
Evaluation of a Wearable Non-Invasive Thermometer for Monitoring Ear Canal Temperature during Physically Demanding (Outdoor) Work

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Materials
2.2.1. Cosinuss° °Temp
2.2.2. Ambient Conditions Box
2.2.3. Reference Ear Canal Infrared Thermometer
2.2.4. Mercury Thermometer
2.3. Study Design
2.4. Data Analysis
3. Results
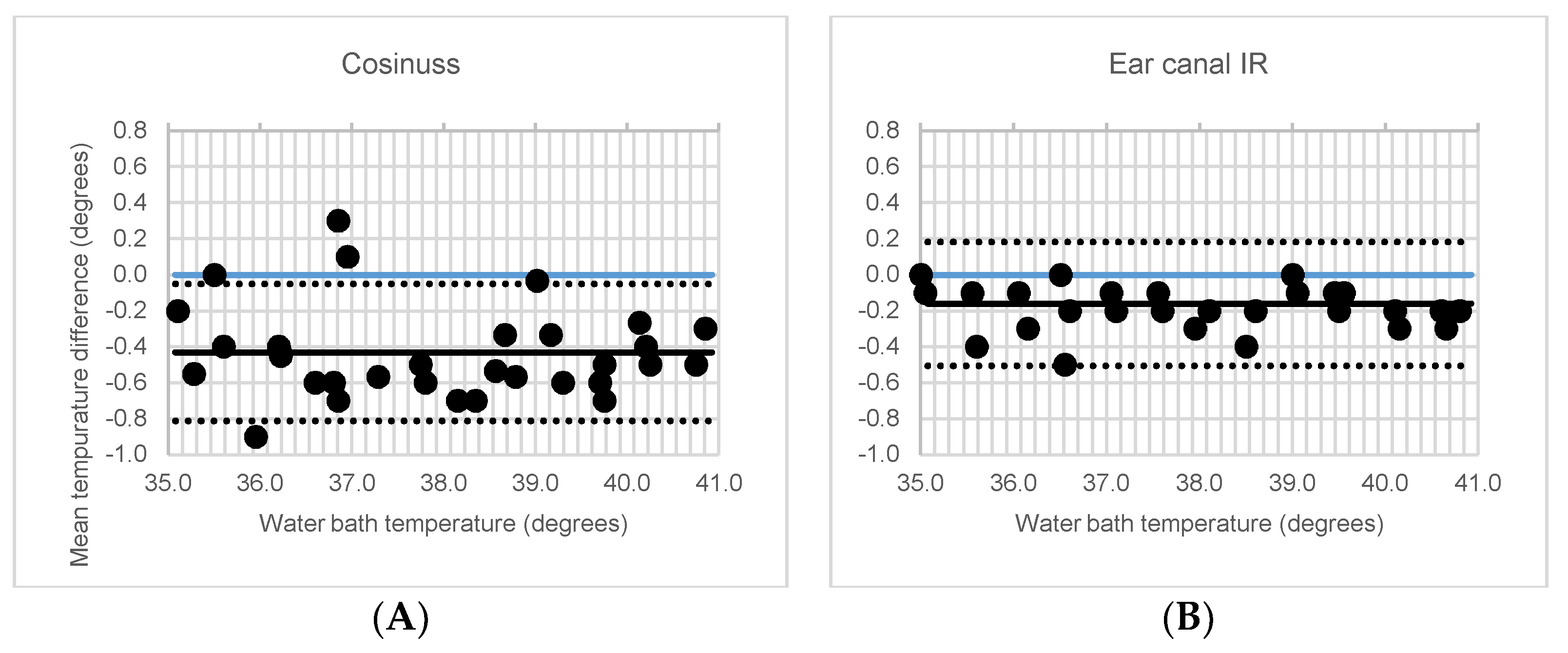
3.1. In-Vitro Accuracy
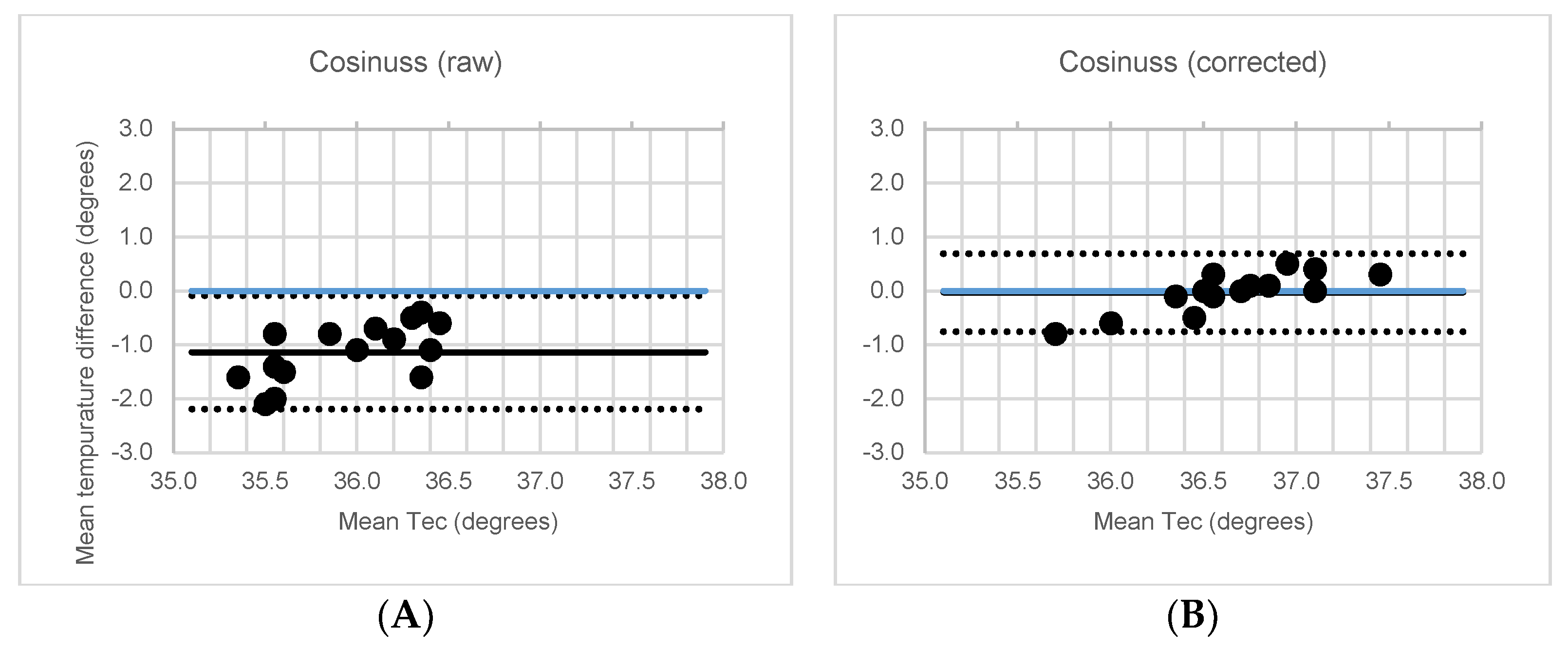
3.2. In-Vivo Accuracy under Controlled Conditions
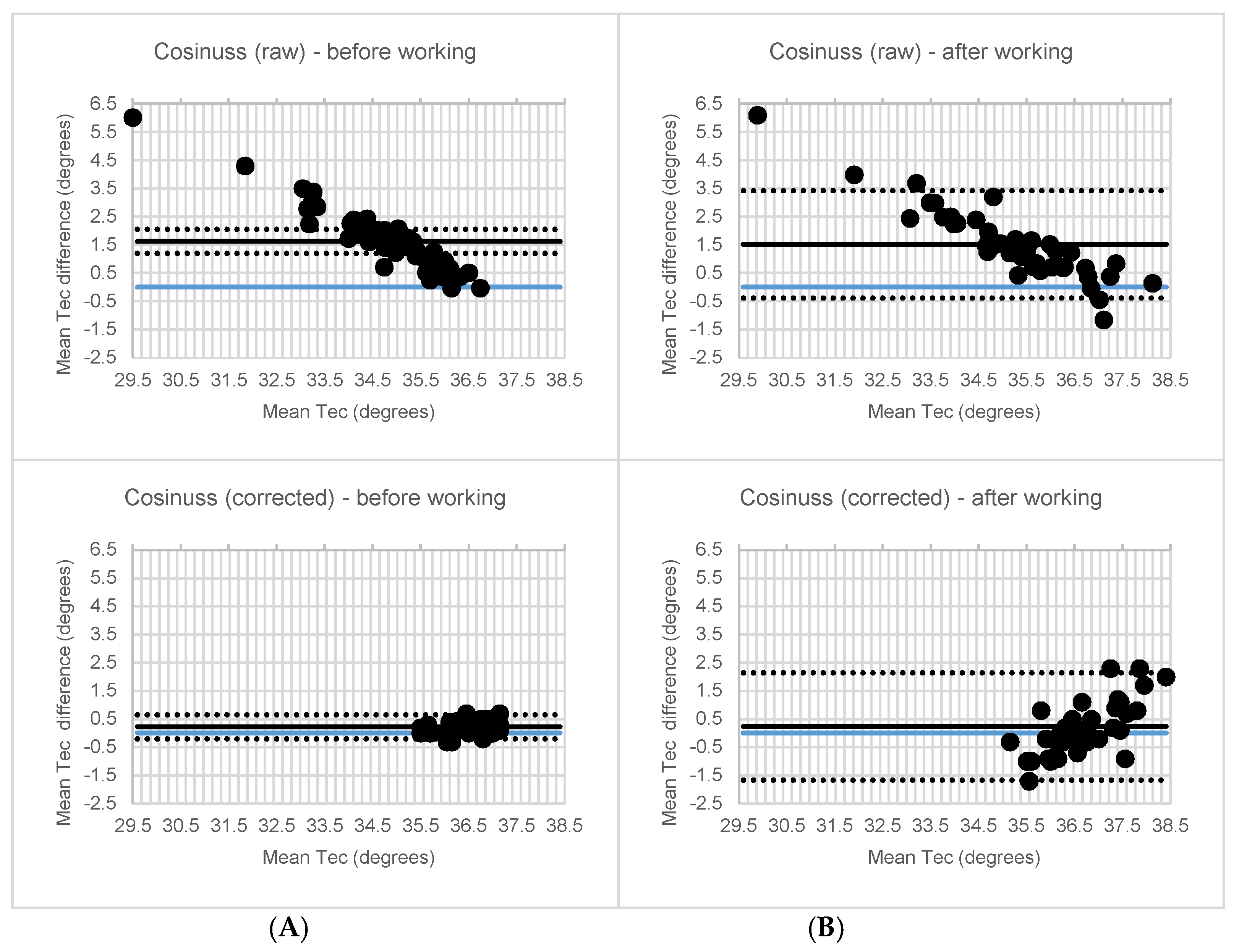
3.3. In Vivo Accuracy under Real-Life Conditions
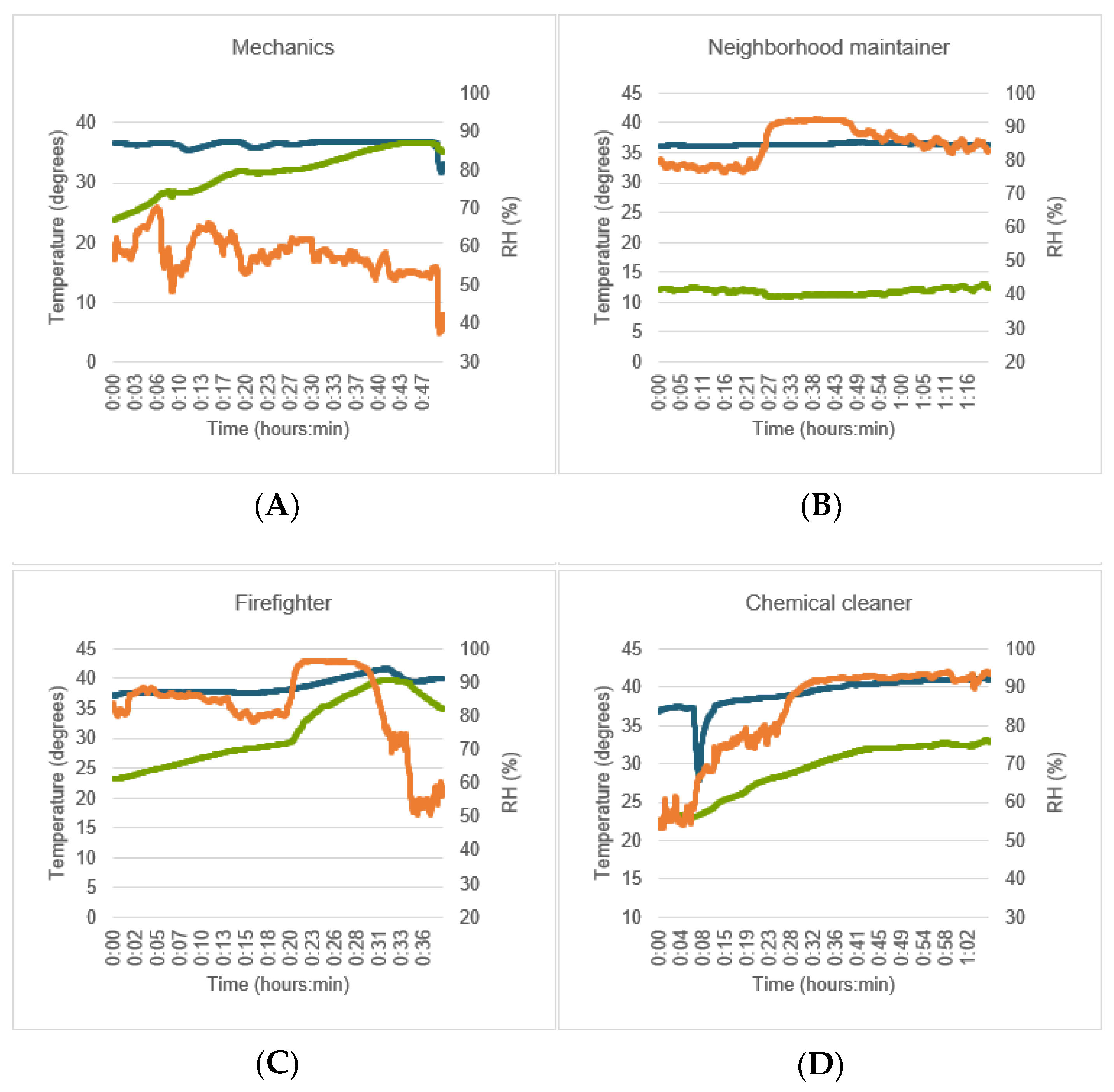
3.4. Influences of Real-Life Working Conditions on Accuracy
3.5. Usability
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Job Type | n | Mean TEC (°C) (raw) | Max TEC (°C) (raw) |
|---|---|---|---|
| All subjects | 49 | 34.88 ± 1.93 | 44.71 ± 2.32 |
| Chemical cleaners | 9 | 34.70 ± 2.87 | 38.77 ± 3.32 |
| Mechanics | 13 | 34.62 ± 1.51 | 37.25 ± 0.82 |
| Firefighters | 14 | 35.97 ± 1.18 | 44.71 ± 2.15 |
| Neighborhood maintainers | 13 | 34.13 ± 1.90 | 42.58 ± 2.18 |
| Job Type | n | MD ± SD [95% CI] | p | ICC [95% CI] | p |
|---|---|---|---|---|---|
| Before performance of the job | |||||
| Chemical cleaners | 9 | −1.67 ± 0.36 [−1.94;−1.39] | 0.000 | 0.19 [−0.02;0.64] | 0.001 |
| Mechanics | 13 | −1.04 ± 0.73 [−1.48;−0.60] | 0.000 | 0.17 [−0.11;0.55] | 0.092 |
| Firefighters | 14 | −1.64 ± 0.87 [−2.13;−1.13] | 0.000 | 0.08 [−0.08;0.36] | 0.167 |
| Neighborhood maintainers | 13 | −1.65 ± 1.86 [−2.77;−0.52] | 0.008 | 0.09 [−0.21;0.50] | 0.309 |
| After performance of the job | |||||
| Chemical cleaners | 7 | −1.46 ± 0.59 [−2.00;−0.92] | 0.001 | 0.21 [−0.07;0.71] | 0.039 |
| Mechanics | 13 | −1.37 ± 0.94 [−1.94;−0.80] | 0.000 | 0.18 [−0.11;0.57] | 0.077 |
| Firefighters | 13 | −1.21 ± 1.05 [−1.85;−0.57] | 0.001 | 0.25 [−0.13;0.64] | 0.066 |
| Neighborhood maintainers | 10 | −1.92 ± 2.02 [−3.37;−0.47] | 0.015 | 0.01 [−0.26;0.46] | 0.487 |
References
- Gao, C.; Kuklane, K.; Ostergren, P.; Kjellstrom, T. Occupational heat stress assessment and protective strategies in the context of climate change. Int. J. Biometeorol. 2018, 62, 359–371. [Google Scholar] [PubMed]
- Udayraj; Wang, F.; Song, W.; Ke, Y.; Xu, P.; Chow, C.S.W.; Noor, N. Performance enhancement of hybrid personal cooling clothing in a hot. Ergonomics 2019, 62, 928–939. [Google Scholar] [CrossRef] [PubMed]
- Song, W.; Wang, F. The hybrid personal cooling system (PCS) could effectively reduce the heat strain while exercising in a hot and moderate humid environment. Ergonomics 2016, 59, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.; Guo, Y.P.; Wong, F.K.W.; Li, Y.; Sun, S.; Han, X. The development of anti-heat stress clothing for construction workers in hot and humid weather. Ergonomics 2016, 59, 479–495. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurthy, M.; Ramalingam, P.; Perumal, K.; Kamalakannan, L.P.; Chinnadurai, J.; Shanmugam, R.; Srinivasan, K.; Venugopal, V. Occupational Heat Stress Impacts on Health and Productivity in a Steel Industry in Southern India. Saf. Health Work 2017, 8, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, A.; Moreira, D.G.; Brito, C.J.; da Silva, C.D.; Sillero-Quintana, M.; Pimenta, E.M.; Bach, A.J.; Garcia, E.S.; Marins, J.C.B. Validity of inner canthus temperature recorded by infrared thermography as a non-invasive surrogate measure for core temperature at rest, during exercise and recovery. J. Therm. Biol. 2016, 62, 50–55. [Google Scholar] [CrossRef]
- Larsen, B.; Snow, R.; Vincent, G.; Tran, J.; Wolkow, A.; Aisbett, B. Multiple Days of Heat Exposure on Firefighters’ Work Performance and Physiology. PLoS ONE 2015, 10, e136413. [Google Scholar]
- Epstein, Y.; Moran, D. Thermal effects on the Heat Stress Indices. Ind. Health 2006, 2006, 388–398. [Google Scholar]
- Jacklitsch, B.; Williams, W.J.; Musolin, K.; Coca, A.; Kim, J.H.; Turner, N. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS. In NIOSH Criteria for a Recommended Standard: Occupational Exposure to Heat and Hot; NIOSH: Cincinnati, OH, USA, 2018. [Google Scholar]
- Roghanchi, P.; Kocsis, K. Challenges in Selecting an Appropriate Heat Stress Index to Protect Workers in Hot and Humid Underground Mines. Saf. Health Work 2018, 9, 10–16. [Google Scholar] [CrossRef]
- Morgado, M.; Talaia, M.; Teixeira, L. A new simplified model for evaluating thermal environment and thermal sensation: An approach to avoid occupational disorders. Int. J. Ind. Ergon. 2017, 60, 3–13. [Google Scholar]
- Broday, E.; de Paula Xavier, A.; de Oliveira, R. Comparative analysis of methods for determining the clothing surface temperature (tcl) in order to provide a balance between man and the environment. Int. J. Ind. Ergon. 2017, 2017, 80–87. [Google Scholar] [CrossRef]
- Sunkpal, M.; Roghanchi, P.; Kocsis, K. A Method to Protect Mine Workers in Hot and Humid Environments. Saf. Health Work 2018, 9, 149–158. [Google Scholar] [CrossRef]
- Piil, J.; Lundbye-Jensen, J.; Christiansen, L.; Ioannou, L.; Tsoutsoubi, L.; Dallas, C.N.; Mantzios, K.; Flouris, A.D.; Nybo, L. High prevalence of hypohydration in occupations with heat stress—Perspectives for performance in combined cognitive and motor tasks. PLoS ONE 2018, 13, e205321. [Google Scholar] [CrossRef] [Green Version]
- Quinn, T.; Seo, Y.; Yorio, P.L.; AlJaroudi, A.; Coca, A.; Kim, J.-H.; Roberge, R.J.; Williams, W.J. Using trunk posture to monitor heat strain at work. Ergonomics 2018, 61, 1560–1568. [Google Scholar] [CrossRef]
- Costello, J.; Stewart, K.; Stewart, I. The effects of metabolic work rate and ambient environment on philological tolerance times while wearing explosive and chemical personal protective equipment. BioMed Res. Int. 2015, 2015, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Dube, P.; Imbeau, D.; Dubeau, D.; Auger, I. Worker heat stress prevention and work metabolism estimation: Comparing two assessment methods of the heart rate thermal component. Ergonomics 2019, 62, 1066–1085. [Google Scholar] [CrossRef]
- Smith, D.; Petruzzello, J. Selected physiological and psychological responses to live-fire drills in diffrent configurations of firefighting gear. Ergonomics 1998, 41, 1141–1154. [Google Scholar] [CrossRef]
- Horn, G.; Kesler, R.M.; Kerber, S.; Fent, K.W.; Schroeder, T.J.; Scott, W.S.; Fehling, P.C.; Fernhall, B.; Smith, D.L. Thermal response to firefighting activities in residential structure fires: Impact of job assignment and suppression tactic. Ergonomics 2018, 61, 404–419. [Google Scholar] [CrossRef]
- Taylor, N.; Tipton, M.; Kenny, G. Considerations for the measurement of core, skin and mean body temperatures. J. Therm. Biol. 2014, 46, 72–101. [Google Scholar] [CrossRef] [Green Version]
- Langridge, P.; Ruzic, A.; Larsen, B.; Lord, C.; Aisbett, B. Assessing the validity of tympanic temperature to predict core temperature of firefighters in different environmental conditions. In Proceedings of the Bushfire CRC & AFAC 2012 Conference Research Forum, Perth, Australia, 28 August 2012; pp. 150–159. [Google Scholar]
- Gonzalez-Alonso, J.; Teller, C.; Andersen, S.L.; Jensen, F.B.; Hyldig, T.; Nielsen, B. Influence of body temperature on the development of fatigue during prolonged exercise in the heat. Hyperth. Fatigue 1999, 86, 1032–1039. [Google Scholar] [CrossRef] [Green Version]
- Moran, D.; Mendal, L. Core temperature measurement: Methods and current insights. Sports Med. 2002, 32, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Buller, M.; Tharion, W.; Duhamel, C.; Yokota, M. Real-time core body temperature estimation from heart rate for first responders wearing different levels of personal protective equipment. Ergonomics 2015, 58, 1830–1841. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.; Byrne, C.; Lee, J. Human Thermoregulation and Measurement of Body Temperature in Exercise and Clinical Settings. Ann. Acad. Med. Singap. 2008, 37, 347–353. [Google Scholar] [PubMed]
- Holland, E.; Laing, R.; Lemmon, T.; Niven, B. Helmet design to facilitate thermoneutrality during harvesting. Ergonomics 2002, 45, 699–716. [Google Scholar] [CrossRef]
- Saurabh, K.; Rao, H.; Amrutur, B.; Sundarranjan, A. Continuous core body temperature estimation via surface temperature measurements using wearable sensors: Is it feasible? Biodevices 2014, 181–186. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Weng, W.; Wang, F.; Song, G. Integrating a human thermoregulatory model with a clothing model. Appl. Ergon. 2017, 61, 168–177. [Google Scholar] [CrossRef]
- Ng, K.; Wong, S.; Lim, S.; Goh, Z. Evaluation of the Cadi ThermoSENSOR Wireless Skin-Contact Thermometer Against Ear and Axillary Temperatures in Children. J. Pediatric Nurs. 2009, 25, 176–186. [Google Scholar] [CrossRef]
- Chaglla, J.; Celik, N.; Balanchandran, W. Measurement of Core Body Temperature Using Graphene Inked Infrared Thermopile Sensor. Sensors 2018, 18, 3315. [Google Scholar] [CrossRef] [Green Version]
- Mazgoaker, S.; Ketko, I.; Yanovich, R.; Heled, Y.; Epstein, Y. Measuring core body temperature with a non-invasive sensor. J. Therm. Biol. 2017, 66, 17–20. [Google Scholar] [CrossRef]
- Pancardo, P.; Acosta, F.D.; Hernández-Nolasco, J.A.; Wister, M.A.; López-De-Ipiña, D. Real-Time Personalized Monitoring to Estimate Occupational Heat Stress in Ambient Assisted Working. Sensors 2015, 15, 16956–16980. [Google Scholar] [CrossRef]
- Roossien, C.; Heus, R.; Reneman, M.; Verkerke, G. Monitoring core temperature of firefighters to validate a wearable non-invasive core thermometer in different types of protective clothing: Concurrent in-vivo validation. Appl. Ergon. 2020, 83, 103001. [Google Scholar] [CrossRef]
- Muir, I.; Bishop, P.; Lomax, R.; Green, J. Prediction of rectal temperature from ear canal temperature. Ergonomics 2001, 44, 962–972. [Google Scholar] [CrossRef]
- Towey, C.; Easton, C.; Simpson, R.; Pedlar, C. Conventional and novel body temperature measurement during rest and exercise induced hyperthermia. J. Therm. Biol. 2017, 63, 124–130. [Google Scholar] [CrossRef] [Green Version]
- Ganio, M.S.; Brown, C.M.; Casa, D.J.; Becker, S.M.; Yeargin, S.W.; McDermott, B.P.; Boots, L.M.; Boyd, P.W.; Armstrong, L.E.; Maresh, C.M. Validity and Reliability of Devices That Assess Body Temperature During Indoor Exercise in the Heat. J. Athl. Train. 2009, 44, 124–135. [Google Scholar] [CrossRef] [Green Version]
- Casa, D.; Becker, S.M.; Ganio, M.S.; Brown, C.M.; Yeargin, S.W.; Roti, M.W.; Siegler, J.; A Blowers, J.; Glaviano, N.R.; Huggins, R.A.; et al. Validity of devices that assess body temperature during outdoor exercise in the heat. J. Athl. Train. 2007, 42, 333–342. [Google Scholar]
- Cosinuss. Technisches Datenblatt Cosinuss One; Cosinuss GmbH: Munchen, Germany, 2016. [Google Scholar]
- Sensirion. Datasheet SHT1x (SHT10, SHT11, SHT15)—Humidity and Temperature Sensor; Sensirion AG: Staefa ZH, Switzerland, 2010. [Google Scholar]
- CTS GmbH. CTS-Climatic Test Chambers; CTS GmbH: Hechingen, Germany, unknown.
- Braun GmbH. ThermoScan® 7 Met Age Precision®–IRT6520—User Manual. 2017. Available online: www.brauntherms.com/nl/producten/thermoscan-7-oor-thermometer-irt6520/ (accessed on 30 April 2017).
- LAUDA R. WOBSER GmbH & Co. KG. Betriebsanleitung; LAUDA R. WOBSER GmbH & Co. KG: Lauda-Koningshofen, Germany, 1998. [Google Scholar]
- Ansell Protective Solutions AB. Product Sheet Trellechem Super; Ansell Protective Solutions AB: Trelleborg, Sweden, 2017. [Google Scholar]
- Cicchetti, D. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]
- Bland, J.; Altman, D. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef]
- Shrout, P.; Fleiss, J. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Calusic, A.; Marin, M.; Marija, V.V.; Branko, P.; Jelena, M.; Nevenka, K.; Ana, L.V.; Daver, Z. Biomarkers of mild hyperthermia related to flashover training in firefighters. J. Therm. Biol. 2012, 37, 548–555. [Google Scholar] [CrossRef]
- Itani, M.; Ghaddar, N.; Ouahrani, D.; Ghali, K.; Khater, B. An optimal two-bout strategy with phase change material cooling vests to improve comfort in hot environment. J. Therm. Biol. 2018, 72, 10–25. [Google Scholar] [CrossRef]
- Coso, J.; Aguado-Jimenez, R.; Mora-Roderiguez, R. Infrared tympanic thermometry in a hot environment. Int. J. Sports Med. 2008, 29, 713–718. [Google Scholar] [CrossRef]
- van Staaij, B.; Rovers, M.; Schilder, A.; Hoes, A. Accuracy and feasibility of daily infrared tympanic membrane temperature measurements in the identification of fever in children. Int. J. Pediatr. Otorhinolaryngol. 2003, 67, 1091–1097. [Google Scholar] [CrossRef]
- Gasim, G.; Musa, I.; Abdien, M.; Adam, I. Accuracy of tympanic temperature measurement using an infrared tympanic membrane thermometer. BMC Res. Notes 2013, 6, 194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shelton-Rayner, G.K.; Mian, S.R.; Chandler, D.; Robertson, D.; Macdonald, D.W. Leukocyte responsiveness, a quantitative assay for subjective mental workload. Int. J. Ind. Ergon. 2012, 42, 25–33. [Google Scholar] [CrossRef]
- Kocoglue, H.; Goksu, S.; Isik, M.; Akturk, Z.; Bayazit, Y. Infrared tympanic thermometer can accurately measure the body temperature in children in an emergency room setting. Int. J. Pediatr. Otorhinolaryngol. 2012, 65, 39–43. [Google Scholar] [CrossRef]
- Ammann, R.A.; Teuffel, O.; Agyeman, P.K.A.; Amport, N.; Leibundgut, K. The Influence of Different Fever Definitions on the Rate of Fever in Neutropenia Diagnosed in Children with Cancer. PLoS ONE 2015, 10, e117528. [Google Scholar] [CrossRef] [Green Version]
- Levander, M.; Grodzinsky, E. Variation in Normal Ear Temperature. Am. J. Med. Sci. 2017, 354, 370–378. [Google Scholar] [CrossRef] [Green Version]
- Kuht, J.; Farmery, A. Body temperature and its regulation. Anaesth. Intensive Care Med. 2014, 15, 273–278. [Google Scholar] [CrossRef]
- Mogensen, C.; Wittenhoff, L.; Frurhoj, G.; Hansen, S. Forehead or ear temperature measurement cannot replace rectal measurements, except for screening purposes. BMC Pediatr. 2018, 18, 15. [Google Scholar] [CrossRef] [Green Version]
- Teunissen, L.; de Haan, A.; de Koning, J.; Daanen, H. Telemetry pill versus rectal and esophageal temperature during extreme rates of exercise-induced core temperature change. Physiol. Meas. 2012, 33, 915–924. [Google Scholar] [CrossRef]
- Uth, M.; Koch, J.; Sattler, F. Body core temperature sensing: Challenges and new sensor technologies. Procedia Eng. 2016, 168, 89–92. [Google Scholar] [CrossRef]
- Dias, D.; Cunha, J. Wearable Health Devices—Vital Sign Monitoring, Systems and Technologies. Sensors 2018, 18, 2414. [Google Scholar] [CrossRef] [Green Version]
- Sun, X.; Zhang, Y. Design and Implementation of Portable ECG and Body Temperature Monitor. In Proceedings of the International Symposium on Computer, Consumer and Control, Taichung, Taiwan, 6–8 December 2014. [Google Scholar]
- Mansor, H.; Shukor, M.H.A.; Meskam, S.S.; Rusli, N.Q.A.M.; Zamery, N.S. Body temperature measurement for remote health monitoring system. In Proceedings of the IEEE International Conference on Smart Instrumentation, Measurement and Applications (ICSIMA), Kuala Lumpur, Malaysia, 26–27 November 2013. [Google Scholar]
- Al Rasyid, M.; Lee, B.; Sudarsono, A. Wireless body area network for monitoring body temperature, heart beat and oxygen in blood. In Proceedings of the 2015 International Seminar on Intelligent Technology and Its Applications (ISITIA), Surabaya, Indonesia, 20–22 May 2015. [Google Scholar]
- Jones, W. Taking body temperature, inside out [body temperature monitoring]. IEEE Spectr. 2006, 43, 13–15. [Google Scholar] [CrossRef]






| MD ± SD [95% CI] | p | ICC [95% CI] | p | LoA | |
|---|---|---|---|---|---|
| Cosinuss° | −0.4 ± 0.2 [−0.6;−0.3] | <0.001 | 0.97 [0.13;1.00] | <0.001 | ±0.37 |
| Ear canal IR | −0.2 ± 0.1 [−0.3;−0.1] | <0.001 | 0.99 [0.87;1.007] | <0.001 | ±0.24 |
| MD ± SD [95% CI] | p | ICC [95% CI] | p | LoA | |
|---|---|---|---|---|---|
| Raw | 1.4 ± 0.5 [1.1;1.7] | <0.001 | 0.07 [−0.05;0.31] | 0.083 | ±1.05 |
| With correction factor | 0.0 ± 0.4 [−0.2;0.2] | 0.729 | 0.72 [0.33;0.90] | 0.001 | ±0.72 |
| Working | MD ± SD [95% CI] | p | ICC [95% CI] | p | LoA |
|---|---|---|---|---|---|
| Raw | |||||
| Before working (n = 49) | 1.5 ± 1.2 [1.1;1.8] | <0.001 | 0.13 [−0.08;0.37] | 0.021 | ±2.23 |
| After working (n = 43) | 1.5 ± 1.2 [1.1;1.8] | <0.001 | 0.25 [−0.09;0.54] | 0.002 | ±2.44 |
| Corrected per subject | |||||
| Before working (n = 49) | −0.2 ± 0.2 [−0.3;−0.2] | <0.001 | 0.77 [0.19;0.91] | <0.001 | ±0.43 |
| After working (n = 43) | −0.2 ± 1.0 [−0.5;0.1] | 0.110 | 0.55 [0.32;0.73] | <0.001 | ±1.90 |
| Job Type | n | Mean TEC (°C) (Corrected) | Mean Tcli (°C) | Mean RH (%) | Max TEC (°C) | Max Tcli (°C) | Max RH (%) |
|---|---|---|---|---|---|---|---|
| All subjects | 49 | 36.8 ± 1.6 | 26.9 ± 4.9 | 62.6 ± 12.7 | 46.4 ± 2.0 | 39.5 ± 6.1 | 92.6 ± 13.6 |
| Chemical cleaners | 9 | 37.6 ± 1.5 | 26.9 ± 1.9 | 78.8 ± 5.7 | 46.4 ± 2.8 | 33.0 ± 1.8 | 91.9 ± 2.1 |
| Mechanics | 13 | 36.1 ± 0.8 | 28.0 ± 2.2 | 49.7 ± 9.0 | 38.3 ± 0.6 | 36.5 ± 2.7 | 75.9 ± 10.9 |
| Firefighters | 14 | 37.9 ± 0.7 | 31.2 ± 2.2 | 67.6 ± 7.7 | 41.6 ± 1.2 | 39.5 ± 3.0 | 92.5 ± 3.4 |
| Neighborhood maintainers | 13 | 36.0 ± 2.0 | 21.2 ± 4.8 | 60.1 ± 8.7 | 42.7 ± 2.0 | 28.9 ± 4.8 | 88.4 ± 8.2 |
| Job Type | n | MD ± SD [95% CI] | p | ICC [95% CI] | p |
|---|---|---|---|---|---|
| Before performance of the job | |||||
| Chemical cleaners | 9 | −0.2 ± 0.2 [−0.4;−0.1] | 0.007 | 0.88 [0.16;0.98] | <0.001 |
| Mechanics | 13 | −0.1 ± 0.2 [−0.3;0.0] | 0.087 | 0.81 [0.47;0.94] | <0.001 |
| Firefighters | 14 | −0.3 ± 0.2 [−0.4;−0.3] | <0.001 | 0.51 [−0.08;0.85] | <0.001 |
| Neighborhood maintainers | 13 | −0.2 ± 0.3 [−0.4;−0.1] | 0.012 | 0.67 [0.11;0.90] | 0.001 |
| After performance of the job | |||||
| Chemical cleaners | 7 | −0.4 ± 0.6 [−0.9;0.1] | 0.083 | 0.60 [−0.06;0.91] | 0.029 |
| Mechanics | 13 | 0.2 ± 0.5 [−0.1;0.5] | 0.121 | 0.63 [0.18;0.87] | 0.005 |
| Firefighters | 13 | −0.7 ± 1.0 [0.6;1.9] | 0.029 | 0.28 [−0.16;0.68] | 0.110 |
| Neighborhood maintainers | 10 | 0.1 ± 1.2 [−0.8;1.0] | 0.796 | −0.09 [−0.77;0.57] | 0.594 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roossien, C.C.; Hodselmans, A.P.; Heus, R.; Reneman, M.F.; Verkerke, G.J. Evaluation of a Wearable Non-Invasive Thermometer for Monitoring Ear Canal Temperature during Physically Demanding (Outdoor) Work. Int. J. Environ. Res. Public Health 2021, 18, 4896. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094896
Roossien CC, Hodselmans AP, Heus R, Reneman MF, Verkerke GJ. Evaluation of a Wearable Non-Invasive Thermometer for Monitoring Ear Canal Temperature during Physically Demanding (Outdoor) Work. International Journal of Environmental Research and Public Health. 2021; 18(9):4896. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094896
Chicago/Turabian StyleRoossien, Charlotte Christina, Audy Paul Hodselmans, Ronald Heus, Michiel Felix Reneman, and Gijsbertus Jacob Verkerke. 2021. "Evaluation of a Wearable Non-Invasive Thermometer for Monitoring Ear Canal Temperature during Physically Demanding (Outdoor) Work" International Journal of Environmental Research and Public Health 18, no. 9: 4896. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094896