
Assessing the Feasibility of Providing a Family Skills Intervention, “Strong Families”, for Refugee Families Residing in Reception Centers in Serbia †



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedures
2.2. Confidentiality and Ethical Considerations
2.3. Data Collection
2.4. Data Analysis
2.5. Program Intervention
3. Results
3.1. Quantitative Data Results
3.1.1. Demographic Results
3.1.2. SDQ Results
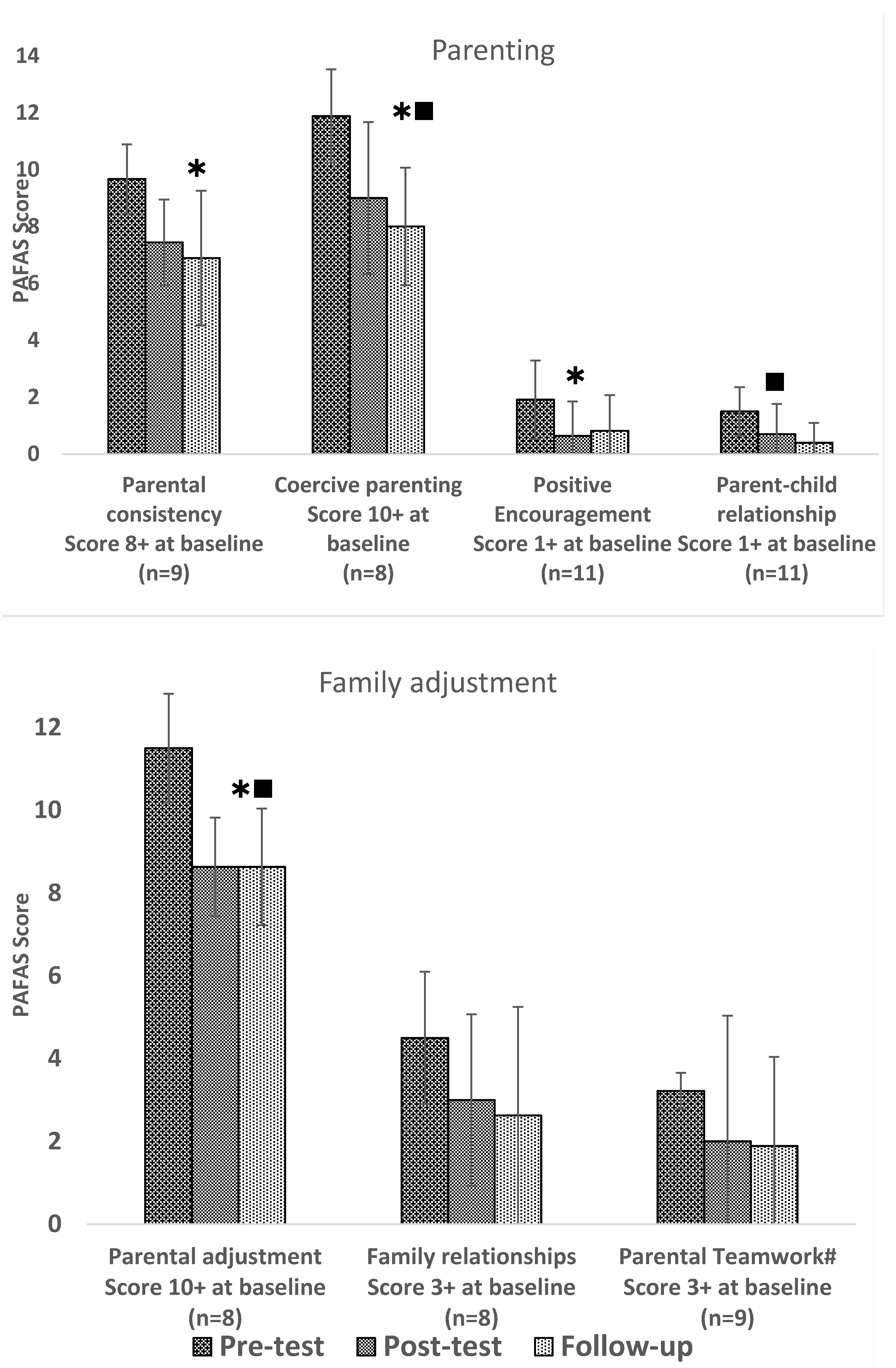
3.1.3. PAFAS Results
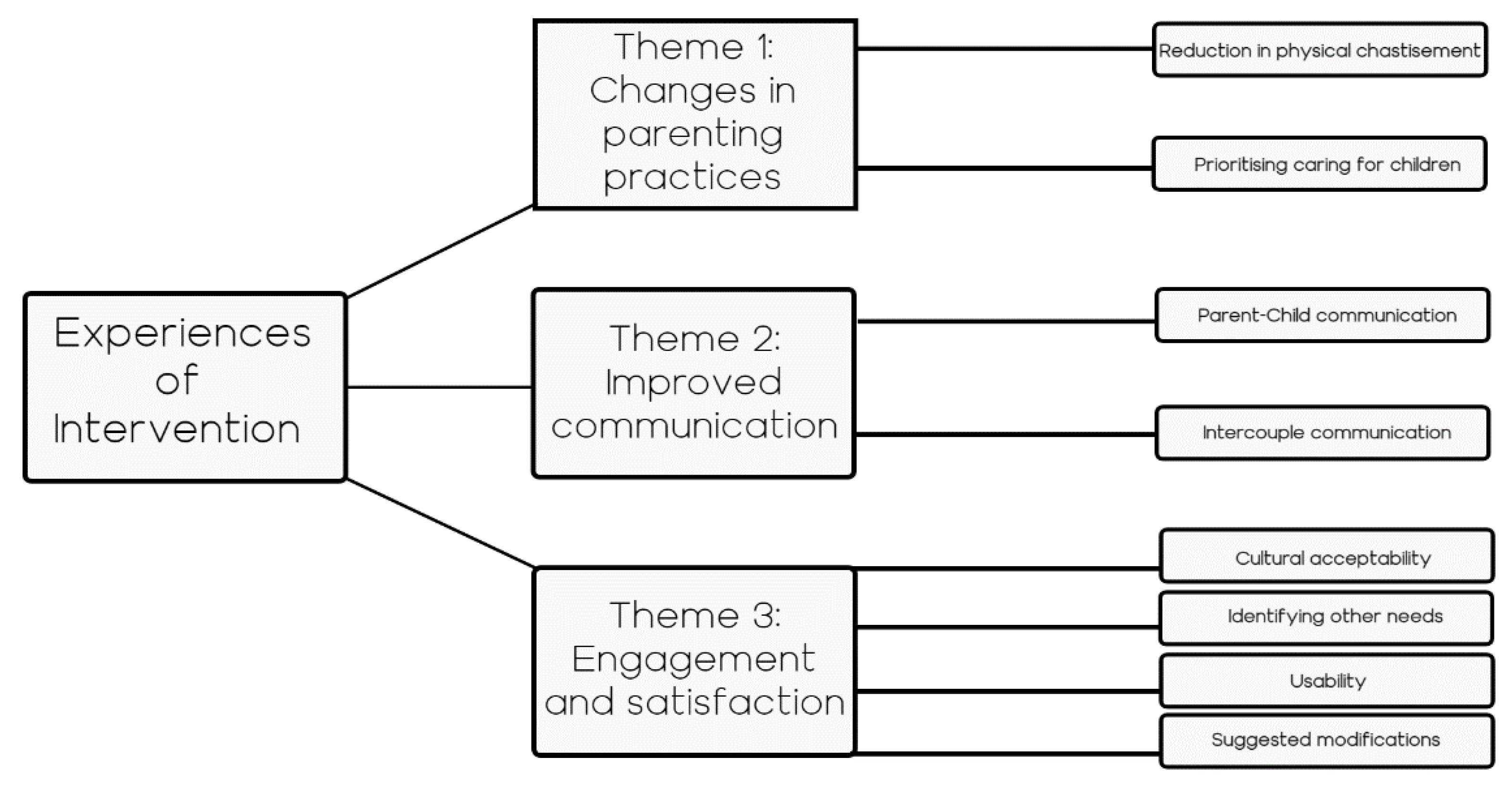
3.2. Qualitative Data Results
“I was always angry at what they were doing, thinking they did something serious. But now I see it differently, so I act differently”.(C3)
“To tell the truth I used to beat them every day, now I don’t do that anymore, I try to verbalize it, not start hitting them immediately. That’s different. I also get a better effect from them this way”.(C2)
“It helped me and other people, because sometimes people would want to hit their kids, they used to hit them before, but this program has helped us behave in a different way. It’s hard in this camp and then we get angry, I would slap the kids a little before, but now it’s better”.(C8)
“I can now control myself better. When I am angry I tell myself ‘I must not behave this way’, and then I behave much better. I learnt to control myself…and actually they listen more, they listen well”.(C4)
“I learnt about the kids for example to help [them] more, listen to them more, hear them out, hear what they say, control myself more, have more self-control. This feels very good and makes me happy and them happy too”.(C8)
“We had a lot of trouble along the way, so that we forgot we were mothers, then we lost that feeling, the feeling of being a mother. Now I remember again. I know how I should act with my children. As a mother, to be a real mother again”.(C7)
“The parents are really busy thinking about what they will do next [their future], and then maybe at some point the children end up in the background. I think that in this way [taking part in the intervention], the children were put to the foreground a bit and I think the children liked it. I think it gave them importance”.(F4)
“In our country there has always been war, we never had the opportunity to think about things like this. No one even asked us about our children or told us how to act with them”.(C2)
“Before I didn’t know how to look after them [children] right. Either I would show too much, love or be too strict. Now I have learnt how to explain things. Several days ago, one of my children did not want to go to bed, but I said, ‘you need to be in bed on time’ and explained why. I knew what to do”.(C5)
“They have only now become aware of some of their children’s feelings and that the children feel this situation and everything that’s happening to them. We had some emotional reactions in some. I really think it was successful and it was meaningful”.(F3)
“Communication in the family is not at the level it should be. Of course, this is expected in such life circumstances, but the communication is really bad. Children didn’t listen to their caregivers enough, and don’t even have anyone to talk to about their problems and everything, and I wasn’t much surprised by that picture. Now they share and both talk to each other”.(F2)
“We learnt to talk with this tone, a different tone that we practiced. This is really good for the kids. Not to talk so angrily to the kids but to use another tone. Now it’s better, much better really. I talk more to them and in a kinder way and then they in return behave better”.(C1)
“I was always angry with the kid. In fact, I didn’t even know why the kid was fighting. I learnt that I need to talk with the kid. Now I talk and I know how to react. I know what’s going on, so I react appropriately”.(C3)
“We would hardly talk about how the kids should be, now we talk every couple of days for about half an hour, perhaps an hour when there’s a problem. About how we should treat them [children]. This was certainly not how it was before the program”.(C2)
“Before, both of us [husband and wife] would argue a lot. We would fight about our son and because he [husband] was always angry at him [son]. But we learnt that this is not how it should be, no one is benefitting. We all act differently and talk better now. He [son] acts differently and so do we, and so then there is much less fighting”.(C3)
“We began talking to each other, we had a shared topic to discuss. I was the one who took part, so I told him what I had learnt and I also told my other kids. He was receptive and took it in. We soon started talking about other things again, sometimes good memories and sometimes hard things”.(C1)
“I grew up in a Muslim family and real Islam is like that; the family is paramount. The relationship between family members should be good, just like we learnt in this program. What we learnt [in the intervention] is all in our religion; to respect each other, our families as well and respect the elderly”.(C4)
“We identified two children, that we would later on start working with further, during the sessions we noticed signs of stress like bed-wetting which is very alarming and must be addressed. This wasn’t explored by the doctors previously. It was effective [the intervention] in the sense of identifying the signs for the identification of children’s needs, so that some form of individual work may be later on designed”.(F1)
“They [participating caregivers] and us [facilitators] learnt that some symptoms, which we may think are harmless, are actually very worrying and not so harmless. We learnt to be aware of signs of stress and challenges that are not normal reactions to the situation of these families. Caregivers learnt that spending more time with their children is what will help you identify such things”.(F1)
“The deep breathing exercise is very good. I go to the terrace and there I breathe deeply and it feels really nice”.(C5)
“I have learnt not to dwell on stress a lot. I now understand it does not make much sense to dwell on it and it makes me unable to be a good father when I do. I have learnt tapping and breathing, and these are very useful in my life now generally”.(C6)
“Our children were thrilled with the program and kept asking when the next sessions were”.(C2)
“Strong Families should be made accessible to everyone in all Reception Centers. Not only where we are. It’s well suited for other nationalities, and for us too [Serbian facilitators].(F1)
“We are in a closed camp and we have got nowhere to go, and it was really good that we participated, had a chance to talk and get to know new people, feeling like we are not alone. That was good, it’s really boring in the camp and parents also like to do something, something new”.(C4)
“Every day it’s the same, just eat, sleep. It’s not right at all. The program motivated them, it was dynamic and interesting. The topic well covered, to really talk and to be useful for them”.(F6)
“It’s best for both parents to be there, so both can get the experience and learn. If there is a parent who is ignorant to the needs of the child and needs to understand the child more and to build this relationship with the child, being informed second hand from their partner won’t be enough”.(F3)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- UNICEF. For Every Child, Every Right; Annual Report. 2018. Available online: https://www.unicef.org/media/55486/file/UNICEF-annual-report-2018%20revised%201.pdf (accessed on 12 December 2020).
- Sim, A.; Fazel, M.; Bowes, L.; Gardner, F. Pathways linking war and displacement to parenting and child adjustment: A qualitative study with Syrian refugees in Lebanon. Soc. Sci. Med. 2018, 200, 19–26. [Google Scholar] [CrossRef] [PubMed]
- El-Khani, A.; Ulph, F.; Peters, S.; Calam, R. Syria: Coping mechanisms utilised by displaced refugee parents caring for their children in pre-resettlement contexts. Intervention 2017, 15, 34–50. [Google Scholar] [CrossRef]
- Montgomery, E.; Foldspang, A. Seeking asylum in Denmark: Refugee children’s mental health and exposure to violence. Eur. J. Public Health 2005, 15, 233–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halevi, G.; Djalovski, A.; Vengrober, A.; Feldman, R. Risk and resilience trajectories in war-exposed children across the first decade of life. J. Child Psychol. Psychiatry. 2016, 57, 1183–1193. [Google Scholar] [CrossRef] [PubMed]
- Sim, A.L.; Bowes, L.; Maignant, S.; Magber, S.; Gardner, F. “Modeling the effects of war exposure and daily stressors on maternal mental health, parenting, and child psychosocial adjustment: A cross-sectional study with Syrian refugees in Lebanon. Global Mental Health. 2018, 5, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eltanamly, H.; Leijten, P.; Jak, S.; Overbeek, G. Parenting in times of war: A meta-analysis and qualitative synthesis of war exposure, parenting, and child adjustment. Trauma Violence Abus. 2021, 22, 146–160. [Google Scholar] [CrossRef]
- Masten, A.S.; Monn, A.R. Child and family resilience: A call for integrated science, practice, and professional training. Fam. Relat. 2015, 64, 5–21. [Google Scholar] [CrossRef]
- Putnick, D.L.; Bornstein, M.H.; Lansford, J.E.; Chang, L.; Deater-Deckard, K.; Di Giunta, L.; Skinner, A.T. Parental acceptance–rejection and child prosocial behavior: Developmental transactions across the transition to adolescence in nine countries, mothers and fathers, and girls and boys. Dev. Psychol. 2018, 54, 1881. [Google Scholar] [CrossRef] [PubMed]
- Sim, A.L.; Bowes, L.; Maignant, S.; Magber, S.; Gardner, F. Acceptability and Preliminary Outcomes of a Parenting Intervention for Syrian Refugees. Res. Soc. Work Pract. 2021, 31, 14–25. [Google Scholar] [CrossRef]
- El-Khani, A.; Ulph, F.; Peters, S.; Calam, R. Syria: Refugee parents’ experiences and need for parenting support in camps and humanitarian settings. Vulnerable Child. Youth Stud. 2018, 3, 19–29. [Google Scholar] [CrossRef]
- Timshel, I.; Montgomery, E.; Dalgaard, N.T. A systematic review of risk and protective factors associated with family related violence in refugee families. Child Abus. Negl. 2017, 70, 315–330. [Google Scholar] [CrossRef]
- UNHCR. Global Trends: Forced Displacement in 2015. 2016. Available online: https://www.unhcr.org/576408cd7.pdf (accessed on 12 December 2020).
- Haj-Yahia, M.M.; Clark, C.J. Intimate partner violence in the occupied Palestinian territory: Prevalence and risk factors. J. Fam. Violence 2013, 28, 797–809. [Google Scholar] [CrossRef]
- Panter-Brick, C.; Goodman, A.; Tol, W.; Eggerman, M. Mental health and childhood adversities: A longitudinal study in Kabul, Afghanistan. J. Am. Acad. Child Adolesc. Psychiatry 2011, 50, 349–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maalouf, W.; Campello, G. The influence of family skills programmes on violence indicators: Experience from a multi-site project of the United Nations Office on Drugs and Crime in low and middle income countries. Aggress. Violent Behav. 2014, 19, 616–624. [Google Scholar] [CrossRef]
- Barry, M.M. Promoting positive mental health: Theoretical frameworks for practice. Int. J. Ment. Health Promot. 2001, 3, 25–34. [Google Scholar]
- Murphy, K.M.; Rodrigues, K.; Costigan, J.; Annan, J. Raising children in conflict: An integrative model of parenting in war. Peace and conflict. J. Peace Psychol. 2017, 23, 40–46. [Google Scholar] [CrossRef]
- El-Khani, A.; Haar, K.; Maalouf, W.; Baker, D.A.; Zahra, N.; Noubani, A.; Cartwright, K.; Calam, R. Enhancing Teaching Recovery Techniques (TRT) with parenting skills: RCT of TRT+Parenting with trauma-affected Syrian refugees in Lebanon utilising remote training with implications for insecure contexts and COVID19. 2019; Under review. [Google Scholar]
- Ponguta, L.A.; Issa, G.; Aoudeh, L.; Maalouf, C.; Hein, S.D.; Zonderman, A.L.; Katsovich, L.; Khoshnood, K.; Bick, J.; Awar, A.; et al. Effects of the mother-child education program on parenting stress and disciplinary practices among refugee and other vulnerable communities in Lebanon: A pilot randomized controlled trial. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 727–738. [Google Scholar] [CrossRef] [Green Version]
- Miller, K.E.; Koppenol-Gonzalez, G.V.; Arnous, M.; Tossyeh, F.; Chen, A.; Nahas, N.; Jordans, M.J. Supporting Syrian families displaced by armed conflict: A pilot randomized controlled trial of the caregiver support intervention. Child Abus. Negl. 2020, 106, 104512. [Google Scholar] [CrossRef]
- Ballard, J.; Wieling, E.; Forgatch, M. Feasibility of implementation of a parenting intervention with Karen refugees resettled from Burma. J. Marital. Fam. Ther. 2018, 44, 220–234. [Google Scholar] [CrossRef]
- Gardner, F.; Burton, J.; Klimes, I. Randomised controlled trial of a parenting intervention in the voluntary sector for reducing child conduct problems: Outcomes and mechanisms of change. J. Child Psychol. Psychiatry 2006, 47, 1123–1132. [Google Scholar] [CrossRef]
- Haar, K.; El-Khani, A.; Molgaard, V.; Maalouf, W. Strong families: A new family skills training programme for challenged and humanitarian settings: A single-arm intervention tested in Afghanistan. BMC Public Health 2020, 20, 1–6. [Google Scholar]
- UNHCR. Serbia; Interagency Operational Update July–August 2017. 2018. Available online: http://www.unhcr.rs/ (accessed on 12 December 2020).
- Save the Children. Refugees and Migrant at the Western Balkans Route in 2018. 2018. Available online: https://resourcecentre.savethechildren.net/library/balkans-migration-and-displacement-hub-data-and-trend-analysis-data-regional-overview-july (accessed on 12 December 2020).
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Sanders, M.R.; Haslam, D.M.; Filus, A.; Fletcher, R. Parenting and Family Adjustment Scales (PAFAS): Validation of a brief parent-report measure for use in assessment of parenting skills and family relationships. Child Psychiatry Hum. Dev. 2014, 45, 255–272. [Google Scholar] [CrossRef] [PubMed]
- Mejia, A.; Calam, R.; Morawska, A.; Sanders, M.R. Measuring parenting practices and family functioning with brief and simple instruments: Validation of the Spanish version of the PAFAS. Child Psychiatry Hum. Dev. 2015, 46, 426–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Khani, A.; Maalouf, W.; Baker, D.A.; Zahra, N.; Noubani, A.; Cartwright, K. Caregiving for children through conflict and displacement: A pilot study testing the feasibility of delivering and evaluating a light touch parenting intervention for caregivers in the West Bank. Int. J. Psychol. 2019, 55, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Nunnally, J.C. An Overview of Psychological Measurement. In Clinical Diagnosis of Mental Disorders; Wolman, B.B., Ed.; Springer: Boston, MA, USA, 1978. [Google Scholar]
- Laerd Statistics. Two-way mixed ANOVA Using SPSS Statistics. Statistical Tutorials and Software Guides. 2015. Available online: https://statistics.laerd.com/ (accessed on 12 December 2020).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Potter, J.; Wetherell, M. Discourse and Social Psychology: Beyond Attitudes and Behaviour; Sage: London, UK, 1987. [Google Scholar]
- Maalouf, W.; Haar, K.; Molgaard, V.; Molgaard, L.; Stojanovic, M.; Gomez, B.; El-Khani, A. Strong Families: Multisite Pilot of an Open Sourced Family Skills Programme Designed for Challenged and Humanitarian Settings. In Proceedings of the Annual conference of the Society for Prevention Research 27th, San Francisco, CA, USA, 28 May 2019. [Google Scholar]
- UNODC. Strong Families Programme Vienna: United Nations Office on Drugs and Crime. 2015. Available online: https://www.unodc.org/documents/drug-prevention-and-treatment/Strong_families_Brochure.pdf (accessed on 14 April 2021).
- Mejia, A.; Calam, R.; Sanders, M.R. A pilot randomized controlled trial of a brief parenting intervention in low-resource settings in Panama. Prev. Sci. 2015, 16, 707–717. [Google Scholar] [CrossRef]
- Betancourt, T.S.; Khan, K.T. The mental health of children affected by armed conflict: Protective processes and pathways to resilience. Int. Rev. Psychiatry 2008, 20, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Deković, M.; Asscher, J.J.; Hermanns, J.; Reitz, E.; Prinzie, P.; Van Den Akker, A.L. Tracing changes in families who participated in the home-start parenting program: Parental sense of competence as mechanism of change. Prev. Sci. 2010, 11, 263–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanders, M.R. New directions in behavioural family intervention with children. In Advances in Clinical Child Psychology; Ollendick, T.H., Prinz, R.J., Eds.; Plenum Press: New York, NY, USA, 1996; Volume 18. [Google Scholar]
- Butler, M.; Percy, A.; Hayes, D.; Devaney, J. Designing Prison-Based Parenting Programs to Maximize Their Outcomes. Int. J. Offender Ther. Comp. Criminol. 2019, 63, 975–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barber, B.K.; Stolz, H.E.; Olsen, J.A.; Collins, W.A.; Burchinal, M. Parental support, psychological control, and behavioral control: Assessing relevance across time, culture, and method. Monographs Soc. Res. Child Dev. 2005, 4, 282–299. [Google Scholar]
 significant difference between t1 and t2,
significant difference between t1 and t2,  significant difference between t1 and t3.
significant difference between t1 and t2, significant difference between t1 and t3.
significant difference between t1 and t3.
significant difference between t1 and t2, significant difference between t1 and t3.


{kind=link}
{kind=link}
| Gender-Based Analysis | Pre-Test Mean (SD) {Min–Max} | Post-Test Mean (SD) {Min–Max} | Follow-Up Mean (SD) {Min–Max} | Two-Way Mixed ANOVA F(dftime, dferror); p-Value; Partial η2 | Repeated Measures ANOVA F(dftime, dferror); p-Value; Partial η2 | Post-Hoc Tests | |
|---|---|---|---|---|---|---|---|
| SDQ subscales | |||||||
| Emotional problem scale {0–10} | Boys (n = 16) | 5.69 (2.39) {2–9} | 4.44 (1.82) {0–7} | 4.56 (2.45) {1–10} | F(2,46) = 1.851; p = 0.169; ηp2 = 0.07 | n.s. | |
| Girls (n = 9) | 5.89 (2.80) {2–10} | 2.78 (1.48) {1–6} | 3.56 (2.65) {1–7} | F(2,16) = 7.840; p = 0.004; ηp2 = 0.50 | Þ | ||
| Overall | 5.76 (2.49) {2–10} | 3.84 (1.86) {0–7} | 4.2 (2.51) {1–10} | --- | F(2,48) = 9.063; p < 0.001; ηp2 = 0.27 | Þ¢ | |
| Conduct problem scale {0–10} | Boys (n = 16) | 2.63 (1.82) {0–5} | 2.44 (1.31) {0–5} | 1.81 (1.22) {0–4} | F(2,46) = 1.327; p = 0.275; ηp2 = 0.06 | F(2,30) = 4.952; p = 0.014; ηp2 = 0.25 | Φ¢ |
| Girls (n = 9) | 2.00 (1.0) {1–3} | 1.00 (1.5) {0–4} | 0.56 (0.88) {0–2} | F(2,16) = 4.189; p = 0.034; ηp2 = 0.34 | ¢ | ||
| Overall | 2.40 (1.58) {0–5} | 1.92 (1.53) {0–5} | 1.36 (1.25) {0–5} | --- | F(2,48) = 8.455; p = 0.001; ηp2 = 0.26 | Φ¢ | |
| Hyperactivity scale {0–10} | Boys (n = 16) | 4.81 (2.90) {0–10} | 3.56 (1.90) {0–7} | 2.75 (1.98) {1–7} | F(2,46) = 1.408; p = 0.255; ηp2 = 0.06 | F(1.319,19.785) = 5.707; p = 0.02; ηp2 = 0.28; | ¢ |
| Girls (n = 9) | 2.44 (2.19) {0–6} | 2.44 (2.70) {0–8} | 1.89 (1.90) {0–5} | n.s. | |||
| Overall | 3.96 (2.86) {0–10} | 3.28 (2.30) {0–8} | 2.44 (1.95) {0–7} | --- | F(1.674,40.167) = 5.346; p = 0.012; ηp2 = 0.18; | ¢ | |
| Peer problem scale {0–10} | Boys (n = 16) | 2.31 (2.24) {0–8} | 2 (2.31) {0–8} | 2.06 (1.53) {0–6} | F(2,46) = 0.269; p = 0.765; ηp2 = 0.01 | n.s. | |
| Girls (n = 9) | 1.67 (1.66) {0–4} | 1.67 (1.32) {0–4} | 1.89 (0.93) {1–4} | n.s. | |||
| Overall | 2.08 (2.04) {0–8} | 1.88 (1.99) {0–8} | 2 (1.32) {0–6} | --- | n.s. | ||
| Prosocial scale {{10–0} | Boys (n = 16) | 8.38 (1.36) {{5–10} | 8.38 (1.36) {6–10} | 8.94 (1.34) {6–10} | F(2,46) = 0.991; p = 0.379; ηp2 = 0.04 | n.s | |
| Girls (n = 9) | 9.44 (0.88) {8–10} | 8.78 (1.79) {5–10} | 9.22 (1.56) {6–10} | n.s | |||
| Overall | 8.76 (1.30) {5–10} | 8.52 (1.50) {5–10} | 9.04 (1.40) {6–10} | --- | n.s. | ||
| Total Difficulty Scale {0–40} | Boys (n = 16) | 15.44 (7.26) {4–29} | 12.44 (5.76) {4–26} | 11.19 (5.02) {3–21} | F(2,46) = 0.243; p = 0.786; ηp2 = 0.01 | F(1.482,22.227) = 6.349; p = 0.011; ηp2 = 0.30; | ¢ |
| Girls (n = 9) | 12.00 (5.32) {5–23} | 7.89 (5.09) {3–19} | 7.89 (4.76) {3–16} | F(2,16) = 5.340; p = 0.017; ηp2 = 0.40 | ¢ | ||
| Overall | 14.2 (6.72) {4–29} | 10.8 (5.86) {3–26} | 10.0 (5.09) {3–21} | --- | F(2,48) = 11.521; p < 0.001; ηp2 = 0.32 | Þ¢ | |
| (Very) High (17+) on Total Difficulty Scale (n = 9) at Baseline | Pre-Test Mean (SD) {Min-Max} | Post-Test Mean (SD) {Min-Max} | Follow-Up Mean (SD) {Min-Max} | Repeated measures ANOVA F(dftime, dferror); p-value; partialη2 | Post-Hoc Tests | ||
| Emotional problem scale | 7.22 (2.33) {3–10} | 5.56 (1.13) {4–7} | 5.00 (1.73) {2–7} | F(2,16) = 7.065; p = 0.006; ηp2 = 0.47 | ¢ | ||
| Conduct problem scale | 3.78 (1.30) {1–5} | 3.11 (1.36) {1–5} | 2.44 (1.01) {1–4} | F(2,16) = 6.857; p = 0.007; ηp2 = 0.46 | ¢ | ||
| Hyperactivity scale | 6.78 (1.64) {4–10} | 4.78 (2.11) {2–8} | 3.44 (2.19) {1–7} | F(1.238,9.907) = 7.696; p = 0.005; ηp2 = 0.49; | Φ¢ | ||
| Peer problem scale | 4.00 (1.73) {2–8} | 2.89 (2.47) {0–8} | 2.67 (1.58) {1–6} | F(2,16) = 5.734; p = 0.013; ηp2 = 0.42 | ¢ | ||
| Prosocial scale | 7.89 (1.36) {5–10} | 8.11 (1.76) {5–10} | 8.56 (1.42) {7–10} | n.s. | |||
| Total Difficulty Scale | 21.78 (3.15) {18–29} | 16.33 (5.39) {11–26} | 13.56 (5.25) {7–21} | F(1.223,9.784) = 19.923; p < 0.001; ηp2 = 0.71; | ÞΦ¢ | ||
| Caregiver Number | Gender | Age |
| 1 | female | 32 |
| 2 | female | 33 |
| 3 | female | 26 |
| 4 | female | 28 |
| 5 | male | 39 |
| 6 | male | 43 |
| 7 | female | 26 |
| 8 | female | 32 |
| Facilitator number | ||
| 1 | male | 25 |
| 2 | female | 28 |
| 3 | male | 32 |
| 4 | female | 25 |
| 5 | female | 39 |
| 6 | male | 24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Khani, A.; Haar, K.; Stojanovic, M.; Maalouf, W. Assessing the Feasibility of Providing a Family Skills Intervention, “Strong Families”, for Refugee Families Residing in Reception Centers in Serbia. Int. J. Environ. Res. Public Health 2021, 18, 4530. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094530
El-Khani A, Haar K, Stojanovic M, Maalouf W. Assessing the Feasibility of Providing a Family Skills Intervention, “Strong Families”, for Refugee Families Residing in Reception Centers in Serbia. International Journal of Environmental Research and Public Health. 2021; 18(9):4530. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094530
Chicago/Turabian StyleEl-Khani, Aala, Karin Haar, Milos Stojanovic, and Wadih Maalouf. 2021. "Assessing the Feasibility of Providing a Family Skills Intervention, “Strong Families”, for Refugee Families Residing in Reception Centers in Serbia" International Journal of Environmental Research and Public Health 18, no. 9: 4530. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094530