
Identification of Health Expenditures Determinants: A Model to Manage the Economic Burden of Cardiovascular Disease

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Study Variables
Explanatory Variables
2.4. Statistical Models and Analysis
3. Results
3.1. Sample Characteristics
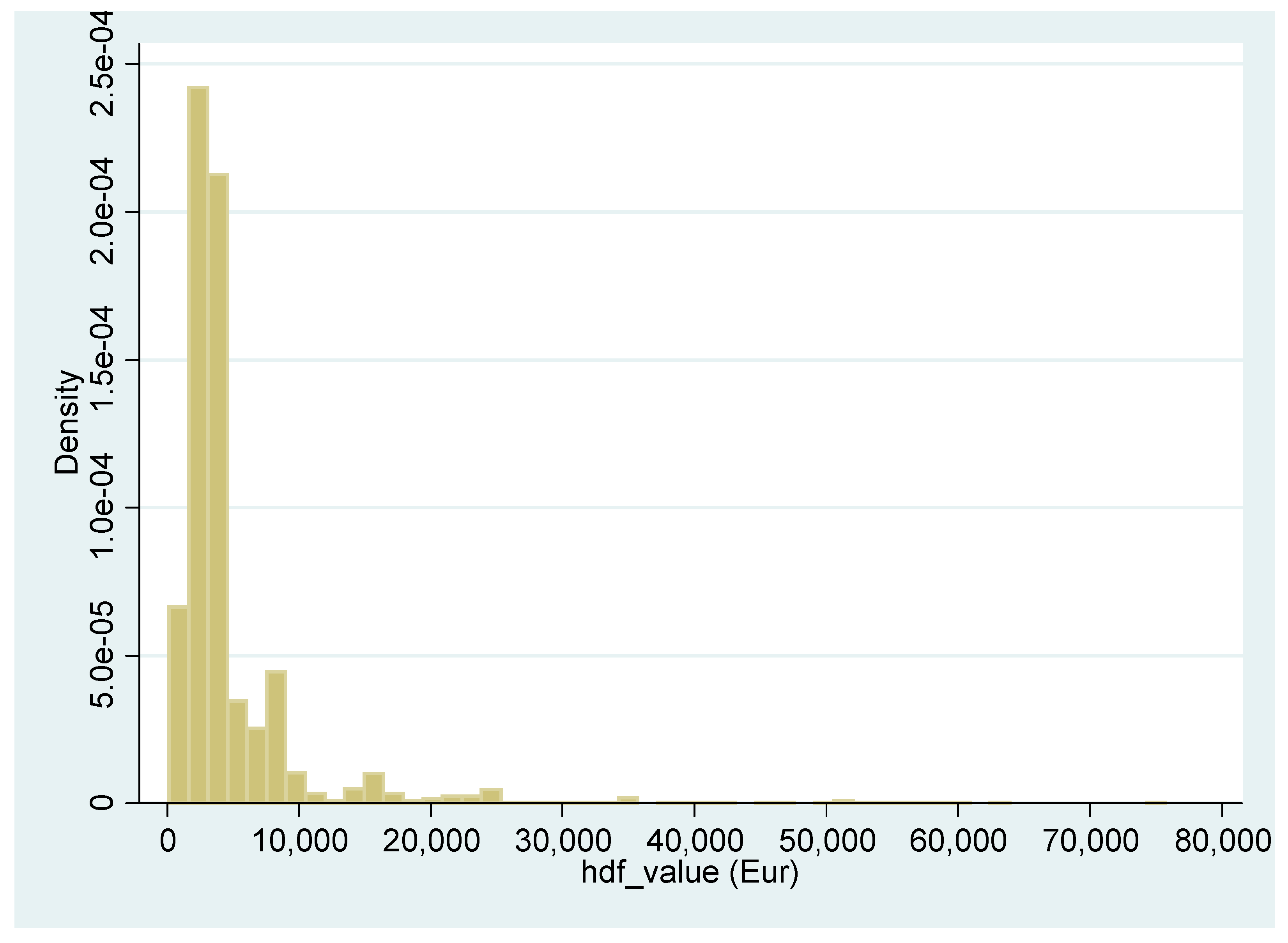
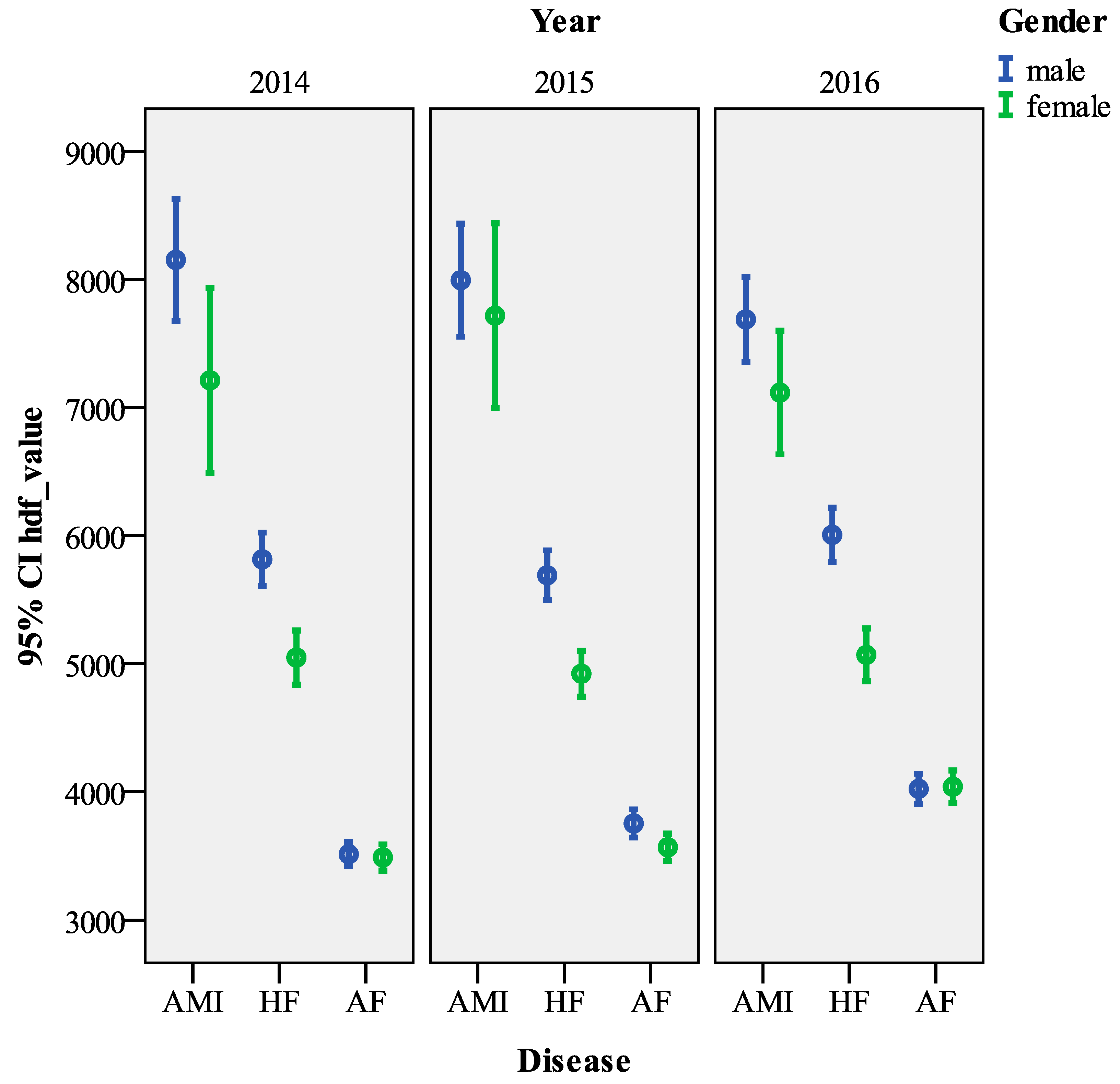
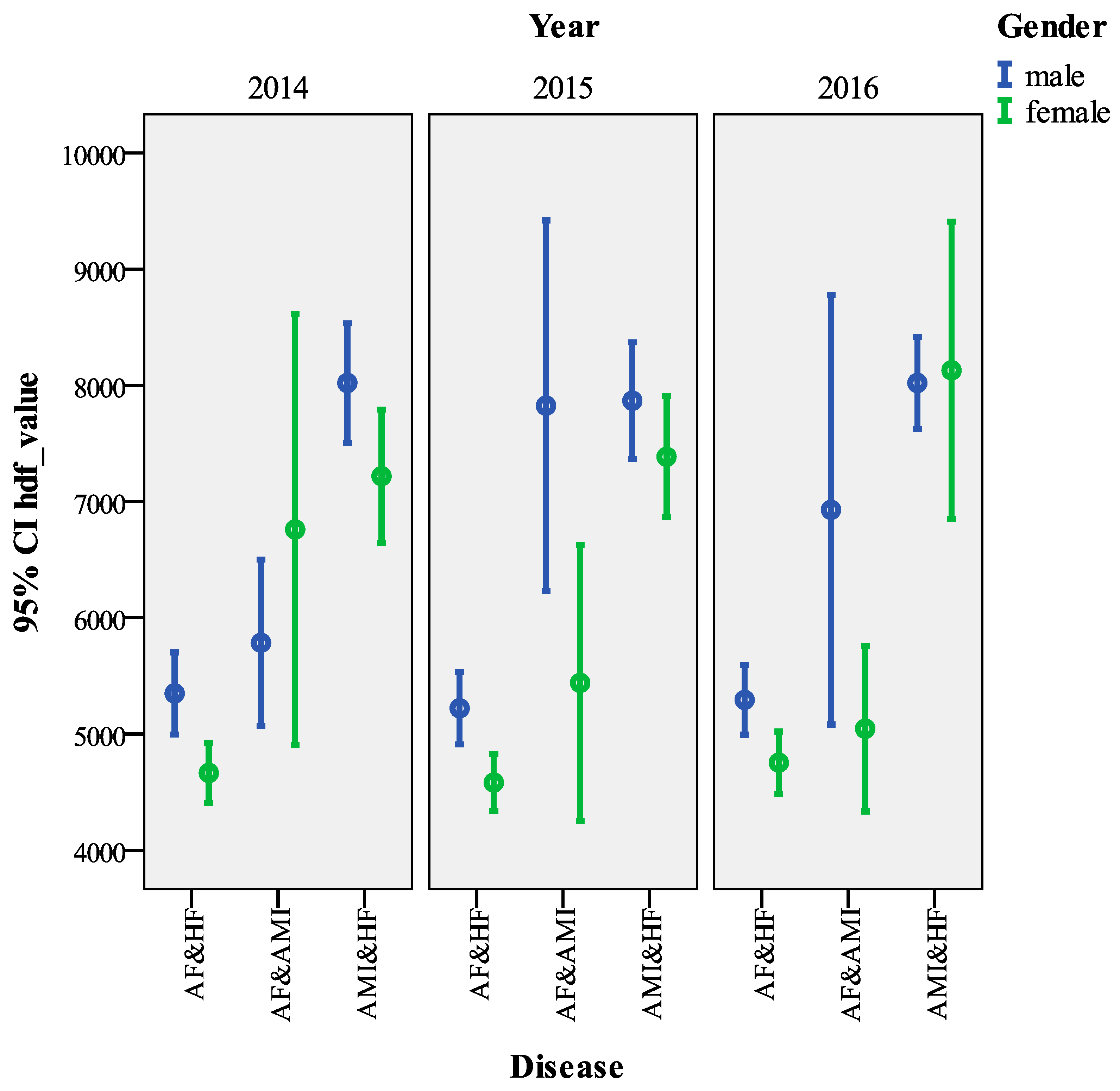
3.2. Descriptive Statistics
3.3. GLM and GLMM Models
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- OECD. Focus on Health Spending—Expenditure by Disease, Age and Gender; OECD: Paris, France, 2016. [Google Scholar]
- WHO. Global Health Observatory Data Repository—Life Expectancy; World Health Organization: Geneva, Switzerland; Available online: http://apps.who.int/gho/data/node.main.688 (accessed on 12 February 2021).
- Walker, I.F.; Garbe, F.; Wright, J.; Newell, I.; Athiraman, N.; Khan, N.; Elsey, H. The Economic Costs of Cardiovascular Disease, Diabetes Mellitus, and Associated Complications in South Asia: A Systematic Review. Value Health Reg. Issues 2018, 15, 12–26. [Google Scholar] [CrossRef]
- Marcellusi, A.; Viti, R.; Sciattella, P.; Aimaretti, G.; De Cosmo, S.; Provenzano, V.; Tonolo, G.; Mennini, F.S. Economic aspects in the management of diabetes in Italy. BMJ Open Diabetes Res. Care 2016, 4, e000197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juying, Z. Semi-parametric identification of determinants of health expenditures—Evidence from inpatients in China. Manag. Decis. 2014, 52, 1302–1318. [Google Scholar] [CrossRef]
- Potrafke, N. The growth of public health expenditures in OECD countries: Do government ideology and electoral motives matter? J. Health Econ. 2010, 29, 797–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sfakianakis, G.; Grigorakis, N.; Galyfianakis, G.; Katharaki, M. The impact of macro-fiscal factors and private health insurance financing on public health expenditure: Evidence from the OECD countries for the period 2000. Euro Med. J. Bus. 2020, 16, 1–24. [Google Scholar] [CrossRef]
- Andrei, C.L.; Oancea, B.; Nedelcu, M.; Sinescu, R.D. Predicting cardiovascular diseases prevalence using neural networks. Econ. Comput. Econ. Cyber. Stud. Res. 2015, 49, 73–84. [Google Scholar]
- Arfaoui, N.; Hofaidhllaoui, M.; Chawla, G. Social performance of the company. Euro Med. J. Bus. 2019, 15, 102–126. [Google Scholar] [CrossRef]
- Rudawska, I. Chronic diseases—An economic problem? Transform. Bus. Econ. 2014, 13, 615–624. [Google Scholar]
- Agnihothri, S.; Agnihothri, R. Application of evidence-based management to chronic disease healthcare: A framework. Manag. Decis. 2018, 56, 2125–2147. [Google Scholar] [CrossRef]
- Roshanghalb, A.; Lettieri, E.; Aloini, D.; Cannavacciuolo, L.; Gitto, S.; Visintin, F. What evidence on evidence-based management in healthcare? Manag. Decis. 2018, 56, 2069–2084. [Google Scholar] [CrossRef]
- Scalone, L.; Cesana, G.; Furneri, G.; Ciampichini, R.; Beck-Peccoz, P.; Chiodini, V.; Mangioni, S.; Orsi, E.; Fornari, C.; Mantovani, L.G. Burden of Diabetes Mellitus Estimated with a Longitudinal Population-Based Study Using Administrative Databases. PLoS ONE 2014, 9, e113741. [Google Scholar] [CrossRef] [PubMed]
- Bansilal, S.; Castellano, J.M.; Fuster, V. WITHDRAWN: Global burden of CVD: Focus on secondary prevention of cardiovascular disease. Int. J. Cardiol. 2016, 201, S1–S7. [Google Scholar] [CrossRef] [Green Version]
- Di Carlo, A.; Bellino, L.; Consoli, D.; Mori, F.; Zaninelli, A.; Baldereschi, M.; Cattarinussi, A.; D’Alfonso, M.G.; Gradia, C.; Sgherzi, B.; et al. Prevalence of atrial fibrillation in the Italian elderly population and projections from 2020 to 2060 for Italy and the European Union: The FAI Project. Europe 2019, 21, 1468–1475. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, L.G.; Fornari, C.; Madotto, F.; Riva, M.A.; Merlino, L.; Ferrario, M.M.; Chiodini, V.; Zocchetti, A.; Corrao, G.; Cesana, G. Burden of acute myocardial infarction. Int. J. Cardiol. 2011, 150, 111–112. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; de Ferranti, S.; Despres, J.-P.; Fullerton, H.J.; Howard, V.J.; et al. Executive summary: Heart disease and stroke statistics—2015 update: A report from the American Heart Association. Circulation 2015, 131, 434–441. [Google Scholar] [CrossRef]
- Pavlušová, M.; Klimeš, J.; Špinar, J.; Zeman, K.; Jarkovský, J.; Benešová, K.; Miklík, R.; Pohludková, L.; Felšöci, M.; Veselá, V.; et al. Chronic heart failure—Impact of the condition on patients and the healthcare system in the Czech Republic: A retrospective cost-of-illness analysis. Cor Vasa 2018, 60, e224–e233. [Google Scholar] [CrossRef] [Green Version]
- Timóteo, A.T.; Gouveia, M.; Soares, C.; Ferreira, R.C. Indirect costs of myocardial infarction in Portugal. Rev. Portug. Cardiol. 2020, 5, 245–251. [Google Scholar] [CrossRef]
- Mozos, I. Links between shift work, cardiovascular risk and disorders. In Shift Work: Impacts, Disorders and Studies 2020; He, W., Yu, L., Eds.; Nova Science: Hauppage, NY, USA, 2020; pp. 23–44. [Google Scholar]
- Koçkaya, G.; Oğuzhan, G.E.; Özin, B.; Yılmaz, K.C.; Çiftçi, O.; Çavuş, F.; Sharaf, A.M.; Buyuktuna, N.; Buyukısık, T.; Saylan, M. Cost analysis of management of cardiovascular disease comorbidities in Turkey. J. Pharm. Health Serv. Res. 2019, 10, 197–202. [Google Scholar] [CrossRef]
- Adepu, S.; Berman, A.E.; Thompson, M.A. Socioeconomic determinants of health and country-level variation in cardio-vascular disease mortality: An exploratory analysis of Georgia during 2014. Prev. Med. Rep. 2020, 19, 101160. [Google Scholar] [CrossRef]
- Kontsevaya, A.; Kalinina, A.; Oganov, R. Economic Burden of Cardiovascular Diseases in the Russian Federation. Value Health Reg. Issues 2013, 2, 199–204. [Google Scholar] [CrossRef] [Green Version]
- Baltagi, B.H.; Moscone, F. Health care expenditure and income in the OECD reconsidered: Evidence from panel data. Econ. Model. 2010, 27, 804–811. [Google Scholar] [CrossRef] [Green Version]
- Fusco, F.; Migliaccio, G. Crisis, sectoral and geographical factors: Financial dynamics of Italian cooperatives. Euro Med. J. Bus. 2018, 13, 130–148. [Google Scholar] [CrossRef]
- Herwartz, H.; Theilen, B. The determinants of health care expenditure: Testing pooling restrictions in small samples. Health Econ. 2003, 12, 113–124. [Google Scholar] [CrossRef]
- Akca, N.; Sönmez, S.; Yilmaz, A. Determinants of health expenditure in OECD countries: A decision tree model. Pak. J. Med. Sci. 2017, 33, 1490–1494. [Google Scholar] [CrossRef] [PubMed]
- Wieser, S.; Riguzzi, M.; Pletscher, M.; Huber, C.A.; Telser, H.; Schwenkglenks, M. How much does the treatment of each major disease cost? A decomposition of Swiss National Health Accounts. Eur. J. Health Econ. 2018, 19, 1149–1161. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, D.; Ibrahim, M.I.B.M.; Boncz, I. What Are the Challenges in Conducting Cost-of-Illness Studies? Value Health Reg. Issues 2014, 4, 115–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larg, A.; Moss, J.R. Cost-of-illness studies: A guide to critical evaluation. Pharmacoeconomics 2011, 29, 653–671. [Google Scholar] [CrossRef]
- Onukwugha, E.; McRae, J.; Kravetz, A.; Varga, S.; Khairnar, R.; Mullins, C.D. Cost-of-Illness Studies: An Updated Review of Current Methods. PharmacoEconomics 2016, 34, 43–58. [Google Scholar] [CrossRef]
- Schoenman, J.A.; Sutton, J.P.; Kintala, S.; Love, D.; Maw, R. The Value of Hospital Discharge Databases; NORC at the University of Chicago: Chicago, IL, USA, 2005. [Google Scholar]
- Cozzolino, F.; Abraha, I.; Orso, M.; Mengoni, A.; Cerasa, M.F.; Eusebi, P.; Ambrosio, G.; Montedori, A. Protocol for validating cardiovascular and cerebrovascular ICD-9-CM codes in healthcare administrative databases: The Umbria Data Value Project. BMJ Open 2017, 7, e013785. [Google Scholar] [CrossRef]
- Italian Ministerial Decree no. 380 of October 27th. 2001. Available online: http://www.salute.gov.it/imgs/C_17_normativa_170_allegato.pdf. (accessed on 16 January 2021).
- De Belvis, A. Esperienzed’uso dell’ICD-9-CM; IstitutoPoligraficodelloStato e ZeccadelloStato: Rome, Italy, 2003; Volume 2. [Google Scholar]
- Liu, Z.; Qin, H.; Yang, Z.; Xia, Y.; Liu, W.; Yang, J.; Jiang, Y.; Zhang, H.; Yang, Z.; Wang, Y.; et al. Randomised clinical trial: The effects of perioperative probiotic treatment on barrier function and post-operative infectious complications in colorectal cancer surgery–a double-blind study. Aliment. Pharmacol. Therap. 2011, 33, 50–63. [Google Scholar] [CrossRef] [PubMed]
- Park, R.E. Estimation with Heteroscedastic Error Terms. Economics 1966, 34, 888. [Google Scholar] [CrossRef]
- Bolker, B.M. Ecological Models and Data in R; Princeton University Press: Princeton, NJ, USA, 2008. [Google Scholar]
- Stroup, W.W.; Kachman, S.D. Generalized Linear Mixed Models—An Overview. In Proceedings of the 1994—6th Annual Conference Proceedings, Addis Abeba, Ethiopia, 3–4 May 1994. [Google Scholar]
- Perrone, V.; Sangiorgi, D.; DegliEsposti, L.; Modugno, G.; Dambrosio, G.; Diaferia, G.; DelVecchio, B.; Dell’Orco, M.L.; Masullo, M.; Ancona, D.; et al. Heart failure in Apulia Region—Italy (Local Health Unit Barletta-Andria-Trani): Analysis of the therapeutic pathways, healthcare resource consumption and related costs. Recenti Progress. Med. 2019, 110, 23–32. [Google Scholar]
- Mosca, L.; Barrett-Connor, E.; Kass Wenger, N. Sex/gender differences in cardiovascular disease prevention: What a difference a decade makes. Circulation 2011, 124, 2145–2154. [Google Scholar] [CrossRef] [Green Version]
- Constanti, M.; Floyd, C.N.; Glover, M.; Boffa, R.; Wierzbicki, A.S.; McManus, R.J. Cost-Effectiveness of Initiating Pharmacological Treatment in Stage One Hypertension Based on 10-Year Cardiovascular Disease Risk: A Markov Modeling Study. Hypertension 2020, 77, 120. [Google Scholar]
- Marra, A.M.; Salzano, A.; Arcopinto, M.; Piccioli, L.; Raparelli, V. The impact of gender in cardiovascular medicine: Lessons from the gender/sex-issue in heart failure. Monaldi Arch. Chest Dis. 2018, 88, 48–52. [Google Scholar] [CrossRef]
- Liakos, M.; Parikh, P.B. Gender Disparities in Presentation, Management, and Outcomes of Acute Myocardial Infarction. Curr. Cardiol. Rep. 2018, 20, 64. [Google Scholar] [CrossRef]
- Aloini, D.; Cannavacciuolo, L.; Gitto, S.; Lettieri, E.; Malighetti, P.; Visintin, F. Evidence-Based Management for Performance Improvement in HealthCare. Manag. Decis. 2018, 56, 2063–2068. [Google Scholar] [CrossRef] [Green Version]
- Hartley, J. Innovation in governance and public services: Past and present. Publ. Money Manag. 2005, 25, 27–34. [Google Scholar]
- Morgan, J.; Tumlinson, J. Corporate provision of public goods. Manag. Sci. 2019, 65, 4489–4504. [Google Scholar] [CrossRef] [Green Version]
- Beebe, G.; Novicevic, M.; Popoola, I.T.; Holland, J. Entrepreneurial public leadership: 5As framework for wellness pro-motion. Manag. Decis. 2019, 57, 1443–1456. [Google Scholar] [CrossRef]
- Balzaretti, C.M.; Ventura, V.; Ratti, S.; Ferrazzi, G.; Spallina, A.; Carruba, M.O.; Castrica, M. Improving the overall sustainability of the school meal chain: The role of portion sizes. Eating and Weight Disorders-Studies on Anorexia. Bulim. Obes. 2020, 25, 107–116. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Diagnosis | Description |
|---|---|
| Acute myocardial infarction | 410.0 Anterolateral wall |
| 410.1 Other anterior wall | |
| 410.2 Inferolateral wall | |
| 410.3 Inferoposterior wall | |
| 410.4 Other inferior wall | |
| 410.5 Other lateral wall | |
| 410.6 True posterior wall infarction | |
| 410.7 Subendocardial infarction | |
| 410.8 Other specified sites | |
| 410.9 Unspecified site | |
| Atrial fibrillation and flutter | 427.31 Atrial fibrillation |
| 427.32 Atrial flutter | |
| Heart failure | 428.0 Congestive heart failure. unspecified |
| 428.1 Left heart failure | |
| 428.2 Systolic heart failure | |
| 428.20 Unspecified | |
| 428.21 Acute | |
| 428.22 Chronic | |
| 428.23 Acute on chronic | |
| 428.3 Diastolic heart failure | |
| 428.30 Unspecified | |
| 428.31 Acute | |
| 428.32 Chronic | |
| 428.33 Acute on chronic | |
| 428.4 Combined systolic and diastolic heart failure | |
| 428.40 Unspecified | |
| 428.41 Acute | |
| 428.42 Chronic | |
| 428.43 Acute on chronic | |
| 428.9 Heart failure unspecified |
| Patients’ Sample | n (%) or Mean ± SD |
|---|---|
| 98,829 (100) | |
| Panel A—Socio-demographic characteristics | |
| Gender | |
| Male | 52,184 (52.8) |
| Female | 46,645 (47.2) |
| Age (years) | |
| Mean ± SD | 75.46 ± 12.37 |
| Range | 1–107 |
| Marital status | |
| Married | 53,866 (54.5) |
| Divorced/separate | 9561 (9.6) |
| Widowed | 16,418 (16.6) |
| Single | 5409 (5.5) |
| Undeclared | 13,575 (13.7) |
| Nationality | |
| Italy | 97,941 (99.1) |
| Europe | 402 (0.4) |
| Asia | 50 (0.05) |
| Africa | 82 (0.08) |
| America | 18 (0.01) |
| Oceania | 18 (0.01) |
| Stateless | 333 (0.3) |
| Times the patient is detected in the register | |
| Mean ± SD | 1.59 ± 1.16 |
| Range | 1−25 |
| DRG (Euros) | |
| Mean ± SD | 218.85± 174.17 |
| Range | 1−579 |
| Hospital stay (day) | |
| Mean ± SD | 9.50 ± 11.56 |
| Range | 1–361 |
| Panel B—Pathologies characteristics | |
| Patients with a single disease | |
| HF | 23,449 (23.7) |
| AF | 39,086 (39.5) |
| AMI | 12,239 (12.4) |
| Patients with two pathologies | |
| HF&AF | 17,484 (17.7) |
| HF&AMI | 3738 (3.8) |
| AF&AMI | 1536 (1.6) |
| Patients with all three diseases | |
| HF&AF&AMI | 1297 (1.3) |
| Categorical Variables | N | hdf_value (Mean ± SD, Euros) | Kruskal–Wallis Test | |
|---|---|---|---|---|
| Gender | Male | 83,395 | 4916.15 ± 4969.12 | 1142.823 *** |
| Female | 73,677 | 4197.89± 4129.42 | ||
| Age | <20 | 165 | 5459.21 ± 8460.20 | 357.290 *** |
| <39 | 1129 | 4054.95 ± 4247.45 | ||
| <59 | 14,444 | 5261.53 ± 5482.95 | ||
| <79 | 72,023 | 4893.93 ± 5213.21 | ||
| Over 80 | 69,311 | 4116.49 ± 3569.05 | ||
| Hospitalization type | Ordinary hospitalization | 154,104 | 4624.65 ± 4636.66 | 2676.288 *** |
| Day hospitalization | 2968 | 2221.47 ± 1405.62 | ||
| Surgery | absence | 8434 | 3282.49 ± 1992.35 | 14,691.171 *** |
| presence | 72,732 | 6082.95 ± 6086.81 | ||
| Year | 2014 | 52,603 | 4517.89 ± 4657.98 | 173.555 *** |
| 2015 | 53,237 | 4670.34 ± 4636.97 | ||
| 2016 | 51,232 | 4670.34 ± 4636.97 | ||
| Single disease | HF | 14,602 | 5490.92 ± 5185.076 | 6846.585 *** |
| AF | 35,494 | 3724.67 ± 4328.88 | ||
| AMI | 3694 | 7775.32 ± 6316.08 | ||
| Double disease | AF&HF | 5591 | 4975.27 ± 4517.73 | 1528.284 *** |
| AF&AMI | 330 | 6407.50 ± 85,488.35 | ||
| AMI&HF | 1284 | 7836.86 ± 4313.88 | ||
| Triple disease | HF&AMI&AF | 140 | 7441.93 ± 5389.08 | |
| hdf_value (Euros) | Model 1 (GLM) | Model 2 (GLMM) |
|---|---|---|
| 2014 (Base) | - | - |
| 2015 | −0.0004 | 0.0037 |
| 2016 | 0.0255 *** | 0.0238 *** |
| Male (Base) | - | - |
| Female | −0.04683 *** | −0.04635 *** |
| Age | 0.00039 | 0.0017 *** |
| Ordinary hospitalization (Base) | - | - |
| Day hospitalization | −0.56661 *** | −0.6482 *** |
| Drg (Euros) | 0.0014 *** | 0.0015 *** |
| Hospital stay | 0.0181 | 0.01616 *** |
| Absence (Base) | - | - |
| Presence | 0.3370466 *** | 0.2874 *** |
| HF | ||
| Absence (Base) | - | - |
| Presence | 0.1392167 *** | 0.1672 *** |
| AMI | ||
| Absence (Base) | - | - |
| Presence | 0.1773 | 0.2202 *** |
| AF | ||
| Absence (Base) | - | - |
| Presence | −0.05545 *** | −0.0603 |
| _Cons | 7.6349 *** | 7.5031 *** |
| Patient Var | - | 0.0649288 |
| AIC | 2,840,619 | 2,833,922 |
| BIC | 2,840,748 | 2,834,062 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvatore, F.P.; Spada, A.; Fortunato, F.; Vrontis, D.; Fiore, M. Identification of Health Expenditures Determinants: A Model to Manage the Economic Burden of Cardiovascular Disease. Int. J. Environ. Res. Public Health 2021, 18, 4652. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094652
Salvatore FP, Spada A, Fortunato F, Vrontis D, Fiore M. Identification of Health Expenditures Determinants: A Model to Manage the Economic Burden of Cardiovascular Disease. International Journal of Environmental Research and Public Health. 2021; 18(9):4652. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094652
Chicago/Turabian StyleSalvatore, Fiorella Pia, Alessia Spada, Francesca Fortunato, Demetris Vrontis, and Mariantonietta Fiore. 2021. "Identification of Health Expenditures Determinants: A Model to Manage the Economic Burden of Cardiovascular Disease" International Journal of Environmental Research and Public Health 18, no. 9: 4652. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094652