
A Telephone-Based Tobacco Cessation Program in the State of Qatar: Protocol of a Feasibility Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
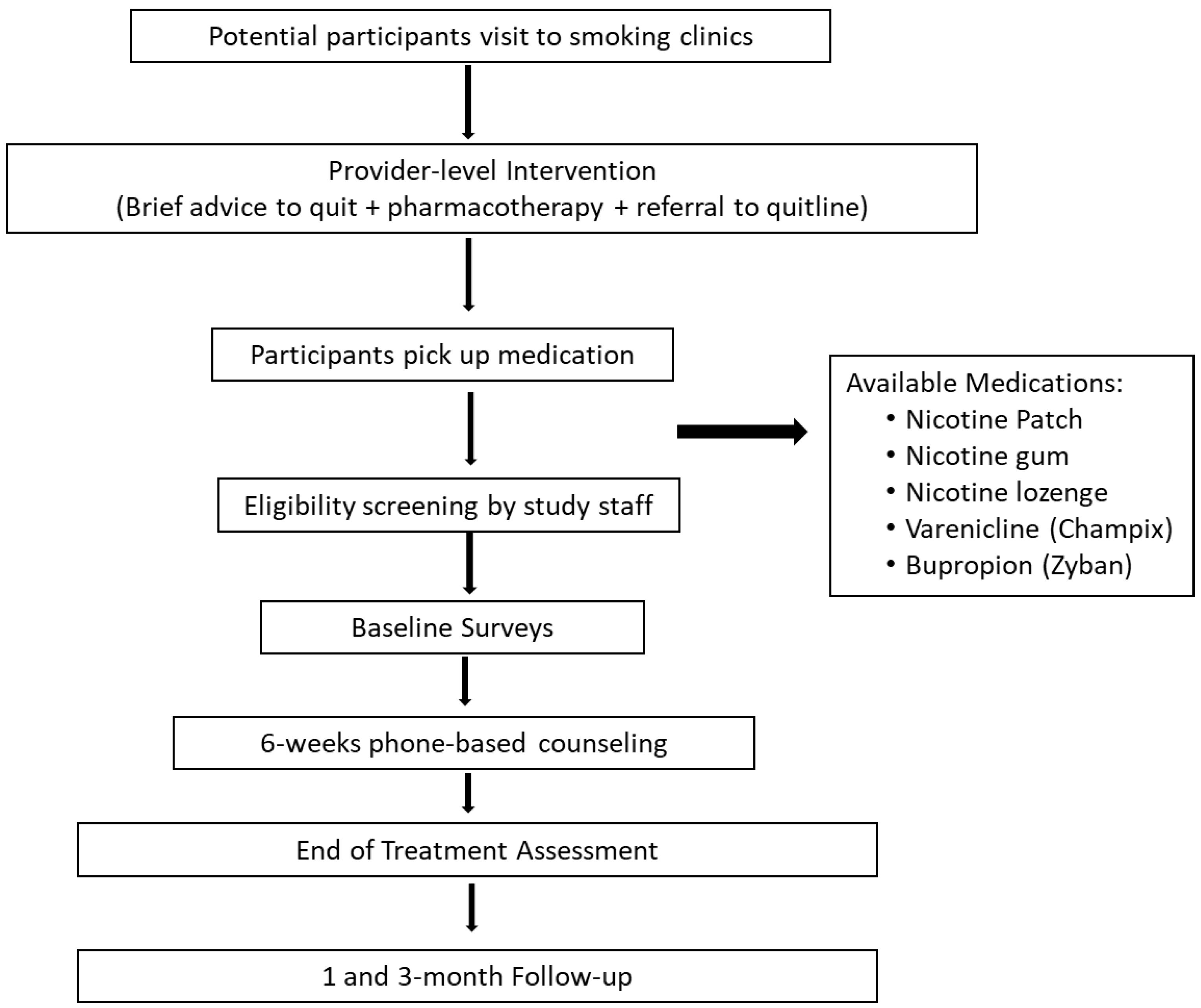
2.1. Study Design
2.2. Development of Healthcare System Referrals
2.3. Counseling Intervention
2.4. Counselor Training and Fidelity
2.5. Data Collection and Measures
2.6. Study Outcomes
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ENDS | Electronic nicotine delivery system |
| HIPAA | Health Insurance Portability and Accountability Act |
| IRB | Institutional Review Board |
| PHCC | Primary healthcare centers |
| US | United States |
| UK | United Kingdom |
References
- WHO Report on the Global Tobacco Epidemic, 2017: Monitoring Tobacco Use and Prevention Policies; World Health Organization: Geneva, Switzerland, 2017; ISBN 978-92-4-151282-4.
- WHO. Leading Cause of Death, Illness and Impoverishment. Available online: https://www.who.int/news-room/fact-sheets/detail/tobacco (accessed on 28 April 2021).
- WHO Global Report on Trends in Prevalence of Tobacco Use 2000–2025, 3rd ed. Available online: https://apps.who.int/iris/bitstream/handle/10665/330221/9789240000032-eng.pdf?ua=1 (accessed on 28 April 2021).
- Bener, A.; Zirie, M.A.; Kim, E.J.; Buz, R.; Zaza, M.; Al-Nufal, M.; Basha, B.; Riboli, E. Measuring burden of diseases in a rapidly developing economy: State of Qatar. Glob. J. Health Sci. 2013, 5, 134–144. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, W.H.; Rasul, K.I.; Khinji, A.; Ahmed, M.S.; Bener, A. Clinical and epidemiological characteristics of lung cancer cases in Qatar. East. Mediterr. Health J. 2010, 16, 166–170. [Google Scholar] [CrossRef]
- WHO Report on the Global Tobacco Epidemic 2019: Offer Help to Quit Tobacco Use; World Health Organization: Geneva, Switzerland, 2019.
- Anderson, C.M.; Zhu, S.H. Tobacco quitlines: Looking back and looking ahead. Tob. Control 2007, 6, i81–i86. [Google Scholar] [CrossRef] [Green Version]
- Abrams, D.B.; Graham, A.L.; Levy, D.T.; Mabry, P.L.; Orleans, C.T. Boosting population quits through evidence-based cessation treatment and policy. Am. J. Prev. Med. 2010, 38 (Suppl. 3), S351–S363. [Google Scholar] [CrossRef] [Green Version]
- McAfee, A.T. Quitlines a tool for research and dissemination of evidence-based cessation practices. Am. J. Prev. Med. 2007, 33 (Suppl. 6), S357–S367. [Google Scholar] [CrossRef]
- Lichtenstein, E.; Zhu, S.H.; Tedeschi, G.J. Smoking cessation quitlines: An underrecognized intervention success story. Am. Psychol. 2010, 65, 252–261. [Google Scholar] [CrossRef] [Green Version]
- Zhu, S.H.; Lee, M.; Zhuang, Y.L.; Gamst, A.; Wolfson, T. Interventions to increase smoking cessation at the population level: How much progress has been made in the last two decades? Tob. Control 2012, 21, 110–118. [Google Scholar] [CrossRef] [Green Version]
- North American Quitline Consortium 2018. Results from the 2018 NAQC Annual Survey of Quitlines. Available online: https://cdn.ymaws.com/www.naquitline.org/resource/resmgr/2018_survey/NAQC_FY2018_Annual_Survey_Da.pdf (accessed on 28 April 2021).
- Matkin, W.; Ordóñez-Mena, J.; Hartmann-Boyce, J. Telephone counselling for smoking cessation. Cochrane Dat. Syst. Rev. 2019, 5, CD002850. [Google Scholar] [CrossRef]
- Cummins, S.E.; Bailey, L.; Campbell, S.; Koon-Kirby, C.; Zhu, S.H. Tobacco cessation quitlines in North America: A descriptive study. Tob. Control 2007, 16 (Suppl. 1), 9–15. [Google Scholar] [CrossRef] [PubMed]
- Fiore, M.C.; Jaén, C.R.; Baker, T.B.; Bailey, W.C.; Bennett, G.; Benowitz, N.L.; Christiansen, B.A. A clinical practice guideline for treating tobacco use and dependence: 2008 update. A U.S. Public Health Service report. Am. J. Prev. Med. 2008, 35, 158–176. [Google Scholar]
- Hartmann-Boyce, J.; Chepkin, S.C.; Ye, W.; Bullen, C.; Lancaster, T. Nicotine replacement therapy versus control for smoking cessation. Cochrane Dat. Syst. Rev. 2018, 31, CD000146. [Google Scholar] [CrossRef] [PubMed]
- El Hajj, M.S.; Kheir, N.; Al Mulla, A.M.; Shami, R.; Fanous, N.; Mahfoud, Z.R. Effectiveness of a pharmacist-delivered smoking cessation program in the State of Qatar: A randomized controlled trial. BMC Public Health 2017, 17, 215. [Google Scholar] [CrossRef] [Green Version]
- Heckman, C.J.; Egleston, B.L. Efficacy of motivational interviewing for smoking cessation: A systematic review and meta-analysis. Tob. Control 2010, 19, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K.O. The Fagerstrom test for nicotine dependence: A revision of the Fagerstrom tolerance questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef]
- Pomerleau, C.S.; Carton, S.M.; Lutzke, M.L.; Flessland, K.A.; Pomerleau, O.F. Reliability of the Fagerstrom tolerance questionnaire and the Fagerstrom test for nicotine dependence. Addict. Behav. 1994, 19, 33–39. [Google Scholar] [CrossRef] [Green Version]
- Etter, J.F.; Bergman, M.M.; Humair, J.P.; Perneger, T.V. Development and validation of a scale measuring self-efficacy of current and former smokers. Addiction 2000, 95, 901–913. [Google Scholar] [CrossRef]
- O’Connell, K.A.; Gerkovich, M.M.; Cook, M.R.; Shiffman, S.; Hickcox, M.; Kakolewski, K.E. Coping in real time: Using Ecological Momentary Assessment techniques to assess coping with the urge to smoke. Res. Nurs. Health 1998, 21, 487–497. [Google Scholar] [CrossRef]
- Van Dam, N.T.; Earleywine, M. Validation of the Center for Epidemiologic Studies Depression Scale--Revised (CESD-R): Pragmatic depression assessment in the general population. Psychiatry Res. 2011, 186, 128–132. [Google Scholar] [CrossRef]
- Colina, S.; Marone, N.; Ingram, M.; Sanchez, D. Translation Quality Assessment in Health Research: A Functionalist Alternative to Back-Translation. Eval. Health Prof. 2017, 40, 267–293. [Google Scholar] [CrossRef] [PubMed]
- Borland, R.; Balmford, J.; Bishop, N.; Segan, C.; Piterman, L.; McKay-Brown, J.; Kirby, C. In-practice management versus quit-line referral for enhancing smoking cessation in general practice: A cluster randomized trial. Fam. Pract. 2008, 25, 382–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumenthal, D.S. Barriers to the provision of smoking cessation services reported by clinicians serving underserved communities. J. Am. Board Fam. Med. 2007, 20, 272–279. [Google Scholar] [CrossRef] [Green Version]
- Park, E.R.; Gareen, I.F.; Japuntich, S.; Lennes, I.; Hyland, K.; DeMello, S.; Sicks, J.D. Primary Care Provider-Delivered Smoking Cessation Interventions and Smoking Cessation among Participants in the National Lung Screening Trial. JAMA Intern. Med 2015, 175, 1509–1516. [Google Scholar] [CrossRef] [Green Version]
- Ferketich, A.K.; Khan, Y.; Wewers, M.E. Are physicians asking about tobacco use and assisting with cessation? Results from the 2001–2004 National Ambulatory Medical Care Survey (NAMCS). Prev. Med. 2006, 43, 472–476. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sessions | Topics Covered |
|---|---|
| Session 1 |
|
| Session 2 |
|
| Session 3 (Quit Day) |
|
| Session 4 |
|
| Session 5 |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Thani, M.; Leventakou, V.; Sofroniou, A.; Eltayeb, S.M.; Sadoun, E.; Hakim, I.A.; Thomson, C.; Nair, U. A Telephone-Based Tobacco Cessation Program in the State of Qatar: Protocol of a Feasibility Study. Int. J. Environ. Res. Public Health 2021, 18, 4750. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094750
Al Thani M, Leventakou V, Sofroniou A, Eltayeb SM, Sadoun E, Hakim IA, Thomson C, Nair U. A Telephone-Based Tobacco Cessation Program in the State of Qatar: Protocol of a Feasibility Study. International Journal of Environmental Research and Public Health. 2021; 18(9):4750. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094750
Chicago/Turabian StyleAl Thani, Mohammed, Vasiliki Leventakou, Angeliki Sofroniou, Safa M. Eltayeb, Eman Sadoun, Iman A. Hakim, Cynthia Thomson, and Uma Nair. 2021. "A Telephone-Based Tobacco Cessation Program in the State of Qatar: Protocol of a Feasibility Study" International Journal of Environmental Research and Public Health 18, no. 9: 4750. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094750