
A Decision-Tree Approach to Assist in Forecasting the Outcomes of the Neonatal Brain Injury

 , ,
, ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Methods
2.2. Data Analysis
2.2.1. Statistical Analysis
2.2.2. Machine Learning Approach
3. Results
3.1. Etiology
3.2. Demographics
3.2.1. Gestational Age and Birthweight
3.2.2. Apgar Scores, Reanimation and Ultrasound Imaging
3.2.3. Seizure Events
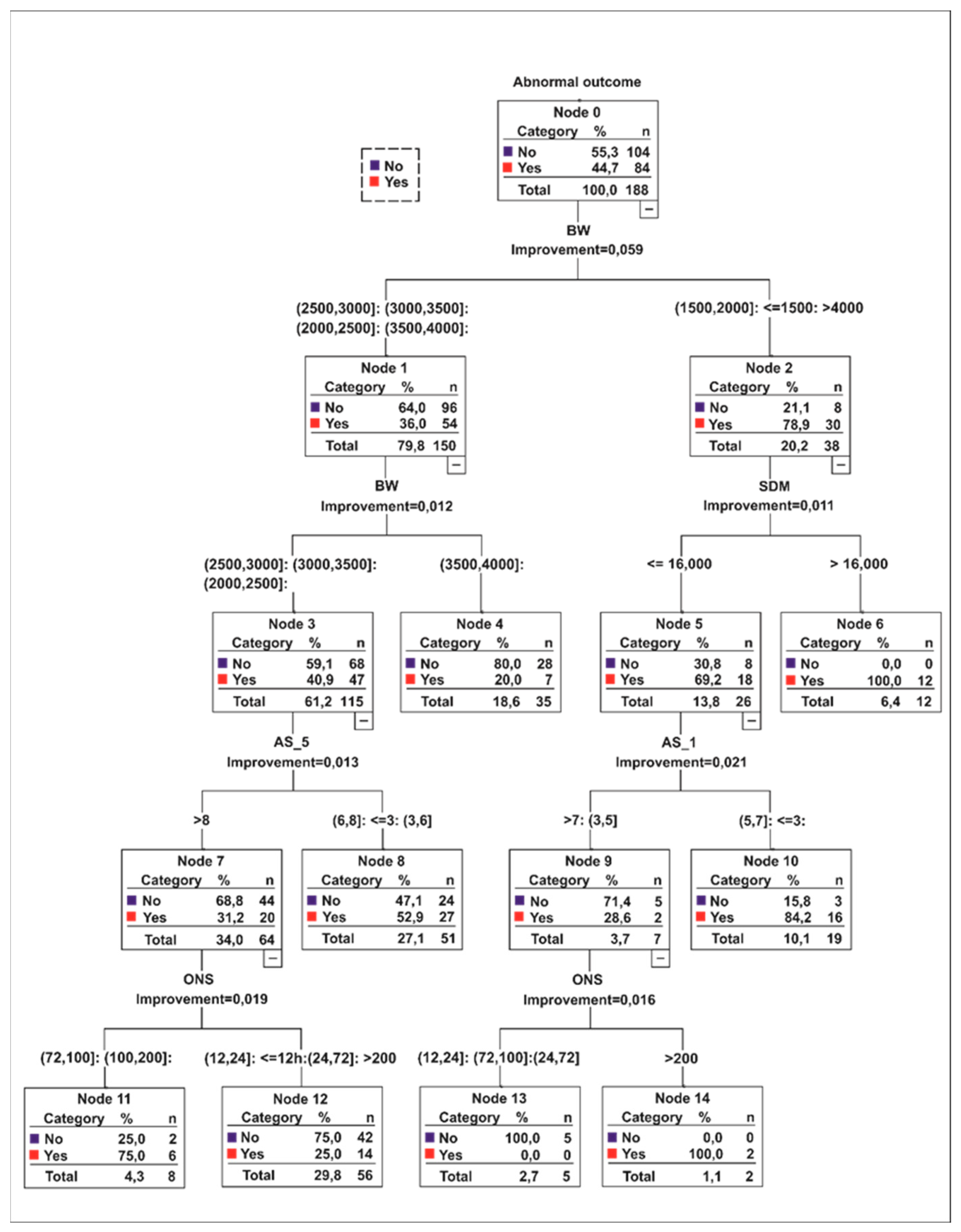
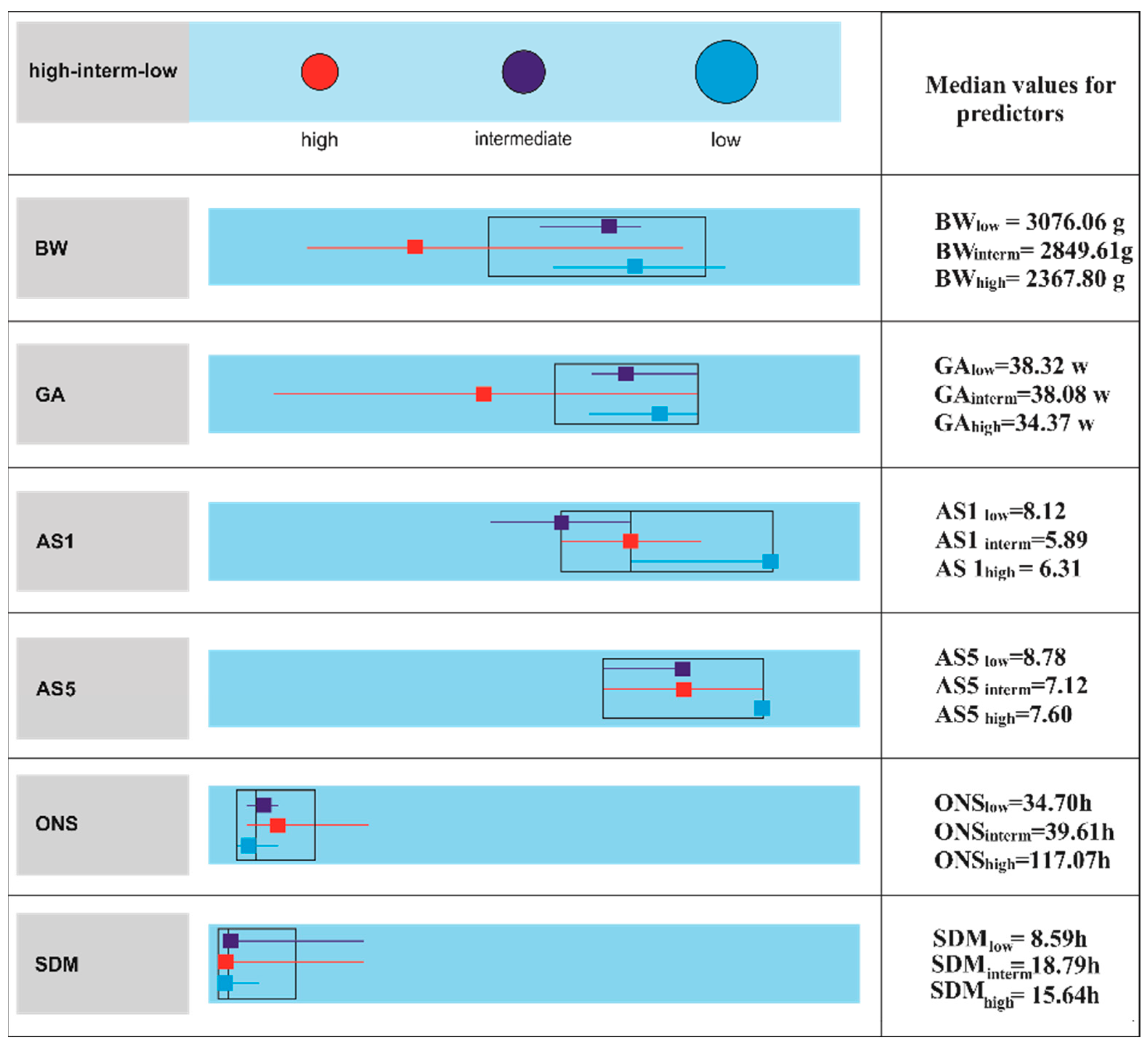
3.3. CART and CLUSTER Analysis
4. Discussion
4.1. Preterms
4.2. Full-Terms
4.3. Decision-Tree Approach
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. In Depth Analysis of the Subjects’ Records
- (1)
- Epilepsy was categorized accordingly, based on the proposed guidelines of International League Against Epilepsy (ILAE). The infants presenting recurrent unprovoked seizures events were classified as epileptic.
- (2)
- Cerebral palsy was clinically formulated as an early non-progressive motor deficit with objective changes in motor movements and posture on medical examination according to the guidelines provided by the Executive Committee for the Definition of Cerebral Palsy in 2005 [17].
- (3)
- Hydrocephaly was defined based on working definition proposed by International Society for Hydrocephalus and Cerebrospinal Fluid Disorders and as an active distension of the ventricular system of the brain resulting from the inadequate passage of CSF from its point of production within the ventricles to its point of resorption into the systemic circulation [18,19].
- (4)
- The developmental delay was defined based on the Practice Guidelines proposed by the American Academy of Neurology-Child Neurology Society Practice Guidelines. We looked for a significant delay, at least two standard deviations below the mean with standardized tests, affecting one or more developmental domains (global delay): Gross or fine motor, Speech/language, Cognition, Social/personal, Activities of daily living. We collected thru standardized questionnaires completed by the pediatric neurologist for each patient for the evaluations at 1 month, 6 months, first year and second year of life, based on Munich Functional Development Diagnostics standardized tests.
Appendix A.2. Pregnancy Pathologies and Seizures’ Management
Appendix A.3. Mathematical Models for CART and CLUSTER Algorithms
Appendix A.3.1. CART Algorithm
Appendix A.3.2. CLUSTER Algorithm
References
- Kurinczuk, J.J.; White-Koning, M.; Badawi, N. Epidemiology of neonatal encephalopathy and hypoxic-ischaemic encephalopathy. Early Hum. Dev. 2010, 86, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Iliodromiti, Z.; Zygouris, D.; Karagianni, P.; Belitsos, P.; Daniilidis, A.; Vrachnis, N. Chapter4-brain injury in preterm infants. In Neonatal Care, Deborah Raines and Zoe Iliodromiti; IntechOpen: London, England, 2012; pp. 73–86. [Google Scholar] [CrossRef] [Green Version]
- Wyatt, J.S. Mechanisms of brain injury in the Newborn. Eye 2007, 21, 1261–1263. [Google Scholar] [CrossRef] [Green Version]
- Volpe, J.J. Brain injury in premature infants: A complex amalgam of destructive and developmental disturbances. Lancet Neurol. 2009, 8, 110–124. [Google Scholar] [CrossRef] [Green Version]
- Ambalavanan, N.; Carlo, W.A.; Shankaran, S.; Bann, C.M.; Emrich, S.L.; Higgins, R.D.; Tyson, J.E.; O’Shea, T.M.; Laptook, A.R.; Ehrenkranz, R.A.; et al. Predicting outcome of neonates diagnosed with hypoxemicischemic encephalopathy. Pediatrics 2006, 118, 2084–2093. [Google Scholar] [CrossRef] [PubMed]
- Garfinkle, J.; Shevell, M.I. Prognostic factors and development of a scoring system for outcome of neonatal seizures in term infants. Eur. J. Paediatr. Neurol. 2011, 15, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Soltirovska-Salamon, A.; Neubauer, D.; Petrovcic, A.; Paro-Panjan, D. Risk factors and scoring system as a prognostic tool for epilepsy after neonatal seizures. Pediatr. Neurol. 2014, 50, 77–84. [Google Scholar] [CrossRef]
- Lai, Y.H.; Ho, C.S.; Chiu, N.C.; Tseng, C.F.; Huang, Y.L. Prognostic factors of developmental outcome in neonatal seizures in term infants. Pediatr. Neonatol. 2013, 54, 166–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, S.P.; Ramaswamy, V.; Michelson, D.; Barkovich, A.J.; Holshouser, B.; Wycliffe, N.; Glidden, D.V.; Deming, D.; Partridge, J.C.; Wu, Y.W.; et al. Patterns of brain injury in term neonatal encephalopathy. J. Pediatr. 2005, 146, 453–460. [Google Scholar] [CrossRef]
- Glass, H.C.; Grinspan, Z.M.; Shellhaas, R.A. Outcomes after acute symptomatic seizures in neonates. Semin. Fetal Neonatal Med. 2018, 23, 218–222. [Google Scholar] [CrossRef]
- Stafstrom, C.E.; Jantzie, L.L. COVID-19: Neurological considerations in neonates and children. Children (Basel) 2020, 7, 133. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, P.; Curtis, N. COVID-19 in children, pregnancy and neonates: A review of epidemiologic and clinical features. Pediatr. Infect. Dis. J. 2020, 39, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Sarnat, H.B.; Sarnat, M.S. Neonatal encephalopathy following fetal distress. A clinical and electroencephalographic study. Arch. Neurol. 1976, 33, 696–705. [Google Scholar] [CrossRef]
- Nunes, M.L.; Martins, M.P.; Barea, B.M.; Wainberg, R.C.; Da Costa, J.C. Neurological outcome of newborns with neonatal seizures: A cohort study in a tertiary university hospital. Arq. Neuro Psiquiatr. 2008, 66, 168–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volpe, J.J. Chapter 5-neonatal seizures. In Neurology of the Newborn, 5th ed.; Saunders Elsevier: Philadelphia, PA, USA, 2008; pp. 203–245. ISBN 9781416039952. [Google Scholar]
- Pisani, F.; Sisti, L.; Seri, S. A scoring system for early prognostic assessment after neonatal seizures. Pediatrics 2009, 124, e580–e587. [Google Scholar] [CrossRef] [PubMed]
- Bax, M.; Goldstein, M.; Rosenbaum, P.; Leviton, A.; Paneth, N.; Bernard, D.; Jacobsson, B.; Damiano, D. Proposed definition and classification of cerebral palsy, April 2005-Introduction. Dev. Med. Child Neurol. 2015, 47, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Rekate, H.L. A consensus on the classification of hydrocephalus: Its utility in the assessment of abnormalities of cerebrospinal fluid dynamics. Childs Nerv. Syst. 2011, 27, 1535–1541. [Google Scholar] [CrossRef] [Green Version]
- Wright, Z.; Larrew, T.W.; Eskandari, R. Pediatric hydrocephalus: Current state of diagnosis and treatment. Pediatr. Rev. 2016, 37, 478–490. [Google Scholar] [CrossRef] [PubMed]
- Breiman, L.; Friedman, J.; Olshen, R.; Stone, C. Classification and Regression Trees; Chapman & Hall/CRC Press: Boca Raton, FL, USA, 1984. [Google Scholar]
- Hastie, T.J.; Tibshirani, R.J.; Friedman, J.H. The Elements of Statistical Learning: Data Mining, Inference and Prediction, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2009; ISBN 978-0-387-84857-0. [Google Scholar]
- Hapfelmeier, A.; Hothorn, T.; Ulm, K. Recursive partitioning on incomplete data using surrogate decisions and multiple imputation. Comput. Stat. Data Anal. 2012, 56, 1552–1565. [Google Scholar] [CrossRef]
- Valencia-Zapata, G.A.; Salazar-Uribe, J.C. Classification and regression trees for handling missing values in a CMBD to reduce malware in an information system. In Proceedings of the International Conference on Data Science (ICDATA); The Steering Committee of The World Congress in Computer Science, Computer Engineering and Applied Computing (WorldComp), Las Vegas, NV, USA, 16–19 July 2012. [Google Scholar] [CrossRef]
- Quinlan, R. Unknown attribute values in induction. In Proceedings of the Sixth International Workshop on Machine Learning; Elsevier Inc.: Amsterdam, The Netherlands, 1989; pp. 164–168. [Google Scholar]
- Tierney, N.J.; Harden, F.A.; Harden, M.J.; Mengersen, K.L. Using decision trees to understand structure in missing data. BMJ Open 2015, 5, e007450. [Google Scholar] [CrossRef] [Green Version]
- McDonough, T.; Paolicchi, J.; Heier, L.; Das, N.; Engel, M.; Perlman, J.; Grinspan, Z. Prediction of future epilepsy in neonates with HIE who received selective head cooling. J. Child Neurol. 2017, 32, 630–637. [Google Scholar] [CrossRef]
- Patel, N.; Upadhyay, S. Study of various decision tree pruning methods with their empirical comparison in WEKA. Int. J. Comp. Appl. 2012, 60, 20–25. [Google Scholar] [CrossRef]
- Hayes, T.; Usami, S.; Jacobucci, R.; McArdle, J. Using Classification and Regression Trees (CART) and Random Forests to Analyze Attrition: Results from two simulations. Psychol. Aging 2015, 30, 911–929. [Google Scholar] [CrossRef] [Green Version]
- Pressler, R.M. Neonatal Seizures, The National Society for Epilepsy; Library of Articles: Chalfont St Peter, Buckinghamshire, UK, 2015; Chapter 6. [Google Scholar]
- Brunquell, P.J.; Glennon, C.M.; DiMario, F.J.; Lerer, T.; Eisenfeld, L. Prediction of outcome based on clinical seizure type in newborn infants. J. Pediatr. 2002, 140, 707–712. [Google Scholar] [CrossRef]
- Glass, H.C. Neonatal seizures. Curr. Treat. Options Neurol. 2009, 11, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Sabzehei, M.K.; Behnaz, B.; Hassan, B. The etiology, clinical type, and short outcome of seizures in newborns hospitalized in Besat Hospital/Hamadan/Iran. Iran. J. Child Neurol. 2014, 8, 24–28. [Google Scholar]
- Weeke, L.C.; Groenendaal, F.; Toet, M.C.; Groenendaal, F.; Toet, M.C.; Benders, M.J.N.L.; Nievelstein, R.A.J.; Van Rooij, L.G.M.; De Vries, L.S. The aetiology of neonatal seizures and the diagnostic contribution of neonatal cerebral magnetic resonance imaging. Dev. Med. Child. Neurol. 2015, 57, 248–256. [Google Scholar] [CrossRef]
- Heljic, S.; Uzicanin, S.; Catibusic, F.; Zubcevic, S. Predictors of mortality in neonates with seizures: A prospective cohort study. Med. Arch. 2016, 70, 182–185. [Google Scholar] [CrossRef] [Green Version]
- Yi, B.; Wu, L.; Liu, H.; Fang, W.; Hu, Y.; Wang, Y. Rural-urban differences of neonatal mortality in a poorly developed province of China. BMC Public Health 2011, 11, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kayode, G.A.; Ansah, E.; Agyepong, I.A.; Amoakoh-Coleman, M.; Grobbee, D.E.; Klipstein-Grobusch, K. Individual and community determinants of neonatal mortality in Ghana: A multilevel analysis. BMC Pregnancy Childbirth 2014, 14, 165. [Google Scholar] [CrossRef] [Green Version]
- Adewuyi, E.O.; Zhao, Y. Determinants of neonatal mortality in rural and urban Nigeria: Evidence from a population-based national survey. Pediatrics Int. 2017, 59, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Ronen, G.M.; Buckley, D.; Penney, S.; Streiner, D.L. Long-term prognosis in children with neonatal seizures: A population-based study. Neurology 2007, 69, 1816–1822. [Google Scholar] [CrossRef]
- Vasudevan, C.; Levene, M. Epidemiology and aetiology of neonatal seizures. Semin. Fetal Neonatal. Med. 2013, 18, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Al Yazidi, G.; Srour, M.; Wintermark, P. Risk factors for intraventricular haemorrhage in term asphyxiated newborns treated with hypothermia. Pediatr. Neurol. 2014, 50, 630–635. [Google Scholar] [CrossRef]
- Saliba, E.; Debillon, T.; Auvin, S.; Baud, O.; Biran, V.; Chabernaud, J.; Chabrier, S.; Cneude, F.; Cordier, A.; Darmency-Stamboul, V.; et al. Neonatal arterial ischemic stroke: Review of the current guidelines. Arch. Pédiatrie 2017, 24, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Ramaswamy, V.; Miller, S.P.; Barkovich, A.J.; Partridge, J.C.; Ferriero, D.M. Perinatal stroke in term infants with neonatal encephalopathy. Neurology 2004, 62, 2088–2091. [Google Scholar] [CrossRef]
- Jensen, F.E. Neonatal seizures: An update on mechanisms and management. Clin. Perinatol. 2009, 36, 881–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisani, F.; Copioli, C.; Turco, E.C.; Sisti, L.; Cossu, G.; Seri, S. Mortality risk after neonatal seizures in very preterm newborns. J. Child. Neurol. 2012, 27, 1264–1269. [Google Scholar] [CrossRef]
- Eun, S.; Lee, J.M.; Yi, D.Y.; Lee, N.M.; Kim, H.; Yun, S.W.; Lim, I.; Choi, E.S.; Chae, S.A. Assessment of the association between Apgar scores and seizures in infants less than 1 year old. Seizure 2016, 37, 48–54. [Google Scholar] [CrossRef] [Green Version]
- Rennie, J.M.; Boylan, G.B. Seizure disorders of the neonate. In Fetal and Neonatal Neurology and Neurosurgery, 4th ed.; Levene, M.I., Chervenak, F.A., Eds.; Elsevier: Philadelphia, PA, USA, 2009; pp. 698–710. [Google Scholar]
- Buraniqi, E.; Sansevere, A.J.; Kapur, K.; Bergin, A.M.; Pearl, P.L.; Loddenkemper, T. Electrographic seizures in preterm neonates in the neonatal intensive care unit. J Child Neurol. 2017, 32, 880–885. [Google Scholar] [CrossRef]
- Pisani, F.; Barilli, A.L.; Sisti, L.; Bevilacqua, G.; Seri, S. Preterm infants with video-EEG confirmed seizures: Outcome at 30 months of age. Brain Dev. 2008, 30, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.M.; Guillet, R.; Shankaran, S.; Laptook, A.R.; McDonald, S.A.; Ehrenkranz, R.A. Clinical seizures in neonatal hypoxiceischemic encephalopathy have no independent impact on neurodevelopmental outcome: Secondary analyses of date from the neonatal research network hypothermia trial. J. Child Neurol. 2011, 26, 322. [Google Scholar] [CrossRef] [PubMed]
- Bergman, I.; Painter, M.J.; Hirsch, R.P.; Crumin, P.K.; David, R. Outcome in neonates with convulsions treated in ICU. Ann. Neurol. 1983, 14, 642–647. [Google Scholar] [CrossRef]
- Thoker, A.H.; Sheikh, M.; Thoker, P.A.; Thoker, M. Neurodevelopmental outcome in perinatal asyphxia. Am. J. Exp. Clin. Res. 2017, 4, 206–209. [Google Scholar]
- Li, A.M.; Chau, V.; Poskitt, K.J.; Sargent, M.A.; A Lupton, B.; Hill, A.; Roland, E.; Miller, S.P. White matter injury in term newborns with neonatal encephalopathy. Pediatr. Res. 2009, 65, 85–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harteman, J.C.; Groenendaal, F.; Toet, M.C.; Benders, M.J.; Van Haastert, I.C.; Nievelstein, R.A.; Koopman-Esseboom, C.; De Vries, L.S. Diffusion-weighted imaging changes in cerebral watershed distribution following neonatal encephalopathy are not invariably associated with an adverse outcome. Dev. Med. Child Neurol. 2013, 55, 642–653. [Google Scholar] [CrossRef] [Green Version]
- Jeganathan, R.; Karalasingam, S.D.; Hussein, J.; Allotey, P.; Reidpath, D.D. Factors associated with recovery from 1 minute Apgar score < 4 in live, singleton, term births: An analysis of Malaysian National Obstetrics Registry data 2010–2012. BMC Pregnancy Childbirth 2017, 17, 110. [Google Scholar]
- Glass, H.C.; Shellhaas, R.A.; Tsuchida, T.N.; Chang, T.; Wusthoff, C.J.; Chu, C.J.; Cilio, M.R.; Bonifacio, S.L.; Massey, S.L.; Abend, N.S.; et al. Seizures in preterm neonates: A multicenter observational cohort study. Pediatric Neurol. 2017, 72, 19–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Alton, M.E.; Hankins, G.D.V.; Berkowitz, R.L.; Bienstock, J.; Ghidini, A.; Goldsmith, J.; Higgins, R.; Moore, T.R.; Natale, R.; Nelson, K.B.; et al. Neonatal Encephalopathy and Neurologic Outcome, 2nd ed.; Report of the American College of Obstetricians and Gynecologists’ Task Force on Neonatal Encephalopathy, Pediatrics; American Academy of Pediatrics: Itasca, IL, USA, 2014; Volume 133, pp. e1482–e1488. [Google Scholar]
- Martinello, K.; Hart, A.R.; Yap, S.; Mitra, S.; Robertson, N.J. Management and investigation of neonatal encephalopathy: 2017 update. Arch. Dis. Child. Fetal Neonatal. Ed. 2017, 102, F346. [Google Scholar] [CrossRef]
- Costea, R.; Neamtu, M.; Neamtu, B. Febrile seizures–EEG study and risks factors for recurrence and for epilepsy. Eur. J. Pediatr. 2016, 175, 1393. [Google Scholar] [CrossRef] [Green Version]
- Maniu, I.; Maniu, G.; Dospinescu, C.; Visa, G. A Factor Analysis Model for Dimension Reduction of Outcome Factors in Neonatal Seizure Context; BRAIN Broad Res. Artif. Intell. Neurosci. 2018, 9, 95–103. [Google Scholar]
- Maniu, I.; Maniu, G.; Visa, G.; Costea, R.; Neamtu, B. Frequent pattern mining of risk factors predicting neonatal seizures outcomes. BRAIN Broad Res. Artif. Intell. Neurosci. 2018, 9, 161–170. [Google Scholar]
- Maniu, I.; Maniu, G.; Balan, C.; Neamtu, B. Scoring systems for predicting outcomes of neonatal seizure. Acta Med. Transilv. 2017, 22, 48–50. [Google Scholar]
- Zhang, C.; Garrard, L.; Keighley, J.; Carlson, S.; Gajewski, B.J. Subgroup identification of early preterm birth (ePTB): Informing a future prospective enrichment clinical trial design. BMC Pregnancy Childbirth 2017, 17, 18. [Google Scholar] [CrossRef] [Green Version]
- Mehta, R.; Bahatt, N.; Ganatra, A. A survey on data mining technologies for decision support system of maternal care domain. Int. J. Comput. Appl. 2016, 138, 975–8887. [Google Scholar] [CrossRef]
- Vovsha, I.; Rajan, A.; Salleb-Aouissi, A.; Raja, A.; Radeva, A.; Diab, H.; Tomar, A.; Wapner, R. Predicting preterm birth is not elusive: Machine learning paves the way to individual wellness. AAAI Spring Symp. Tech. Rep. SS 2014, 14, 82–89. [Google Scholar]
- Ferreira, D.; Oliveira, A.; Freitas, A. Applying data mining techniques to improve diagnosis in neonatal jaundice. BMC Med. Inform. Decis. Mak. 2012, 12, 143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mardikyan, S.; Aksoy, I.; Badur, B. Finding hidden patterns of hospital infections on newborn: A data mining approach. Istanb. Univ. J. School Bus. Adm. 2010, 39, 210–226. [Google Scholar]
- Costea, R.M.; Maniu, I.; Dobrota, L.; Neamtu, B. Stress hyperglycemia as predictive factor of recurrence in children with febrile seizures. Brain Sci. 2020, 10, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sokhadze, E.; Sears, L.; El-Baz, A.; Tasman, A.; Casanova, M. Clinical Applications of Electrophysiological Approaches Based on Cortical Modularity. In Recent Advances on the Modular Organization of the Cortex; Casanova, M.F., Opris, I., Eds.; Springer: New York, NY, USA, 2015; Chapter 14; pp. 239–270. [Google Scholar]
- IBM SPSS Decision Trees 22. Available online: http://www.sussex.ac.uk/its/pdfs/SPSS_Decision_Trees_22.pdf (accessed on 10 January 2021).
- Maresova, P.; Hruska, J.; Klimova, B.; Barakovic, S.; Krejcar, O. Activities of daily living and associated costs in the most widespread neurodegenerative diseases: A systematic review. Clin. Interv. Aging. 2020, 15, 1841–1862. [Google Scholar] [CrossRef]
- Sarstedt, M.; Mooi, E. Introduction to Market Research. In A Concise Guide to Market Research.Springer Texts in Business and Economics; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar] [CrossRef]
- Cheng, L.K.; Selamat, A.; Zabil, M.H.M.; Selamat, H.; Alias, R.A.; Puteh, F.; Mohamed, F.; Krejcar, O. Comparing the Accuracy of Hierarchical Agglomerative and K-Means Clustering on Mobile Augmented Reality Usability Metrics. In Proceedings of the 2019 IEEE Conference on Big Data and Analytics (ICBDA), Pulau Pinang, Malaysia, 19–21 November 2019; pp. 34–40. [Google Scholar] [CrossRef]
- Wilks, D.S. Chapter 15-cluster analysis. In Statistical Methods in the Atmospheric Sciences, 3rd ed.; International Geophysics, Academic Press: Cambridge, MA, USA, 2011; Volume 100, pp. 603–616. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Categories | Total (N/P) b | Outcome (N/P) | Abnormal Outcome Types a (N/P) | ||||
|---|---|---|---|---|---|---|---|
| Normal | Abnormal | Epilepsy | Cognitive Delays | Motor Delays | HCEP | ||
| Patients | 188 | 104 (55.3) | 84 (44.7) | 30 (16) | 51 (27.1) | 71 (37.8) | 24 (12.8) |
| Etiology | |||||||
| HIE | 133 (70.74) | 76 (57.14) | 57 (42.86) | 20 (15.04) | 34 (25.56) | 45 (33.83) | 16 (12.03) |
| HC | 11 (5.85) | 4 (36.36) | 7 (63.64) | 3 (27.27) | 7 (63.64) | 7 (63.64) | 1 (9.09) |
| INF | 13 (6.91) | 3 (23.08) | 10 (76.92) | 3 (23.08) | 4 (30.77) | 9 (69.23) | 5 (38.46) |
| MALF | 5 (2.66) | 0 (0.00) | 5 (100.00) | 2 (40) | 3 (60.00) | 5 (100) | 2 (40) |
| AVC c | 2 (1.06) | 0 (0.00) | 2 (100.00) | 2 (100) | 2 (100) | 2 (100) | 0 (0) |
| METAB | 22 (11.70) | 19 (86.36) | 3 (13.64) | 0 (0) | 1 (4.55) | 3 (13.64) | 0 (0) |
| DRUG | 2 (1.06) | 2 (100.00) | 0 (0.00) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Variables (Number of Cases) | Total | Outcome | p-Value a | |
|---|---|---|---|---|
| Normal | Abnormal | |||
| M ± SD (95%CI); MIN, MAX, IQR (MEDIAN) | ||||
| GA in weeks | 37.39 ± 4.16 (36.79–37.99) 26–44 36–40 (38) | 38.29 ± 2.97 (37.71–38.87) 27–44 37–40 (39) | 36.27 ± 5.05 (35.17–37.37) 26–43 33–40 (38) | p = 0.005 b |
| BW in grams | 2860.17 ± 772.94 (2748.96–2971.37) 900–4450 2.350–3.490 (2997.5) | 3014.88 ± 636.92 (2891.00–3138.74) 900–4225 2.615–3.530 (3085) | 2668.63 ± 880.62 (2477.52–2859.73) 900–4450 1992–3260 (2810) | p = 0.003 |
| AS1 | 7.16 ± 2.31 | 7.55 ± 2.18 | 6.66 ± 2.37 | p = 0.005 |
| (6.81–7.51) | (7.11–7.99) | (6.11–7.21) | ||
| 1–10 | 1–10 | 1–10 | ||
| 6–9 (7) | 7–9 (8) | 6–9 (7) | ||
| AS5 | 7.99 ± 1.64 | 8.25 ± 1.40 | 7.68 ± 1.84 | p = 0.082 |
| (7.67–8.30) | (7.88–8.62) | (7.15–8.20) | ||
| 2–10 | 3–10 | 2–10 | ||
| 7–9 (8) | 8–9 (9) | 7–9 (8) | ||
| Categories | Total (N/P) a | Outcome (N/P) | Abnormal Outcome Types (N/P) | ||||
|---|---|---|---|---|---|---|---|
| Normal | Abnormal | Epilepsy | Cognitive Delays | Motor Delays | HCEP | ||
| Seizures types | |||||||
| Subtle | 142 (75.53) | 85 (59.86) | 57 (40.14) | 17 (11.97) | 37 (26.06) | 50 (35.21) | 17 (11.97) |
| Clonic | 87 (46.28) | 42 (48.28) | 45 (51.72) | 19 (21.84) | 30 (34.48) | 35 (40.23) | 12 (13.79) |
| Tonic | 57 (30.32) | 28 (49.12) | 29 (50.88) | 13 (22.81) | 21 (36.84) | 24 (42.11) | 10 (17.54) |
| Myoclonic | 41 (21.81) | 21 (51.22) | 20 (48.78) | 11 (26.83) | 13 (31.71) | 18 (43.90) | 10 (24.39) |
| Generalized | 26 (13.83) | 12 (46.15) | 14 (53.85) | 9 (34.62) | 10 (38.46) | 10 (38.49) | 6 (23.08) |
| Variables (Number of Cases) | Total | Outcome | p-Value a | |
|---|---|---|---|---|
| Normal | Abnormal | |||
| M ± SD (95%CI); MIN, MAX, IQR (MEDIAN) | ||||
| ONS in hours | 55.95 ± 81.06 | 53.65 ± 83.01 | 58.84 ± 78.98 | p = 0.467 |
| (43.95–67.94) | (37.08–70.20) | (41.14–76.52) | ||
| 1–500 | 1–500 | 1–400 | ||
| 23–72 (29) | 23–48 (28) | 21–72 (32) | ||
| SDM in hours | 12.90 ± 19.98 | 11.38 ± 19.76 | 15.2 ± 20.28 | p = 0.102 |
| (9.37–16.42) | (6.86–15.89) | (9.43–20.96) | ||
| 1–96 | 1–96 | 1–82 | ||
| 2–12 (3) | 2–10 (3) | 2–24 (4) | ||
| High | Intermediate | Low | ||||
|---|---|---|---|---|---|---|
| N (PT/FT) | N (PT/FT) | N (PT/FT) | ||||
| Etiology | ||||||
| HIE | 29 (13/16) | 70.73% | 35 (9/26) | 68.63% | 69 (18/51) | 71.88% |
| HC | 2 (2/0) | 4.88% | 5 (0/5) | 9.80% | 4 (0/4) | 4.17% |
| INF | 7 (7/0) | 17.07% | 2 (1/1) | 3.92% | 4 (1/3) | 4.17% |
| MALF | 0 (0/0) | 0.00% | 4 (0/4) | 7.84% | 1 (0/1) | 1.04% |
| AVC | 2 (0/2) | 4.88% | 0 (0/0) | 0.00% | 0 (0/0) | 0.00% |
| METAB | 1 (0/1) | 2.44% | 3 (0/3) | 5.88% | 18 (2/16) | 18.75% |
| DRUGS | 0 (0/0) | 0.00% | 2 (0/2) | 3.92% | 0 (0/0) | 0.00% |
| Outcome a | ||||||
| Epilepsy | 14 (5/9) | 34.15% | 11 (2/9) | 21.57% | 5 (1/4) | 5.21% |
| Cognitive delays | 23 (11/12) | 56.10% | 14 (2/12) | 27.45% | 14 (3/11) | 14.58% |
| Motor delays | 32 (19/13) | 78.05% | 23 (5/18) | 45.10% | 16 (4/12) | 16.67% |
| HCEP | 12 (8/4) | 29.27% | 9 (2/7) | 17.65% | 3 (1/2) | 3.12% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neamțu, B.M.; Visa, G.; Maniu, I.; Ognean, M.L.; Pérez-Elvira, R.; Dragomir, A.; Agudo, M.; Șofariu, C.R.; Gheonea, M.; Pitic, A.; et al. A Decision-Tree Approach to Assist in Forecasting the Outcomes of the Neonatal Brain Injury. Int. J. Environ. Res. Public Health 2021, 18, 4807. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094807
Neamțu BM, Visa G, Maniu I, Ognean ML, Pérez-Elvira R, Dragomir A, Agudo M, Șofariu CR, Gheonea M, Pitic A, et al. A Decision-Tree Approach to Assist in Forecasting the Outcomes of the Neonatal Brain Injury. International Journal of Environmental Research and Public Health. 2021; 18(9):4807. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094807
Chicago/Turabian StyleNeamțu, Bogdan Mihai, Gabriela Visa, Ionela Maniu, Maria Livia Ognean, Rubén Pérez-Elvira, Andrei Dragomir, Maria Agudo, Ciprian Radu Șofariu, Mihaela Gheonea, Antoniu Pitic, and et al. 2021. "A Decision-Tree Approach to Assist in Forecasting the Outcomes of the Neonatal Brain Injury" International Journal of Environmental Research and Public Health 18, no. 9: 4807. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094807