Improving Health Literacy Responsiveness: A Randomized Study on the Uptake of Brochures on Doctor-Patient Communication in Primary Health Care Waiting Rooms

 , ,
, ,
Abstract
:1. Introduction
1.1. The Waiting Room as an Opportunity for Improving Health Literacy Responsiveness
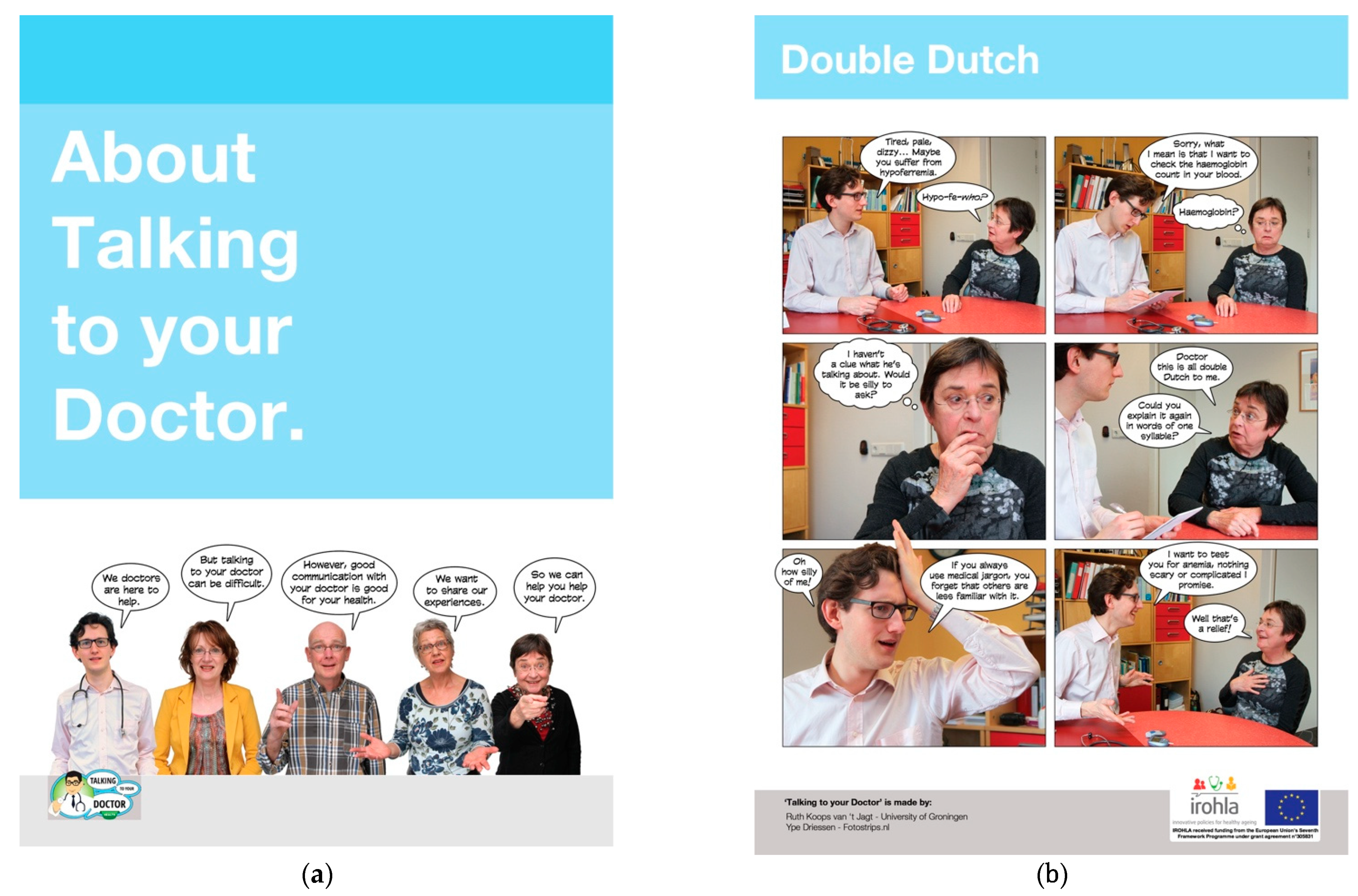
1.2. Narrative Health Education Materials, in Particular Photo Stories
1.3. Exposure to Health Information Materials as a Condition for Effectiveness
1.4. Aims of the Study
2. Materials and Methods
2.1. Setting
2.2. Patients
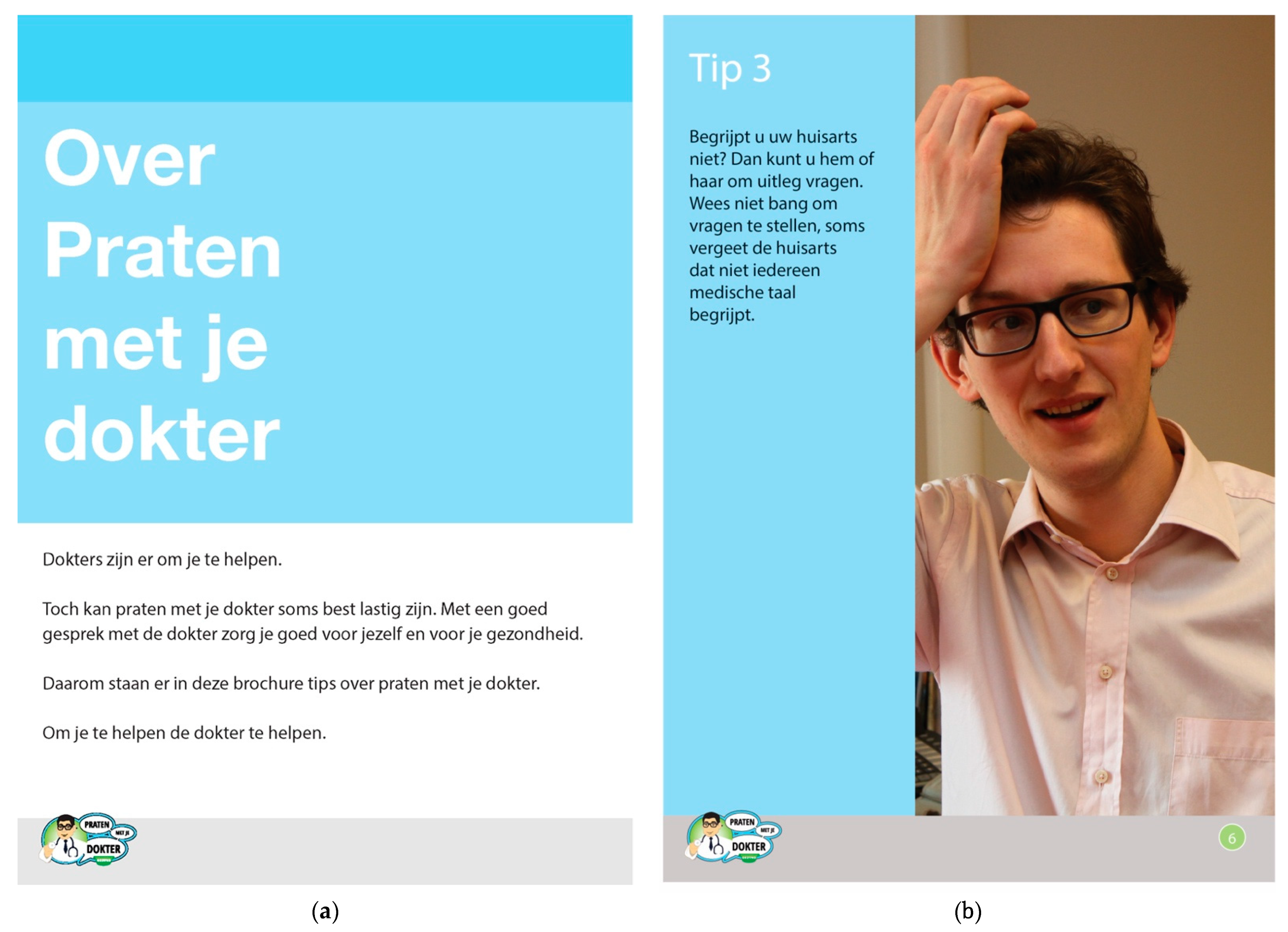
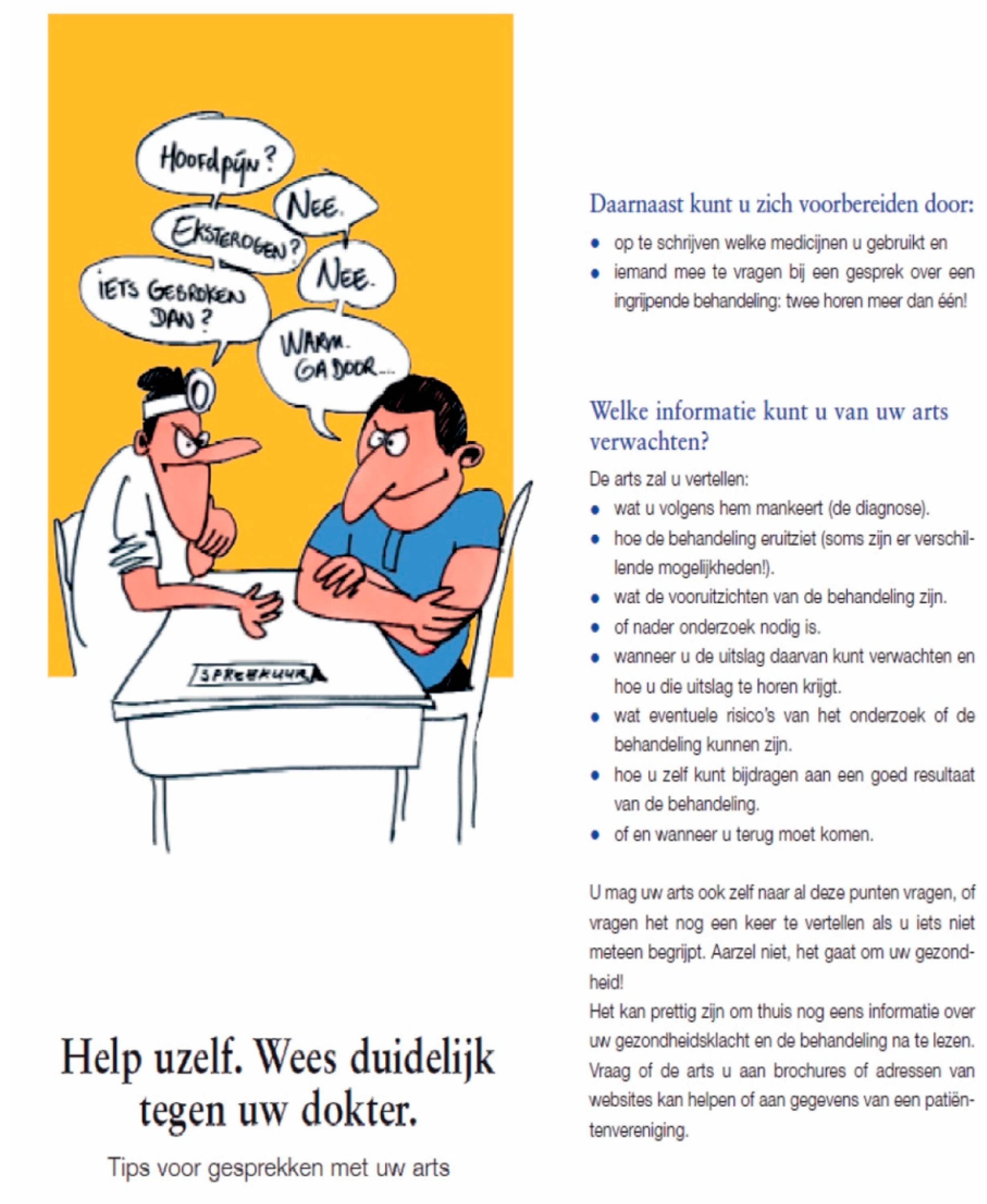
2.3. Intervention Materials: Three Brochures
2.4. Procedure and Measurements
Outcome Measures
2.5. Analysis
3. Results
3.1. Background Characteristics of Sample
3.2. Number of Brochures Noticed, Browsed and Taken per Brochure
3.2.1. Observations
3.2.2. Interviews
3.3. Participants’ Responses per Brochure
4. Discussion
4.1. Strengths and Limitations
4.2. Implications for Practice
4.3. Implications for Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Geboers, B.; Reijneveld, S.A.; Koot, J.A.R.; De Winter, A.F. Moving towards a comprehensive approach for health literacy interventions: The development of a health literacy intervention model. Int. J. Environ. Res. Public Health 2018, 15, 1268. [Google Scholar] [CrossRef] [Green Version]
- Jansen, C.; De Stadler, L.; Douma, A. (Eds.) Communicate as a Professional; Amsterdam University Press: Amsterdam, The Netherlands, 2019. [Google Scholar]
- McCormack, L.; Thomas, V.; Lewis, M.A.; Rudd, R. Improving low health literacy and patient engagement: A social ecological approach. Patient Educ. Couns. 2018, 100, 8–13. [Google Scholar] [CrossRef]
- International Union for Health Promotion and Education (IUHPE). IUHPE Position Statement on Health Literacy: A Practical Vision for a Health Literate World. IUHPE Global Working Group on Health Literacy; IUHPE: Paris, France, 2018. [Google Scholar]
- Batterham, R.W.; Beauchamp, A.; Osborne, R.H. Health Literacy. In The International Encyclopedia of Public Health, 2nd ed.; Quah, S.R., Cockerham, W.C., Eds.; Academic Press: Oxford, UK, 2017; Volume 3, pp. 428–437. [Google Scholar]
- Trezona, A.; Dodson, S.; Osborne, R.H. Development of the organisational health literacy responsiveness (Org-HLR) framework in collaboration with health and social services professionals. BMC Health Serv. Res. 2017, 17, 513. [Google Scholar] [CrossRef] [Green Version]
- McDonald, C.E.; Remedios, L.J.; Said, C.M.; Granger, C.L. Health Literacy in hospital outpatient waiting areas: An observational study of what is available to and accessed by consumers. Herd-Health Environ. Res. 2020, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Cass, S.J.; Ball, L.E.; Leveritt, M.D. Passive interventions in primary healthcare waiting rooms are effective in promoting healthy lifestyle behaviours: An integrative review. Aust. J. Prim. Health 2016, 22, 198–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moerenhout, T.; Borgermans, L.; Schol, S.; Vansintejan, J.; Van De Vijver, E.; Devroey, D. Patient health information materials in waiting rooms of family physicians: Do patient care? Patient Prefer. Adher. 2013, 7, 489–497. [Google Scholar]
- Arneill, A.B.; Devlin, A.S. Perceived quality of care: The influence of the waiting room environment. J. Environ. Psychol. 2002, 22, 345–360. [Google Scholar] [CrossRef]
- Oermann, M.H. Effects of educational intervention in waiting room on patient satisfaction. J. Ambul. Care Manag. 2003, 26, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Maskell, K.; McDonald, P.; Paudyal, P. Effectiveness of health education materials in general practice waiting rooms: A cross-sectional study. Br. J. Gen. Pract. 2018, 68, e869–e876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, C.; Elliott, K.; Gall, J.; Woodward-Kron, R. Patient and clinician engagement with health information in the primary care waiting room: A mixed methods case study. J. Public Health Res. 2019, 8, 1476. [Google Scholar] [CrossRef] [Green Version]
- Brach, C.; Dreyer, B.; Schyve, P.; Hernandez, L.M.; Baur, C.; Lemerise, A.J.; Parker, R. Attributes of a Health Literate Organization; National Academies Press: Washington, DC, USA, 2012. [Google Scholar]
- Kenny, T.; Wilson, R.G.; Purves, I.N.; Newton, L.D.; Newton, D.P.; Moseley, D.V. A PIL for every ill? Patient information leaflets (PILs): A review of past, present and future use. Fam. Pract. 1998, 15, 471–477. [Google Scholar] [CrossRef]
- Protheroe, J.; Estacio, E.V.; Saidy-Khan, S. Patient information materials in general practices and promotion of health literacy: An observational study of their effectiveness. Br. J. Gen. Pract. 2015, 65, e192–e197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singhal, A.; Rogers, E.M. Entertainment-Education: A Communication Strategy for Social Change; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1999. [Google Scholar]
- Hinyard, L.J.; Kreuter, M.W. Using narrative communication as a tool for health behavior change: A conceptual, theoretical, and empirical overview. Health Educ. Behav. 2007, 34, 777–792. [Google Scholar] [CrossRef]
- Kopfman, J.E.; Smith, S.W.; Ah Yun, J.K.; Hodges, A. Affective and cognitive reactions to narrative versus statistical evidence organ donation messages. J. Appl. Commun. Res. 1998, 26, 279–300. [Google Scholar] [CrossRef]
- Greene, K.; Brinn, L.S. Messages influencing college women’s tanning bed use: Statistical versus narrative evidence format and a self-assessment to increase perceived susceptibility. J. Health Commun. 2003, 8, 443–461. [Google Scholar] [CrossRef] [PubMed]
- Mazor, K.M.; Baril, J.; Dugan, E.; Spencer, F.; Burgwinkle, P.; Gurwitz, J.H. Patient education about anticoagulant medication: Is narrative evidence or statistical evidence more effective? Patient Educ. Couns. 2007, 69, 145–157. [Google Scholar] [CrossRef] [PubMed]
- Kreuter, M.W.; Holmes, K.; Alcaraz, K.; Kalesan, B.; Rath, S.; Richert, M.; Clark, E.M. Comparing narrative and informational videos to increase mammography in low-income African American women. Patient Educ. Couns. 2010, 81 (Suppl. 1), S6–S14. [Google Scholar] [CrossRef] [Green Version]
- Zabrucky, K.M.; Moore, D. Influence of text genre on adults’ monitoring of understanding and recall. Educ. Gerontol. 1999, 25, 691–710. [Google Scholar]
- Glaser, M.; Garsoffky, B.; Schwan, S. Narrative-based learning: Possible benefits and problems. Communications 2009, 34, 429–447. [Google Scholar] [CrossRef]
- van’t Jagt, R.K.; Hoeks, J.C.J.; Duizer, E.; Baron, M.; Molina, G.B.; Unger, J.B.; Jansen, C.J.M. Sweet Temptations: How does reading a fotonovela about diabetes affect Dutch adults with different levels of literacy? Health Commun. 2018, 33, 284–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreuter, M.W.; Green, M.C.; Cappella, J.N.; Slater, M.D.; Wise, M.E.; Story, D.; Clark, E.M.; O’Keefe, D.; Erwin, D.O.; Holmes, K.; et al. Narrative Communication in cancer prevention and control: A framework to guide research and application. Ann. Behav. Med. 2007, 33, 221–235. [Google Scholar] [CrossRef] [Green Version]
- Shen, F.; Sheer, V.C.; Li, R. Impact of narratives on persuasion in health communication: A meta-analysis. J. Advert. 2015, 44, 105–113. [Google Scholar] [CrossRef]
- De Graaf, A.; Sanders, J.; Hoeken, H. Characteristics of narrative interventions and health effects: A review of the content, form, and context of narratives in health-related narrative persuasion research. Rev. Commun. Res. 2016, 4, 88–131. [Google Scholar]
- Moyer-Gusé, E.; Nabi, R.L. Explaining the persuasive effects of narrative in an entertainment television program: Overcoming resistance to persuasion. Hum. Commun. Res. 2010, 36, 26–52. [Google Scholar] [CrossRef]
- Mar, R.A.; Oatley, K. The function of fiction is the abstraction and simulation of social experience. Perspect. Psychol. Sci. 2008, 3, 173–192. [Google Scholar] [CrossRef]
- Schank, R.C.; Abelson, R.P. Knowledge and memory: The real story. In Advances in Social Cognition; Wyer, R.S., Jr., Ed.; Erlbaum: Hillsdale, NJ, USA, 1995; Volume 8, pp. 1–85. [Google Scholar]
- James, S.; Reddy, P.S.; Ruiter, R.A.C.; Taylor, M.; Jinabhai, C.C.; Van Empelen, P.; Van den Borne, B. The effects of a systematically developed photo-novella on knowledge, attitudes, communication and behavioural intentions with respect to sexually transmitted infections among secondary school learners in South Africa. Health Promot. Int. 2005, 20, 157–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unger, J.B.; Molina, G.B.; Baron, M. Evaluation of Sweet Temptations, a fotonovela for diabetes education. Hisp. Health Care Int. 2009, 7, 145–152. [Google Scholar] [CrossRef]
- Unger, J.B.; Cabassa, L.J.; Molina, G.B.; Contreras, S.; Baron, M. Evaluation of a fotonovela to increase depression knowledge and reduce stigma among Hispanic adults. J. Immigr. Minor. Health 2013, 15, 398–406. [Google Scholar] [CrossRef] [Green Version]
- Boyte, R.M.; Pilisuk, T.; Matiella, A.C.; Macario, E. Developing a bilingual fotonovela to encourage human papillomavirus preteen immunization in California: A case study. Calif. J. Health Promot. 2014, 12, 1–13. [Google Scholar] [CrossRef]
- Davis, B.; Jansen, C. Using a fotonovela to battle chrystal meth in South Africa. J. Ethn. Subst. Abuse 2020, 19, 151–169. [Google Scholar] [CrossRef]
- Mayer, R.E. The Cambridge Handbook of Multimedia Learning; Cambridge University Press: Cambridge, UK, 2005. [Google Scholar]
- Sweller, J.; Ayres, P.; Kalyuga, S. Cognitive Load Theory; Springer: New York, NY, USA, 2011. [Google Scholar]
- van’t Jagt, R.K.; Tan, S.L.; Hoeks, J.C.J.; Spoorenberg, S.; Reijneveld, S.A.; De Winter, A.F.; Lippke, S.; Jansen, C.J.M. Using photo stories to support doctor-patient communication: Evaluating a communicative health literacy intervention for older adults. Int. J. Environ. Res. Public Health 2019, 16, 3726. [Google Scholar] [CrossRef] [Green Version]
- McGuire, W.J. McGuire’s classic input-output framework for constructing persuasive messages. In Public Communication Campaigns, 4th ed.; Rice, R.E., Atkin, C.K., Eds.; Sage: Thousand Oaks, CA, USA, 2012; pp. 136–146. [Google Scholar]
- Lloyd-Williams, F. The effect of an intervention programme to improve health education leaflet uptake and distribution in community pharmacies. Patient Educ. Couns. 2003, 49, 27–33. [Google Scholar] [CrossRef]
- Williams, M.; Bethea, J. Patient awareness of oral cancer health advice in a dental access centre: A mixed methods study. Br. Dent. J. 2011, 210, e9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, H.D. Spyt kom te laat: The Development and Evaluation of a Health-related Fotonovela about Methamphetamine (‘tik’) Use in the Western Cape and Northern Cape Provinces of South Africa. Ph.D. Dissertation, Stellenbosch University, Stellenbosch, South Africa, 2017. Available online: http://scholar.sun.ac.za/handle/10019.1/102845 (accessed on 17 April 2021).
- van’t Jagt, R.K.; De Winter, A.F.; Reijneveld, S.A.; Hoeks, J.C.J.; Jansen, C.J.M. Development of a communication intervention for older adults with limited health literacy: Photo stories to support doctor-patient communication. J. Health Commun. 2016, 21 (Suppl. 2), 69–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 1–42. [Google Scholar] [CrossRef] [Green Version]
- CBS Statline. Available online: https://opendata.cbs.nl/statline/#/CBS/en/dataset/81178ENG/table?ts=1618672508578 (accessed on 17 April 2021).
- Kaper, M.S.; De Winter, A.F.; Bevilacqua, R.; Giammarchi, C.; McCusker, A.; Sixsmith, J.; Koot, J.A.R.; Reijneveld, S.A. Positive outcomes of a comprehensive health literacy communication training for health professionals in three European countries: A multi-centre pre-post intervention study. Int. J. Environ. Res. Public Health 2019, 16, 3923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaper, M.S.; Reijneveld, S.A.; Van Es, F.D.; De Zeeuw, J.; Almansa, J.; Koot, J.A.R.; De Winter, A.F. Effectiveness of a comprehensive health literacy consultation skills training for undergraduate medical students: A randomized controlled trial. Int. J. Environ. Res. Public Health 2020, 17, 81. [Google Scholar] [CrossRef] [Green Version]
- Kaper, M.S.; Sixsmith, J.; Meijering, L.; Vervoordeldonk, J.; Doyle, P.; Barry, M.M.; De Winter, A.F.; Reijneveld, S.A. Implementation and long-term outcomes of organizational health literacy interventions in Ireland and the Netherlands: A longitudinal mixed-methods study. Int. J. Environ. Res. Public Health 2019, 16, 4812. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Primary Health Care Practice A | Primary Health Care Practice B | Primary Health Care Practice C | ||
|---|---|---|---|---|
| week 1 | Monday | Non-narrative | Photo stories | Existing |
| Tuesday | Photo stories | Existing | Non-narrative | |
| Wednesday | Existing | Non-narrative | Photo stories | |
| Thursday | Non-narrative | Photo stories | Existing | |
| Friday | Photo stories | Existing | Non-narrative | |
| week 2 | Monday | Existing | Non-narrative | Photo stories |
| Tuesday | Non-narrative | Photo stories | Existing | |
| Wednesday | Photo stories | Existing | Non-narrative | |
| Thursday | Existing | Non-narrative | Photo stories | |
| Friday | Non-narrative | Photo stories | Existing | |
| week 3 | Monday | Photo stories | Existing | Non-narrative |
| Tuesday | Existing | Non-narrative | Photo stories | |
| Wednesday | Non-narrative | Photo stories | Existing | |
| Thursday | Photo stories | Existing | Non-narrative | |
| Friday | Existing | Non-narrative | Photo stories |
| Primary Health Care Practice A | Primary Health Care Practice B | Primary Health Care Practice C | |
|---|---|---|---|
| Number of registered patients | 14,157 | 5284 | 4465 |
| Male/female (%) | 49.2%/50.8% | 49.4%/50.6% | 48.4%/51.6% |
| Age range | 0–100 | 0–100 | 0–99 |
| Number of GPs | 8 | 7 | 3 |
| Number of other health professionals (nurses etc.) | 23 | 8 | 6 |
| Average number of GP visits per week | circa 500 | circa 350 | circa 250 |
| Waiting room characteristics | Large space, where people can enter at two points; many tables with space for leaflets | Medium large space; reading table with space for leaflets | Small space with little room for information leaflets; displays on a small side table and in the window sills. |
| Did you notice this brochure? | |||
| Yes | No | Total | |
| Photo stories | 59 (48.4%) | 63 (51.6%) | 122 |
| Non-narrative | 39 (30.5%) | 89 (69.5%) | 128 |
| Existing | 37 (26.4%) | 103 (73.6%) | 140 |
| Did you browse this brochure? (only asked if people had noticed the brochure) | |||
| Yes | No | Total | |
| Photo stories | 18 (30.5%) | 41 (69.5%) | 59 |
| Non-narrative | 14 (35.9%) | 25 (64.1%) | 39 |
| Existing | 16 (43.2%) | 21 (56.8%) | 37 |
| Did you take this brochure with you? (only asked if people had noticed the brochure) | |||
| Yes | No | Total | |
| Photo stories | 7 (11.9%) | 52 (88.1%) | 59 |
| Non-narrative | 3 (8.1%) | 34 (91.9%) | 37 (2 missing values) |
| Existing | 8 (21.6%) | 29 (78.4%) | 37 |
| Not browsing the brochure (N = 87), because of… | |||
| Situation-related factors | Self-related factors | ||
| Motivation | Opportunity | Motivation | Opportunity |
| Too many brochures available (PSV:2; NNV:0; EB:0) | Not enough time (PSV:4; NNV:5; EB:2) | Other activities/attention elsewhere, e.g., reading something else, watching children, looking at smartphone, just sitting (PSV:11; NNV:0; EB:7) | Too stressed, distracted, tired or ill (PSV:0; NNV:4; EB:4) |
| Placing suggested other target group (PSV:1) | Not within reach, too many people in waiting room (PSV:3; NNV:2; EB:4) | Not interested, not relevant, no need, information already known (PSV:13; NNV:12; EB:9) | No reading glasses (PSV:1; NNV:2; EB:1) |
| Not a typical reader of brochures (PSV:3; NNV:2; EB:1) | Insufficient Dutch language proficiency (PSV:1; NNV:0; EB:0) | ||
| Only read the front cover (PSV:0; NNV:5; EB:0) | |||
| No particular reason/did not consider/don’t know (PSV:4; NNV:1; EB:1) | |||
| Browsing the brochure (N = 48), because of | |||
| Situation-related factors | Self-related factors | ||
| Motivation | Opportunity | Motivation | Opportunity |
| Within reach (PSV:2; NNV:0; EB:0) | Interested/curious/relevant topic (PSV:9; NNV:5; EB:4) | ||
| Someone else mentioned brochure (PSV:1; NNV:0; EB:0) | Killing time (PSV:4; NNV:1; EB:2) | ||
| Brochure stood out/great appeal compared to other brochures (PSV:1; NNV:3; EB:2) | Great appeal brochure (PSV:3; NNV:1; EB:0) | ||
| Overheard interviewer (PSV:0; NNV:0; EB:1) | Always looking at brochures (PSV:0; NNV:0; EB:1) | ||
| Noticed brochure being put down (PSV:0; NNV:0; EB:1) | |||
| Not taking the brochure (N = 115), because of… | |||
| Situation-related factors | Self-related factors | ||
| Motivation | Opportunity | Motivation | Opportunity |
| Not my GP (PSV:1; NNV:0; EB:0) | Not enough time (PSV:2; NNV:0; EB:1) | No interest/need/relevance (PSV:13; NNV:20; EB:15) | Too stressed/distracted/tired/ill: (PSV:1; NNV:0; EB:3) |
| Not within reach/waiting room too busy (PSV:2; NNV:0; EB:1) | Reading it was sufficient (PSV:7; NNV:1; EB:0) | Too difficult (PSV:1; NNV:0; EB:0) | |
| Couldn’t see what it was about (PSV:0; NNV:1; EB:0) | Attention elsewhere (PSV:2; NNV:0; EB:0) | Left it for other people to read (PSV:1; NNV:0; EB:0) | |
| Not the type of person to take brochures (PSV:1; NNV:0; EB:1) | No reading glasses (PSV:0; NNV:0; EB:1) | ||
| No particular reason/did not consider/don’t know (PSV:8; NNV:5; EB:5) | |||
| Taking the brochure (N = 18), because of… | |||
| Situation-related factors | Self-related factors | ||
| Motivation | Opportunity | Motivation | Opportunity |
| Interested/curious/relevant (PSV:2; NNV:0; EB:1) | To read again further/at (PSV:2; NNV:1; EB:1) | ||
| Took it for someone else (PSV:2; NNV:0; EB:1) | |||
| PSV (N = 18) | Motivation | Comprehensibility | Possible Impact on Behavior | Other |
|---|---|---|---|---|
| Positive comments | Not to be missed (1) Fun (4) Attractive (3) Made curious (1) Interesting (1) | Clear, understandable (16) Clear pictures (3) Good font size (1) Accessible (1) | Striking content (1) Beneficial (1) Useful (2) Recognizable situations (5) Thought provoking (2) Important content (2) Great for shy people (1) | Neutral (8) Good brochure (1) |
| Negative comments | Childish (2) Commercial (1) Old-fashioned (1) | Too simple (1) | Already informed/no need (5) | |
| NNV (N = 14) | Motivation | Comprehensibility | Possible impact on behavior | Other |
| Positive comments | Interesting (1) Nice (1) Really beautiful (1) Notable, distinct (1) | Clear, understandable (3) Understandable language (3) Clear pictures (1) | Useful (2) Great for people who do not visit doctors regularly (1) Informative (1) Realistic situations (1) | Neutral (3) Good (1) Positive (1) |
| Negative comments | Not interesting (2) Stinks (1) | |||
| EB (N = 16) | Motivation | Comprehensibility | Possible impact on behavior | Other |
| Positive comments | Distinct/funny cartoon (4) Made curious (1) Colorful (1) Good headline (1) | Good font size (2) Clear, understandable (4) Simple (1) Accessible (2) Good size (1) | Useful (3) Refreshes memory (1) Well prepared after reading (1) Good to draw people’s attention to this topic (2) Good content (1) | Good (1) Neutral (1) Okay (1) |
| Negative comments | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jansen, C.J.M.; Koops van ’t Jagt, R.; Reijneveld, S.A.; van Leeuwen, E.; de Winter, A.F.; Hoeks, J.C.J. Improving Health Literacy Responsiveness: A Randomized Study on the Uptake of Brochures on Doctor-Patient Communication in Primary Health Care Waiting Rooms. Int. J. Environ. Res. Public Health 2021, 18, 5025. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18095025
Jansen CJM, Koops van ’t Jagt R, Reijneveld SA, van Leeuwen E, de Winter AF, Hoeks JCJ. Improving Health Literacy Responsiveness: A Randomized Study on the Uptake of Brochures on Doctor-Patient Communication in Primary Health Care Waiting Rooms. International Journal of Environmental Research and Public Health. 2021; 18(9):5025. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18095025
Chicago/Turabian StyleJansen, Carel J. M., Ruth Koops van ’t Jagt, Sijmen A. Reijneveld, Ellen van Leeuwen, Andrea F. de Winter, and John C. J. Hoeks. 2021. "Improving Health Literacy Responsiveness: A Randomized Study on the Uptake of Brochures on Doctor-Patient Communication in Primary Health Care Waiting Rooms" International Journal of Environmental Research and Public Health 18, no. 9: 5025. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18095025