
Influence of the Duration and Timing of Data Collection on Accelerometer-Measured Physical Activity, Sedentary Time and Associated Insulin Resistance

 ,
,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
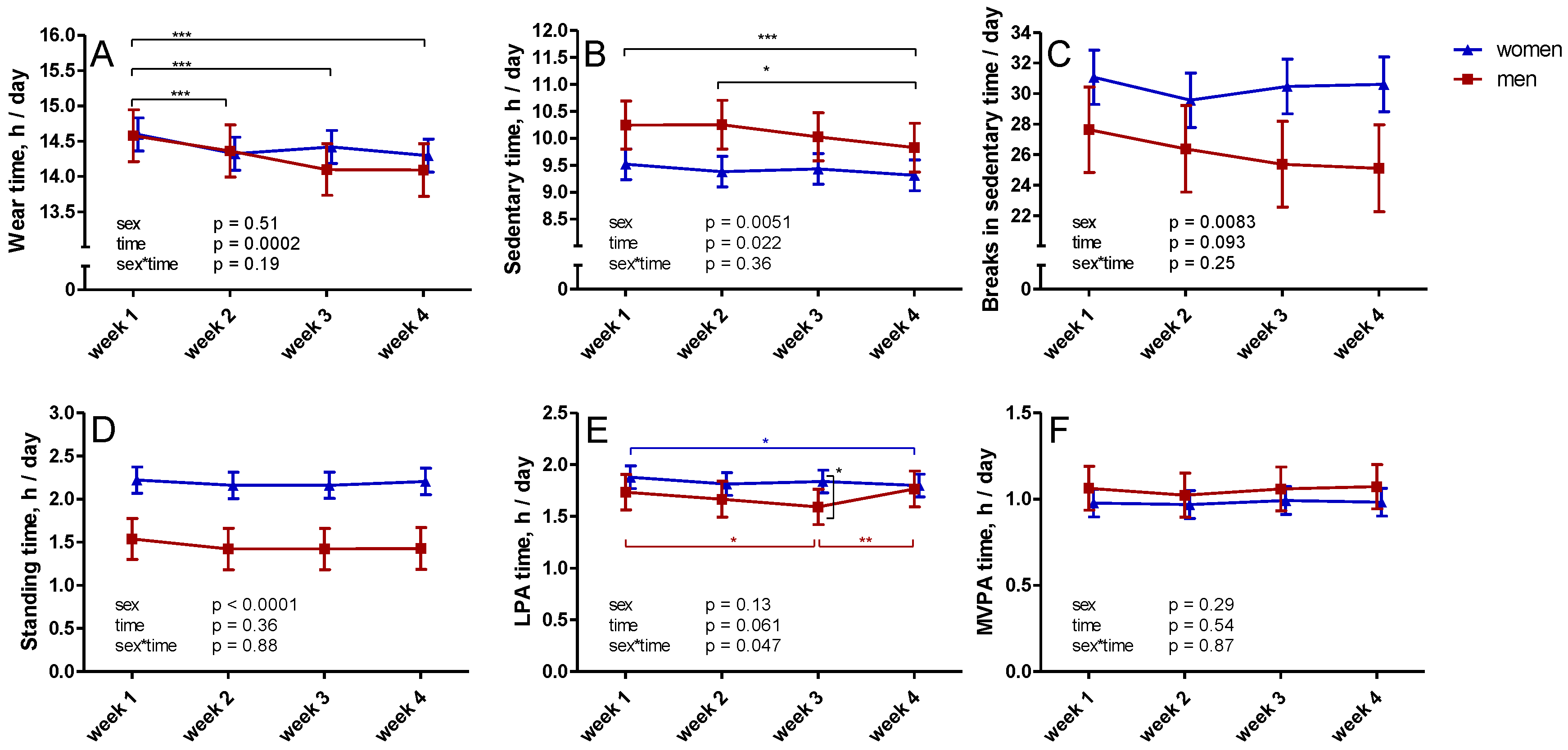
3.1. Changes in Measured SB and PA over Four Weeks
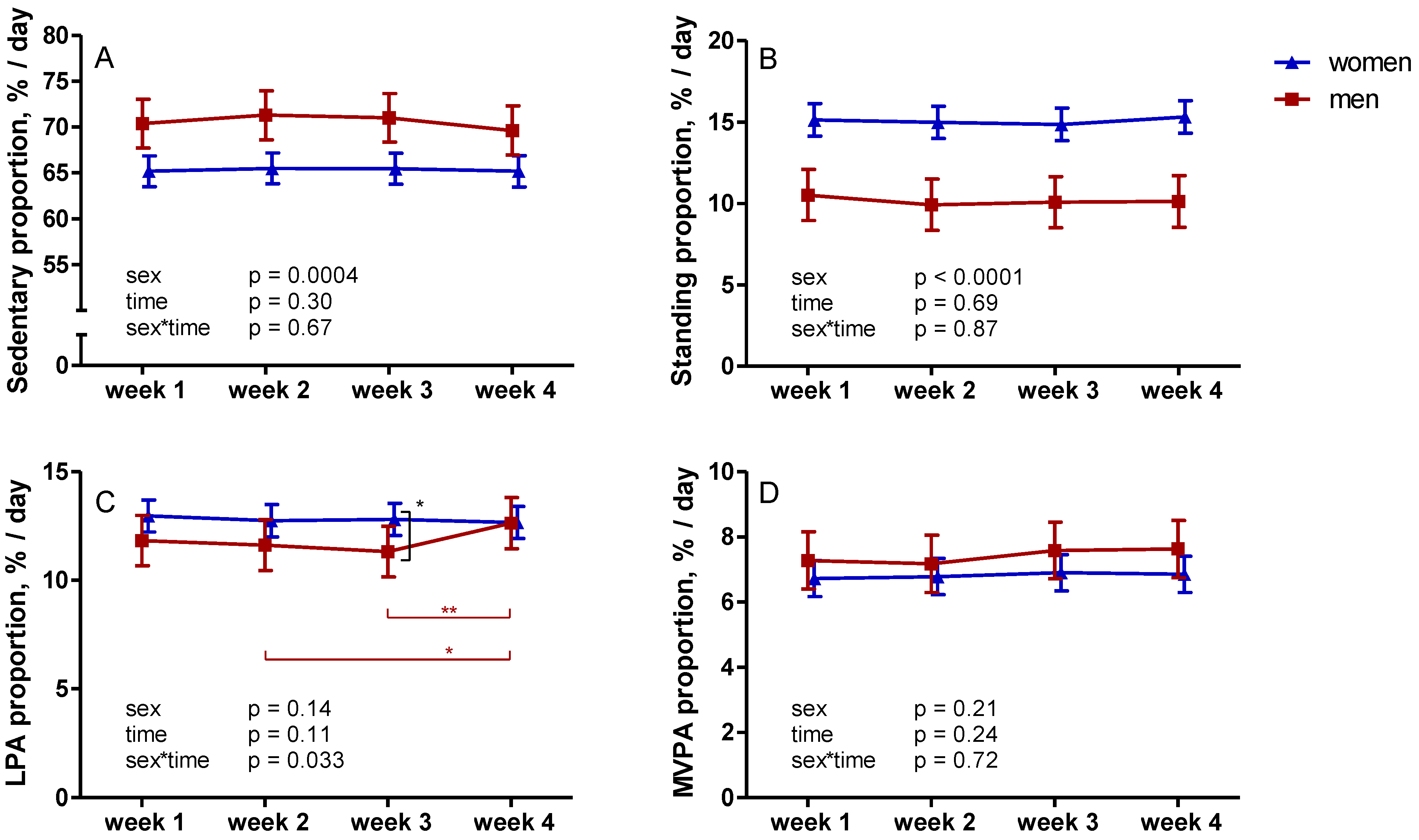
3.2. Proportions of Different Activity Categories
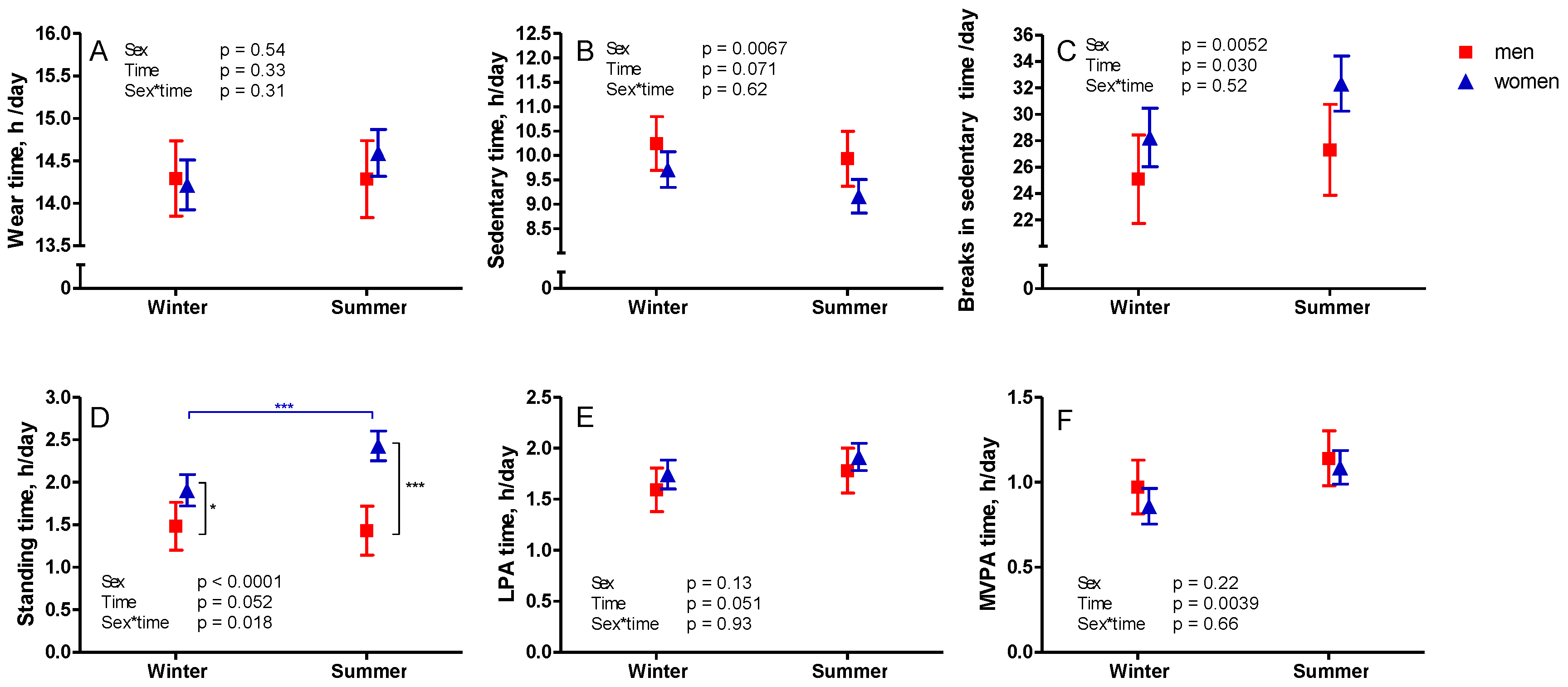
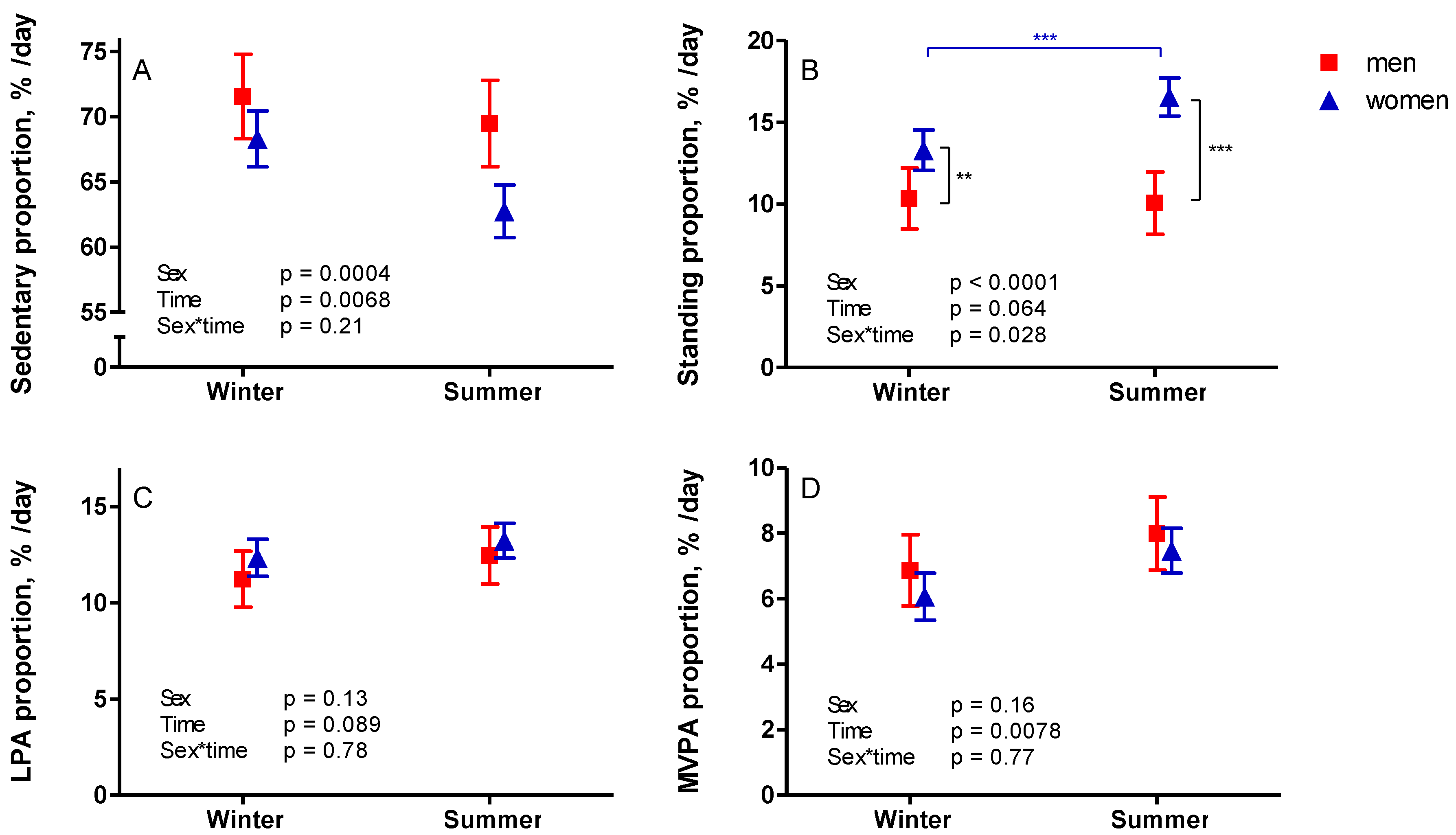
3.3. Seasonal Variation
3.4. Duration of Accelerometer Data Collection in Predicting Insulin Resistance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.A. Sedentary Time and Its Association with Risk for Disease Incidence, Mortality, and Hospitalization in Adults: A Systematic Review and Meta-analysis. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef]
- Ekelund, U.; Brown, W.J.; Steene-Johannessen, J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.E.; Lee, I.M. Do the associations of sedentary behaviour with cardiovascular disease mortality and cancer mortality differ by physical activity level? A systematic review and harmonised meta-analysis of data from 850 060 participants. Br. J. Sports Med. 2019, 53, 886–894. [Google Scholar] [CrossRef] [PubMed]
- Patterson, R.; McNamara, E.; Tainio, M.; de Sá, T.H.; Smith, A.D.; Sharp, S.J.; Edwards, P.; Woodcock, J.; Brage, S.; Wijndaele, K. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: A systematic review and dose response meta-analysis. Eur. J. Epidemiol. 2018, 33, 811–829. [Google Scholar] [CrossRef] [Green Version]
- Van der Berg, J.D.; Stehouwer, C.D.A.; Bosma, H.; van der Velde, J.H.P.M.; Willems, P.J.B.; Savelberg, H.H.C.M.; Schram, M.T.; Sep, S.J.S.; van der Kallen, C.J.H.; Henry, R.M.A.; et al. Associations of total amount and patterns of sedentary behaviour with type 2 diabetes and the metabolic syndrome: The Maastricht Study. Diabetologia 2016, 59, 709–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wijndaele, K.; Orrow, G.; Ekelund, U.; Sharp, S.J.; Brage, S.; Griffin, S.J.; Simmons, R.K. Increasing objectively measured sedentary time increases clustered cardiometabolic risk: A 6-year analysis of the ProActive study. Diabetologia 2014, 57, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Yates, T.; Edwardson, C.L.; Henson, J.; Zaccardi, F.; Khunti, K.; Davies, M.J. Prospectively Reallocating Sedentary Time: Associations with Cardiometabolic Health. Med. Sci. Sports Exerc. 2020, 52, 844–850. [Google Scholar] [CrossRef]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. BMJ 2019, 366, l4570. [Google Scholar] [CrossRef] [Green Version]
- Bergman, P.; Hagströmer, M. No one accelerometer-based physical activity data collection protocol can fit all research questions. BMC Med. Res. Methodol. 2020, 20, 141. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Ramirez Varela, A.; Bauman, A.E.; Ekelund, U.; Lee, I.M.; Heath, G.; Katzmarzyk, P.T.; Reis, R.; Pratt, M. Towards better evidence-informed global action: Lessons learnt from the Lancet series and recent developments in physical activity and public health. Br. J. Sports Med. 2020, 54, 462–468. [Google Scholar] [CrossRef] [Green Version]
- Sievänen, H.; Kujala, U.M. Accelerometry—Simple, but challenging. Scand. J. Med. Sci. Sports 2017, 27, 574–578. [Google Scholar] [CrossRef] [PubMed]
- Janssen, X.; Cliff, D.P. Issues Related to Measuring and Interpreting Objectively Measured Sedentary Behavior Data. Meas. Phys. Educ. Exerc. Sci. 2015, 19, 116–124. [Google Scholar] [CrossRef] [Green Version]
- Matthews, C.E.; Hagströmer, M.; Pober, D.M.; Bowles, H.R. Best practices for using physical activity monitors in population-based research. Med. Sci. Sports Exerc. 2012, 44, S68–S76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergman, P. The number of repeated observations needed to estimate the habitual physical activity of an individual to a given level of precision. PLoS ONE 2018, 13, e0192117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aadland, E.; Ylvisåker, E. Reliability of Objectively Measured Sedentary Time and Physical Activity in Adults. PLoS ONE 2015, 10, e0133296. [Google Scholar]
- Hart, T.L.; Swartz, A.M.; Cashin, S.E.; Strath, S.J. How many days of monitoring predict physical activity and sedentary behaviour in older adults? Int. J. Behav. Nutr. Phys. Act. 2011, 8, 62. [Google Scholar] [CrossRef] [Green Version]
- Kang, M.; Bassett, D.R.; Barreira, T.V.; Tudor-Locke, C.; Ainsworth, B.; Reis, J.P.; Strath, S.; Swartz, A. How many days are enough? A study of 365 days of pedometer monitoring. Res. Q.Exerc. Sport 2009, 80, 445–453. [Google Scholar] [CrossRef]
- Hróbjartsson, A.; Gøtzsche, P.C. Placebo interventions for all clinical conditions. Cochrane database Syst. Rev. 2010, 2010, CD003974. [Google Scholar] [CrossRef]
- Linde, K.; Fässler, M.; Meissner, K. Placebo interventions, placebo effects and clinical practice. Philos. Trans. R. Soc. B Biol. Sci. 2011, 366, 1905–1912. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Sjöros, T.; Vähä-Ypyä, H.; Laine, S.; Garthwaite, T.; Lahesmaa, M.; Laurila, S.M.; Latva-Rasku, A.; Savolainen, A.; Miikkulainen, A.; Löyttyniemi, E.; et al. Both sedentary time and physical activity are associated with cardiometabolic health in overweight adults in a 1 month accelerometer measurement. Sci. Rep. 2020, 10, 20578. [Google Scholar] [CrossRef]
- Vähä-Ypyä, H.; Vasankari, T.; Husu, P.; Mänttäri, A.; Vuorimaa, T.; Suni, J.; Sievänen, H. Validation of Cut-Points for Evaluating the Intensity of Physical Activity with Accelerometry-Based Mean Amplitude Deviation (MAD). PLoS ONE 2015, 10, e0134813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vähä-Ypyä, H.; Husu, P.; Suni, J.; Vasankari, T.; Sievänen, H. Reliable recognition of lying, sitting, and standing with a hip-worn accelerometer. Scand. J. Med. Sci. Sports 2018, 28, 1092–1102. [Google Scholar] [CrossRef] [Green Version]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Hagströmer, M.; Oja, P.; Sjöström, M. Physical Activity and Inactivity in an Adult Population Assessed by Accelerometry. Med. Sci. Sport. Exerc. 2007, 39, 1502–1508. [Google Scholar] [CrossRef]
- Herrmann, S.D.; Barreira, T.V.; Kang, M.; Ainsworth, B.E. Impact of accelerometer wear time on physical activity data: A NHANES semisimulation data approach. Br. J. Sports Med. 2014, 48, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Aadland, E.; Andersen, L.B.; Skrede, T.; Ekelund, U.; Anderssen, S.A.; Resaland, G.K. Reproducibility of objectively measured physical activity and sedentary time over two seasons in children; Comparing a day-by-day and a week-by-week approach. PLoS ONE 2017, 12, e0189304. [Google Scholar] [CrossRef]
- Aadland, E.; Nilsen, A.K.O.; Ylvisåker, E.; Johannessen, K.; Anderssen, S.A. Reproducibility of objectively measured physical activity: Reconsideration needed. J. Sports Sci. 2020, 38, 1132–1139. [Google Scholar] [CrossRef]
- Chevenne, D.; Letailleur, A.; Trivin, F.; Porquet, D. Effect of hemolysis on the concentration of insulin in serum determined by RIA and IRMA. Clin. Chem. 1998, 44, 354–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n, (% men) | 143 (29) |
|---|---|
| Median age, years (IQR) | 59 (9) |
| Body mass index, kg/m2 | 31.7 (4.0) |
| Waist circumference, cm | 109.5 (11.4) |
| Fasting plasma glucose, mmol/l | 5.8 (0.8) |
| Median fasting plasma insulin, mU/l (IQR) | 11 (8) |
| Median HOMA-IR (IQR) | 2.7 (2.2) |
| Antihypertensive medication, n (%) | 56 (39) |
| Cholesterol lowering medication, n (%) | 19 (13) |
| Duration, h/day (SD) | Measurement Duration, days (SD) | Estimate, B | p | |
|---|---|---|---|---|
| Sedentary time, h/day | ||||
| 1 week | 9.73 (1.47) | 6.7 (0.7) | 0.01 | 0.45 |
| 2 weeks | 9.68 (1.39) | 12.8 (1.8) | 0.01 | 0.34 |
| 3 weeks | 9.65 (1.36) | 19.1 (2.5) | 0.01 | 0.32 |
| 4 weeks | 9.61 (1.32) | 24.9 (3.5) | 0.02 | 0.24 |
| Standing time, h/day | ||||
| 1 week | 2.02 (0.86) | 6.7 (0.7) | −0.03 | 0.17 |
| 2 weeks | 1.98 (0.79) | 12.8 (1.8) | −0.03 | 0.21 |
| 3 weeks | 1.97 (0.76) | 19.1 (2.5) | −0.04 | 0.15 |
| 4 weeks | 1.97 (0.76) | 24.9 (3.5) | −0.03 | 0.23 |
| LPA time, h/day | ||||
| 1 week | 1.84 (0.59) | 6.7 (0.7) | −0.05 | 0.13 |
| 2 weeks | 1.80 (0.54) | 12.8 (1.8) | −0.06 | 0.073 |
| 3 weeks | 1.79 (0.52) | 19.1 (2.5) | −0.07 | 0.041 |
| 4 weeks | 1.79 (0.50) | 24.9 (3.5) | −0.07 | 0.042 |
| MVPA time, h/day | ||||
| 1 week | 1.01 (0.39) | 6.7 (0.7) | −0.12 | 0.017 |
| 2 weeks | 0.99 (0.38) | 12.8 (1.8) | −0.12 | 0.017 |
| 3 weeks | 1.00 (0.38) | 19.1 (2.5) | −0.13 | 0.010 |
| 4 weeks | 1.00 (0.38) | 24.9 (3.5) | −0.14 | 0.0065 |
| Mean %/day (SD) | Measurement Duration, days (SD) | Estimate, B | p | |
|---|---|---|---|---|
| Sedentary proportion, %/day | ||||
| 1 week | 66.6 (8.9) | 6.7 (0.7) | 0.42 | 0.055 |
| 2 weeks | 67.0 (8.6) | 12.8 (1.8) | 0.46 | 0.044 |
| 3 weeks | 67.0 (8.3) | 19.1 (2.5) | 0.52 | 0.026 |
| 4 weeks | 66.8 (8.1) | 24.9 (3.5) | 0.55 | 0.023 |
| Standing proportion, %/day | ||||
| 1 week | 13.8 (5.6) | 6.7 (0.7) | −0.40 | 0.27 |
| 2 weeks | 13.6 (5.3) | 12.8 (1.8) | −0.40 | 0.30 |
| 3 weeks | 13.6 (5.1) | 19.1 (2.5) | −0.48 | 0.24 |
| 4 weeks | 13.6 (5.0) | 24.9 (3.5) | −0.43 | 0.30 |
| LPA proportion, %/day | ||||
| 1 week | 12.7 (3.9) | 6.7 (0.7) | −0.64 | 0.18 |
| 2 weeks | 12.5 (3.6) | 12.8 (1.8) | −0.85 | 0.095 |
| 3 weeks | 12.5 (3.5) | 19.1 (2.5) | −1.00 | 0.060 |
| 4 weeks | 12.5 (3.4) | 24.9 (3.5) | −1.04 | 0.054 |
| MVPA proportion, %/day | ||||
| 1 week | 6.9 (2.6) | 6.7 (0.7) | −1.49 | 0.041 |
| 2 weeks | 6.9 (2.6) | 12.8 (1.8) | −1.57 | 0.033 |
| 3 weeks | 7.0 (2.6) | 19.1 (2.5) | −1.68 | 0.023 |
| 4 weeks | 7.0 (2.6) | 24.9 (3.5) | −1.87 | 0.012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sjöros, T.; Vähä-Ypyä, H.; Laine, S.; Garthwaite, T.; Löyttyniemi, E.; Sievänen, H.; Kalliokoski, K.K.; Knuuti, J.; Vasankari, T.; Heinonen, I.H.A. Influence of the Duration and Timing of Data Collection on Accelerometer-Measured Physical Activity, Sedentary Time and Associated Insulin Resistance. Int. J. Environ. Res. Public Health 2021, 18, 4950. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094950
Sjöros T, Vähä-Ypyä H, Laine S, Garthwaite T, Löyttyniemi E, Sievänen H, Kalliokoski KK, Knuuti J, Vasankari T, Heinonen IHA. Influence of the Duration and Timing of Data Collection on Accelerometer-Measured Physical Activity, Sedentary Time and Associated Insulin Resistance. International Journal of Environmental Research and Public Health. 2021; 18(9):4950. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094950
Chicago/Turabian StyleSjöros, Tanja, Henri Vähä-Ypyä, Saara Laine, Taru Garthwaite, Eliisa Löyttyniemi, Harri Sievänen, Kari K. Kalliokoski, Juhani Knuuti, Tommi Vasankari, and Ilkka H. A. Heinonen. 2021. "Influence of the Duration and Timing of Data Collection on Accelerometer-Measured Physical Activity, Sedentary Time and Associated Insulin Resistance" International Journal of Environmental Research and Public Health 18, no. 9: 4950. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094950