018, 18, 1031–1037. [Google Scholar] [CrossRef]
- Vennu, V.; Misra, H. Evaluation of gait speed over time in adults with arthritis: Data from the osteoarthritis initiative. Indian J. Rheumatol. 2018, 13, 154. [Google Scholar] [CrossRef]
- Jiang, L.; Rong, J.; Wang, Y.; Hu, F.; Bao, C.; Li, X.; Zhao, Y. The relationship between body mass index and hip osteoarthritis: A systematic review and meta-analysis. Jt. Bone Spine 2011, 78, 150–155. [Google Scholar] [CrossRef]
- Jiang, L.; Tian, W.; Wang, Y.; Rong, J.; Bao, C.; Liu, Y.; Zhao, Y.; Wang, C. Body mass index and susceptibility to knee osteoarthritis: A systematic review and meta-analysis. Jt. Bone Spine 2012, 79, 291–297. [Google Scholar] [CrossRef]
- Reijman, M.; Pols, H.; Bergink, A.; Hazes, J.; Belo, J.; Lievense, A.; Bierma-Zeinstra, S. Body mass index associated with onset and progression of osteoarthritis of the knee but not of the hip: The Rotterdam Study. Ann. Rheum. Dis. 2006, 66, 158–162. [Google Scholar] [CrossRef] [Green Version]
- Alenazi, A.M.; AlShehri, M.M.; Alothman, S.; Alqahtani, B.; Rucker, J.; Sharma, N.K.; Bindawas, S.M.; Kluding, P.M. The Association of Diabetes with Knee Pain Locations, Pain While Walking, and Walking Speed: Data from the Osteoarthritis Initiative. Phys. Ther. 2020, 100, 1977–1986. [Google Scholar] [CrossRef]
- Louati, K.; Vidal, C.; Berenbaum, F.; Sellam, J. Association between diabetes mellitus and osteoarthritis: Systematic literature review and meta-analysis. RMD Open 2015, 1, e000077. [Google Scholar] [CrossRef]
- Boeckxstaens, P.; Peersman, W.; Goubin, G.; Ghali, S.; De Maeseneer, J.; Brusselle, G.; De Sutter, A. A practice-based analysis of combinations of diseases in patients aged 65 or older in primary care. BMC Fam. Pract. 2014, 15, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alenazi, A.M.; Alothman, S.; AlShehri, M.M.; Rucker, J.; Waitman, L.R.; Wick, J.; Sharma, N.K.; Kluding, P.M. The prevalence of type 2 diabetes and associated risk factors with generalized osteoarthritis: A retrospective study using ICD codes for clinical data repository system. Clin. Rheumatol. 2019, 38, 3539–3547. [Google Scholar] [CrossRef]
- Rahman, M.M.; Cibere, J.; Anis, A.H.; Goldsmith, C.H.; Kopec, J.A. Risk of Type 2 Diabetes among Osteoarthritis Patients in a Prospective Longitudinal Study. Int. J. Rheumatol. 2014, 2014, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Kendzerska, T.; King, L.K.; Lipscombe, L.; Croxford, R.; Stanaitis, I.; Hawker, G.A. The impact of hip and knee osteoarthritis on the subsequent risk of incident diabetes: A population-based cohort study. Diabetologia 2018, 61, 2290–2299. [Google Scholar] [CrossRef] [Green Version]
- Jylhä, M.; Guralnik, J.M.; Balfour, J.; Fried, L.P. Walking difficulty, walking speed, and age as predictors of self-rated health: The women’s health and aging study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M609–M617. [Google Scholar] [CrossRef] [Green Version]
- Perera, S.; Patel, K.V.; Rosano, C.; Rubin, S.M.; Satterfield, S.; Harris, T.; Ensrud, K.; Orwoll, E.; Lee, C.G.; Chandler, J.M.; et al. Gait Speed Predicts Incident Disability: A Pooled Analysis. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2016, 71, 63–71. [Google Scholar] [CrossRef]
- Alenazi, A.M.; Alshehri, M.M.; Alothman, S.; Gray, C.; Yahya, A.A.; Rucker, J.; Alqahtani, B.A.; Bindawas, S.M.; Kluding, P.M. Diabetes is Associated with Slow Walking Speed in People with Knee Osteoarthritis: 91: Board #7 May 29 9:30 AM–11:30 AM. Med. Sci. Sports Exerc. 2019, 51, 13. [Google Scholar]
- Nakanishi, S.; Takezawa, G.; Taooka, Y.; Kikkawa, K.; Matsumoto, N.; Hidaka, T. Gait speed may predict development of Type 2 diabetes: A pilot study among elderly Japanese. J. Diabetes Mellit. 2014, 4, 38–43. [Google Scholar] [CrossRef] [Green Version]
- Eitner, A.; Pester, J.; Vogel, F.; Marintschev, I.; Lehmann, T.; Hofmann, G.O.; Schaible, H.-G. Pain sensation in human osteoarthritic knee joints is strongly enhanced by diabetes mellitus. Pain 2017, 158, 1743–1753. [Google Scholar] [CrossRef]
- Alenazi, A.M.; AlShehri, M.M.; Alothman, S.; Alqahtani, B.A.; Rucker, J.; Sharma, N.; Segal, N.A.; Bindawas, S.M.; Kluding, P.M. The Association of Diabetes with Knee Pain Severity and Distribution in People with Knee Osteoarthritis using Data from the Osteoarthritis Initiative. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Charen, D.A.; Solomon, D.; Zubizarreta, N.; Poeran, J.; Colvin, A.C. Examining the Association of Knee Pain with Modifiable Cardiometabolic Risk Factors. Arthritis Rheum. 2020. [Google Scholar] [CrossRef] [PubMed]
- Eitner, A.; Culvenor, A.G.; Wirth, W.; Schaible, H.; Eckstein, F. Impact of Diabetes Mellitus on Knee Osteoarthritis Pain and Physical and Mental Status: Data from the Osteoarthritis Initiative. Arthritis Rheum. 2021, 73, 540–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alenazi, A.M.; Obaidat, S.M.; AlShehri, M.M.; Alothman, S.; Gray, C.; Rucker, J.; Waitman, L.R.; Kluding, P.M. Type 2 Diabetes Affects Joint Pain Severity in People with Localized Osteoarthritis: A Retrospective Study. Pain Med. 2019, 21, 1025–1031. [Google Scholar] [CrossRef]
- Schneider, A.L.C.; Pankow, J.S.; Heiss, G.; Selvin, E. Validity and Reliability of Self-reported Diabetes in the Atherosclerosis Risk in Communities Study. Am. J. Epidemiol. 2012, 176, 738–743. [Google Scholar] [CrossRef] [Green Version]
- Margolis, K.L.; Lihong, Q.; Brzyski, R.; Bonds, D.E.; Howard, B.V.; Kempainen, S.; Liu, S.; Robinson, J.G.; Safford, M.M.; Tinker, L.T.; et al. Validity of diabetes self-reports in the Women’s Health Initiative: Comparison with medication inventories and fasting glucose measurements. Clin Trials 2008, 5, 240–247. [Google Scholar] [CrossRef] [Green Version]
- Motyl, J.M.; Driban, J.B.; McAdams, E.; Price, L.L.; McAlindon, T.E. Test-retest reliability and sensitivity of the 20-meter walk test among patients with knee osteoarthritis. BMC Musculoskelet. Disord. 2013, 14, 166. [Google Scholar] [CrossRef] [Green Version]
- Twisk, J.W.R.; Smidt, N.; de Vente, W. Applied analysis of recurrent events: A practical overview. J. Epidemiol. Community Health 2005, 59, 706–710. [Google Scholar] [CrossRef] [Green Version]
- Twisk, J.; de Vente, W. Attrition in longitudinal studies: How to deal with missing data. J. Clin. Epidemiol. 2002, 55, 329–337. [Google Scholar] [CrossRef]
- Williams, A.; Kamper, S.J.; Wiggers, J.H.; O’Brien, K.M.; Lee, H.; Wolfenden, L.; Yoong, S.L.; Robson, E.; McAuley, J.H.; Hartvigsen, J.; et al. Musculoskeletal conditions may increase the risk of chronic disease: A systematic review and meta-analysis of cohort studies. BMC Med. 2018, 16, 1–9. [Google Scholar] [CrossRef]
- Alenazi, A.M.; Alshehri, M.M.; Alqahtani, B.A.; Alanazi, A.D.; Bindawas, S.M. Combined diabetes and arthritis are associated with declined gait speed. Clin. Rheumatol. 2021, 40, 1593–1598. [Google Scholar] [CrossRef] [PubMed]
- Dubey, N.K.; Ningrum, D.N.A.; Dubey, R.; Deng, Y.-H.; Li, Y.-C.; Wang, P.D.; Wang, J.R.; Syed-Abdul, S.; Deng, W.-P. Correlation between Diabetes Mellitus and Knee Osteoarthritis: A Dry-To-Wet Lab Approach. Int. J. Mol. Sci. 2018, 19, 3021. [Google Scholar] [CrossRef] [Green Version]
- Shirinsky, I.V.; Shirinsky, V.S. Effects of medication-treated diabetes on incidence and progression of knee osteoarthritis: A longitudinal analysis of the Osteoarthritis Initiative data. Rheumatol. Int. 2017, 37, 983–991. [Google Scholar] [CrossRef]
- Eymard, F.; Parsons, C.; Edwards, M.; Petit-Dop, F.; Reginster, J.-Y.; Bruyère, O.; Richette, P.; Cooper, C.; Chevalier, X. Diabetes is a risk factor for knee osteoarthritis progression. Osteoarthr. Cartil. 2015, 23, 851–859. [Google Scholar] [CrossRef] [Green Version]
- Nieves-Plaza, M.; Castro-Santana, L.E.; Font, Y.M.; Mayor, A.M.; Vilá, L.M. Association of Hand or Knee Osteoarthritis with Diabetes Mellitus in a Population of Hispanics From Puerto Rico. J. Clin. Rheumatol. 2013, 19, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Al-Jarallah, K.; Shehab, D.; Abdella, N.; Al Mohamedy, H.; Abraham, M. Knee Osteoarthritis in Type 2 Diabetes Mellitus: Does Insulin Therapy Retard Osteophyte Formation? Med. Princip. Pract. 2015, 25, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Eymard, F.; Parsons, C.; Edwards, M.H.; Petit-Dop, F.; Reginster, J.-Y.; Bruyère, O.; Chevalier, X.; Cooper, C.; Richette, P. Statin use and knee osteoarthritis progression: Results from a post-hoc analysis of the SEKOIA trial. Jt. Bone Spine 2018, 85, 609–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Driban, J.B.; Lo, G.H.; Eaton, C.B.; Lapane, K.L.; Nevitt, M.; Harvey, W.F.; McCulloch, C.E.; McAlindon, T.E. Exploratory analysis of osteoarthritis progression among medication users: Data from the Osteoarthritis Initiative. Ther. Adv. Musculoskelet. Dis. 2016, 8, 207–219. [Google Scholar] [CrossRef] [Green Version]
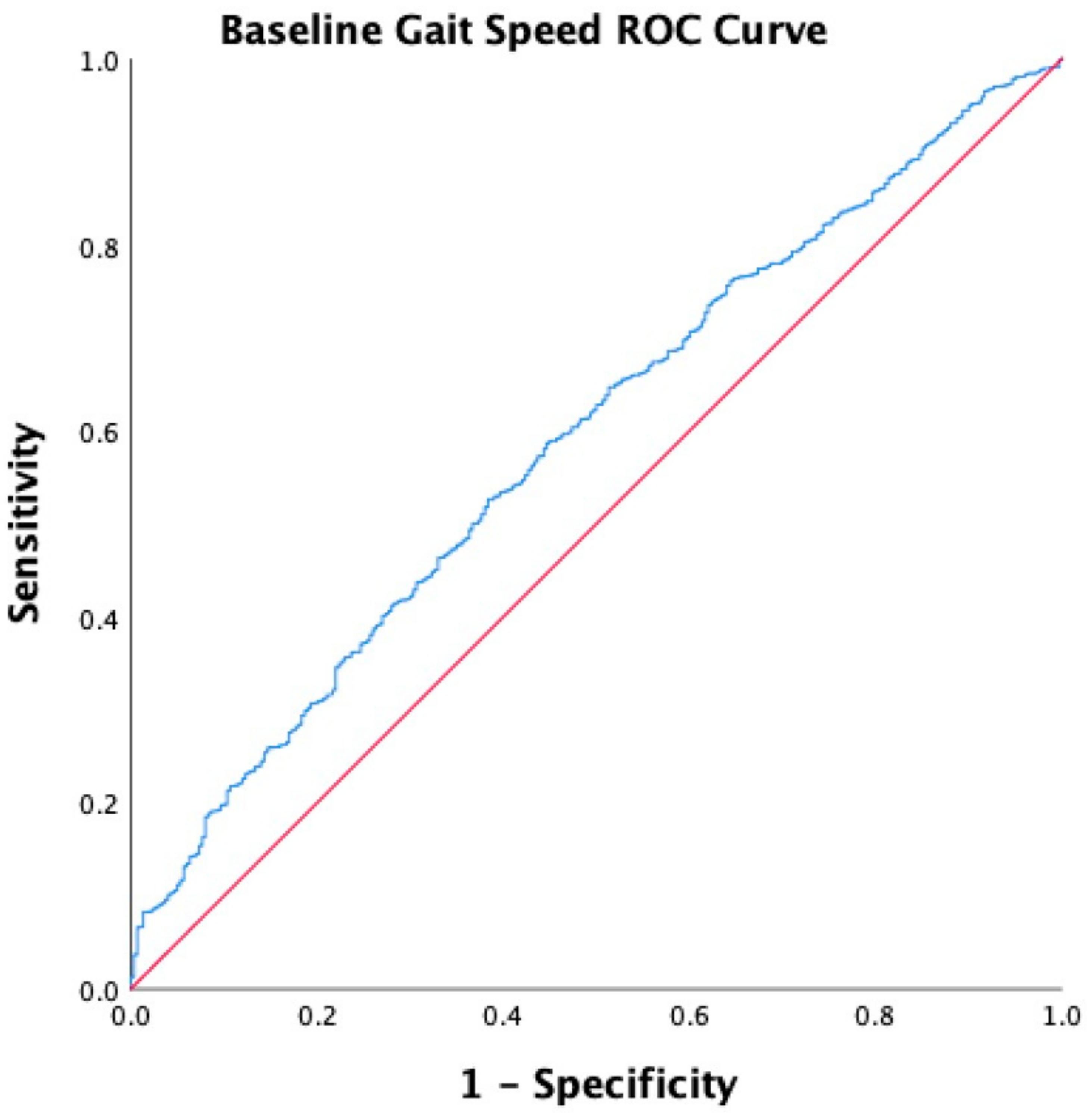
- Mandrekar, J.N. Receiver Operating Characteristic Curve in Diagnostic Test Assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef] [Green Version]
- Langlois, J.A.; Keyl, P.M.; Guralnik, J.M.; Foley, D.J.; Marottoli, R.A.; Wallace, R.B. Characteristics of older pedestrians who have difficulty crossing the street. Am. J. Public Health 1997, 87, 393–397. [Google Scholar] [CrossRef] [Green Version]
- Andrews, A.W.; Chinworth, S.A.; Bourassa, M.; Garvin, M.; Benton, D.; Tanner, S. Update on distance and velocity requirements for community ambulation. J. Geriatr. Phys. Ther. 2010, 33, 128–134. [Google Scholar]
- Van Kan, G.A.; Rolland, Y.; Andrieu, S.; Bauer, J.; Beauchet, O.; Bonnefoy, M.; Cesari, M.; Donini, L.M.; Gillette-Guyonnet, S.; Inzitari, M.; et al. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. J. Nutr. Health Aging 2009, 13, 881–889. [Google Scholar] [CrossRef]
- White, D.K.; Niu, J.; Zhang, Y. Is symptomatic knee osteoarthritis a risk factor for a trajectory of fast decline in gait speed? Results from a longitudinal cohort study. Arthritis Rheum. 2013, 65, 187–194. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total Sample (N = 4313) |
|---|---|
| Age categories | |
| <55 years, n (%) | 1395 (32.3) |
| 56–65 years, n (%) | 1413 (32.8) |
| 66–75 years, n (%) | 1213 (28.1) |
| >76 years, n (%) | 292 (6.8) |
| Sex, female, n (%) | 2532 (58.7) |
| Race | |
| White, n (%) | 3469 (80.4) |
| African American, n (%) | 735 (17.0) |
| Asian, n (%) | 34 (0.8) |
| Others, n (%) | 70 (1.6) |
| Missing, n (%) | 5 (0.1) |
| Number of comorbidities | |
| None, n (%) | 3404 (78.9) |
| One, n (%) | 543 (12.6) |
| Two, n (%) | 227 (5.3) |
| Three or more, n (%) | 77 (1.8) |
| Missing, n (%) | 62 (1.4) |
| Baseline Body Mass Index, mean (SD) | 28.5 (4.8) |
| Kellgren and Lawrence grade | |
| Grade 0, n (%) | 1110 (25.7) |
| Grade 1, n (%) | 624 (14.5) |
| Grade 2, n (%) | 1249 (29.0) |
| Grade 3, n (%) | 808 (18.7) |
| Grade 4, n (%) | 266 (6.2) |
| Missing, n (%) | 256 (5.9) |
| Sub-cohort assignment | |
| At risk of knee OA cohort, n (%) | 3074 (71.3) |
| Established knee OA cohort, n (%) | 1239 (28.7) |
| Gait speed, m/s, mean (SD) | 1.32 (0.21) |
| Cumulative Incidence Time | Study Sample N = 4288 Participants with Incident DM, N (%) |
|---|---|
| At 24 months | 95 (2.2) |
| At 48 months | 181 (4.2) |
| At 96 months | 301 (7.0) |
| N | RR [95% CI] | p-Value | |
|---|---|---|---|
| Model 1 | 4274 | 0.21 [0.13, 0.35] | <0.001 |
| Model 2 | 3983 | 0.24 [0.13, 0.44] | <0.001 |
| Model 3 | 3983 | 0.44 [0.22, 0.86] | 0.018 |
| N | RR [95% CI] | p-Value | |
|---|---|---|---|
| Model 1 | 4274 | 1.77 [1.39, 2.26] | <0.001 |
| Model 2 | 3983 | 1.70 [1.29, 2.23] | <0.001 |
| Model 3 | 3983 | 1.35 [1.01, 1.79] | 0.042 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alenazi, A.M.; Alqahtani, B.A.; Vennu, V.; Alshehri, M.M.; Alanazi, A.D.; Alrawaili, S.M.; Khunti, K.; Segal, N.A.; Bindawas, S.M. Gait Speed as a Predictor for Diabetes Incidence in People with or at Risk of Knee Osteoarthritis: A Longitudinal Analysis from the Osteoarthritis Initiative. Int. J. Environ. Res. Public Health 2021, 18, 4414. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094414
Alenazi AM, Alqahtani BA, Vennu V, Alshehri MM, Alanazi AD, Alrawaili SM, Khunti K, Segal NA, Bindawas SM. Gait Speed as a Predictor for Diabetes Incidence in People with or at Risk of Knee Osteoarthritis: A Longitudinal Analysis from the Osteoarthritis Initiative. International Journal of Environmental Research and Public Health. 2021; 18(9):4414. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094414
Chicago/Turabian StyleAlenazi, Aqeel M., Bader A. Alqahtani, Vishal Vennu, Mohammed M. Alshehri, Ahmad D. Alanazi, Saud M. Alrawaili, Kamlesh Khunti, Neil A. Segal, and Saad M. Bindawas. 2021. "Gait Speed as a Predictor for Diabetes Incidence in People with or at Risk of Knee Osteoarthritis: A Longitudinal Analysis from the Osteoarthritis Initiative" International Journal of Environmental Research and Public Health 18, no. 9: 4414. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094414