
Negative Impact of Fear of COVID-19 on Health-Related Quality of Life Was Modified by Health Literacy, eHealth Literacy, and Digital Healthy Diet Literacy: A Multi-Hospital Survey

 , , , , ,
, , , , ,  , and
, and  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Study Sample and Data Collection
2.3. Instruments and Measurements
2.3.1. Health-Related Quality of Life
2.3.2. Fear of COVID-19
2.3.3. Health Literacy and Digital Healthy Diet Literacy
2.3.4. eHealth Literacy
2.3.5. Participants’ Characteristics
2.3.6. Lifestyle Changes
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Associations of HL, eHEALS, DDL, and FCoV-19S with HRQoL
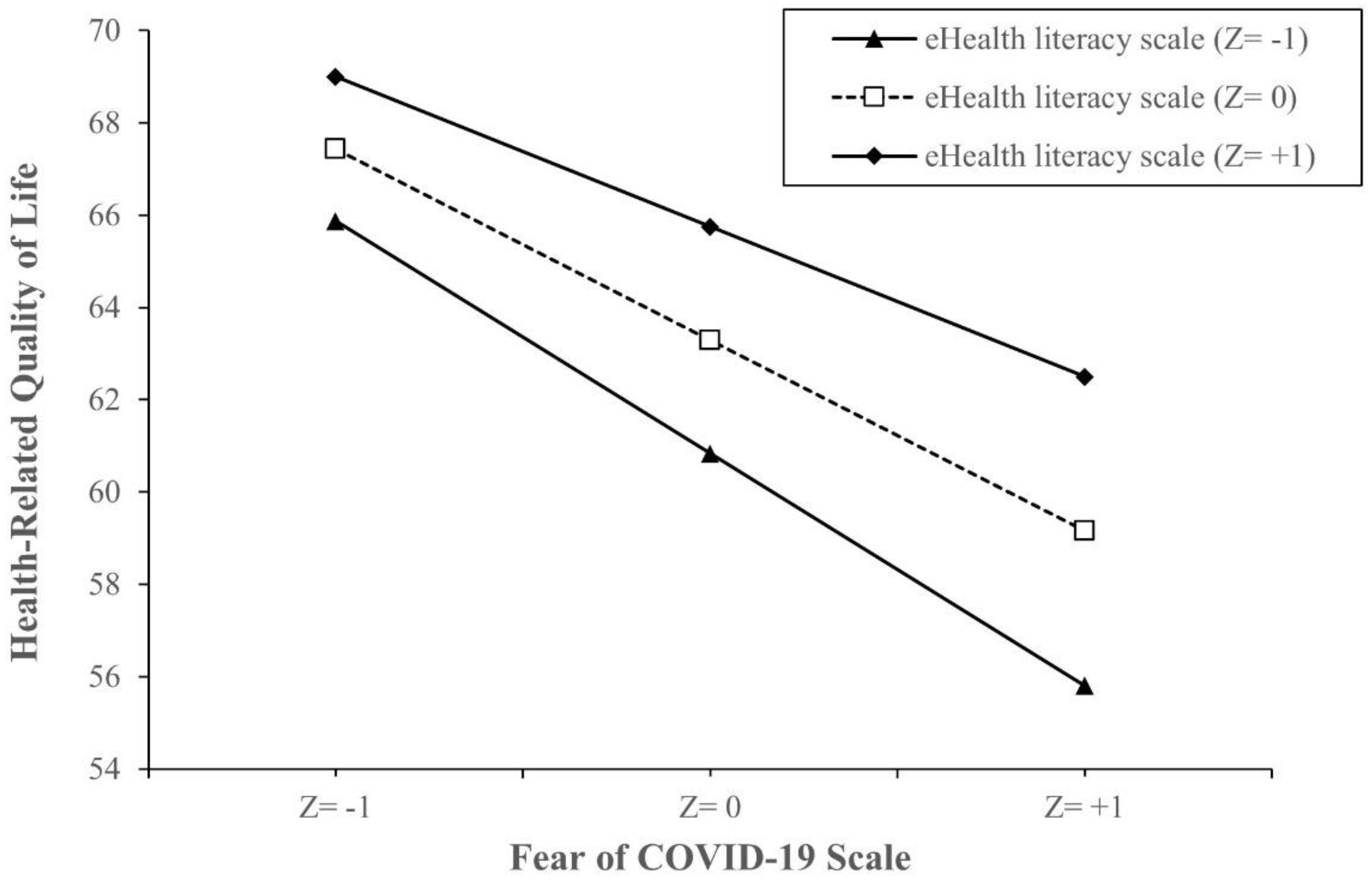
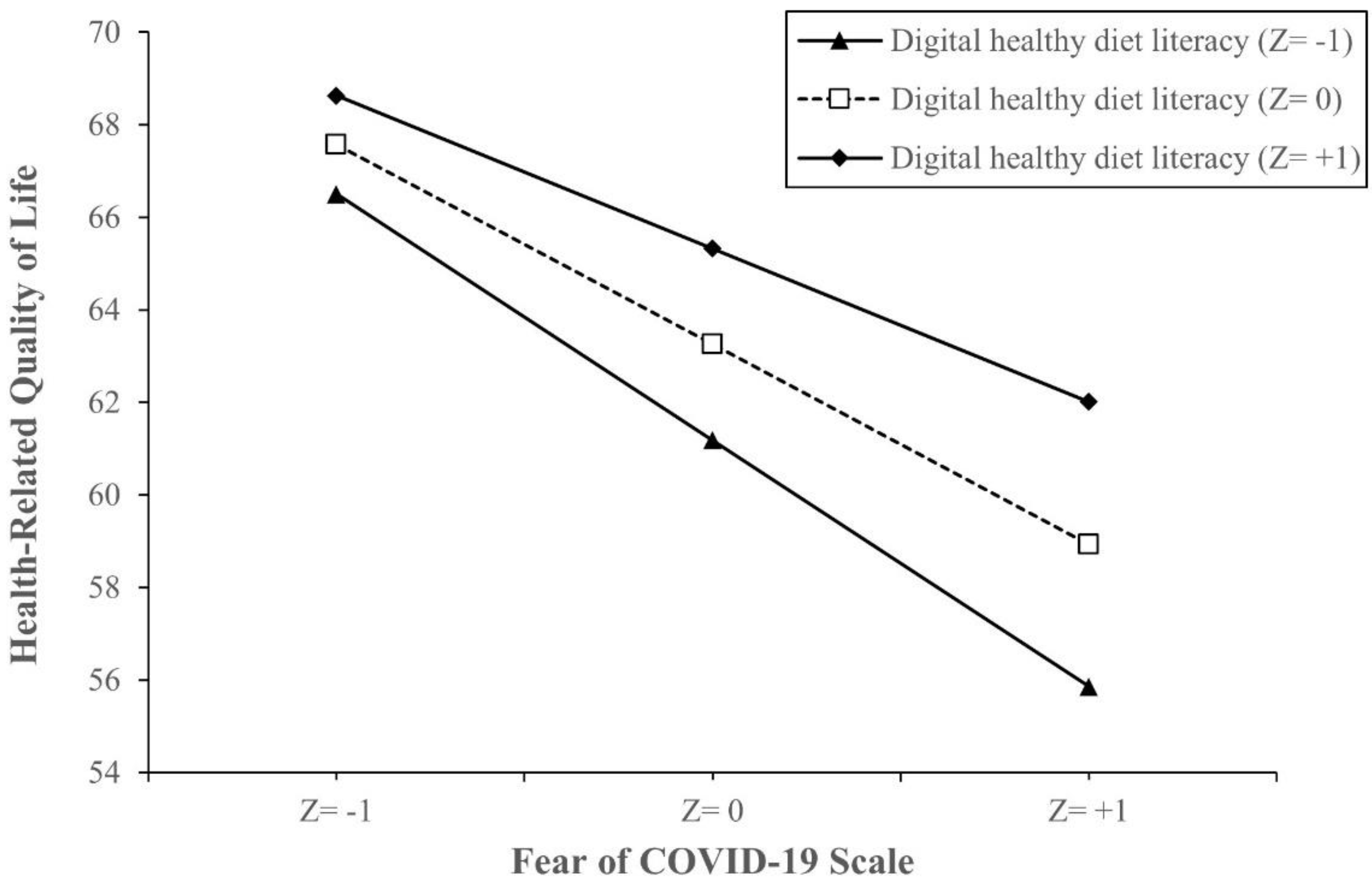
3.3. Effect Modification by eHEALS and DDL on the Association between FCoV-19S and HRQoL
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| B | Unstandardized regression coefficient |
| DDL | Digital healthy diet literacy |
| eHEALS | eHealth Literacy Scale |
| FCoV-19S | Fear of COVID-19 Scale |
| HL | Health literacy |
| HLS-SF12 | 12-item short-form health literacy questionnaire |
| HRQoL | Health-related quality of life |
| OPD | Outpatient departments |
| S-COVID-19-S | Suspected COVID-19 symptoms |
References
- Phelan, A.L.; Katz, R.; Gostin, L.O. The Novel Coronavirus Originating in Wuhan, China: Challenges for Global Health Governance. JAMA 2020, 323, 709–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, N.; Docherty, M.; Gnanapragasam, S.; Wessely, S. Managing mental health challenges faced by healthcare workers during covid-19 pandemic. BMJ 2020, 368, m1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. Coronavirus disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 15 September 2020).
- Nazir, M.; Hussain, I.; Tian, J.; Akram, S.; Mangenda Tshiaba, S.; Mushtaq, S.; Shad, M.A. A Multidimensional Model of Public Health Approaches Against COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 3780. [Google Scholar] [CrossRef] [PubMed]
- Wei, K.; Nyunt, M.S.Z.; Gao, Q.; Wee, S.L.; Ng, T.P. Long-term changes in nutritional status are associated with functional and mortality outcomes among community-living older adults. Nutrition 2019, 66, 180–186. [Google Scholar] [CrossRef]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Cohen Silver, R.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Goyal, K.; Chauhan, P.; Chhikara, K.; Gupta, P.; Singh, M.P. Fear of COVID 2019: First suicidal case in India! Asian J. Psychiatr. 2020, 49, 101989. [Google Scholar] [CrossRef]
- Lazzerini, M.; Barbi, E.; Apicella, A.; Marchetti, F.; Cardinale, F.; Trobia, G. Delayed access or provision of care in Italy resulting from fear of COVID-19. Lancet Child Adolesc Health 2020, 4, e10–e11. [Google Scholar] [CrossRef]
- World Health Organisation. COVID-19: Vulnerable and High Risk Groups. Available online: https://www.who.int/westernpacific/emergencies/covid-19/information/high-risk-groups (accessed on 8 May 2020).
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.F.; Guo, Q.H.; Ji, R.; Wang, H.J.; Wang, Y.P.; Zhou, Y.N. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef]
- Tsao, S.F.; Chen, H.; Tisseverasinghe, T.; Yang, Y.; Li, L.; Butt, Z.A. What social media told us in the time of COVID-19: A scoping review. Lancet Digit Health 2021, 3, e175–e194. [Google Scholar] [CrossRef]
- Liao, Q.; Yuan, J.; Dong, M.; Yang, L.; Fielding, R.; Lam, W.W.T. Public Engagement and Government Responsiveness in the Communications About COVID-19 During the Early Epidemic Stage in China: Infodemiology Study on Social Media Data. J. Med. Internet Res. 2020, 22, e18796. [Google Scholar] [CrossRef]
- Bao, Y.; Sun, Y.; Meng, S.; Shi, J.; Lu, L. 2019-nCoV epidemic: Address mental health care to empower society. Lancet 2020, 395, e37–e38. [Google Scholar] [CrossRef] [Green Version]
- Norman, C.D.; Skinner, H.A. eHealth Literacy: Essential Skills for Consumer Health in a Networked World. J. Med. Internet Res. 2006, 8, e9. [Google Scholar] [CrossRef]
- Diviani, N.; van den Putte, B.; Giani, S.; van Weert, J.C. Low health literacy and evaluation of online health information: A systematic review of the literature. J. Med. Internet Res. 2015, 17, e112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, Y.Y.; Cheng, H.Y.; Chan, H.Y.L.; Chien, W.T.; Wong, S.Y.S. COVID-19 pandemic, infodemic and the role of eHealth literacy. Int. J. Nurs. Stud. 2020, 108, 103644. [Google Scholar] [CrossRef]
- Do, B.N.; Tran, T.V.; Phan, D.T.; Nguyen, H.C.; Nguyen, T.T.P.; Nguyen, H.C.; Ha, T.H.; Dao, H.K.; Trinh, M.V.; Do, T.V.; et al. Health Literacy, eHealth Literacy, Adherence to Infection Prevention and Control Procedures, Lifestyle Changes, and Suspected COVID-19 Symptoms Among Health Care Workers During Lockdown: Online Survey. J. Med. Internet Res. 2020, 22, e22894. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T. Health literacy: Towards system level solutions. BMJ 2015, 350, h1026. [Google Scholar] [CrossRef] [Green Version]
- Gasmi, A.; Noor, S.; Tippairote, T.; Dadar, M.; Menzel, A.; Bjørklund, G. Individual risk management strategy and potential therapeutic options for the COVID-19 pandemic. Clin. Immunol. 2020, 215, 108409. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Liu, Y. Potential interventions for novel coronavirus in China: A systematic review. J. Med. Virol. 2020, 92, 479–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kakodkar, P.; Kaka, N.; Baig, M.N. A Comprehensive Literature Review on the Clinical Presentation, and Management of the Pandemic Coronavirus Disease 2019 (COVID-19). Cureus 2020, 12, e7560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morais, A.H.A.; Aquino, J.S.; da Silva-Maia, J.K.; Vale, S.H.L.; Maciel, B.L.L.; Passos, T.S. Nutritional status, diet and viral respiratory infections: Perspectives for severe acute respiratory syndrome coronavirus 2. Br. J. Nutr. 2020, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Jayedi, A.; Soltani, S.; Abdolshahi, A.; Shab-Bidar, S. Healthy and unhealthy dietary patterns and the risk of chronic disease: An umbrella review of meta-analyses of prospective cohort studies. Br. J. Nutr. 2020, 124, 1133–1144. [Google Scholar] [CrossRef]
- Butler, M.J.; Barrientos, R.M. The impact of nutrition on COVID-19 susceptibility and long-term consequences. Brain. Behav. Immun. 2020, 87, 53–54. [Google Scholar] [CrossRef] [PubMed]
- Pham, K.M.; Pham, L.V.; Phan, D.T.; Tran, T.V.; Nguyen, H.C.; Nguyen, M.H.; Nguyen, H.C.; Ha, T.H.; Dao, H.K.; Nguyen, P.B. Healthy Dietary Intake Behavior Potentially Modifies the Negative Effect of COVID-19 Lockdown on Depression: A Hospital and Health Center Survey. Front. Nutr. 2020, 7, 230. [Google Scholar] [CrossRef]
- Pike, K.M.; Dunne, P.E. The rise of eating disorders in Asia: A review. J. Eat. Disord. 2015, 3, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, T.T.; Hoang, M.V. Non-communicable diseases, food and nutrition in Vietnam from 1975 to 2015: The burden and national response. Asia Pac. J. Clin. Nutr. 2018, 27, 19–28. [Google Scholar] [CrossRef]
- Duong, T.V.; Pham, K.M.; Do, B.N.; Kim, G.B.; Dam, H.T.B.; Le, V.T.; Nguyen, T.T.P.; Nguyen, H.T.; Nguyen, T.T.; Le, T.T.; et al. Digital Healthy Diet Literacy and Self-Perceived Eating Behavior Change during COVID-19 Pandemic among Undergraduate Nursing and Medical Students: A Rapid Online Survey. Int. J. Environ. Res. Public Health 2020, 17, 7185. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Novel Coronavirus (2019-nCoV) Technical Guidance. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technicalguidance (accessed on 15 April 2020).
- Hays, R.D.; Morales, L.S. The RAND-36 measure of health-related quality of life. Ann. Med. 2001, 33, 350–357. [Google Scholar] [CrossRef]
- Tran, T.V.; Nguyen, H.C.; Pham, L.V.; Nguyen, M.H.; Nguyen, H.C.; Ha, T.H.; Phan, D.T.; Dao, H.K.; Nguyen, P.B.; Trinh, M.V.; et al. Impacts and interactions of COVID-19 response involvement, health-related behaviours, health literacy on anxiety, depression and health-related quality of life among healthcare workers: A cross-sectional study. BMJ Open 2020, 10, e041394. [Google Scholar] [CrossRef]
- Nguyen, H.C.; Nguyen, M.H.; Do, B.N.; Tran, C.Q.; Nguyen, T.T.P.; Pham, K.M.; Pham, L.V.; Tran, K.V.; Duong, T.T.; Tran, T.V.; et al. People with Suspected COVID-19 Symptoms Were More Likely Depressed and Had Lower Health-Related Quality of Life: The Potential Benefit of Health Literacy. J. Clin. Med. 2020, 9, 965. [Google Scholar] [CrossRef] [Green Version]
- Hays, R.D.; Sherbourne, C.D.; Mazel, R.M. The rand 36-item health survey 1.0. Health Econ. 1993, 2, 217–227. [Google Scholar] [CrossRef] [PubMed]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, H.T.; Do, B.N.; Pham, K.M.; Kim, G.B.; Dam, H.T.B.; Nguyen, T.T.; Nguyen, T.T.P.; Nguyen, Y.H.; Sørensen, K.; Pleasant, A.; et al. Fear of COVID-19 Scale-Associations of Its Scores with Health Literacy and Health-Related Behaviors among Medical Students. Int. J. Environ. Res. Public Health 2020, 17, 4164. [Google Scholar] [CrossRef] [PubMed]
- Duong, T.V.; Aringazina, A.; Kayupova, G.; Pham, T.V.; Pham, K.M.; Truong, T.Q.; Nguyen, K.T.; Oo, W.M.; Su, T.T.; Majid, H.A. Development and validation of a new short-form health literacy instrument (HLS-SF12) for the general public in six Asian countries. Health Lit. Res. Pract. 2019, 3, e91–e102. [Google Scholar] [CrossRef] [Green Version]
- Duong, T.V.; Nguyen, T.T.P.; Pham, K.M.; Nguyen, K.T.; Giap, M.H.; Tran, T.D.X.; Nguyen, C.X.; Yang, S.H.; Su, C.T. Validation of the Short-Form Health Literacy Questionnaire (HLS-SF12) and Its Determinants among People Living in Rural Areas in Vietnam. Int. J. Environ. Res. Public Health 2019, 16, 3346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, T.T.; Le, N.T.; Nguyen, M.H.; Pham, L.V.; Do, B.N.; Nguyen, H.C.; Nguyen, H.C.; Ha, T.H.; Dao, H.K.; Nguyen, P.B.; et al. Health Literacy and Preventive Behaviors Modify the Association between Pre-Existing Health Conditions and Suspected COVID-19 Symptoms: A Multi-Institutional Survey. Int. J. Environ. Res. Public Health 2020, 17, 8598. [Google Scholar] [CrossRef]
- Do, B.N.; Nguyen, P.A.; Pham, K.M.; Nguyen, H.C.; Nguyen, M.H.; Tran, C.Q.; Nguyen, T.T.P.; Tran, T.V.; Pham, L.V.; Tran, K.V.; et al. Determinants of Health Literacy and Its Associations With Health-Related Behaviors, Depression Among the Older People With and Without Suspected COVID-19 Symptoms: A Multi-Institutional Study. Front. Public Health 2020, 8, 581746. [Google Scholar] [CrossRef]
- BMJ Editorial Team. Overview of novel coronavirus (2019-nCoV). Available online: https://0-bestpractice-bmj-com.brum.beds.ac.uk/topics/en-gb/3000165 (accessed on 10 March 2020).
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- World Health Organisation. Coronavirus Disease (COVID-19): Advice for the Public. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 15 December 2020).
- Ping, W.; Zheng, J.; Niu, X.; Guo, C.; Zhang, J.; Yang, H.; Shi, Y. Evaluation of health-related quality of life using EQ-5D in China during the COVID-19 pandemic. PLoS ONE 2020, 15, e0234850. [Google Scholar] [CrossRef]
- Fitzpatrick, K.M.; Harris, C.; Drawve, G. Living in the midst of fear: Depressive symptomatology among US adults during the COVID-19 pandemic. Depress. Anxiety 2020, 37, 957–964. [Google Scholar] [CrossRef]
- Mamun, M.A.; Griffiths, M.D. First COVID-19 suicide case in Bangladesh due to fear of COVID-19 and xenophobia: Possible suicide prevention strategies. Asian J. Psychiatr. 2020, 51, 102073. [Google Scholar] [CrossRef]
- Ma, Y.F.; Li, W.; Deng, H.B.; Wang, L.; Wang, Y.; Wang, P.H.; Bo, H.X.; Cao, J.; Wang, Y.; Zhu, L.Y.; et al. Prevalence of depression and its association with quality of life in clinically stable patients with COVID-19. J. Affect. Disord. 2020, 275, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Górnicka, M.; Drywień, M.E.; Zielinska, M.A.; Hamułka, J. Dietary and Lifestyle Changes During COVID-19 and the Subsequent Lockdowns among Polish Adults: A Cross-Sectional Online Survey PLifeCOVID-19 Study. Nutrients 2020, 12, 2324. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Lin, X.; Chiwanda Kaminga, A.; Xu, H. Impact of the COVID-19 Epidemic on Lifestyle Behaviors and Their Association With Subjective Well-Being Among the General Population in Mainland China: Cross-Sectional Study. J. Med. Internet Res. 2020, 22, e21176. [Google Scholar] [CrossRef] [PubMed]
- Watson, R. Europeans with poor “health literacy” are heavy users of health services. BMJ 2011, 343, d7741. [Google Scholar] [CrossRef]
- Britt, R.K.; Collins, W.B.; Wilson, K.; Linnemeier, G.; Englebert, A.M. eHealth Literacy and Health Behaviors Affecting Modern College Students: A Pilot Study of Issues Identified by the American College Health Association. J. Med. Internet Res. 2017, 19, e392. [Google Scholar] [CrossRef]
- Ahmad, A.R.; Murad, H.R. The Impact of Social Media on Panic During the COVID-19 Pandemic in Iraqi Kurdistan: Online Questionnaire Study. J. Med. Internet Res. 2020, 22, e19556. [Google Scholar] [CrossRef]
- Shimizu, K. 2019-nCoV, fake news, and racism. Lancet 2020, 395, 685–686. [Google Scholar] [CrossRef]
- Sentell, T.; Vamos, S.; Okan, O. Interdisciplinary Perspectives on Health Literacy Research Around the World: More Important Than Ever in a Time of COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 3010. [Google Scholar] [CrossRef]
- ACP Decisions. Four Simple Strategies for Improving Your Patients’ Health Literacy. Available online: https://acpdecisions.org/four-simple-strategies-for-improving-your-patients-health-literacy/ (accessed on 15 March 2021).
- Poelman, M.P.; Dijkstra, S.C.; Sponselee, H.; Kamphuis, C.B.M.; Battjes-Fries, M.C.E.; Gillebaart, M.; Seidell, J.C. Towards the measurement of food literacy with respect to healthy eating: The development and validation of the self perceived food literacy scale among an adult sample in the Netherlands. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonaccio, M.; Di Castelnuovo, A.; Bonanni, A.; Costanzo, S.; De Lucia, F.; Pounis, G.; Zito, F.; Donati, M.B.; de Gaetano, G.; Iacoviello, L. Adherence to a Mediterranean diet is associated with a better health-related quality of life: A possible role of high dietary antioxidant content. BMJ Open 2013, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, F.; Cohen, S.A.; Lofgren, I.E.; Greene, G.W.; Delmonico, M.J.; Greaney, M.L. Relationship between Diet Quality, Physical Activity and Health-Related Quality of Life in Older Adults: Findings from 2007–2014 National Health and Nutrition Examination Survey. J. Nutr. Health Aging 2018, 22, 1072–1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.Y.; Zhuang, L.H.; Li, W.; Guo, H.W.; Zhang, J.H.; Zhao, Y.K.; Hu, J.W.; Gao, Q.Q.; Luo, S.; Ohinmaa, A.; et al. The influence of diet quality and dietary behavior on health-related quality of life in the general population of children and adolescents: A systematic review and meta-analysis. Qual. Life Res. 2019, 28, 1989–2015. [Google Scholar] [CrossRef] [PubMed]
- Milte, C.M.; Thorpe, M.G.; Crawford, D.; Ball, K.; McNaughton, S.A. Associations of diet quality with health-related quality of life in older Australian men and women. Exp. Gerontol. 2015, 64, 8–16. [Google Scholar] [CrossRef] [Green Version]
- McCullough, M.L.; Feskanich, D.; Stampfer, M.J.; Giovannucci, E.L.; Rimm, E.B.; Hu, F.B.; Spiegelman, D.; Hunter, D.J.; Colditz, G.A.; Willett, W.C. Diet quality and major chronic disease risk in men and women: Moving toward improved dietary guidance. Am. J. Clin. Nutr. 2002, 76, 1261–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulze, M.B.; Martínez-González, M.A.; Fung, T.T.; Lichtenstein, A.H.; Forouhi, N.G. Food based dietary patterns and chronic disease prevention. BMJ 2018, 361, k2396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molendijk, M.; Molero, P.; Ortuño Sánchez-Pedreño, F.; Van der Does, W.; Angel Martínez-González, M. Diet quality and depression risk: A systematic review and dose-response meta-analysis of prospective studies. J. Affect. Disord. 2018, 226, 346–354. [Google Scholar] [CrossRef] [Green Version]
- Vietnam Ministry of Health. Coronavirus Disease (COVID-19) Outbreak in Vietnam. Available online: https://ncov.moh.gov.vn/ (accessed on 7 June 2020).



{kind=link}
{kind=link}
| Geographic Location | Hospitals | Studied Participants |
|---|---|---|
| Northern area | ||
| Ha Noi city | ||
| 1. Military Hospital 103 | 501 | |
| 2. E Hospital | 183 | |
| 3. General Hospital of Agricultural | 300 | |
| Hai Phong city | ||
| 4. Hai Phong University of Medicine and Pharmacy Hospital | 490 | |
| 5. Kien An Hospital | 492 | |
| Quang Ninh province | ||
| 6. Bai Chay Hospital | 364 | |
| 7. Quang Ninh Obstetrics and Pediatrics Hospital | 280 | |
| 8. Quang Ninh General Hospital | 309 | |
| Bac Ninh city | ||
| 9. Bac Ninh Obstetrics and Pediatrics Hospital | 500 | |
| Central area | ||
| Da Nang city | ||
| 10. Da Nang Oncology Hospital | 421 | |
| Southern area | ||
| Can Tho city | ||
| 11. Can Tho University of Medicine and Pharmacy Hospital | 508 | |
| Total | 4348 |
| Variables | Total (N = 4348) | HRQoL | |
|---|---|---|---|
| n (%) | Mean (SD) | p * | |
| Age (years), mean (SD) | 42.8 (16.7) | ||
| Age groups | <0.001 | ||
| <60 | 3412(78.5) | 65.8 (17.6) | |
| ≥60 | 936 (21.5) | 53.8 (15.6) | |
| Gender | 0.454 | ||
| Women | 2694 (62.0) | 63.0 (18.1) | |
| Men | 1654 (38.0) | 63.5 (17.5) | |
| Marital status | <0.001 | ||
| Never married | 772 (17.8) | 69.7 (15.6) | |
| Ever married | 3560 (82.2) | 61.8 (18.1) | |
| Education attainment | <0.001 | ||
| Secondary school or below | 1007 (23.2) | 58.2 (18.3) | |
| High school | 1196 (27.5) | 61.1 (18.2) | |
| College/university or higher | 2139 (49.3) | 66.8 (16.7) | |
| Occupation | <0.001 | ||
| Unemployed | 474 (10.9) | 56.5 (19.5) | |
| Employed | 3874 (89.1) | 64.0 (17.5) | |
| Ability to pay for treatments | <0.001 | ||
| Very or fairly difficult | 2712 (62.5) | 60.9 (17.7) | |
| Very or fairly easy | 1626 (37.5) | 67.1 (17.5) | |
| Social status | <0.001 | ||
| Low | 921 (21.2) | 59.6 (20.6) | |
| Middle or high | 3419 (78.8) | 64.2 (16.9) | |
| BMI, kg/m2 | 0.156 | ||
| Normal weight (BMI < 25.0) | 3791 (87.4) | 63.3 (18.0) | |
| Overweight/obese (BMI ≥ 25.0) | 546 (12.6) | 62.2 (17.2) | |
| Suspected COVID-19 symptoms ** | <0.001 | ||
| No | 2595 (59.7) | 65.5 (17.2) | |
| Yes | 1753 (40.3) | 59.7 (18.3) | |
| Comorbidity | <0.001 | ||
| No | 3094 (71.2) | 64.6 (17.8) | |
| Yes | 1254 (28.8) | 59.6 (17.6) | |
| Smoking tobacco *** | 0.329 | ||
| Never, stopped, or smoke less | 3994 (91.9) | 63.1 (18.0) | |
| Unchanged or smoke more | 354 (8.1) | 64.1 (16.4) | |
| Drinking alcohol *** | 0.918 | ||
| Never, stopped, or drink less | 4015 (92.6) | 63.2 (18.1) | |
| Unchanged or drink more | 321 (7.4) | 63.3 (15.6) | |
| Physical activity *** | <0.001 | ||
| Never, stopped, or exercise less | 2515 (57.8) | 58.5 (17.5) | |
| Unchanged or exercise more | 1833 (42.2) | 69.7 (16.3) | |
| Healthy eating *** | <0.001 | ||
| Less healthy | 325 (7.5) | 55.6 (12.8) | |
| Unchanged or healthier | 4002 (92.5) | 63.8 (18.1) | |
| Health literacy, mean (SD) | 26.5 (10.5) | ||
| eHealth Literacy Scale, mean (SD) | 27.9 (6.9) | ||
| Digital healthy diet literacy, mean (SD) | 25.9 (12.2) | ||
| Fear of COVID-19 Scale, mean (SD) | 20.6 (5.4) |
| Variables | HRQoL | |||
|---|---|---|---|---|
| Model 1 ** | Model 2 *** | |||
| B (95% CI) | p | B (95% CI) | p | |
| Fear of COVID-19 Scale, 1-score increment * | −0.83 (−0.93, −0.74) | <0.001 | −0.78 (−0.87, −0.70) | <0.001 |
| Health literacy, 1-score increment * | 0.41 (0.36, 0.46) | <0.001 | 0.20 (0.15, 0.25) | <0.001 |
| eHealth Literacy Scale, 1-score increment * | 0.50 (0.42, 0.57) | <0.001 | 0.24 (0.17, 0.32) | <0.001 |
| Digital healthy diet literacy, 1-score increment * | 0.38 (0.33, 0.42) | <0.001 | 0.18 (0.14, 0.22) | <0.001 |
| Interactions | HRQoL | |||
|---|---|---|---|---|
| Model 1 * | Model 2 ** | |||
| B (95% CI) | p | B (95% CI) | p | |
| Interaction between FCoV-19S and HL | ||||
| FCoV-19S, 1-score increment | −1.16 (−1.39, −0.92) | <0.001 | −1.00 (−1.21, −0.78) | <0.001 |
| HL, 1-score increment | 0.22 (0.05, 0.38) | 0.008 | 0.11 (−0.05, 0.26) | 0.177 |
| FCoV-19S × HL | 0.01 (0.00, 0.02) | 0.017 | 0.01 (−0.01, 0.02) | 0.079 |
| Interaction between FCoV-19S and eHEALS | ||||
| FCoV-19S, 1-score increment | −1.51 (−1.86, −1.17) | <0.001 | −1.18 (−1.51, −0.85) | <0.001 |
| eHEALS, 1-score increment | 0.14 (−1.11, 0.38) | 0.273 | 0.09 (−0.14, 0.32) | 0.451 |
| FCoV-19S × eHEALS | 0.02 (0.01, 0.03) | <0.001 | 0.01 (0.01, 0.02) | 0.034 |
| Interaction between FCoV-19S and DDL | ||||
| FCoV-19S, 1-score increment | −1.12 (−1.33, −0.91) | <0.001 | −1.02 (−1.22, −0.82) | <0.001 |
| DDL, 1-score increment | 0.17 (0.02, 0.32) | 0.026 | 0.03 (−0.11, 0.17) | 0.652 |
| FCoV-19S × DDL | 0.01 (0.00, 0.02) | 0.003 | 0.01 (0.00, 0.02) | 0.016 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, M.H.; Pham, T.T.M.; Nguyen, K.T.; Nguyen, Y.H.; Tran, T.V.; Do, B.N.; Dao, H.K.; Nguyen, H.C.; Do, N.T.; Ha, T.H.; et al. Negative Impact of Fear of COVID-19 on Health-Related Quality of Life Was Modified by Health Literacy, eHealth Literacy, and Digital Healthy Diet Literacy: A Multi-Hospital Survey. Int. J. Environ. Res. Public Health 2021, 18, 4929. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094929
Nguyen MH, Pham TTM, Nguyen KT, Nguyen YH, Tran TV, Do BN, Dao HK, Nguyen HC, Do NT, Ha TH, et al. Negative Impact of Fear of COVID-19 on Health-Related Quality of Life Was Modified by Health Literacy, eHealth Literacy, and Digital Healthy Diet Literacy: A Multi-Hospital Survey. International Journal of Environmental Research and Public Health. 2021; 18(9):4929. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094929
Chicago/Turabian StyleNguyen, Minh H., Thu T. M. Pham, Kien T. Nguyen, Yen H. Nguyen, Tien V. Tran, Binh N. Do, Hung K. Dao, Huu C. Nguyen, Ngoc T. Do, Tung H. Ha, and et al. 2021. "Negative Impact of Fear of COVID-19 on Health-Related Quality of Life Was Modified by Health Literacy, eHealth Literacy, and Digital Healthy Diet Literacy: A Multi-Hospital Survey" International Journal of Environmental Research and Public Health 18, no. 9: 4929. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094929