
Trait and State: Interoceptive Accuracy during Anticipation of Public Speaking in Junior Secondary Shy Students from an Eastern Province of China



Abstract
:1. Introduction
1.1. Shyness
1.2. Shyness and Interoceptive Accuracy
1.3. Interoception in Shy Adolescents
1.4. Study Purpose
- Will the shy students exhibit higher IAc than non-shy participants?
- Will IAc in the anticipation condition be higher than that in the baseline condition?
- Will the shy group exhibit higher IAc gain than the non-shy group from baseline to anticipation condition?
2. Materials and Methods
2.1. Participants
2.2. Measure
Self-Reported Measures
2.3. Interoceptive Accuracy
2.4. Procedure
2.5. Hypotheses and Data Analysis
3. Results
3.1. Check on Manipulation
3.2. Interoceptive Accuracy: The State and Trait Variable
4. Discussion
4.1. Speech Anticipation Enhances IAc
4.2. Shy Adolescents Have Better Heartbeat Perception
4.3. Limitation and Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B
Appendix C

References
- Henderson, L.; Zimbardo, P. Shyness. In Encyclopedia of Mental Health; Academic Press: San Diego, CA, USA, 1998. [Google Scholar]
- Coplan, R.J.; Findlay, L.C.; Nelson, L.J. Characteristics of preschoolers with lower perceived competence. J. Abnorm. Child. Psychol. 2004, 32, 399–408. [Google Scholar] [CrossRef]
- Henderson, L.; Zimbardo, P.; Carducci, B. Shyness. In The Corsini Encyclopedia of Psychology, 4th ed.; John Wiley and Sons: Hoboken, NJ, USA, 2010. [Google Scholar]
- Rubin, K.H.; Coplan, R.J.; Bowker, J.C. Social withdrawal in childhood. Annu. Rev. Psychol. 2009, 60, 141–171. [Google Scholar] [CrossRef] [Green Version]
- Chang, L. Variable Effects of children’s aggression, social withdrawal, and prosocial leadership as functions of teacher beliefs and behaviors. Child. Dev. 2003, 74, 535–548. [Google Scholar] [CrossRef] [PubMed]
- Cheah, C.S.L.; Rubin, K.H. European American and Mainland Chinese mothers’ responses to aggression and social withdrawal in preschoolers. Int. J. Behav. Dev. 2004, 28, 83–94. [Google Scholar] [CrossRef]
- Chen, X.; Cen, G.; Li, D.; He, Y. Social functioning and adjustment in Chinese children: The Imprint of Historical Time. Child. Dev. 2005, 76, 182–195. [Google Scholar] [CrossRef]
- Xu, Y.; Farver, J.A.M.; Yang, Y.; Zeng, Q. Chinese children’s conceptions of shyness: A prototype approach. Merrill Palmer Q. 2008, 54, 515–544. [Google Scholar] [CrossRef]
- Xu, Y.; Farver, J.A.M.; Yang, Y.; Zeng, Q. Three types of shyness in Chinese children and the relation to effortful control. J. Abnorm. Soc. Psychol. 2009, 97, 1061–1073. [Google Scholar] [CrossRef]
- Craig, A.D. How do you feel—Now? The anterior insula and human awareness. Nat. Rev. Neurosci. 2009, 10, 59–70. [Google Scholar] [CrossRef]
- Tsakiris, M.; Critchley, H. Interoception beyond homeostasis: Affect, cognition and mental health. Philos. Trans. R. Soc. B 2016, 371, 20160002. [Google Scholar] [CrossRef] [Green Version]
- Garfinkel, S.N.; Seth, A.K.; Barrett, A.B.; Suzuki, K.; Critchley, H.D. Knowing your own heart: Distinguishing interoceptive accuracy from interoceptive awareness. Biol. Psychol. 2015, 104, 65–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damasio, A.R. Self Comes to Mind: Constructing the Conscious Brain; Heinemann: London, UK, 2010. [Google Scholar]
- Wells, A.; Papageorgiou, C. Social phobic interoception: Effects of bodily information on anxiety, beliefs and self-processing. Behav. Res. 2001, 39, 1–11. [Google Scholar] [CrossRef]
- Gerlach, A.L.; Mourlane, D.; Rist, F. Public and private heart rate feedback in social phobia: A manipulation of anxiety visibility. Cogn. Behav. 2004, 33, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Werner, N.S.; Kerschreiter, R.; Kindermann, N.K.; Duschek, S. Interoceptive awareness as a moderator of affective responses to social exclusion. J. Psychophysiol. 2013, 27, 39–50. [Google Scholar] [CrossRef]
- Dunn, B.D.; Dalgleish, T.; Ogilvie, A.D.; Lawrence, A.D. Heartbeat perception in depression. Behav. Res. 2007, 45, 1921–1930. [Google Scholar] [CrossRef] [PubMed]
- Domschke, K.; Stevens, S.; Pfleiderer, B.; Gerlach, A.L. Interoceptive sensitivity in anxiety and anxiety disorders: An overview and integration of neurobiological findings. Clin. Psychol. Rev. 2010, 30, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Stevens, S.; Gerlach, A.L.; Cludius, B.; Silkens, A.; Craske, M.G.; Hermann, C. Heartbeat perception in social anxiety before and during speech anticipation. Behav. Res. 2011, 49, 138–143. [Google Scholar] [CrossRef]
- Maister, L.; Hodossy, L.; Tsakiris, M. You fill my heart: Looking at one’s partner increases interoceptive accuracy. Psychol. Conscious. 2017, 4, 248–257. [Google Scholar] [CrossRef]
- Ainley, V.; Maister, L.; Brokfeld, J.; Farmer, H.; Tsakiris, M. More of myself: Manipulating interoceptive awareness by heightened attention to bodily and narrative aspects of the self. Conscious. Cogn. 2013, 22, 1–1238. [Google Scholar] [CrossRef]
- Ainley, V.; Tajadura-Jiménez, A.; Fotopoulou, A.; Tsakiris, M. Looking into myself: Changes in interoceptive sensitivity during mirror self-observation. Psychophysiology 2012, 49, 1504–1508. [Google Scholar] [CrossRef] [Green Version]
- Durlik, C.; Brown, G.; Tsakiris, M. Enhanced interoceptive awareness during anticipation of public speaking is associated with fear of negative evaluation. Cogn. Emot. 2014, 28, 530–540. [Google Scholar] [CrossRef]
- Durlik, C.; Tsakiris, M. Decreased interoceptive accuracy following social exclusion. Int. J. Psychophysiol. 2015, 96, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Durlik, C.; Cardini, F.; Tsakiris, M. Being watched: The effect of social self-focus on interoceptive and exteroceptive somatosensory perception. Conscious. Cogn. 2014, 25. [Google Scholar] [CrossRef] [Green Version]
- Steinberg, L. Cognitive and affective development in adolescence. Trends Cogn. Sci. 2005, 9, 69–74. [Google Scholar] [CrossRef]
- Hazel, N.A.; Oppenheimer, C.W.; Technow, J.R.; Young, J.F.; Hankin, B.L. Parent relationship quality buffers against the effect of peer stressors on depressive symptoms from middle childhood to adolescence. Dev. Psychol. 2014, 50, 2115. [Google Scholar] [CrossRef] [Green Version]
- McLaughlin, K.A.; Hatzenbuehler, M.L.; Mennin, D.S.; Nolen-Hoeksema, S. Emotion dysregulation and adolescent psychopathology: A prospective study. Behav. Res. 2011, 49, 544–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paus, T.; Keshavan, M.; Giedd, J.N. Why do many psychiatric disorders emerge during adolescence? Nat. Rev. Neurosci. 2008, 9, 947–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reardon, L.E.; Leen-Feldner, E.W.; Hayward, C. A critical review of the empirical literature on the relation between anxiety and puberty. Clin. Psychol. Rev. 2009, 29, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Li, D.; Zucker, N.L.; Kragel, P.A.; Covington, V.E.; LaBar, K.S. Adolescent development of insula-dependent interoceptive regulation. Dev. Sci. 2017, 20, e12438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berk, L.; Stewart, J.L.; May, A.C.; Wiers, R.W.; Davenport, P.W.; Paulus, M.P.; Tapert, S.F. Under pressure: Adolescent substance users show exaggerated neural processing of aversive interoceptive stimuli. Addiction 2015, 110, 2025–2036. [Google Scholar] [CrossRef] [Green Version]
- Murphy, J.; Brewer, R.; Catmur, C.; Bird, G. Interoception and psychopathology: A developmental neuroscience perspective. Dev. Cogn. Neurosci. 2017, 23, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Cheek, J.M.; Carpentieri, A.M.; Smith, T.G.; Rierdan, J.; Koff, E. Adolescent shyness. In Shyness; Springer: Boston, MA, USA, 1986; pp. 105–115. [Google Scholar]
- Zimbardo, P.G. Shyness: What It Is, What to Do About It; Perseus: Reading, MA, USA, 1977. [Google Scholar]
- Tian, L.; Jiang, S.; Huebner, E.S. The big two personality traits and adolescents’ complete mental health: The mediation role of perceived school stress. Sch. Psychol. Q. 2019, 34, 32. [Google Scholar] [CrossRef]
- Weeks, M.; Ooi, L.L.; Coplan, R.J. Cognitive biases and the link between shyness and social anxiety in early adolescence. J. Early Adolesc. 2015, 36, 1095–1117. [Google Scholar] [CrossRef]
- Wang, X.; Wang, X.L.; Ma, H. (Eds.) Handbook of Mental Health Assessment Scales; Journal of Mental Health Press: Beijing, China, 1999; pp. 238–241, 246–248. [Google Scholar]
- Schandry, R. Heart beat perception and emotional experience. Psychophysiology 1981, 18, 483–488. [Google Scholar] [CrossRef]
- Dunn, B.D.; Galton, H.C.; Morgan, R.; Evans, D.; Oliver, C.; Meyer, M.; Dalgleish, T. Listening to your heart: How interoception shapes emotion experience and intuitive decision making. Psychol Sci. 2010, 21, 1835–1844. [Google Scholar] [CrossRef] [Green Version]
- Van der Does, W.A.J.; Antony, M.M.; Ehlers, A.; Barsky, A.J. Heartbeat perception in panic disorder: A reanalysis. Behav. Res. 2000, 38, 47–62. [Google Scholar] [CrossRef]
- Harmat, L.; Örjan de Manzano, T.T.; Högman, L.; Fischer, H.; Ullén, F. Physiological correlates of the flow experience during computer game playing. Int. J. Psychophysiol. 2015, 97, 1–7. [Google Scholar] [CrossRef]
- Poole, K.L.; Lieshout, R.J.V.; Schmidt, L.A. Exploring relations between shyness and social anxiety disorder: The role of sociability. Pers. Individ. Differ. 2017, 110, 55–59. [Google Scholar] [CrossRef]
- Moscovitch, D.A.; Suvak, M.K.; Hofmann, S.G. Emotional response patterns during social threat in individuals with generalized social anxiety disorder and non-anxious controls. J. Anxiety Disord. 2010, 24, 785–791. [Google Scholar] [CrossRef]
- Antony, M.M.; Brown, T.A.; Craske, M.G.; Barlow, D.H.; Mitchell, W.B.; Meadows, E.A. Accuracy of heartbeat perception in panic disorder, social phobia, and non-anxious subjects. J. Anxiety Disord. 1995, 9, 355–371. [Google Scholar] [CrossRef]
- Wild, J.; Clark, D.M.; Ehlers, A.; McManus, F. Perception of arousal in social anxiety: Effects of false feedback during a social interaction. J. Behav. Ther. Exp. Psychiatry 2008, 39, 102–116. [Google Scholar] [CrossRef] [Green Version]
- Füstös, J.; Gramann, K.; Herbert, B.M.; Pollatos, O. On the embodiment of emotion regulation: Interoceptive awareness facilitates reappraisal. Soc. Cogn. Affect Neurosci. 2012, 8, 911–917. [Google Scholar] [CrossRef] [Green Version]
- Grynberg, D.; Pollatos, O. Perceiving one’s body shapes empathy. Physiol. Behav. 2015, 140, 54–60. [Google Scholar] [CrossRef]
- Weiss, S.; Sack, M.; Henningsen, P.; Pollatos, O. On the interaction of self-regulation, interoception and pain perception. Psychopathology 2014, 47, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Fischer, D.; Berberich, G.; Zaudig, M.; Krauseneck, T.; Weiss, S.; Pollatos, O. Interoceptive processes in anorexia nervosa in the time course of cognitive-behavioral therapy: A pilot study. Front. Psychiatry 2016, 7, 199. [Google Scholar] [CrossRef] [Green Version]
- Paulus, M.P.; Stein, M.B. Interoception in anxiety and depression. Brain Struct. Funct. 2010, 214, 451–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paulus, M.P.; Stein, M.B. An insular view of anxiety. Biol. Psychiatry 2006, 60, 383–387. [Google Scholar] [CrossRef]
- Pollatos, O.; Traut-Mattausch, T.; Schroeder, H.; Schandry, R. Interoceptive awareness mediates the relationship between anxiety and the in-tensity of unpleasant feelings. J. Anxiety Disord. 2007, 21, 931–943. [Google Scholar] [CrossRef] [PubMed]
- Erle, T.M.; Mitschke, V.; Schultchen, D. Did my heart just leap or sink? The role of personality for the relation between cardiac in-teroception and well-being. Pers. Individ. 2021, 170, 110493. [Google Scholar] [CrossRef]
- Herbert, B.M.; Pollatos, O. The body in the mind: On the relationship between interoception and embodiment. Top. Cogn. Sci. 2012, 4, 692–704. [Google Scholar] [CrossRef]
- Ring, C.; Brener, J. Heartbeat counting is unrelated to heartbeat detection: A comparison of methods to quantify interoception. Psychophysiology 2018, 55, e13084. [Google Scholar] [CrossRef] [Green Version]
- Zamariola, G.; Maurage, P.; Luminet, O.; Corneille, O. Interoceptive accuracy scores from the heartbeat counting task are problematic: Evidence from simple bivariate correlations. Biol. Psychol. 2018, 137, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Zimprich, D.; Nusser, L.; Pollatos, O. Are interoceptive accuracy scores from the heartbeat counting task problematic? A comment on Zamariola et al.(2018). Biol. Psychol. 2020, 152, 107868. [Google Scholar] [CrossRef] [PubMed]
- Ferentzi, E.; Horváth, Á.; Köteles, F. Do body-related sensations make feel us better? Subjective well-being is associated only with the subjective aspect of interoception. Psychophysiology 2019, 56, e13319. [Google Scholar] [CrossRef] [PubMed]
- Bögels, S.M. Task concentration training versus applied relaxation, in combination with cognitive therapy, for social phobia patients with fear of blushing, trembling, and sweating. Behav. Res. Ther. 2006, 44, 1199–1210. [Google Scholar] [CrossRef]
- Clark, D.M.; Ehlers, A.; Hackmann, A.; McManus, F.; Fennell, M.; Grey, N.; Waddington, L.; Wild, J. Cognitive therapy versus exposure and applied relaxation in social phobia: A randomized controlled trial. J. Consult. Clin. Psychol. 2006, 74, 568–578. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Non-Shy (n = 31) | Shy (n = 30) | t | |
|---|---|---|---|
| Girl | 16 | 16 | |
| Boy | 15 | 14 | |
| Age | 13.16 (0.86) | 13.03 (0.67) | 0.65 |
| Body mass index | 18.98 (3.32) | 20.10 (2.59) | −1.48 |
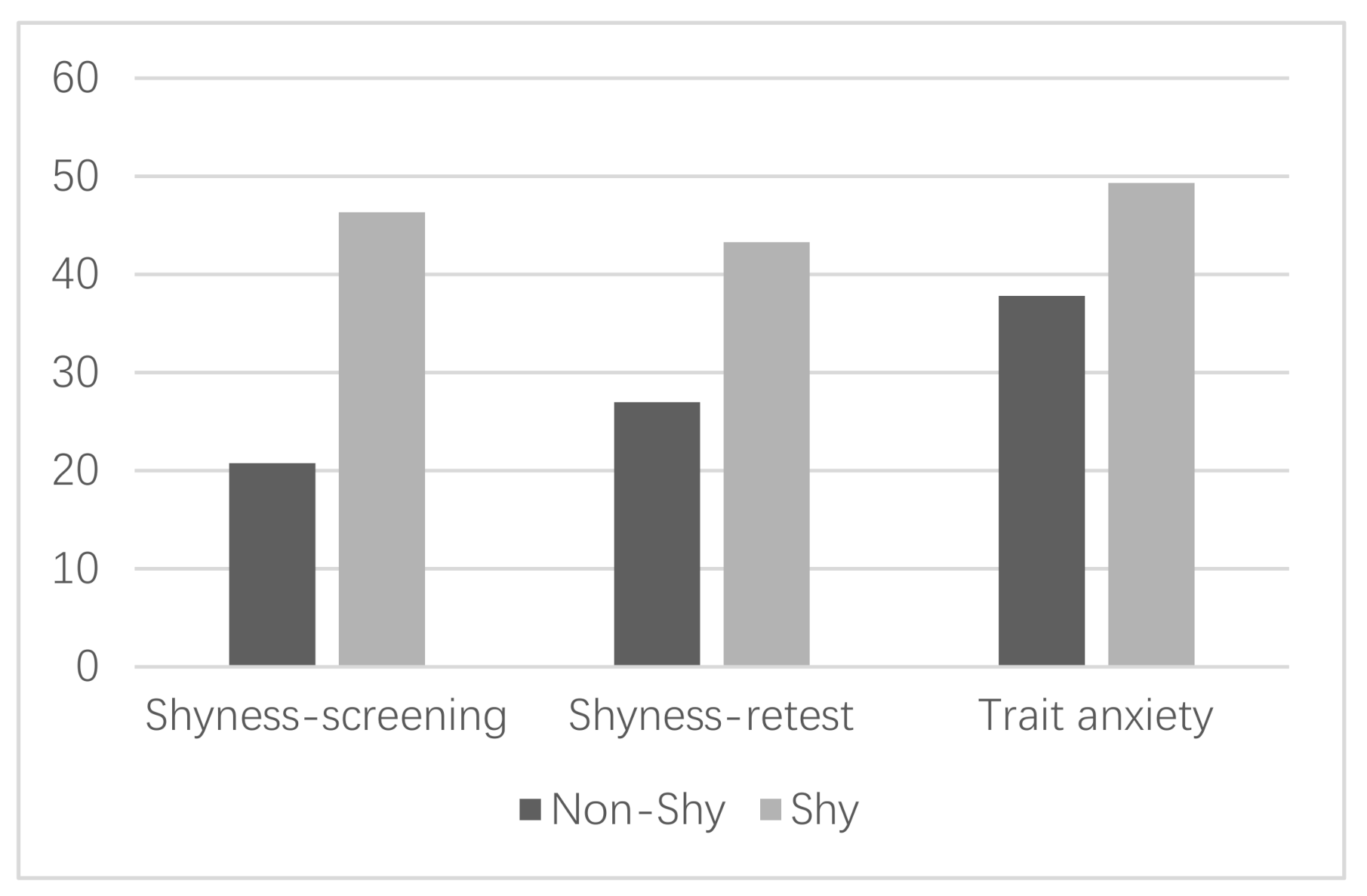
| Shyness-screening | 20.75 (1.52) | 46.33 (2.28) | −51.72 *** |
| Trait anxiety | 37.81 (6.37) | 49.32 (7.17) | −6.64 *** |
| Shyness-retest | 26.97 (6.09) | 43.30 (6.57) | −10.08 *** |
| Baseline | Anticipation | IAc Gain | |||||
|---|---|---|---|---|---|---|---|
| Anxiety Mood (VAS) | Heart Rate (bpm) | IAc | Anxiety Mood (VAS) | Heart Rate (bpm) | IAc | ||
| Non-shy n = 31 | 11.90 (3.46) | 86.03(12.33) | 0.29 (0.26) | 14.87 (4.64) | 92.98 (12.97) | 0.37 (0.29) | 0.08 (0.19) |
| Shy n = 30 | 15.97 (5.53) | 92.68(12.10) | 0.55 (0.16) | 19.47 (7.00) | 99.62 (11.14) | 0.60 (0.21) | 0.05 (0.17) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, J.; Li, H.; Wu, Y. Trait and State: Interoceptive Accuracy during Anticipation of Public Speaking in Junior Secondary Shy Students from an Eastern Province of China. Int. J. Environ. Res. Public Health 2021, 18, 4951. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094951
Wu J, Li H, Wu Y. Trait and State: Interoceptive Accuracy during Anticipation of Public Speaking in Junior Secondary Shy Students from an Eastern Province of China. International Journal of Environmental Research and Public Health. 2021; 18(9):4951. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094951
Chicago/Turabian StyleWu, Jianfen, Hui Li, and Yunpeng Wu. 2021. "Trait and State: Interoceptive Accuracy during Anticipation of Public Speaking in Junior Secondary Shy Students from an Eastern Province of China" International Journal of Environmental Research and Public Health 18, no. 9: 4951. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094951