
A Qualitative Analysis of Motivators to Participation in Suicide-Focused Research from a Community-Based Australian Sample

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Participants
2.3. Data Collection
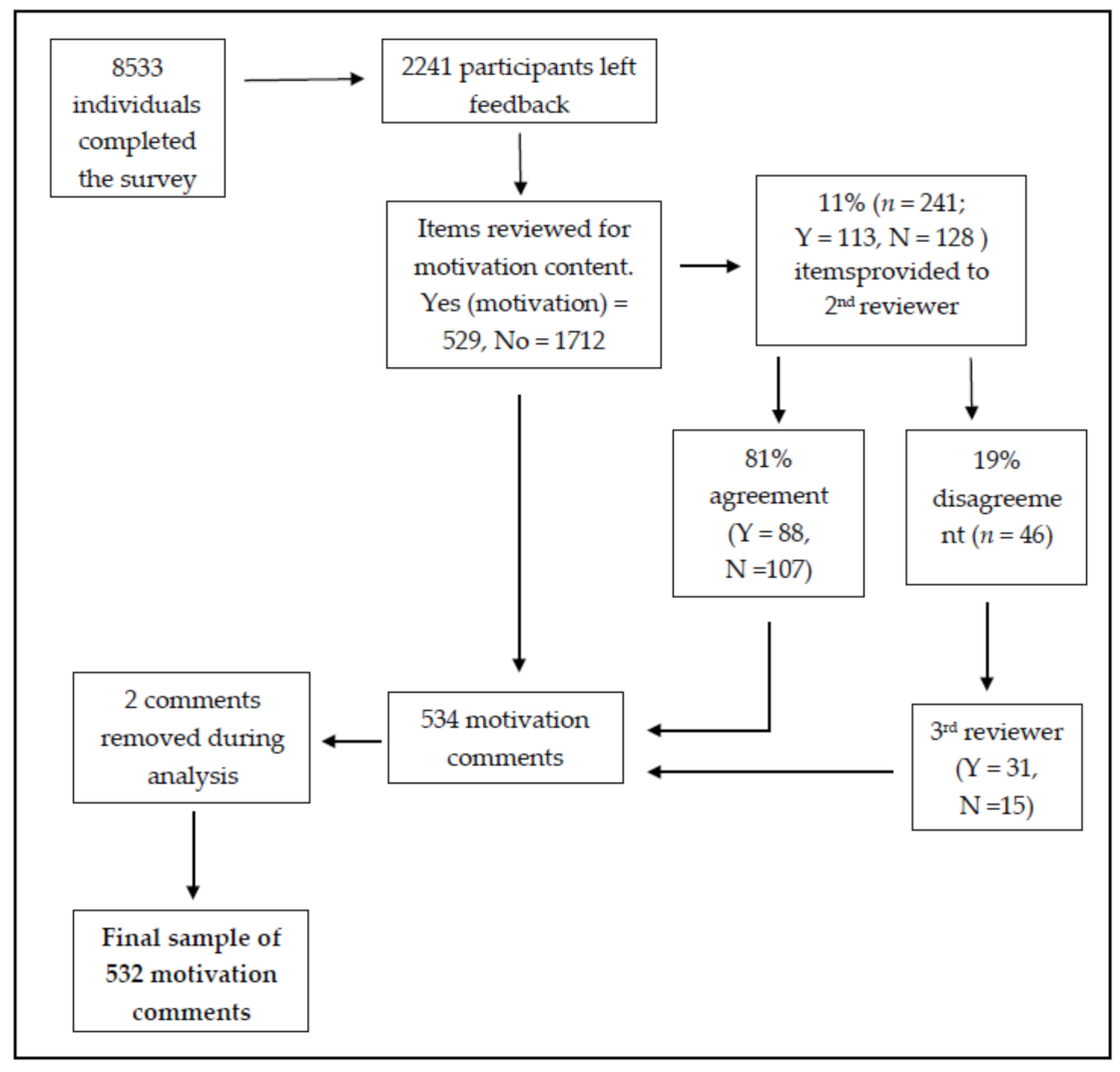
2.4. Procedure
- Motivation—included responses that explicitly indicated motivation or decision to participate, such as “my motivation was”, “I participated because”, “I chose to do the survey because”.
- Not Motivation—responses that did not mention motivation explicitly (i.e., referenced other aspects of the prompt), such as suggested changes to survey structure, participants further explaining their responses or stance on suicide, and/or comments of commendation and support to researchers.
2.5. Data Analysis
3. Results
3.1. Participant Demographics and Representativeness
3.2. Thematic Network Analysis
3.2.1. Altruism
3.2.2. Solve Systemic Problems
“I was motivated to participate because I believe the stigma surrounding mental health needs to be eradicated. I believe if we normalise positive mental health practices and conversations like we have other health issues such as skin cancer (slip slop slap campaign), obesity and nutrition, and smoking, then the number of consumers needing to access mental health resources will be less fearful or cautious in doing so”.
“I am participating because I very strongly believe mental health in Australia needs to be far better resourced and taken far more seriously by both the government and society as a whole. I would like it if everyone had access to the same resources for more robust mental health that I was able to access. (…) To me this is completely unacceptable that anyone in our current society should be unable to seek the help required in a timely fashion due purely to their economic position”.
3.2.3. Lived Experience
“Motivation? I used to believe that people who took their own lives were weak, and cowards. But I know(sic) understand that they see ending their lives as the ONLY answer to completely overwhelming situations where they have no control, and really believe that their family and friends are better off without them. I’ve been in this dark place many times”.
3.2.4. Seeking Personal Insight
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Naghavi, M. Global, regional, and national burden of suicide mortality 1990 to 2016: Systematic analysis for the Global Burden of Disease Study 2016. BMJ 2019, 364, l94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumberg, S.J.; Luke, J.V.; Ganesh, N.; Davern, M.E.; Boudreaux, M.H. Wireless substitution: State-level estimates from the National Health Interview Survey, 2010–2011. Natl. Health Stat. Rep. 2012, 61, 1–15. [Google Scholar]
- Batterham, P.J. Recruitment of mental health survey participants using Internet advertising: Content, characteristics and cost effectiveness. Int. J. Methods Psychiatr. Res. 2014, 23, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Jang, M.; Vorderstrasse, A. Socioeconomic Status and Racial or Ethnic Differences in Participation: Web-Based Survey. JMIR Res. Protoc. 2019, 8, e11865. [Google Scholar] [CrossRef]
- Whitaker, C.J.; Stevelink, S.; Fear, N.T. The Use of Facebook in Recruiting Participants for Health Research Purposes: A Systematic Review. J. Med Internet Res. 2017, 19, e290. [Google Scholar] [CrossRef] [Green Version]
- Heiervang, E.; Goodman, R. Advantages and limitations of web-based surveys: Evidence from a child mental health survey. Soc. Psychiatry Psychiatr. Epidemiol. 2009, 46, 69–76. [Google Scholar] [CrossRef]
- Lee, S.; Torok, M.; Shand, F.; Chen, N.; McGillivray, L.; Burnett, A.; Larsen, M.E.; Mok, K. Performance, Cost-Effectiveness, and Representativeness of Facebook Recruitment to Suicide Prevention Research: Online Survey Study. JMIR Ment. Health 2020, 7, e18762. [Google Scholar] [CrossRef]
- Brick, J.M.; Williams, D. Explaining Rising Nonresponse Rates in Cross-Sectional Surveys. Ann. Am. Acad. Political Soc. Sci. 2012, 645, 36–59. [Google Scholar] [CrossRef]
- Czajka, J.L.; Beyler, A. Background paper declining response rates in federal surveys: Trends and implications. Math. Policy Res. 2016, 1, 1–86. [Google Scholar]
- Bailey, E.; Teh, Z.; Bleeker, C.; Simmons, M.; Robinson, J. Youth partnerships in suicide prevention research: A failed investigator survey. Early Interv. Psychiatry 2020. [Google Scholar] [CrossRef]
- Gibson, S.; Boden, Z.V.R.; Benson, O.; Brand, S.L. The Impact of Participating in Suicide Research Online. Suicide Life Threat. Behav. 2014, 44, 372–383. [Google Scholar] [CrossRef] [Green Version]
- Maple, M.; Sanford, R. Suicide exposure and impact within a non-representative Australian community sample. Death Stud. 2019, 44, 329–337. [Google Scholar] [CrossRef]
- Biddle, L.; Cooper, J.; Owen-Smith, A.; Klineberg, E.; Bennewith, O.; Hawton, K.; Kapur, N.; Donovan, J.; Gunnell, D. Qualitative interviewing with vulnerable populations: Individuals’ experiences of participating in suicide and self-harm based research. J. Affect. Disord. 2013, 145, 356–362. [Google Scholar] [CrossRef]
- Dyregrov, K.; Dieserud, G.; Straiton, M.; Rasmussen, M.L.; Hjelmeland, H.; Knizek, B.L.; Leenaars, A.A. Motivation for Research Participation among People Bereaved by Suicide. Omega J. Death Dying 2011, 62, 149–168. [Google Scholar] [CrossRef]
- Wong, P.W.C.; Chan, W.S.C.; Beh, P.S.L.; Yau, F.W.S.; Yip, P.S.F.; Hawton, K. Research Participation Experiences of Informants of Suicide and Control Cases. Crisis 2010, 31, 238–246. [Google Scholar] [CrossRef]
- Woodall, A.; Howard, L.; Morgan, C. Barriers to participation in mental health research: Findings from the Genetics and Psychosis (GAP) Study. Int. Rev. Psychiatry 2011, 23, 31–40. [Google Scholar] [CrossRef]
- Maple, M.; Wayland, S.; Sanford, R.; Spillane, A.; Coker, S. Carers’ Motivations for, and Experiences of, Participating in Suicide Research. Int. J. Environ. Res. Public Health 2020, 17, 1733. [Google Scholar] [CrossRef] [Green Version]
- Cerel, J.; Brown, M.M.; Maple, M.; Singleton, M.; Van De Venne, J.; Moore, M.; Flaherty, C. How Many People Are Exposed to Suicide? Not Six. Suicide Life Threat. Behav. 2018, 49, 529–534. [Google Scholar] [CrossRef]
- Cerel, J.; Maple, M.; Van De Venne, J.; Moore, M.; Flaherty, C.; Brown, M. Exposure to Suicide in the Community: Prevalence and Correlates in One U.S. State. Public Health Rep. 2016, 131, 100–107. [Google Scholar] [CrossRef] [Green Version]
- Maple, M.; McKay, K.; Sanford, R. The Attempt Was My Own! Suicide Attempt Survivors Respond to an Australian Community-Based Suicide Exposure Survey. Int. J. Environ. Res. Public Health 2019, 16, 4549. [Google Scholar] [CrossRef] [Green Version]
- Ellis, L.A.; McCabe, K.L.; Rahilly, K.A.; Nicholas, M.A.; Davenport, T.A.; Burns, J.M.; Hickie, I.B. Encouraging young men’s participation in mental health research and treatment: Perspectives in our technological age. Clin. Investig. 2014, 4, 881–888. [Google Scholar] [CrossRef]
- Canetto, S.S.; Sakinofsky, I. The gender paradox in suicide. Suicide Life Threat. Behavior. 1998, 28, 1–23. [Google Scholar] [CrossRef]
- Crestani, C.; Masotti, V.; Corradi, N.; Schirripa, M.L.; Cecchi, R.; Carlo, C.; Vittoria, M.; Natalia, C.; Maria, L.S.; Rossana, C. Suicide in the elderly: A 37-years retrospective study. Acta Bio Med. Atenei Parm. 2019, 90, 68–76. [Google Scholar] [CrossRef]
- Fairweather, A.K.; Anstey, K.J.; Rodgers, B.; Butterworth, P. Factors distinguishing suicide attempters from suicide ideators in a community sample: Social issues and physical health problems. Psychol. Med. 2006, 36, 1235–1245. [Google Scholar] [CrossRef]
- Malakouti, S.K.; Nojomi, M.; Bolhari, J.; Hakimshooshtari, M.; Poshtmashhadi, M.; De Leo, D. Prevalence of Suicide Thoughts, Plans and Attempts in a Community Sample from Karaj, Iran. Community Ment. Health J. 2008, 45, 37–41. [Google Scholar] [CrossRef] [Green Version]
- Shand, F.; Torok, M.; Cockayne, N.; Batterham, P.J.; Calear, A.L.; MacKinnon, A.; Martin, D.; Zbukvic, I.; Mok, K.; Chen, N.; et al. Protocol for a stepped-wedge, cluster randomized controlled trial of the LifeSpan suicide prevention trial in four communities in New South Wales, Australia. Trials 2020, 21, 332. [Google Scholar] [CrossRef]
- McAlister, A.; Lee, D.; Ehlert, K.; Kajfez, R.; Faber, C.; Kennedy, M. Qualitative Coding: An Approach to Assess Inter-Rater Reliability. In Proceedings of the 2017 ASEE Annual Conference & Exposition, Columbus, OH, USA, 25–28 June 2018. [Google Scholar]
- Mauthner, N.S.; Doucet, A. Reflexive Accounts and Accounts of Reflexivity in Qualitative Data Analysis. Sociology 2003, 37, 413–431. [Google Scholar] [CrossRef] [Green Version]
- Attride-Stirling, J. Thematic networks: An analytic tool for qualitative research. Qual. Res. 2001, 1, 385–405. [Google Scholar] [CrossRef]
- Batson, C.D.; Powell, A.A. Altruism and Prosocial Behavior. In Handbook of Psychology; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2003; pp. 463–484. [Google Scholar] [CrossRef]
- McCann, S.K.; Campbell, M.K.; Entwistle, V.A. Reasons for participating in randomised controlled trials: Conditional altruism and considerations for self. Trials 2010, 11, 31. [Google Scholar] [CrossRef] [Green Version]
- Maple, M.; Edwards, H.; Plummer, D.; Minichiello, V. Silenced voices: Hearing the stories of parents bereaved through the suicide death of a young adult child. Health Soc. Care Community 2009, 18, 241–248. [Google Scholar] [CrossRef]
- Andriessen, K.; Krysinska, K.; Draper, B.; Dudley, M.; Mitchell, P.B. Harmful or Helpful? A Systematic Review of How Those Bereaved Through Suicide Experience Research Participation. Crisis 2018, 39, 364–376. [Google Scholar] [CrossRef] [PubMed]
- Kingston, D.; Austin, M.-P.; Van Zanten, S.V.; Harvalik, P.; Giallo, R.; McDonald, S.D.; MacQueen, G.; Vermeyden, L.; Lasiuk, G.; Sword, W.; et al. Pregnant Women’s Views on the Feasibility and Acceptability of Web-Based Mental Health E-Screening Versus Paper-Based Screening: A Randomized Controlled Trial. J. Med Internet Res. 2017, 19, e88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradley, M.; Braverman, J.; Harrington, M.; Wicks, P. Patients’ motivations and interest in research: Characteristics of volunteers for patient-led projects on PatientsLikeMe. Res. Involv. Engag. 2016, 2, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Saleh, A.; Bista, K. Examining Factors Impacting Online Survey Response Rates in Educational Research: Perceptions of Graduate Students. J. Multidiscip. Eval. 2017, 13, 63–74. [Google Scholar]
- Watling, D.; Preece, M.; Hawgood, J.; Bloomfield, S.; Kõlves, K. Developing an Intervention for Suicide Prevention: A Rapid Review of Lived Experience Involvement. Arch. Suicide Res. 2020. [Google Scholar] [CrossRef]
- Warner, C.H.; Appenzeller, G.N.; Grieger, T.; Belenkiy, S.; Breitbach, J.; Parker, J.; Warner, C.M.; Hoge, C. Importance of anonymity to encourage honest reporting in mental health screening after combat deployment. Arch. Gen. Psychiatry 2011, 68, 1065–1071. [Google Scholar] [CrossRef] [Green Version]
- Alexander, S.; Pillay, R.; Smith, B. A systematic review of the experiences of vulnerable people participating in research on sensitive topics. Int. J. Nurs. Stud. 2018, 88, 85–96. [Google Scholar] [CrossRef] [Green Version]
- Blades, C.A.; Stritzke, W.G.; Page, A.C.; Brown, J.D. The benefits and risks of asking research participants about suicide: A meta-analysis of the impact of ex-posure to suicide-related content. Clin. Psychol. Rev. 2018, 64, 1–12. [Google Scholar] [CrossRef]
- Omerov, P.; Steineck, G.; Dyregrov, K.; Runeson, B.; Nyberg, U. The ethics of doing nothing. Suicide-bereavement and research: Ethical and methodological considerations. Psychol. Med. 2013, 44, 3409–3420. [Google Scholar] [CrossRef] [Green Version]
- Hjelmeland, H.; Knizek, B.L. Why We Need Qualitative Research in Suicidology. Suicide Life Threat. Behav. 2010, 40, 74–80. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Motivation Comment | All Participants | Motivation Comments Versus All Participants | |||
|---|---|---|---|---|---|
| n (%) | n (%) | Chi-Square (df, n) | p Value | ||
| Gender | |||||
| Female | 344 (65.0) | 5675 (67.2) | 1.08 (df = 1, n = 8972) | 0.299 | |
| Male | 185 (35.0) | 2768 (32.8) | |||
| Age | |||||
| 18–34 years | 140 (26.5) | 2413 (28.6) | 4.51 (df = 2, n = 8977) | 0.105 | |
| 35–59 years | 299 (56.6) | 4882 (57.8) | |||
| 60+ years | 89 (16.9) | 1154 (13.7) | |||
| Relationship status | |||||
| Never coupled | 133 (21.2) | 2012 (23.8) | 2.05 (df = 2, n = 8996) | 0.359 | |
| Coupled | 321 (60.3) | 4871 (57.6) | |||
| No longer coupled | 98 (18.4) | 1581 (18.7) | |||
| Employment status | |||||
| Full-time | 220 (41.4) | 3836 (45.3) | 3.53 (df = 2, n = 8991) | 0.172 | |
| Part-time | 144 (27.1) | 2228 (26.3) | |||
| Unemployed | 167 (31.5) | 2396 (28.3) | |||
| Education | |||||
| School-based | 136 (25.7) | 1860 (21.9) | 5.48 (df = 2, n = 9024) | 0.065 | |
| Undergraduate | 327 (61.7) | 5343 (62.9) | |||
| Postgraduate | 67 (12.6) | 1291 (15.2) | |||
| Previous mental health diagnosis | |||||
| No | 148 (27.8) | 2819 (33.2) | 6.55 (df = 1, n = 9025) | 0.010 * | |
| Yes | 384 (72.2) | 5674 (66.8) | |||
| Network | Global Themes | Organising Themes | |
|---|---|---|---|
| 1 | Altruism (n = 187) | Help Other People | Participated due to wanting to help other people or the community, or specifically people with mental health concerns. Some wanted to use their personal experience to help others. |
| Desire to Help | Broad desire to help with no specific target and considered the survey an easy way to provide help. | ||
| Hopeful to Provide Help | Hopeful contribution will be of help, to other people, or to no specific target. | ||
| External Motivation Source | Participated due to a friend’s request or because of a positive association with the institute conducting the research. | ||
| 2 | Solve Systemic Problems (n = 195) | Want to Solve Identified Problem | Participants saw partaking in the survey as a method to help address problems such as the need to raise awareness, to change attitude and stigma around suicide, assist suicide prevention, and increase and/or improve services. |
| Add to Suicide Knowledge | Adding to the knowledge and understanding of suicide, and the role of assisting researchers in that, were motivators. One participant was motivated by a desire to share their negative view of suicide. | ||
| 3 | Lived Experience (n = 229) | Personal Experience | Personal experience with suicide attempts, suicidal thoughts, and mental health motivated participants through connection to the survey content. |
| Loved One with Personal Experience | Experience of a loved one with suicidal thoughts and actions motivated participants through a desire to ensure resources were available to help their loved ones. Having a loved one with mental health issues, as well as suicidal thoughts or behaviours, created a stronger awareness in participants, encouraging their participation. | ||
| Bereaved by Suicide | Knowing someone who has died by suicide drove motivation to participate through participants increased knowledge and strong emotional reactions to the loss. | ||
| Professional Experience | Working in a mental health profession or support role, as well as being exposed to training or education in suicide, increased participant awareness of suicide and motivated participation. Employment in a profession at high risk of suicide also acted as motivation due to the increased awareness of the impacts of suicide. | ||
| 4 | Seeking Personal Insight (n = 23) | Intellectual Inquisitiveness | Participant interest in and curiosity about mental health research, the process involved, and the nature of the questions asked. |
| Clarity of Oneself | Using the participation in the survey as a way of making sense of individual’s own thoughts or experiences with suicide. Participation was also seen as an avenue to self-improvement. | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rheinberger, D.; Shand, F.; Mok, K.; McGillivray, L.; Maple, M.; Burnett, A.; Sharwood, L.N.; Chen, N.A.; Torok, M. A Qualitative Analysis of Motivators to Participation in Suicide-Focused Research from a Community-Based Australian Sample. Int. J. Environ. Res. Public Health 2021, 18, 4705. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094705
Rheinberger D, Shand F, Mok K, McGillivray L, Maple M, Burnett A, Sharwood LN, Chen NA, Torok M. A Qualitative Analysis of Motivators to Participation in Suicide-Focused Research from a Community-Based Australian Sample. International Journal of Environmental Research and Public Health. 2021; 18(9):4705. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094705
Chicago/Turabian StyleRheinberger, Demee, Fiona Shand, Katherine Mok, Lauren McGillivray, Myfanwy Maple, Alexander Burnett, Lisa N. Sharwood, Nicola A. Chen, and Michelle Torok. 2021. "A Qualitative Analysis of Motivators to Participation in Suicide-Focused Research from a Community-Based Australian Sample" International Journal of Environmental Research and Public Health 18, no. 9: 4705. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094705