
Examining the Availability and Accessibility of Rehabilitation Services in a Rural District of South Africa: A Mixed-Methods Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Context
2.2. Capability Approach Framework
2.3. Rehabilitation Service Capacity
2.4. Accessibility of Rehabilitation Services
3. Results
3.1. Availability of Rehabilitation Services
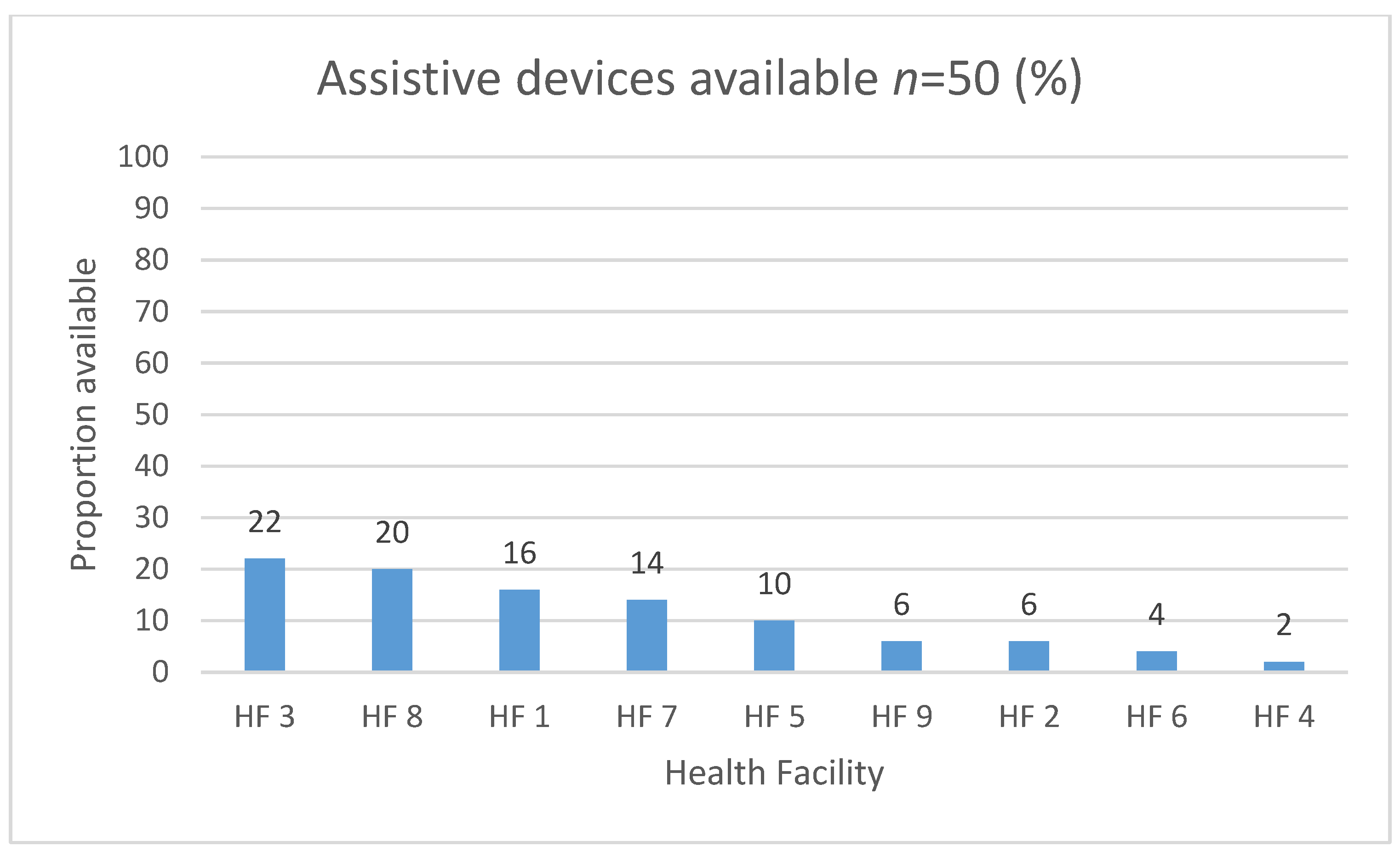
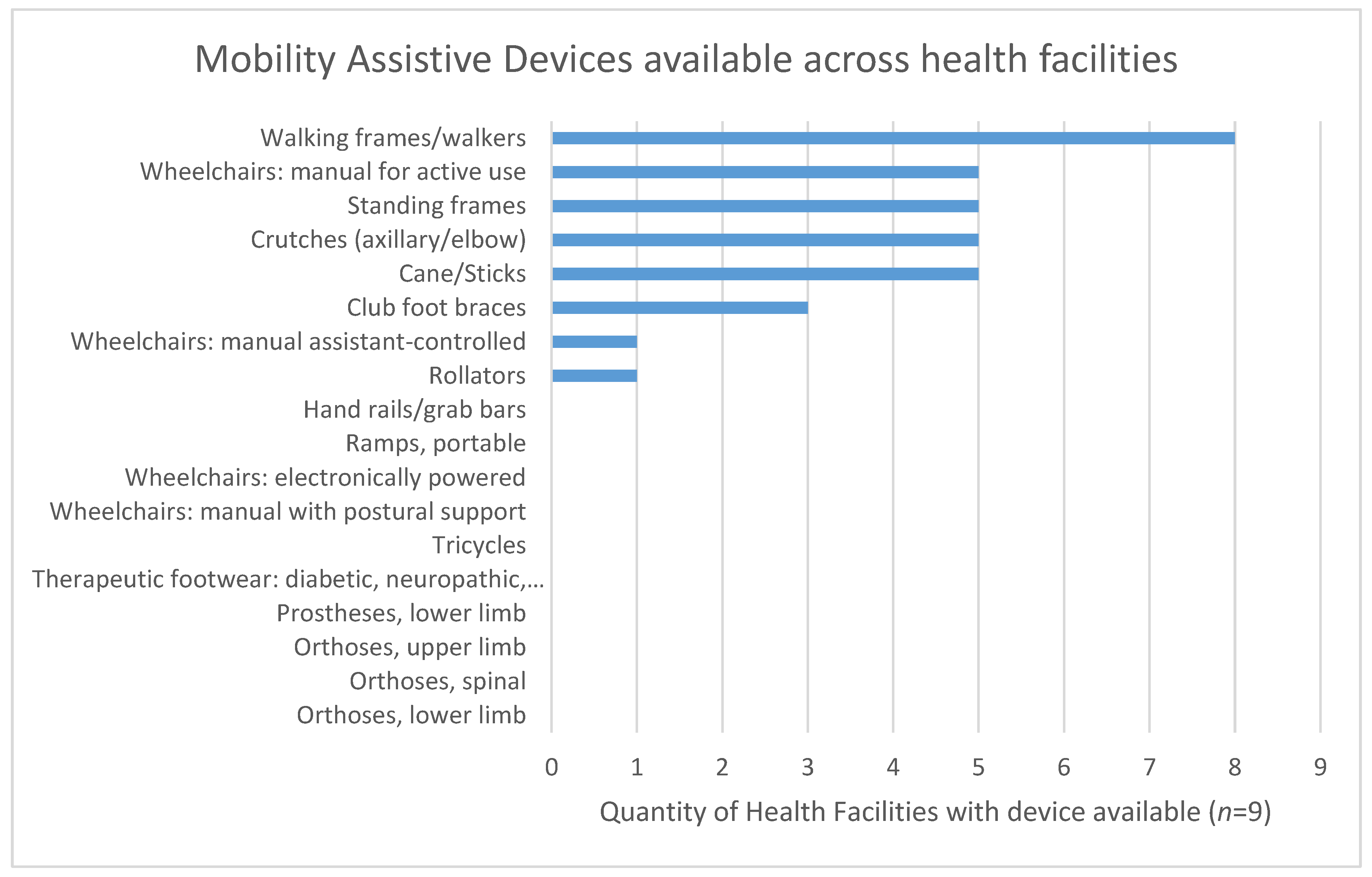
3.2. Assistive Devices
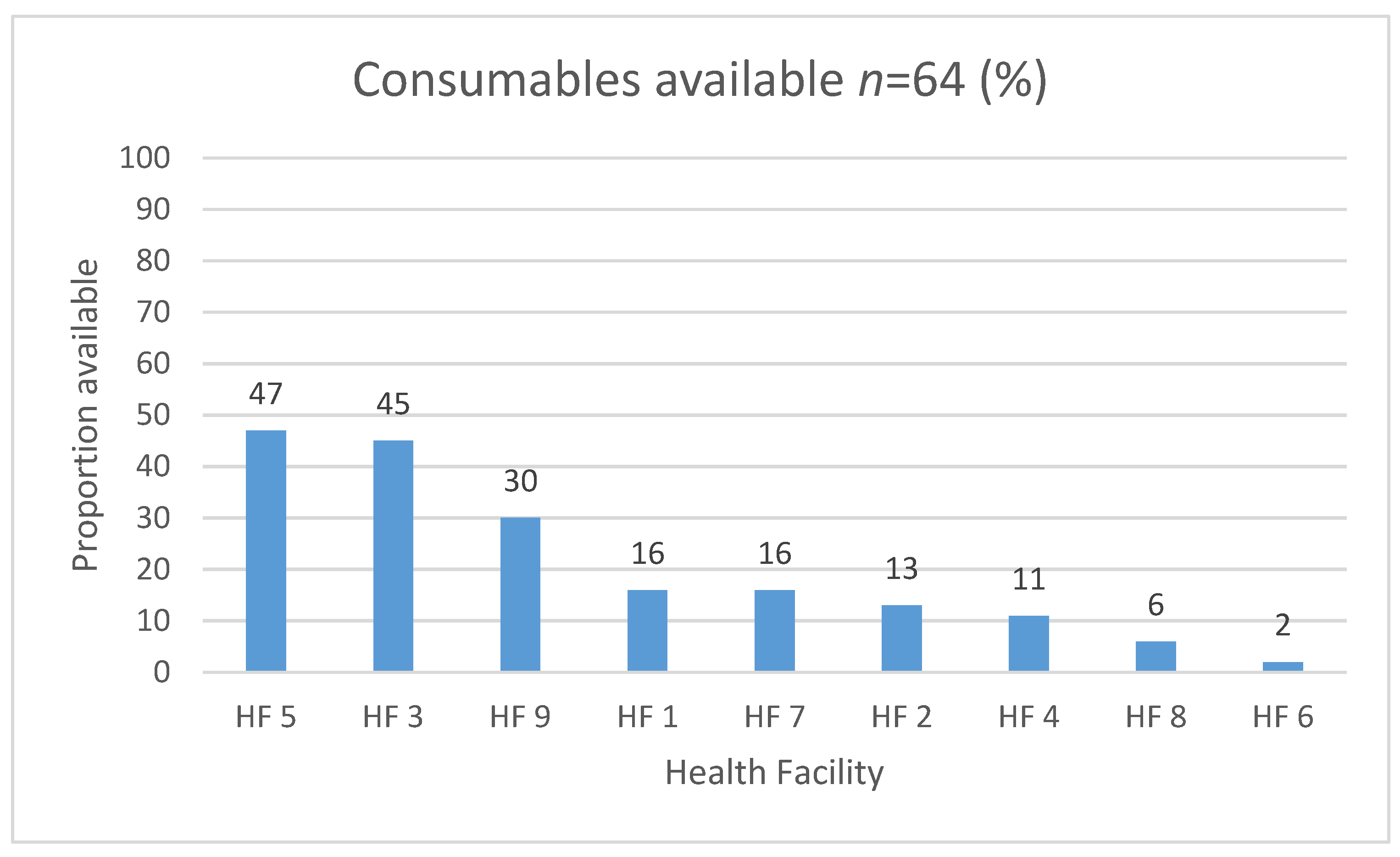
3.3. Consumables
3.4. Availability of Rehabilitation Providers
3.5. Accessibility of Rehabilitation Services
3.6. Barriers to Access
3.6.1. Referral Pathways
I only go to the clinic to check up on blood pressure, diabetes and arthritis. I have never been informed about such doctors (physiotherapists). Not even the doctor who referred me to the clinic that I am using.(Female, 75y, HF7)
I wish it was not only in (name) hospital where they focus on our type of sickness (impairment) because it gets really full there. All these surrounding hospitals send their patients to that one hospital.(Female, 35y, HF1)
3.6.2. Financial Considerations
I didn’t go because of financial constraints… I take two taxis and same applies too when I am coming back. And the taxi drops me off at (the taxi stop) and I would walk from there to here.(Male, 40y, HF5)
3.6.3. Transport and Road Considerations
Some of them (taxi drivers) leave you at the side of the road because you are not worth the trouble and some of them tell me that I have to pay for the wheelchair.(Female, 45y, HF5)
They (public transport) are scarce. And taxis are not conducive to my condition anyway(Female, 66y, Hf8)
3.6.4. Equipment Availability
There are no assistive devices for disabled people.(Female, 60y, HF2)
I was well-treated. She even told me that it was hard to get wheelchairs. It takes three years for one to get it.(Male, 39y, HF8)
I was taken out of the hospital on a wheelchair and then put in the car and the wheelchair was taken back to the hospital…There was no explanation given. We were told that the doctor who was supposed to give the wheelchair was on leave at that time.(Female, 70y, HF7)
As compared to previous times, now there are machines that can be used to exercise and they go the extra mile to make sure I get what I need.(Female, 45y, HF5)
It was not suitable for outdoor purposes (so) I was given a different wheelchair. There is a difference because the one I used before was not able to go outdoors, it was meant for indoor use only.(Male, 40y, HF3)
3.7. Consequences
When I wake up, Sisi (respectful term for older sister) lifts me up… I wake up and bathe. When I’m done, Sisi puts me on this chair to watch TV and then eat till evening. When it’s time to sleep, Sisi lifts me up again and puts me in bed. She does everything for me.(Female, 27y, HF2)
I just wish she could recover and get back to how she was because this is a burden.(Caregiver of Female, 27y, HF2)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Rehabilitation 2030: The Need to Scale up Rehabilitation. 2017. Available online: http://www.who.int/disabilities/care/rehab-2030/en/ (accessed on 27 April 2021).
- Louw, Q.; Twizeyemariya, A.; Grimmer, K.; Leibbrandt, D. Estimating the costs and benefits of stroke rehabilitation in South Africa. J. Eval. Clin. Pr. 2019, 26, 1181–1187. [Google Scholar] [CrossRef]
- Hashemi, G.; Kuper, H.; Wickenden, M. SDGs, Inclusive Health and the path to Universal Health Coverage. Disabil. Glob. S. 2017, 4, 1088–1111. Available online: www.dgsjournal.org (accessed on 4 May 2018).
- Bernhardt, J.; Urimubenshi, G.; Gandhi, D.B.C.; Eng, J.J. Stroke rehabilitation in low-income and middle-income countries: A call to action. Lancet 2020, 396, 1452–1462. [Google Scholar] [CrossRef]
- Jesus, T.S.; Landry, M.D.; Hoenig, H.; Zeng, Y.; Kamalakannan, S.; Britto, R.R.; Pogosova, N.; Sokolova, O.; Grimmer, K.; Louw, Q.A. Physical Rehabilitation Needs in the BRICS Nations from 1990 to 2017: Cross-National Analyses Using Data from the Global Burden of Disease Study. Int. J. Environ. Res. Public Health 2020, 17, 4139. [Google Scholar] [CrossRef] [PubMed]
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 2006–2017. [Google Scholar] [CrossRef]
- Kamaleri, Y.; Eide, A.H. Living Conditions among People with Disabilities in Lesotho: A National Representative Study. 2011. Available online: www.sintef.no (accessed on 29 March 2019).
- Bernabe-Ortiz, A.; Diez-Canseco, F.; Vasquez, A.; Miranda, J.J. Disability, caregiver’s dependency and patterns of access to rehabilitation care: Results from a national representative study in Peru. Disabil. Rehabil. 2015, 38, 582–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamalakannan, S.; Venkata, M.G.; Prost, A.; Natarajan, S.; Pant, H.; Chitalurri, N.; Goenka, S.; Kuper, H. Rehabilitation Needs of Stroke Survivors After Discharge from Hospital in India. Arch. Phys. Med. Rehabil. 2016, 97, 1526–1532.e9. [Google Scholar] [CrossRef] [Green Version]
- Matter, R.A.; Eide, A.H. Access to assistive technology in two Southern African countries. BMC Health Serv. Res. 2018, 18, 792. [Google Scholar] [CrossRef]
- Pryor, W.; Nguyen, L.; Islam, Q.N.; Jalal, F.A.; Marella, M. Unmet Needs and Use of Assistive Products in Two Districts of Bangladesh: Findings from a Household Survey. Int. J. Environ. Res. Public Health 2018, 15, 2901. [Google Scholar] [CrossRef] [Green Version]
- United Nations Realization of the Sustainable Development Goals by, for and with Persons with Disabilities: UN Flagship Report on Disability and Development 2018 (Advance Unedited Version). Available online: https://www.un.org/development/desa/disabilities/wp-content/uploads/sites/15/2018/12/UN-Flagship-Report-Disability.pdf (accessed on 4 August 2020).
- O.R. Tambo District Municipality. Integrated Development Plan, 2017–2022. 2017. Available online: http://www.nelsonmandelabay.gov.za/datarepository/documents/adopted-2016-2021-golden-five-years-idp-june-2016-web.pdf (accessed on 27 April 2021).
- OR Tambo District Municipality. Integrated Development Plan Review 2016/17. South Africa. Available online: https://www.ortambodm.gov.za/folder.php?id=INjwf2vAj. (accessed on 27 April 2021).
- Massyn, N.; Tanna, G.; Day, C.; Ndlovu, N. District Health Barometer: District Health Profiles 2018/19; Health Systems Trust: Durban, South African, 2020. [Google Scholar]
- IHME. South Africa. 2020. Available online: http://www.healthdata.org/south-africa (accessed on 15 April 2021).
- Statistics South Africa Census 2011: Profile of Persons with Disabilities in South Africa. Pretoria, 2014. Available online: www.statssa.gov.za (accessed on 12 October 2018).
- Department of Health. Primary Health Care Facilities and Services. 2019. Available online: https://www.healthestablishments.org.za/Home/Facility (accessed on 27 March 2020).
- Gupta, N.; Castillo-Laborde, C.; Landry, M.D. Health-related rehabilitation services: Assessing the global supply of and need for human resources. BMC Health Serv. Res. 2011, 11, 276. [Google Scholar] [CrossRef] [Green Version]
- Mitra, S. The Capability Approach and Disability. J. Disabil. Policy Stud. 2006. Available online: https://0-search-proquest-com.brum.beds.ac.uk/docview/211211409/fulltextPDF/81DCE5AAB26E4B9EPQ/1?accountid=13042 (accessed on 7 March 2018).
- Alkire, S. The Capability Approach to the Quality of Life. Available online: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.667.8228&rep=rep1&type=pdf. (accessed on 15 April 2021).
- Robeyns, I. An Unworkable Idea or a Promising Alternative? Sen’s Capability Approach Re-examined. Cambridge, UK, 2000. Available online: http://www.econ.kuleuven.be/ces/discussionpapers/default.htm (accessed on 28 February 2017).
- Bickenbach, J. Reconciling the capability approach and the ICF. Alter 2014, 8, 10–23. [Google Scholar] [CrossRef] [Green Version]
- Tellez, J.; Krishnakumar, J.; Bungener, M.; Le Galès, C. Capability deprivation of people with Alzheimer’s disease: An empirical analysis using a national survey. Soc. Sci. Med. 2016, 151, 56–68. [Google Scholar] [CrossRef]
- Trani, J.-F.; Bakhshi, P.; Brown, D.; Lopez, D.; Gall, F. Disability as deprivation of capabilities: Estimation using a large-scale survey in Morocco and Tunisia and an instrumental variable approach. Soc. Sci. Med. 2018, 211, 48–60. [Google Scholar] [CrossRef]
- Borg, J.; Östergren, P.-O.; Larsson, S.; Rahman, A.A.; Bari, N.; Khan, A.N. Assistive technology use is associated with reduced capability poverty: A cross-sectional study in Bangladesh. Disabil. Rehabil. Assist. Technol. 2011, 7, 112–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherry, K. Occupations of Citizenship: The Missing Layer in Empowered Engagement between Rural People with Disabilities and Primary Healthcare Workers in South Africa. Ph.D. Thesis, University of Cape Town, Cape Town, South Africa, 2016. Available online: https://open.uct.ac.za/bitstream/item/23177/thesis_hsf_2016_sherry_kate.pdf?sequence=1 (accessed on 17 November 2017).
- DHS Program. Service Provision Assessment Survey: Inventory Questionnaire. 2014. Available online: https://dhsprogram.com/publications/publication-spaq1-spa-questionnaires-and-manuals.cfm (accessed on 27 April 2021).
- WHO. Service Availability and Readiness Assessment [SARA]: An Annual Monitoring System for Service Delivery. In Implementation Guide, Version 2.2; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Health Systems Trust. The National Health Care Facilities Baseline Audit; National Summary Report: Durban, South African, 2013. [Google Scholar]
- WHO. Priority Assistive Products List, The GATE Initiative; WHO: Geneva, Switzerland, 2016. [Google Scholar] [CrossRef]
- ATscale. ATscale: Global Partnership for Assistive Technology. 2018. Available online: https://atscale2030.org/global-partnership (accessed on 23 November 2020).
- Department of Health. National Health Commodities Catalogue for Primary Health Care Facilities; South African National Department of Health: Pretoria, South African, 2018. [Google Scholar]
- Pope, C.; Mays, N. The Role of Theory in Qualitative Research. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/abs/10.1002/9781119410867.ch2 (accessed on 15 April 2021).
- Guba, E.G.; Lincoln, Y.S. Competing Paradigms in Qualitative Research. In Handbook of Qualitative Research; Sage: Thousand Oaks, CA, USA, 1994; pp. 105–117. [Google Scholar]
- Neuman, L.W. Social Research Methods: Qualitative and Quantitative Approaches, 7th ed.; Pearson Education Limited: Essex, UK, 2014; Available online: www.pearsoned.co.uk (accessed on 28 November 2018).
- Hinton, L.; Ryan, S. Interviews. Qualitative Research in Health Care. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/abs/10.1002/9781119410867.ch4 (accessed on 1 October 2020).
- Washington Group. Washington Group-Extended Question Set on Functioning (WG ES-F); Washington Group: Budapest, Hungary, 2011; pp. 1–11. [Google Scholar]
- Washington Group on Disability Statistics. Understanding and Interpreting Disability as Measured using the WG Short Set of Questions. Available online: https://www.cdc.gov/nchs/data/washington_gro (accessed on 15 April 2021).
- MacTaggart, I.; Kuper, H.; Murthy, G.V.S.; Oye, J.; Polack, S. Measuring Disability in Population Based Surveys: The Interrelationship between Clinical Impairments and Reported Functional Limitations in Cameroon and India. PLoS ONE 2016, 11, e0164470. [Google Scholar] [CrossRef] [Green Version]
- WHO. Key Components of a Well Functioning Health System. Geneva, 2010. Available online: http://www.who.int/healthsystems/EN_HSSkeycomponents.pdf?ua=1 (accessed on 16 July 2018).
- QSR International. Nvivo 11; QSR International Pty Ltd.: Doncaster, UK, 2017. [Google Scholar]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis: Striving to Meet the Trustworthiness Criteria. Int. J. Qual. Methods 2017, 16, 1. [Google Scholar] [CrossRef]
- Pope, C.; Ziebland, S.; Mays, N. Analysis. In Qualitative Research in Health Care, 4th ed.; Pope, C., Mays, N., Eds.; John Wiley and Sons Ltd.: Hoboken, NJ, USA, 2020; pp. 111–133. [Google Scholar]
- Visagie, S.; Scheffler, E.; Schneider, M. Policy implementation in wheelchair service delivery in a rural South African setting. Afr. J. Disabil. 2013, 2, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bright, T.; Wallace, S.; Kuper, H. A Systematic Review of Access to Rehabilitation for People with Disabilities in Low- and Middle-Income Countries. Int. J. Environ. Res. Public Health 2018, 15, 2165. [Google Scholar] [CrossRef] [Green Version]
- Department of Health. Standardisation of Provision of Assistive Devices in South Africa: A Guideline for use in the Public Sector. Pretoria, 2003. Available online: http://uhambofoundation.org.za/new_wp/wp-content/uploads/2016/06/standardisation_of_provision_of_assistive_devices_in_south_.pdf (accessed on 18 March 2019).
- Department of Health. National Core Standards for Health Establishments in South Africa. Tshwane, 2011. Available online: http://www.rhap.org.za/wp-content/uploads/2014/05/National-Core-Standards-2011-1.pdf (accessed on 19 March 2019).
- Department of Health. Ideal Hospital Realisation and Maintenance Framework Manual: Version 1. South Africa, 2018. Available online: https://www.idealhealthfacility.org.za/docs/hospital/v1/Ideal Hospital Realisation And Maintenance Framework Manual.pdf (accessed on 27 April 2021).
- Maart, S.; Jelsma, J. Disability and access to health care—A community based descriptive study. Disabil. Rehabil. 2013, 36, 1489–1493. [Google Scholar] [CrossRef] [PubMed]
- Hlayisi, V.-G.; Ramma, L. Rehabilitation for disabling hearing loss: Evaluating the need relative to provision of hearing aids in the public health care system. Disabil. Rehabil. 2018, 41, 2704–2707. [Google Scholar] [CrossRef]
- Magnusson, L. Professionals’ perspectives of prosthetic and orthotic services in Tanzania, Malawi, Sierra Leone and Pakistan. Prosthet. Orthot. Int. 2019, 43, 500–507. [Google Scholar] [CrossRef] [PubMed]
- MacLachlan, M.; Scherer, M.J. Systems thinking for assistive technology: A commentary on the GREAT summit. Disabil. Rehabil. Assist. Technol. 2018, 13, 492–496. [Google Scholar] [CrossRef] [Green Version]
- National Department of Health. 2030 Human Resources for Health Strategy: Investing in the Health Workforce for Universal Health Coverage. Available online: https://www.spotlightnsp.co.za/wp-content/uploads/2020/08/2030-HRH-strategy-19-3-2020.pdf (accessed on 27 April 2021).
- Kamenov, K.; Mills, J.-A.; Chatterji, S.; Cieza, A. Needs and unmet needs for rehabilitation services: A scoping review. Disabil. Rehabil. 2019, 41, 1227–1237. [Google Scholar] [CrossRef]
- Cartmill, L.; Comans, T.; Clark, M.J.; Ash, S.; Sheppard, L. Using staffing ratios for workforce planning: Evidence on nine allied health professions. Hum. Resour. Health 2012, 10, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moodley, J.; Ross, E. Inequities in health outcomes and access to health care in South Africa: A comparison between persons with and without disabilities. Disabil. Soc. 2015, 30, 630–644. [Google Scholar] [CrossRef]
- Dulhanty, L.H.; Hulme, S.; Vail, A.; Patel, H.C.; Tyson, S.F. The self-reported needs of patients following subarachnoid hemorrhage (SAH). Disabil. Rehabil. 2020, 42, 3450–3456. [Google Scholar] [CrossRef] [PubMed]
- Mlenzana, N.B.; Frantz, J.M.; Rhoda, A.J.; Eide, A.H. Barriers to and facilitators of rehabilitation services for people with physical disabilities: A systematic review. Afr. J. Disabil. 2013, 2, 6. [Google Scholar] [CrossRef]
- Kumurenzi, A.; Goliath, C.; Mji, G.; Mlenzana, N.; Joseph, C.; Stathum, S.; Rhoda, A. Experiences of patients and service providers with out-patient rehabilitation services in a rehabilitation centre in the Western Cape Province. Afr. J. Disabil. 2015, 4, 7. [Google Scholar] [CrossRef] [Green Version]
- Visagie, S.; Swartz, L. Rural South Africans’ rehabilitation experiences: Case studies from the Northern Cape Province. South Afr. J. Physiother. 2016, 72. [Google Scholar] [CrossRef] [Green Version]
- Visagie, S.; Eide, A.H.; Dyrstad, K.; Mannan, H.; Swartz, L.; Schneider, M.; Mji, G.; Munthali, A.; Khogali, M.; Van Rooy, G.; et al. Factors related to environmental barriers experienced by persons with and without disabilities in diverse African settings. PLoS ONE 2017, 12, e0186342. [Google Scholar] [CrossRef] [Green Version]
- Hanass-Hancock, J.; Nene, S.; Deghaye, N.; Pillay, S. ‘These are not luxuries, it is essential for access to life’: Disability related out-of-pocket costs as a driver of economic vulnerability in South Africa. Afr. J. Disabil. 2017, 6, 10. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, G.; Wickenden, M.; Bright, T.; Kuper, H. Barriers to accessing primary healthcare services for people with disabilities in low and middle-income countries, a Meta-synthesis of qualitative studies. Disabil. Rehabil. 2020, 1–14. [Google Scholar] [CrossRef]
- Banks, L.M.; Kuper, H.; Polack, S. Poverty and Disability in Low- and Middle-Income Countries: A Systematic Review. Available online: https://dx.plos.org/10.1371/journal.pone.0189996 (accessed on 21 April 2021).
- Department of Social Development. Elements of the Financial and Economic Costs of Disability to Households in South Africa: A Pilot Study. Pretoria, 2015. Available online: https://www.unicef.org/southafrica/media/2221/file/ZAF-Elements-of-the-financial-and-economic-costs-of-disability-to-households-in-South-Africa-2015.pdf (accessed on 29 September 2020).
- Banks, L.M.; Polack, S. The Economic Costs of Exclusion and Gains of Inclusion of People with Disabilities: Evidence from Low and Middle Income Countries; International Centre for Evidence in Disability: London, UK, 2013. [Google Scholar]
- Zuurmond, M.; MacTaggart, I.; Kannuri, N.; Murthy, G.; Oye, J.E.; Polack, S. Barriers and Facilitators to Accessing Health Services: A Qualitative Study Amongst People with Disabilities in Cameroon and India. Int. J. Environ. Res. Public Health 2019, 16, 1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Rehabilitation Service | Number of Health Facilities (n = 9) |
|---|---|
| Physiotherapy | 9 |
| Occupational therapy | 6 |
| Speech and Language therapy | 2 |
| Audiology | 2 |
| Orthotics and Prosthetics | 0 |
| Wheelchairs | Hearing Aids | Spectacles | Prosthetics | Smart Products | |
|---|---|---|---|---|---|
| Health Facilities (n = 9) | 5 | 2 | 0 | 0 | 0 |
| Profession | HF 1 | HF 2 | HF 3 | HF 4 | HF 5 | HF 6 | HF 7 | HF 8 | HF 9 | TOTAL |
|---|---|---|---|---|---|---|---|---|---|---|
| Physiotherapists | 2 | 2 | 4 | 1 | 1 | 1 | 1 | 1 | 1 | 14 |
| Occupational Therapists | 2 | 2 | 3 | 0 | 1 | 0 | 1 | 0 | 1 | 10 |
| Speech & Language Therapists | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 2 |
| Audiologists | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 2 |
| Orthotist and Prosthetists | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Rehabilitation Physicians | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Rehabilitation Nurses | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Physiotherapy Assistant | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 2 |
| TOTAL | 5 | 4 | 9 | 1 | 2 | 1 | 3 | 2 | 3 | 30 |
| Characteristics | Number (Total = 48) |
|---|---|
| Gender | Females [21] males [27] |
| Age | 49 years (average) (range 24–83 years) |
| Education | Incomplete primary [29] Complete primary [4] Incomplete secondary [11] Complete secondary [2] Complete post-secondary [2] |
| Disability Grant | 46 recipients 1 does not qualify 1 in process of application |
| Assistive device use (combinations possible) | wheelchairs [24] crutches [20] walking sticks [6] orthotics [4] walking frames [3] prosthetic devices [2] no assistive device [1] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magaqa, Q.; Ariana, P.; Polack, S. Examining the Availability and Accessibility of Rehabilitation Services in a Rural District of South Africa: A Mixed-Methods Study. Int. J. Environ. Res. Public Health 2021, 18, 4692. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094692
Magaqa Q, Ariana P, Polack S. Examining the Availability and Accessibility of Rehabilitation Services in a Rural District of South Africa: A Mixed-Methods Study. International Journal of Environmental Research and Public Health. 2021; 18(9):4692. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094692
Chicago/Turabian StyleMagaqa, Qhayiya, Proochista Ariana, and Sarah Polack. 2021. "Examining the Availability and Accessibility of Rehabilitation Services in a Rural District of South Africa: A Mixed-Methods Study" International Journal of Environmental Research and Public Health 18, no. 9: 4692. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094692