
Progression of Metabolic Syndrome Components along with Depression Symptoms and High Sensitivity C-Reactive Protein: The Bogalusa Heart Study

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethical Procedures
2.3. Eligibility Criteria
2.4. General Measurements
2.5. Depression Symptoms (DS)
2.6. Laboratory Measurements
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Predictors of Metabolic Syndrome by Race
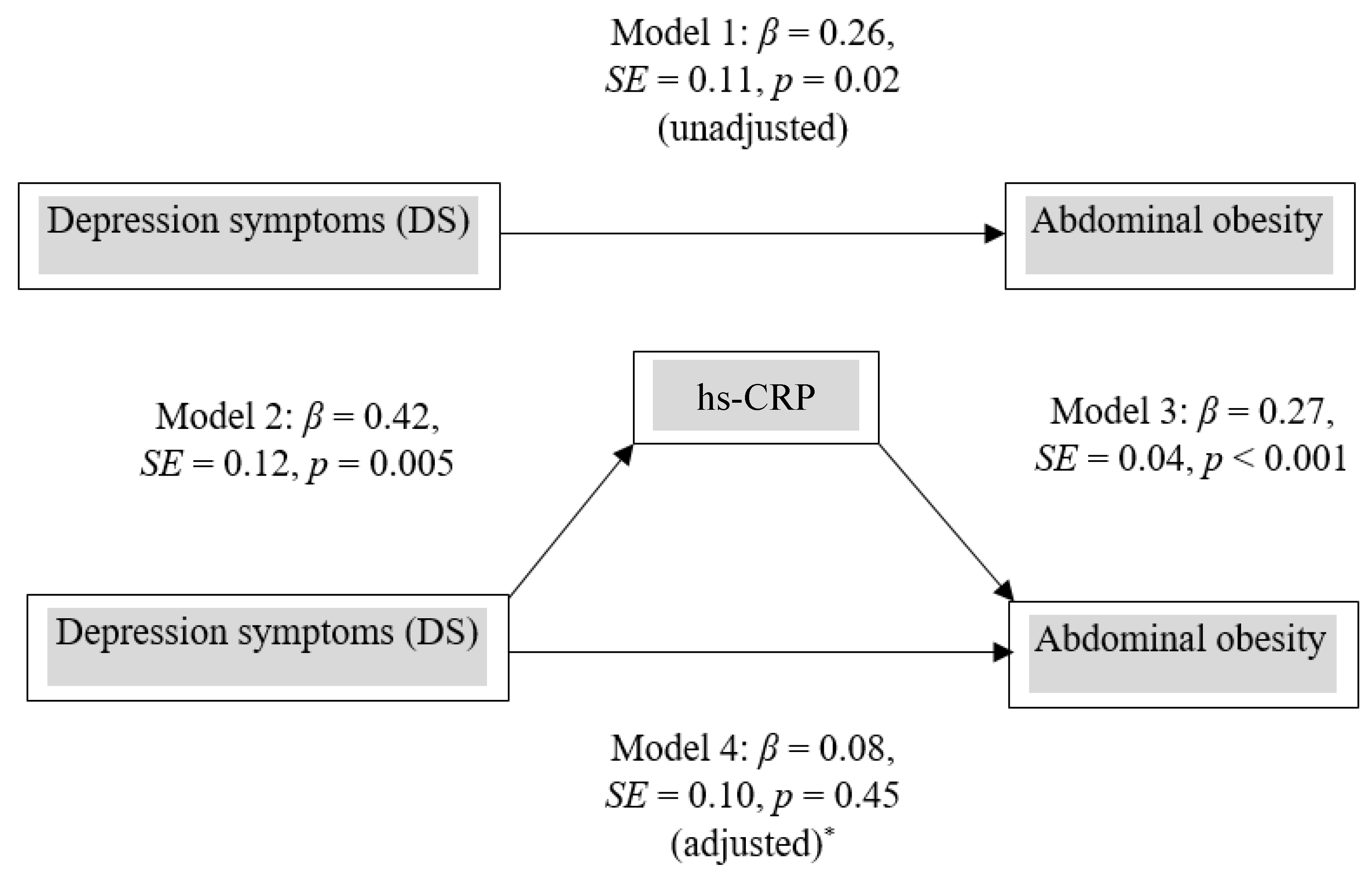
3.3. Mediator Role of hs-CRP on Abdominal Obesity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grundy, S.M. Metabolic Syndrome Pandemic. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 629–636. [Google Scholar] [CrossRef] [Green Version]
- Kassi, E.; Pervanidou, P.; Kaltsas, G.; Chrousos, G. Metabolic syndrome: Definitions and controversies. BMC Med. 2011, 9, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleeman, J.I.; Grundy, S.M.; Becker, D.; Clark, L. Expert panel on detection, evaluation and treatment of high blood cholesterol in adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP III). JAMA 2001, 285, 2486–2497. [Google Scholar]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, E.S.; Li, C.; Sattar, N. Metabolic Syndrome and Incident Diabetes: Current state of the evidence. Diabetes Care 2008, 31, 1898–1904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguilar, M.; Bhuket, T.; Torres, S.; Liu, B.; Wong, R.J. Prevalence of the Metabolic Syndrome in the United States, 2003–2012. JAMA 2015, 313, 1973–1974. [Google Scholar] [CrossRef] [PubMed]
- Musani, S.K.; Martin, L.J.; Woo, J.G.; Olivier, M.; Gurka, M.J.; DeBoer, M.D. Heritability of the Severity of the Metabolic Syndrome in Whites and Blacks in 3 Large Cohorts. Circ. Cardiovasc. Genet. 2017, 10, 001621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.; Srinivasan, S.R.; Li, S.; Xu, J.; Berenson, G.S. Clustering of Long-term Trends in Metabolic Syndrome Variables from Childhood to Adulthood in Blacks and Whites: The Bogalusa Heart Study. Am. J. Epidemiol. 2007, 166, 527–533. [Google Scholar] [CrossRef] [Green Version]
- Stroescu, R.F.; Mărginean, O.; Bizerea, T.; Gafencu, M.; Voicu, A.; Doroș, G. Adiponectin, leptin and high sensitivity C-reactive protein values in obese children–important markers for metabolic syndrome? J. Pediatr. Endocrinol. Metab. 2019, 32, 27–31. [Google Scholar] [CrossRef]
- Voils, S.A.; Cooper-DeHoff, R.M. Association between high sensitivity C-reactive protein and metabolic syndrome in subjects completing the National Health and Nutrition Examination Survey (NHANES) 2009–10. Diabetes Metab. Syndr. Clin. Res. Rev. 2014, 8, 88–90. [Google Scholar] [CrossRef]
- Hirschfeld, R.M.A. The Epidemiology of Depression and the Evolution of Treatment. J. Clin. Psychiatry 2012, 73, 5–9. [Google Scholar] [CrossRef]
- Cohen, B.E.; Edmondson, D.; Kronish, I.M. State of the Art Review: Depression, Stress, Anxiety, and Cardiovascular Disease. Am. J. Hypertens. 2015, 28, 1295–1302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joseph, J.J.; Golden, S.H. Cortisol dysregulation: The bidirectional link between stress, depression, and type 2 diabetes mellitus. Ann. N. Y. Acad. Sci. 2017, 1391, 20–34. [Google Scholar] [CrossRef]
- Lamers, F.; Vogelzangs, N.; Merikangas, K.R.; De Jonge, P.; Beekman, A.T.F.; Penninx, B.W.J.H. Evidence for a differential role of HPA-axis function, inflammation and metabolic syndrome in melancholic versus atypical depression. Mol. Psychiatry 2012, 18, 692–699. [Google Scholar] [CrossRef] [Green Version]
- Rethorst, C.D.; Bernstein, I.; Trivedi, M.H. Inflammation, obesity, and metabolic syndrome in depression: Analysis of the 2009-2010 National Health and Nutrition Examination Survey (NHANES). J. Clin. Psychiatry 2014, 75, e1428-32. [Google Scholar] [CrossRef] [Green Version]
- Goldbacher, E.M.; Bromberger, J.; Matthews, K.A. Lifetime History of Major Depression Predicts the Development of the Metabolic Syndrome in Middle-Aged Women. Psychosom. Med. 2009, 71, 266–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pulkki-Råback, L.; Elovainio, M.; Kivimäki, M.; Mattsson, N.; Raitakari, O.T.; Puttonen, S.; Marniemi, J.; Viikari, J.S.A.; Keltikangas-Järvinen, L. Depressive symptoms and the metabolic syndrome in childhood and adulthood: A prospective cohort study. Health Psychol. 2009, 28, 108–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luc, G.; Arveiler, D.; Evans, A.; Amouyel, P.; Ferrieres, J.; Bard, J.-M.; Elkhalil, L.; Fruchart, J.-C.; Ducimetiere, P. Circulating soluble adhesion molecules ICAM-1 and VCAM-1 and incident coronary heart disease: The PRIME Study. Atherosclerosis 2003, 170, 169–176. [Google Scholar] [CrossRef] [Green Version]
- Pearson, T.A.; Mensah, G.A.; Alexander, R.W.; Anderson, J.L.; Cannon, R.O.; Criqui, M.; Fadl, Y.Y.; Fortmann, S.P.; Hong, Y.; Myers, G.L.; et al. Markers of Inflammation and Cardiovascular Disease. Application to clinical and public health practice: A statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation 2003, 107, 499–511. [Google Scholar] [CrossRef]
- Ross, R. Atherosclerosis—An Inflammatory Disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef]
- Pan, A.; Keum, N.; Okereke, O.I.; Sun, Q.; Kivimaki, M.; Rubin, R.R.; Hu, F.B. Bidirectional Association Between Depression and Metabolic Syndrome: A systematic review and meta-analysis of epidemiological studies. Diabetes Care 2012, 35, 1171–1180. [Google Scholar] [CrossRef] [Green Version]
- Gheshlagh, R.G.; Parizad, N.; Sayehmiri, K. The Relationship Between Depression and Metabolic Syndrome: Systematic Review and Meta-Analysis Study. Iran. Red Crescent Med. J. 2016, 18, e26523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Repousi, N.; Masana, M.F.; Sanchez-Niubo, A.; Haro, J.M.; Tyrovolas, S. Depression and metabolic syndrome in the older population: A review of evidence. J. Affect. Disord. 2018, 237, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Marazziti, D.; Rutigliano, G.; Baroni, S.; Landi, P.; Dell’Osso, L. Metabolic syndrome and major depression. CNS Spectr. 2014, 19, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Dwyer, T.; Viikari, J.; Sinaiko, A.; Burns, T.; Daniels, S.; Juonala, M.; Woo, J.; Urbina, E.; Steinberger, J.; Hu, T.; et al. In Memoriam for Gerald Berenson. Hypertension 2019, 73, 936–937. [Google Scholar] [CrossRef]
- Berenson, G.S.; Srinivasan, S.R.; Bao, W.; Newman, W.P.; Tracy, R.E.; Wattigney, W.A. Association between Multiple Cardiovascular Risk Factors and Atherosclerosis in Children and Young Adults. N. Engl. J. Med. 1998, 338, 1650–1656. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Haringsma, R.; Engels, G.I.; Beekman, A.T.F.; Spinhoven, P. The criterion validity of the Center for Epidemiological Studies Depression Scale(CES-D) in a sample of self-referred elders with depressive symptomatology. Int. J. Geriatr. Psychiatry 2004, 19, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Vilagut, G.; Forero, C.G.; Barbaglia, G.; Alonso, J. Screening for Depression in the General Population with the Center for Epidemiologic Studies Depression (CES-D): A Systematic Review with Meta-Analysis. PLoS ONE 2016, 11, e0155431. [Google Scholar] [CrossRef] [PubMed]
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Soper, D.S. Sobel Test Calculator for the Significance of Mediation [Software]. Available online: https://www.danielsoper.com/statcalc (accessed on 30 April 2021).
- Vogelzangs, N.; Kritchevsky, S.B.; Beekman, A.T.F.; Newman, A.B.; Satterfield, S.; Simonsick, E.M.; Yaffe, K.; Harris, T.B.; Penninx, B.W.J.H. Depressive Symptoms and Change in Abdominal Obesity in Older Persons. Arch. Gen. Psychiatry 2008, 65, 1386–1393. [Google Scholar] [CrossRef] [Green Version]
- Vogelzangs, N.; Beekman, A.T.F.; Kritchevsky, S.B.; Newman, A.B.; Pahor, M.; Yaffe, K.; Rubin, S.M.; Harris, T.B.; Satterfield, S.; Simonsick, E.M.; et al. Psychosocial risk factors and the metabolic syndrome in elderly persons: Findings from the Health, Aging and Body Composition study. J. Gerontol. Ser. A Biol. Sci. Med Sci. 2007, 62, 563–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagby, S.P. Obesity-Initiated Metabolic Syndrome and the Kidney: A Recipe for Chronic Kidney Disease? J. Am. Soc. Nephrol. 2004, 15, 2775–2791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, S.; Gautam, V.; Naseem, S. Acute-phase proteins: As diagnostic tool. J. Pharm. Bioallied Sci. 2011, 3, 118–127. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | White Participants (n = 419) | Black Participants (n = 180) | p Value b |
|---|---|---|---|
| Age (years) a | 36.6 ± 4.3 | 36.1 ± 4.4 | 0.17 |
| Education | |||
| Grade 1–12 or GED | 128 (31.1%) | 109 (61.2%) | <0.001 |
| Vocational/Technical | 81 (19.7%) | 23 (12.9%) | |
| College | 172 (41.8%) | 40 (22.5%) | |
| Postgraduate | 31 (7.5%) | 6 (3.4%) | |
| Income (USD) | |||
| <15,000 | 42 (10.0%) | 96 (54.2%) | <0.001 |
| 15,001–29,999 | 81 (19.4%) | 43 (24.3%) | |
| 30,000–45,000 | 68 (16.3%) | 18 (10.2%) | |
| >45,000 | 227 (54.3%) | 20 (11.3%) | |
| Physical activity | |||
| No/mild | 31 (7%) | 23 (13%) | 0.05 |
| Moderate | 249 (60%) | 92 (51%) | |
| Very active | 138 (33) | 65 (36%) | |
| BMI (kg/m2) a | 26.9 ± 5.4 | 29.6 ± 7.4 | <0.001 |
| Waist circumference (cm) a | 87.6 ± 13.9 | 92.0 ± 16.5 | 0.002 |
| Systolic BP (mmHg) a | 111.4 ± 9.7 | 119.5 ± 15.1 | <0.001 |
| Diastolic BP (mmHg) a | 75.5 ± 7.6 | 80.2 ± 10.7 | <0.001 |
| Fasting blood sugar (mg/dL) ** (25th and 75th percentile) | 81.0 | 82.0 | 0.73 |
| (76.0–87.0) | (75.0–88.0) | ||
| Insulin (µU/mL) median value ** (25th and 75th percentile) | 8.0 | 10.0 | 0.005 |
| (6.0–12.0) | (7.0–17.0) | ||
| * HOMA-IR median value ** (25th and 75th percentile) | 0.52 | 0.71 | 0.003 |
| (0.14–0.93) | (0.23–1.27) | 0.002 | |
| LDL cholesterol (mg/dL) a HDL cholesterol (mg/dL) a | 124.5 ± 32.0 | 115.9 ± 31.10 | <0.001 |
| 48.6 ±13.2 | 54.3 ± 14.3 | <0.001 | |
| Triglycerides (mg/dL) median ** (25th and 75th percentile) | 99.0 | 82.0 | <0.001 |
| (72.0–134.0) | (59.0–106.0) | ||
| hs-CRP (mg/L) median value ** (25th and 75th percentile) | 1.17 | 1.82 | 0.02 |
| (0.47–2.90) | (0.65–3.62) | ||
| ICAM-1 (ng/mL) median value ** (25th and 75th percentile) | 258 | 253 | 0.09 |
| (217–321) | (189–315) | ||
| Smoking prevalence | 125 (30.0%) | 66 (37.0%) | 0.09 |
| Depressed | 238 (57.0%) | 132 (73.3%) | 0.002 |
| Not depressed | 180 (43.0%) | 48 (26.7%) | |
| Drinking alcohol for last 12 months | |||
| No | 150 (35.8%) | 66 (36.7%) | 0.83 |
| Yes | 269 (64.2%) | 114 (63.3%) | 0.17 |
| White Participants | Black Participants | |||||
|---|---|---|---|---|---|---|
| Variables | No MetS (n = 312) | MetS (n = 107) | p Value b | No MetS (n = 126) | MetS (n = 54) | p Value b |
| Gender | 0.18 | 0.73 | ||||
| Male | 123 (39.4%) | 50 (46.7%) | 43 (34.1%) | 17 (31.5%) | ||
| Female | 189 (60.6%) | 57 (53.3%) | 83 (65.9%) | 37 (68.5%) | ||
| Age (years) a | 36.6 (4.3) | 36.6 (4.4) | 0.97 | 36.3 (4.3) | 35.5 (4.5) | 0.27 |
| Education | ||||||
| Grade 1–12 or GED | 90 (29.4%) | 38 (35.9%) | 75 (60.5%) | 34 (31.2%) | 0.81 $ | |
| Vocational/Technical | 64 (20.9%) | 17 (16.0%) | 0.3 | 18 (14.5%) | 5 (21.7%) | |
| College | 126 (41.2%) | 46 (43.4%) | 27 (21.8%) | 13 (32.5%) | ||
| Postgraduate | 26 (8.5%) | 5 (4.7) | 4 (3.2%) | 2 (3.7%) | ||
| Income (USD) | ||||||
| <15,000 | 29 (9.3%) | 13 (12.2%) | 69 (56.1%) | 27 (50.0%) | 0.14 | |
| 15,001–29,999 | 49 (15.8%) | 32 (29.9%) | 0.006 | 33 (26.8%) | 10 (18.5%) | |
| 30,000–45,000 | 52 (16.7%) | 16 (15.0%) | 9 (7.2%) | 9 (16.7%) | ||
| >45,000 | 181 (58.2%) | 46 (43.0%) | 12 (9.8%) | 8 (14.8%) | ||
| Smoking | ||||||
| No | 220 (71.0%) | 72 (67.3%) | 0.47 | 72 (57.6%) | 41 (75.9%) | 0.02 |
| Yes | 72 (29.0%) | 35 (32.7%) | 53 (42.4%) | 13 (24.1%) | ||
| Drinking alcohol | ||||||
| No drinking | 100 (32.0%) | 50 (46.7%) | 0.006 | 42 (33.3%) | 24 (44.4%) | 0.15 |
| Drinking | 212 (68.0%) | 57 (53.3%) | 34 (66.7% | 18 (55.6%) | ||
| Physical activity | ||||||
| No/mild | 20 (6.4%) | 11 (10.3%) | 0.13 | 19 (15.1%) | 4 (7.4%) | 0.23 |
| Moderate | 181 (58.2%) | 68 (63.6%) | 60 (47.6%) | 32 (59.3%) | ||
| Very active | 110 (35.4%) | 28 (26.2%) | 47 (37.3%) | 18 (33.3%) | ||
| BMI (kg/m2) a | 26.0 (5.2) | 29.4 (5.4) | <0.001 | 28.2 (7.3) | 32.9 (6.3) | <0.001 |
| Waist circumference (cm) a | 85.2 (13.3) | 94.7 (13.3) | <0.001 | 88.4 (15.8) | 100.5 (15.0) | <0.001 |
| Systolic BP (mm Hg) a | 110.7 (9.6) | 113.5 (9.7) | 0.01 | 116.8 (12.7) | 125.8 (12.7) | 0.002 |
| Diastolic BP (mm Hg) a | 74.9 (7.5) | 77.0 (7.6) | 0.01 | 78.6 (10.3) | 83.9 (10.6) | 0.002 |
| Fasting blood sugar (mg/dL) median * (25th and 75th percentile) | 80 (75.0–86.0) | 84 (78.0–91.0) | 0.001 | 81 (74.0–87.0) | 85 (78.0–98.00) | 0.006 |
| Insulin (µU/mL) a (25th and 75th percentile) | 8 (6.0–11.0) | 11 (8.0–14.0) | <0.001 | 9 (6.0–13.0) | 15 (9.0–19.0) | <0.001 |
| HOMA-IR (median value) * (25th and 75th percentile) | 0.4 (0.08–0.80) | 0.87 (0.45–1.10) | <0.001 | 0.61 (0.15–1.07) | 1.15 (0.66–1.44) | 0.002 |
| Triglycerides (mg/dL) a (25th and 75th percentile) | 91.5 (67.0–126.0) | 115 (89-153) | <0.001 | 76.5 (53–100) | 94 (72–115) | 0.004 |
| LDL cholesterol (mg/dl) a | 123.0 (31.7) | 129.0 (32.4) | 0.09 | 123.0 (31.7) | 129.0 (32.4) | 0.09 |
| HDL cholesterol (mg/dl) a | 50.2 (13.6) | 44.1 (10.7) | <0.001 | 56.5 (14.4) | 49.3 (12.6) | 0.002 |
| hs-CRP (median value) * (25th and 75th percentile) | 1.04 (0.41–2.89) | 1.62 (0.81–2.93) | 0.005 | 1.2 (0.44–5.61) | 2.89 (1.95–5.44) | <0.001 |
| ICAM-1 median value * (25th and 75th percentile) | 255 (213–320) | 268 (228–322) | 0.42 | 260 (197–312) | 241 (184–322) | 0.33 |
| Model | Parameter Estimates | p Value | Relative Risk (RR) | 95% of RR |
|---|---|---|---|---|
| White Participants | ||||
| Model 1 (unadjusted) | ||||
| DS (yes vs. no) | 0.20 (0.17) | 0.25 | 1.22 | 0.87–1.71 |
| C-reactive protein | 0.15 (0.07) | 0.02 | 1.18 | 1.02–1.32 |
| Model 2 (both in the model) | ||||
| DS (yes vs. no) | 0.14 (0.17) | 0.41 | 1.16 | 0.83–1.63 |
| C-reactive protein | 0.16 (0.06) | 0.01 | 1.17 | 1.03–1.32 |
| Model 3 (adjusted *) | ||||
| DS (yes vs. no) | 0.14 (0.17) | 0.42 | 1.15 | 0.82–1.62 |
| C-reactive protein | 0.03 (0.07) | 0.67 | 1.03 | 0.89–1.19 |
| Black Participants | ||||
| Model 1 (unadjusted) | ||||
| DS | −0.40 (0.22) | 0.08 | 0.67 | 0.42–1.05 |
| C-reactive protein | 0.41 (0.09 | <0.001 | 1.51 | 1.25–1.82 |
| Model 2 (both in the model) | ||||
| DS | −0.31 (0.22) | 0.15 | 0.73 | 0.47–1.12 |
| C-reactive protein | 0.46 (0.10) | <0.003 | 1.58 | 1.32–1.90 |
| Model 3 ** | ||||
| DS (yes vs. no) | −0.21 (0.25) | 0.37 | 0.80 | 0.49–1.31 |
| C-reactive protein | 0.37 (0.11) | 0.005 | 1.44 | 1.18–1.78 |
| Model Selection | Parameter Estimates | p Value | Relative Risk (RR) | 95% of RR |
|---|---|---|---|---|
| White Participants | ||||
| Model 1 (unadjusted) | ||||
| DS (yes vs. no) | 0.26 (0.11) | <0.02 | 1.30 | 1.04–1.62 |
| C-reactive protein | 0.27 (0.04) | <0.001 | 1.31 | 1.21–1.43 |
| ICAM-1 | −0.20 (0.16) | 0.20 | 0.82 | 0.60–1.11 |
| Model 2 (Both in the model) | ||||
| DS (yes vs. no) | 0.14 (0.11) | 0.22 | 1.14 | 0.92–1.42 |
| C-reactive protein | 0.26 (0.04) | <0.001 | 1.30 | 1.19–1.42 |
| Model 3 (adjusted) * | ||||
| DS | 0.08 (0.10) | 0.44 | 1.08 | 0.88–1.32 |
| C-reactive protein | 0.12 (0.05) | 0.01 | 1.12 | 1.02–1.23 |
| Black Participants | ||||
| Model 1 (unadjusted) | ||||
| DS (yes vs. no) | −0.19 (0.12) | 0.12 | 0.82 | 0.64–1.05 |
| C-reactive protein | 0.25 (0.04) | <0.001 | 1.30 | 1.17–1.45 |
| ICAM-1 | −0.04 (0.10) | 0.74 | 0.97 | 0.78–1.19 |
| Model 2 (Both in the model) | ||||
| DS (yes vs. no) | −0.14 (0.11) | 0.23 | 0.91 | 0.75–1.10 |
| C-reactive protein | 0.25 (0.06) | <0.001 | 1.14 | 1.06–1.22 |
| Model 3 (adjusted) ** | ||||
| DS (yes vs. no) | 0.03 (0.12) | 0.91 | 1.01 | 0.80–1.23 |
| C-reactive protein | 0.07 (0.06) | 0.19 | 1.07 | 0.96–1.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhuiyan, A.R.; Payton, M.; Mitra, A.K.; Leggett, S.S.; Xu, J.; Tchounwou, P.B.; Smart, F. Progression of Metabolic Syndrome Components along with Depression Symptoms and High Sensitivity C-Reactive Protein: The Bogalusa Heart Study. Int. J. Environ. Res. Public Health 2021, 18, 5010. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18095010
Bhuiyan AR, Payton M, Mitra AK, Leggett SS, Xu J, Tchounwou PB, Smart F. Progression of Metabolic Syndrome Components along with Depression Symptoms and High Sensitivity C-Reactive Protein: The Bogalusa Heart Study. International Journal of Environmental Research and Public Health. 2021; 18(9):5010. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18095010
Chicago/Turabian StyleBhuiyan, Azad R., Marinelle Payton, Amal K. Mitra, Sophia S. Leggett, Jihua Xu, Paul B. Tchounwou, and Frank Smart. 2021. "Progression of Metabolic Syndrome Components along with Depression Symptoms and High Sensitivity C-Reactive Protein: The Bogalusa Heart Study" International Journal of Environmental Research and Public Health 18, no. 9: 5010. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18095010