1. Introduction
Since its first identification as a cluster of atypical pneumonias in Wuhan, China in December 2019 [
1], the COVID-19 virus has spread to 224 countries around the globe [
2]. Nearly a year after the classification of the outbreak as a global pandemic by the World Health Organization on 11th March 2020 [
1], the disease counts more than 119 million reported cases and over 2 million deaths globally (14 March 2021) [
2]. Protecting people from infection, imposition of public health measures that infringe on personal and collective freedoms, growing financial losses, and conflicting messages from authorities are among the major stressors having contributed to the widespread emotional distress and increased risk of psychological disorders associated with COVID-19. With growing knowledge of the initial impacts of the pandemic on psychological health and well-being and the increasing importance of the infodemic, an information overload observed during large-scale epidemics [
3], research now shifts towards the longitudinal surveillance of these adverse effects and investigating mitigation strategies [
4].
Although signs of hope are appearing among the population, due to rapid advancements in the development, production and distribution of the COVID-19 vaccine, the psychological repercussions of COVID-19 continue to deepen as many countries face the second wave, and even a third one in some cases, of the pandemic. Extensive research on disaster mental health has established that emotional distress is ubiquitous in affected local communities; a finding certain to be echoed during the pandemic, but this time among virtually the entire world population, as no one is immune to its collateral damages [
5,
6]. Throughout the world researchers have found consistent evidence that the pandemic has triggered a surge in psychopathological disorders and symptoms. In Canada, a study exploring the changes in self-reported mental health noted a deterioration in mental health in 38.2% of respondents during the first wave of the pandemic. Individuals with pre-existing mental health conditions, with disabilities and with annual household incomes <25,000
$ CAD were more likely to be affected [
7]. In the United States, about 29% of the adult population reported some depression/anxiety symptoms, with symptoms deteriorating over the month of March [
8]. The key driving forces of this psychological crisis have been economic concerns, health implications and social distancing measures [
8]. Researchers in Italy and Belgium found that lockdown delayed sleep timing, increased time spent in bed, and impaired sleep quality, especially for those who perceived the pandemic as highly stressful [
9]. A study in China reported COVID-19-related increases in generalized anxiety, which were more pronounced among younger people (<25 years) compared to older age groups [
10]. In another study, this time conducted in New Zealand, suicidal ideation was reported by 6% of participants during the COVID-19 lockdown, with 2% reporting making plans for suicide, 2% reporting suicide attempts and with suicidality levels the highest in those aged 18–34 [
11]. Health care workers also seem to be particularly affected. A meta-analysis of 13 studies of mental health among healthcare workers found that almost a quarter exhibited elevated COVID-19-related symptoms of anxiety (23.2%) and depression (22.8%) [
12].
Measures implemented to control the spread of the COVID-19 virus vary greatly by countries and regions [
13]. Countries across the globe faced different epidemiological situations, and even those impacted in a similar manner chose to respond to the pandemic in different ways. Early and effective containment measures have decreased infection rates [
13]; however, the benefits come with huge costs in terms of negative psychological outcomes [
9], especially when individuals are affected by specific stressors such as greater duration of confinement, inadequate supplies, difficulty securing medical care and financial losses [
14]. The home confinement of large swaths of the population for indefinite periods, differences among the stay-at-home orders issued by various jurisdictions, and conflicting messages from government and public health authorities have most likely intensified distress. The confinement also deepened social inequalities, causing more individuals to be vulnerable to the impacts of the pandemic. Although pandemic-related factors have greatly affected the mental health of the population, their interaction with a country’s socio-cultural, historic and political context is also expected to have influenced this response.
Beyond the stressors directly related to the pandemic, it is crucial to consider the infodemic as a critical factor contributing to the adverse outcomes of the COVID-19 pandemic. Not only can mis- and disinformation negatively impact an individual’s physical and mental health, they can ultimately affect countries’ abilities to stop the pandemic, as the effectiveness of public health measures is reduced due to poor compliance [
3]. As the pandemic continues to evolve, the relationship between communication strategies, media discourse and psychosocial impacts continues to strengthen. The negative influence of excessive exposure to media on mental health has been exposed in several studies. Wang et al. (2020) surveyed participants at two-time points following the commencement of the pandemic and found that increased exposure to radio reports about COVID-19 was significantly associated with higher levels of anxiety and depression [
15]. A German study also suggests that increased frequency, duration and diversity of media exposure increase the risk of psychological distress, with higher levels of anxiety and depression when social media is used as the primary type of information resource [
16]. Existing research also highlighted a number of COVID-19-related risks linked to information and communication failure such as confusion, misunderstanding, trust/mistrust, sense of fear, creation of conspiracy theories, denial, racial discrimination and avoidance behaviours, all potentially having harmful effects on mental health.
Various factors play important roles in coping with a highly stressful situation such as the COVID-19 pandemic and the ensuing turmoil [
17]. Given that disruption, loss, and confusion due to the pandemic and the infodemic could realistically affect our everyday lives, recognizing and strengthening these protective factors might be key to mitigating the psychosocial impacts of the current crisis. These encompass not only individual psychological resources, such as one’s sense of coherence (SOC) described in the salutogenic approach of health promotion [
18], but also socio-ecological factors for resilience such as family functioning, social support, social participation, and trust in healthcare institutions. These factors are known to be associated with positive mental health and well-being outcomes [
19]. SOC is a psychological resource that develops over the lifetime and increases individuals’ capacity to use resistance resources to effectively deal with stressful circumstances. Individuals with a higher SOC are able to show an understanding of their stressors, are more confident in their coping abilities, and more motivated to cope with stressors, making them more resilient when faced with stressful situations [
18]. This protective effect has been noted in various studies, where the buffering role of the SOC moderated the link between COVID-19 illness experiences and psychological well-being [
18,
20,
21].
The pandemic has had, and will continue to have, profound psychological effects around the world. It is essential to understand how the adverse mental health outcomes are progressing with the perpetuation of the health crisis, and how they are influenced by the infodemic and other challenges arising in the context of the pandemic. Multilevel factors that positively or negatively contribute to the psychological response of the population must be better understood, to put in place appropriate interventions. Numerous studies have explored these factors in conjunction with prospective changes in mental health, while others demonstrated the association between COVID-19 and mental health along with their influencing factors. However, additional research should be carried out to examine factors that affect the mental health of the population over time, to inform the development of sound mitigation strategies. This study therefore aims to (1) examine the evolution in anxiety and depression with the progression of the pandemic in adult populations from different countries and continents and (2) identify, among a wide range of individual and country-level factors, which ones are positively or negatively contributing to this evolving psychological response.
4. Discussion
The second phase of our interdisciplinary and international survey points to a multitude of findings that contribute to enhance our current understanding of the mental health crisis amid the pandemic. First, large and persistent psychosocial impacts of the COVID-19 among adults were found in a set of very diverse countries (in terms of epidemiological situations and sociocultural backgrounds) all over the world. Second, by using the exact same methodology (e.g., same target populations, recruitment strategies and measurement tools), worsening of anxiety and depression levels have been documented, particularly in young adults, between Phase 1 (May–June 2020) and Phase 2 (November 2020). Third, beyond young age, a wide range of factors negatively influencing mental health in times of the pandemic were highlighted, important factors (based on the magnitude of the effect size) were found, including a weaker SOC, COVID-19-related false beliefs, and self-isolation or quarantine.
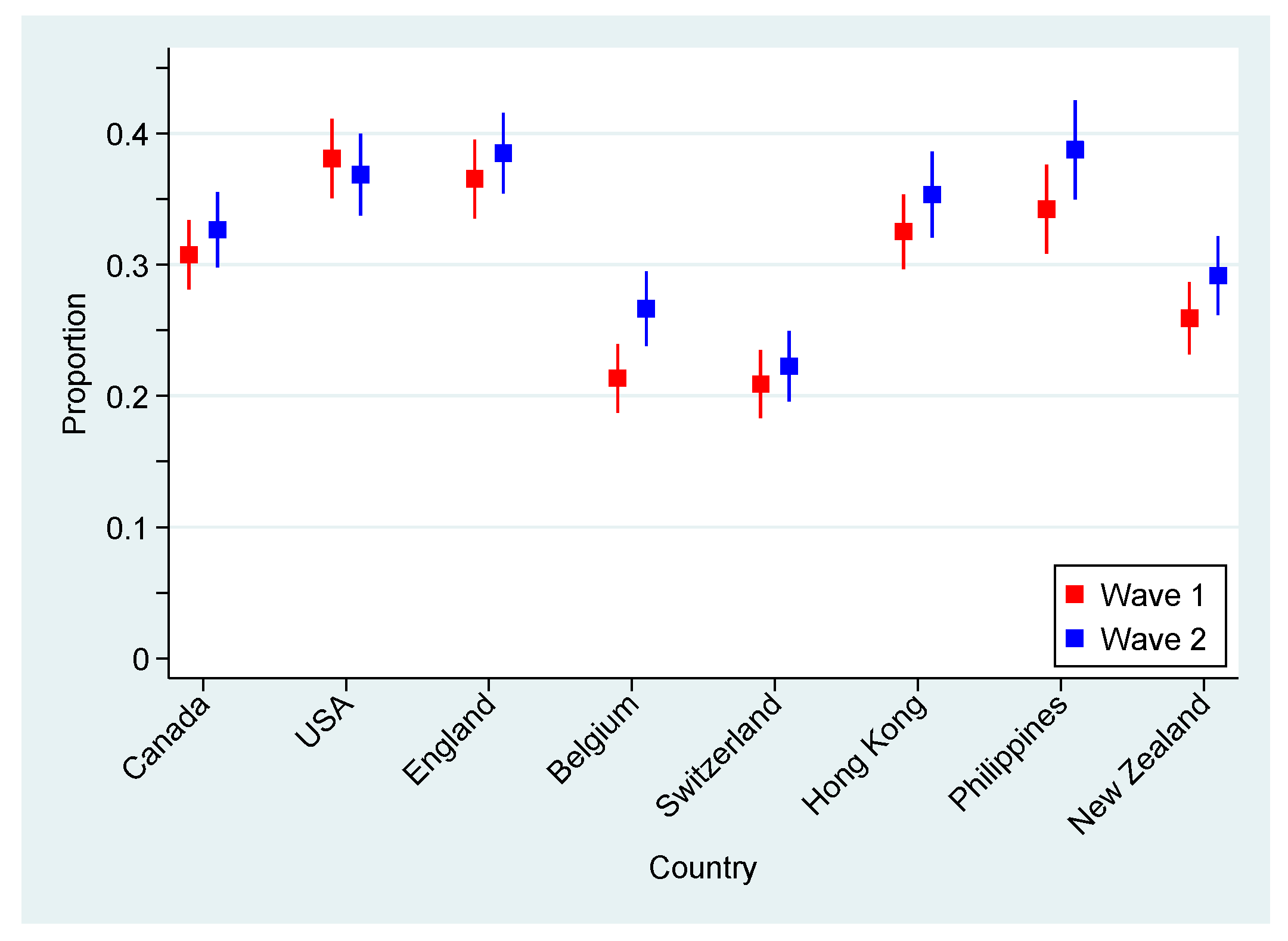
Overall, we found a small but significant deterioration with the progression of the COVID-19 pandemic in the psychological health of the adult population from eight countries and four continents. A global increase of 7.9% in the indication of either GAD or MDE was indeed noted from June–November 2020, with almost a third of the participants (32.5%) exhibiting symptoms consistent with one of these mental disorders in November. As discussed in an earlier article, such prevalence is much greater than what was estimated in the prepandemic era [
22].
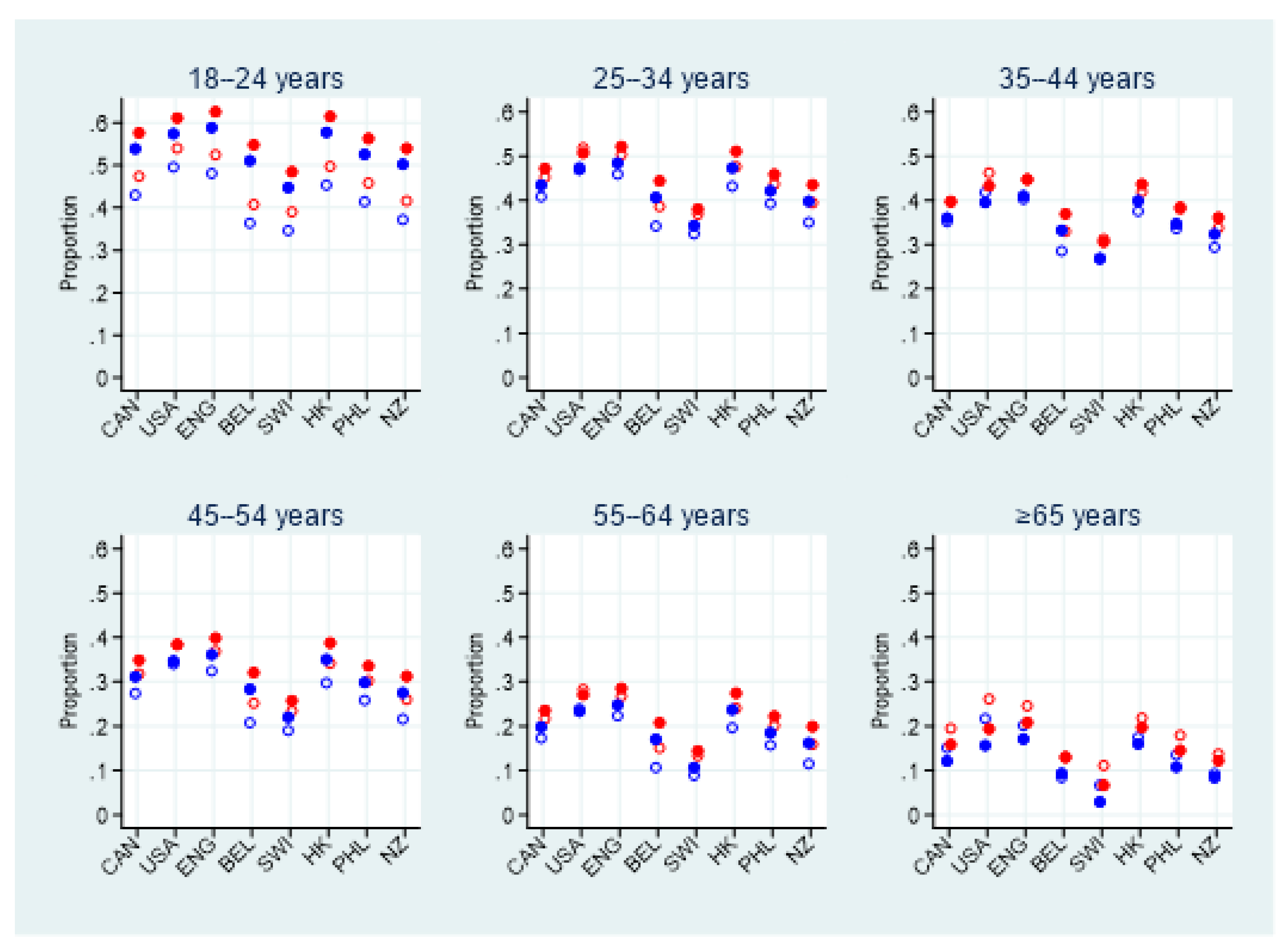
One key observation in the current study is of great importance and deserves full attention: in all countries but Switzerland, more than half of young adults reported symptoms consistent with GAD or MDE. This age group, which was already significantly affected by the pandemic in June 2020, showed deteriorating psychological health at a faster pace in the second half of 2020 than any other age group. There are many possible explanations for these disturbing results. Regardless of the pandemic, the transition from adolescence to adulthood has always been a stressful period filled with changes and adjustments [
30]. Since the beginning of the pandemic, youth faced additional stressors, including an overwhelming sense of loneliness; a reduction in social [
31], sport and cultural activities, homeschooling; loss of employment and financial stress for many [
32]; feeling of injustice due to the imbalance between efforts required and the rewards; and larger effects of the infodemic on this age group (resulting in more confusion and anger) [
32]. At first thought older adults may seem to be more vulnerable to negative psychological outcomes; however, this group was found to be less affected. These results were echoed in other studies were despite their high percentage of emotional distress, adults aged 60 years and older remained at a lower risk of developing depressive and stress consequences from COVID-19 and lockdown than their younger counterparts [
33].
Interestingly, the evolution of the epidemiological situation regarding the COVID-19 morbidity and mortality at the country-level does not seem to influence rates of probable anxiety or mood disorders. Indeed, despite being strongly affected by the second wave of COVID-19 during the time of the study, Switzerland and Belgium remain the two countries with the lowest indication for negative psychological outcomes. These countries seem to be less affected than New Zealand and Hong Kong, which reported very few new cases of the virus at the beginning of the month of November. Several studies have exposed the negative impacts of public health measures such as lockdown or stay-at-home recommendations on mental health regardless of the epidemiological situation in a country [
34]. The different measures applied by each government, their level of severity, their varying length of implementation, and the way the population receives, understands and perceives these measures could explain the variances in mental health outcomes between the participating countries [
34]. The implementation of regional-based measures and lockdowns seen in both Canada and the United States can act as a mental health stressor due to unclear information from public health authorities. This coincides with the observed negative psychological outcomes in these two countries. During the SARS epidemic in Toronto (Canada) in 2003, confusion stemmed from the content of various public health messages due to poor coordination between jurisdictions and levels of government [
34]. Then, it is suggested that longer quarantines could be linked to poorer mental health [
34]. The length of the lockdown enforced in the Philippines, spanning nearly six months since the start of the pandemic, is reflected in the results of the study as this country has one of the highest levels of GAD and MDE observed [
35]. Finally, lockdowns in Belgium and Switzerland were more relaxed than the other participating countries, with establishments such as businesses and restaurants remaining open (with restrictions). These elements could contribute to maintaining a relative normalcy, aiding in mitigating the psychological impacts of the pandemic.
When specifically considering the lower prevalence of GAD and MDE observed for Belgium and Switzerland, many potential factors may play a role in these findings. One aspect that must be considered is the timing between the waves (periods of confinement and deconfinement) in each respective country and the data collection periods. The first phase of data collection in June coincided with the first deconfinement in Belgium and the second phase in November fell just at the beginning of the second confinement. Another study done by the University of Louvain in Belgium revealed high levels of psychological distress for the month of March (the start of the confinement) and April (the peak of the first wave) [
36]. Another important aspect to consider is the internal geopolitical context of each country. Several participating countries have volatile political situations. Although our questionnaire sought to evaluate changes in the mental health outcomes caused by the pandemic, it is difficult for participants to disassociate from co-occurrent events that can also affect their mental health. For instance, the USA is the only participating country that experienced a decline in anxiety and depression levels. This could be owed to the fact that the USA presidential election day was on 3 November 2020, a few days before the second phase of data collection began.
Furthermore, the total population size of a country was found to act as independent predictor of either probable GAD or MDE. At first glance, it could be hypothesized that a larger size country could be affected negatively by both complex crisis management and communication strategies, resulting in increased negative mental health outcomes related to the pandemic. However, the relationship at stake might not be directly attributable to the population size, but rather their impact on trust, confidence and perception of proximity with authorities/elites (including health authorities in the case of COVID-19). Confidence and trust in national and/or local state authorities are expected to be lower in larger populations, often facing more inequalities and economic stress [
37,
38]. Lower trust in authorities leads to a greater sense of uncertainty, stress about future outcomes of the pandemic, and more dis/misinformation (as less confidence towards authorities incites the consumption and sharing of lower quality information), which can all be detrimental to mental health outcomes in a population [
39]. As seen in this study, high scores related to false beliefs and low scores related to trust in authorities both increase negative mental health outcomes, which corroborates the points raised above. In fact, infodemic-related factors (including mistrust, confusion and false beliefs, overload of information, and the use of social media to become informed) were found in our study to play an equally important role, if not more important, than pandemic-related factors in explaining psychological health in times of pandemic. This strongly supports the need for further interdisciplinary studies to investigate a comprehensive range of traditional and less traditional factors. This is crucial for a better understanding of what really undermines mental health in this unique era where erroneous information is spreading even more quickly than the SARS-CoV-2 itself.
As observed in the first phase of the study, the SOC is still critical in protecting against adversity caused by the two concurrent crises (i.e., the pandemic and the infodemic). Recent work has identified courses of action shown to increase SOC and, in general, the adaptive capacities of individuals and communities during stressful situations such as the ongoing pandemic [
40]. Interventions in health promotion that aim to support the strengthening of SOC need to focus on empowerment and reflection, and should be guided by various principles (i.e., positive approach, collaborative work, locally based, adapted to the context and local culture, inclusiveness). Such interventions can take several forms, going from programs focused on the development of mindfulness to artistic and cultural activities.
This study has several limitations, the main one being its cross-sectional nature, precluding our capacity to infer a causal link between risk/protective factors and mental health outcomes. When interpreting the changes in the data over time, it is important to consider that this study uses a repeated-cross sectional design and not a longitudinal approach, making it more difficult to attribute the changes in negative psychological outcomes to the various variables studied. Additionally, despite tremendous efforts in achieving representativeness in our sample, some groups of the population may be underrepresented, including adults with lower literacy levels and those not having access to a computer or the Internet. When considering the possible distorting effects of the weighting of the data, the weights had minimal effects on our main estimates (e.g., probable GAD or MDE). Indeed, probable GAD or MDE was indicated by 32.2% and 32.5% of the respondents using the unweighted and the weighted data, respectively (a 0.9% difference), suggesting that weights did not led to distortions of effects. Although the use of a cut-off value in the PHQ-9 and GAD-7 scales facilitates the interpretation of the data relating to the GAD or MDE (probable disorder: yes or no), it can also lead to some limits. As the original data takes a continuous from, some details are lost when using a cut-off and the prevalence of some of the factors may be overestimated [
41]. Another limitation would be the absence of a valid education level measure (or another indicator of individual socioeconomic status) suitable for the international analyses. Although the lack of such a variable is unfortunate, it was expected as participating countries were purposely selected for their diversity in terms of sociocultural backgrounds. In an attempt to minimize this gap, country-level variables were considered in phase 2 of the international survey, including variables related to the economic context (e.g., GINI index) and others related to the social determinants of health (e.g., mean age of schooling). Although various country-level data were considered in our analyses, including COVID-19 epidemiological data, the present study did not account for changes in public messaging, implemented measures and risk over time. These were difficult to assess as these variables differed greatly at a national level. For example, in Canada, during the observed periods, each province implemented their own restriction guidelines with the federal government only providing general recommendations such as social distancing, face masks and stay at home recommendation as well as enforcing a quarantine for travelers [
42]. Other countries had different approaches, such as England, which implemented a strict lockdown at a national level for a few weeks in November 2020 before returning to a regional approach [
43].


 ,
, 
{kind=link}
{kind=link}

