
Sagittal Integral Morphotype of Female Classical Ballet Dancers and Predictors of Sciatica and Low Back Pain

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Subjects
2.3. Questionnaire
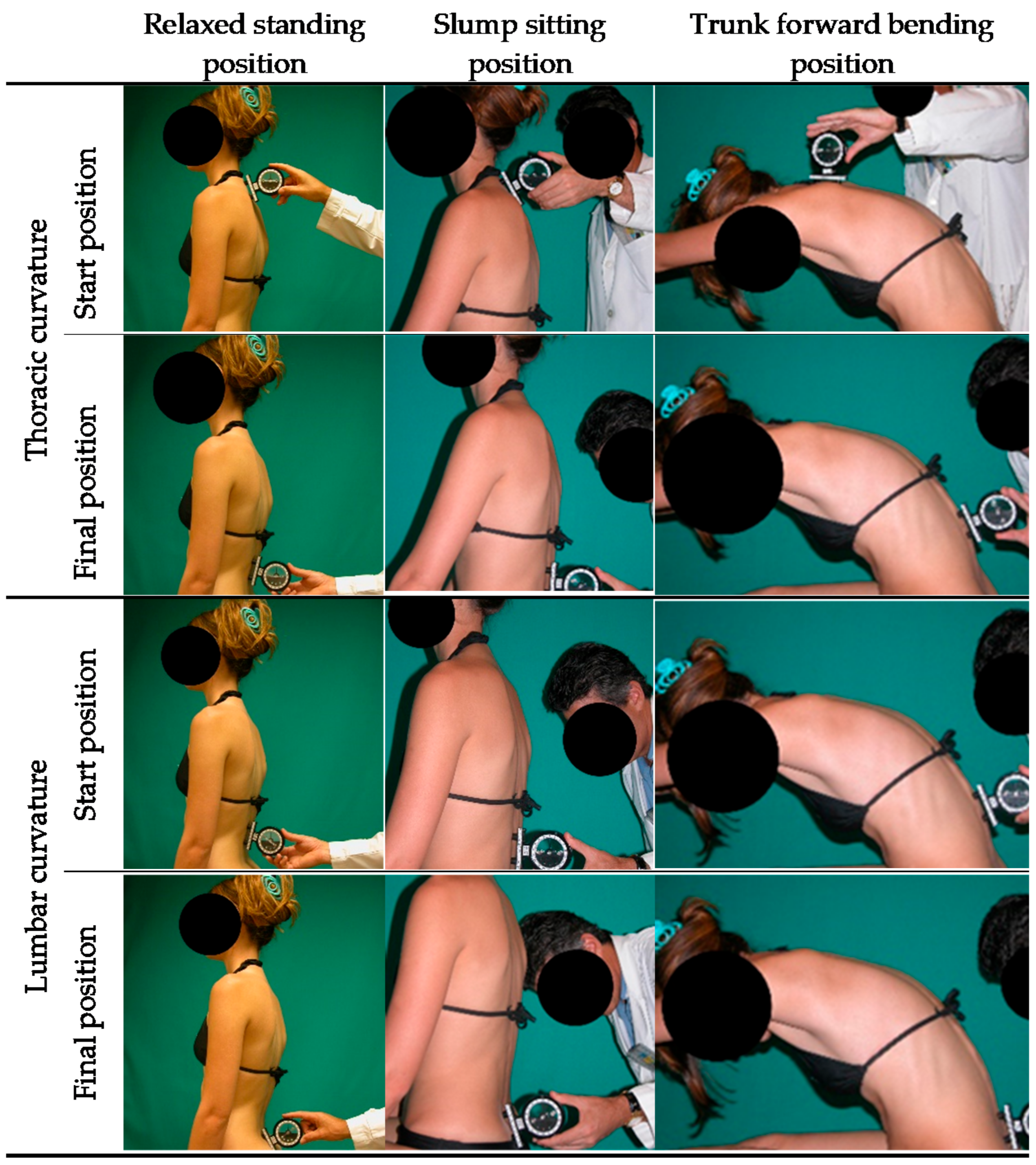
2.4. Evaluation of Potential Predictors Factors for Sciatica and LBP
2.5. Statistical Analyses
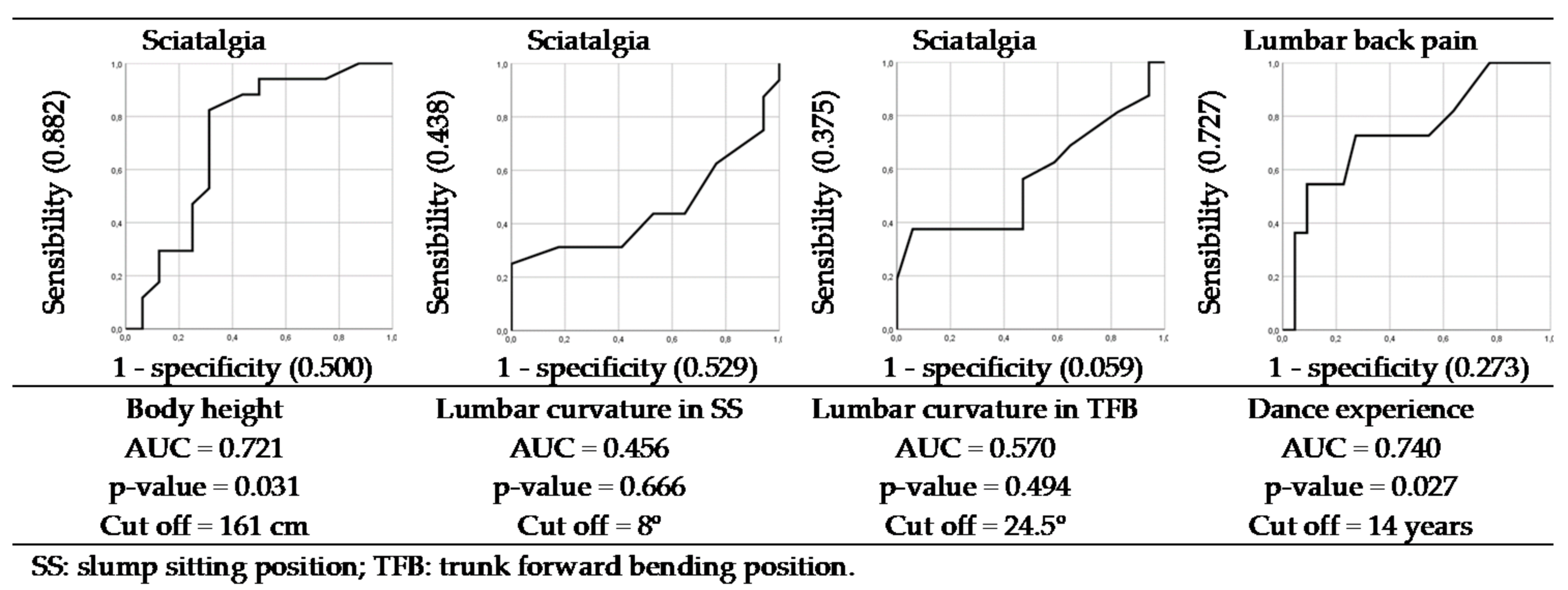
3. Results
4. Discussion
Practical Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gamboa, J.; Maring, J.; Gamboa, J. Injury Patterns in Elite Preprofessional Ballet Dancers and the Utility of Screening Programs to Identify Risk Characteristics. J. Orthop. Sports Phys. Ther. 2008, 126, 126–136. [Google Scholar] [CrossRef]
- Steinberg, N.; Siev-Ner, I.; Peleg, S.; Dar, G.; Masharawi, Y. Injury patterns in young, non-professional dancers. J. Sports Sci. 2011, 29, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Gildea, J.; Hides, J.; Hodges, P. Size and symmetry of trunk muscles in ballet dancers with and without low back pain. J. Orthop. Sports Phys. Ther. 2013, 43, 525–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinberg, N.; Hershkovitz, I.; Peleg, S.; Dar, G.; Masharawi, Y.; Heim, M.; Siev-Ner, I. Range of joint movement in female dancers and nondancers aged 8 to 16 years: Anatomical and clinical implications. Am. J. Sports Med. 2006, 34, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Allen, N.; Nevill, A.; Brooks, J.; Koutedakis, Y.; Wyon, M. Ballet Injuries: Injury Incidence and Severity Over 1 Year. J. Orthop. Sports Phys. Ther. 2012, 42, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, C.; Leanderson, J.; Wykman, A.; Strender, L. The injury panorama in a Swedish professional ballet company. Knee Surg. Sports Traumatol. Arthrosc. 2001, 9, 242–246. [Google Scholar] [CrossRef]
- Capel, A.; Medina-Santonja, F.; Medina, D.; Gómez-Lozano, S. Magnetic resonance study of lumbar disks in female dancers. Am. J. Sports Med. 2009, 37, 1208–1213. [Google Scholar] [CrossRef] [PubMed]
- Swain, C.; Bradshaw, E.; Whyte, D.; Ekegren, C. The prevalence and impact of low back pain in pre-professional and professional dancers: A prospective study. Phys. Ther. Sport 2018, 30, 8–13. [Google Scholar] [CrossRef]
- Nilsson, C.; Wykman, A.; Leanderson, J. Spinal sagittal mobility and joint laxity in young ballet dancers—A comparative study between first-year students at the Swedish Ballet School and a control group. Knee Surg. Sports Traumatol. Arthrosc. 1993, 1, 206–208. [Google Scholar] [CrossRef]
- Gómez-Lozano, S. Spinal Sagittal Study in Ballet and Spanish-Dance Female Dancers; University of Murcia: Murcia, Spain, 2007. [Google Scholar]
- Santonja-Medina, F.; Gómez-Lozano, S.; Baena-Chicón, I.; Vargas-Macías, A. Spinal sagittal mobility in female classical ballet dancers. Rev. Cent. Investig. Flamenco Telethusa 2020, 13, 10–19. [Google Scholar] [CrossRef]
- Ambegaonkar, J.; Caswell, A.; Kenworthy, K.; Cortes, N.; Caswell, S. Lumbar lordosis in female collegiate dancers and gymnasts. Med Probl. Perform. Artist. 2014, 29, 189–192. [Google Scholar] [CrossRef]
- Sainz de Baranda, P.; Cejudo, A.; Moreno-Alcaraz, V.; Martinez-Romero, M.; Aparicio-Sarmiento, A.; Santonja, F. Sagittal spinal morphotype assessment in 8 to 15 years old Inline Hockey players. PeerJ 2020, 8, e8229. [Google Scholar] [CrossRef] [Green Version]
- Hecimovich, M.; Stomski, N. Lumbar sagittal plane spinal curvature and junior-level cricket players. Int. J. Athl. Ther. Train. 2016, 21, 47–52. [Google Scholar] [CrossRef]
- Alricsson, M.; Björklund, G.; Cronholm, M.; Olsson, O.; Viklund, P.; Svantesson, U. Spinal alignment, mobility of the hip and thoracic spine and prevalence of low back pain in young elite cross-country skiers. J. Exerc. Rehabil. 2016, 12, 21. [Google Scholar] [CrossRef] [Green Version]
- Peterson, F.; Kendall, E.; Geise, P. Kendall’s Músculos. Pruebas, Funciones y Dolor Postural; Marbán: Madrid, Spain, 2005. [Google Scholar]
- Santonja-Medina, F.; Collazo-Diéguez, M.; Martínez-Romero, M.; Rodríguez-Ferrán, O.; Aparicio-Sarmiento, A.; Cejudo, A.; Andújar, P.; Sainz De Baranda, P. Classification System of the Sagittal Integral Morphotype in Children from the ISQUIOS Programme (Spain). Int. J. Environ. Res. Public Health 2020, 17, 2467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swain, C.; Bradshaw, E.; Ekegren, C.; Whyte, D. The Epidemiology of Low Back Pain and Injury in Dance: A Systematic Review. J. Orthop. Sports Phys. Ther. 2019, 49, 239–252. [Google Scholar] [CrossRef] [Green Version]
- Cejudo, A.; Ginés-Díaz, A.; Rodríguez-Ferrán, O.; Santonja-Medina, F.; Sainz de Baranda, P. Trunk Lateral Flexor Endurance and Body Fat: Predictive Risk Factors for Low Back Pain in Child Equestrian Athletes. Children 2020, 7, 172. [Google Scholar] [CrossRef]
- Cejudo, A.; Moreno-Alcaraz, V.J.; Izzo, R.; Santonja-Medina, F.; Sainz de Baranda, P. External and Total Hip Rotation Ranges of Motion Predispose to Low Back Pain in Elite Spanish Inline Hockey Players. Int. J. Environ. Res. Public Health 2020, 17, 4858. [Google Scholar] [CrossRef] [PubMed]
- Dionne, C.; Dunn, K.; Croft, P.; Nachemson, A.; Buchbinder, R.; Walker, B.; Wyatt, M.; Cassidy, J.; Rossignol, M.; Leboeuf-Yde, C.; et al. A Consensus Approach Toward the Standardization of Back Pain Definitions for Use in Prevalence Studies. Spine 2008, 33, 95–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santonja-Medina, F.; Pastor, A.; Serna, L. X-Ray diagnosis of sagittal alignment of spine. Selección 2000, 9, 216–229. [Google Scholar]
- Ferrer, V. Repercusiones de la Cortedad Isquiosural Sobre la Pelvis y el Raquis Lumbar; Universidad de Murcia: Murcia, Spain, 1998. [Google Scholar]
- Coombes, B.; Bisset, L.; Vicenzino, B. Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: A systematic review of randomised controlled trials. Lancet 2010, 376, 1751–1767. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Cynn, H.S.; Yi, C.H.; Kwon, O.Y.; Yoon, T.L. Predictor variables for forward scapular posture including posterior shoulder tightness. J. Bodyw. Mov. Ther. 2015, 19, 253–260. [Google Scholar] [CrossRef]
- Janda, V. Muscle Function Testing; Butterworth-Heinemann, Ed.; Elsevier: London, UK, 2013. [Google Scholar]
- Janda, V. Evaluation of muscular imbalance. Rehabilitation of the spine: A practitioner’s manual. In Rehabillitation of the Spine: A Practitioner’s Manual; Liebenson, C.E., Ed.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 1996; pp. 97–112. [Google Scholar]
- Youdas, J.; Garrett, T.; Egan, K.; Therneau, T. Lumbar lordosis and pelvic inclination in adults with chronic low back pain. Phys. Ther. 2000, 80, 261–275. [Google Scholar] [CrossRef] [Green Version]
- Ginés-Díaz, A.; Martinez-Romero, M.; Cejudo, A.; Aparicio-Sarmiento, A.; Sainz de Baranda, P. Sagittal Spinal Morphotype Assessment in Dressage and Show Jumping Riders Physical. J. Sport Rehabil. 2019, 29, 533–540. [Google Scholar] [CrossRef]
- Sanz-Mengibar, J.; Sainz de Baranda, P.; Santonja-Medina, F. Training intensity and sagittal curvature of the spine in male and female artistic gymnasts. J. Sports Med. Phys. Fit. 2018, 58, 465–471. [Google Scholar] [CrossRef]
- Boyajian-O’Neill, L.; McClain, R.; Coleman, M.; Thomas, P. Diagnosis and management of piriformis syndrome: An osteopathic approach. J. Am. Osteopath. Assoc. 2008, 108, 657–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gottschlich, L.; Young, C. Spine injuries in dancers. Curr. Sports Med. Rep. 2011, 10, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Kirschner, J.; Foye, P.; Cole, J. Piriformis syndrome, diagnosis and treatment. Muscle Nerve 2009, 40, 10–18. [Google Scholar] [CrossRef]
- Orsello, C.; Phillips, A.; Rice, G. Height and in-flight low back pain association among military helicopter pilots. Aviat. Space Environ. Med. 2013, 84, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Heuch, I.; Heuch, I.; Hagen, K.; Zwart, J. A comparison of anthropometric measures for assessing the association between body size and risk of chronic low back pain: The HUNT study. PLoS ONE 2015, 10, e0141268. [Google Scholar] [CrossRef] [Green Version]
- Endo, T.; Abe, T.; Akai, K.; Kijima, T.; Takeda, M.; Yamasaki, M.; Isomura, M.; Nabika, T.; Yano, S. Height loss but not body composition is related to low back pain in community-dwelling elderlies: Shimane CoHRE study. BMC Musculoskelet. Disord. 2019, 20, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roussel, N.; Nijs, J.; Mottram, S.; Van Moorsel, A.; Truijen, S.; Stassijns, G. Altered lumbopelvic movement control but not generalized joint hypermobility is associated with increased injury in dancers. A prospective study. Man. Ther. 2009, 14, 630–635. [Google Scholar] [CrossRef]
- Roussel, N.; De Kooning, M.; Mottram, S.; Truijen, S. Motor Control and Low Back Pain in Dancers. Artic. Int. J. Sports Med. 2012, 34, 138–143. [Google Scholar] [CrossRef] [Green Version]
- Negus, V.; Hopper, D.; Briffa, N. Associations between turnout and lower extremity injuries in classical ballet dancers. J. Orthop. Sports Phys. Ther. 2005, 35, 307–318. [Google Scholar] [CrossRef]
- Khan, K.; Brown, J.; Way, S.; Vass, N.; Crichton, K.; Alexander, R.; Baxter, A.; Butler, M.; Wark, J. Overuse Injuries in Classical Ballet. Sports Med. 1995, 19, 341–357. [Google Scholar] [CrossRef] [PubMed]
- Coplan, J. Ballet dancer’s turnout and its relationship to self-reported injury. J. Orthop. Sports Phys. Ther. 2002, 32, 579–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moita, J.; Nunes, A.; Esteves, J.; Oliveira, R.; Xarez, L. The relationship between muscular strength and dance injuries: A systematic review. Med. Probl. Perform. Artist. 2017, 32, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Cupisti, A.; D’Alessandro, C.; Evangelisti, I.; Piazza, M.; Galetta, F.; Morelli, E. Low back pain in competitive rhythmic gymnasts. J. Sports Med. Phys. Fit. 2004, 44, 49–53. [Google Scholar]
- Sainz de Baranda, P.; Santonja-Medina, F.; Rodríguez-Iniesta, M. Tiempo de entrenamiento y plano sagital del raquis en gimnastas de trampolín. Rev. Int. De Med. Y Cienc. De La Act. Física Y El Deporte 2010, 10, 521–536. [Google Scholar]
- Sainz-de-Baranda, P.; Santonja-Medina, F.; Rodríguez-Iniesta, M. Valoración de la disposición sagital del raquis en gimnastas especialistas en trampolín. (Assessment of the sagittal plane of the spine in trampoline gymnasts.). Ricyde. Rev. Int. De Cienc. Del Deporte 2009, 5, 21–33. [Google Scholar] [CrossRef]
- Okamura, S.; Wada, N.; Tazawa, M.; Sohmiya, M.; Ibe, Y.; Shimizu, T.; Usuda, S.; Shirakura, K. Injuries and disorders among young ice skaters: Relationship with generalized joint laxity and tightness. Open Access J. Sports Med. 2014, 5, 191–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeMann, L., Jr. Piriformis involvement in dancers with low back pain—a conservative approach. J. Back Musculoskelet. Rehabil. 1995, 5, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, D.; Peng, P.; Van Zundert, A. Brief review: Piriformis syndrome: Etiology, diagnosis, and management. Can. J. Anesth. 2013, 60, 1003–1012. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Minimum Value | Maximum Value | Total Value 1 |
|---|---|---|---|
| Age (years) | 16.0 | 31.0 | 22.0 ± 3.8 |
| Body mass (kg) | 43.5 | 59.6 | 51.9 ± 4.4 |
| Stature (cm) | 150.0 | 170.5 | 161.7 ± 4.5 |
| Body mass index (kg/m2) | 16.3 | 23.1 | 19.9 ± 1.7 |
| Dance experience (years) | 8.0 | 23.0 | 13.4 ± 4.0 |
| Classical ballet dance experience (years) | 4.0 | 23.0 | 8.8 ± 5.4 |
| Variable | Position | Category 1 | Total Value | N 2 | % 3 |
|---|---|---|---|---|---|
| Thoracic curvature | RS | Hypokyphosis (<20°) | 14.0 ± 5.7 | 2 | 6.1 |
| Normal (20 to 40°) | 29.2 ± 6.8 | 31 | 93.9 | ||
| Hyperkyphosis (≥41°) | − | − | − | ||
| SS | Hypokyphosis (<20°) | 14.4 ± 2.9 | 5 | 15.2 | |
| Normal (20 to 40°) | 32.8 ± 5.9 | 22 | 66.7 | ||
| Hyperkyphosis (≥41°) | 49.8 ± 6.7 | 6 | 18.2 | ||
| TFB | Hypokyphosis (<40°) | 32.8 ± 4.0 | 6 | 18.2 | |
| Normal (40° to 65°) | 51.5 ± 7.3 | 24 | 72.7 | ||
| Hyperkyphosis (≥66°) | 69.0 ± 1.7 | 3 | 9.1 | ||
| Lumbar curvature | RS | Hypolordosis (<−20°) | − | − | − |
| Normal (−20° to −40°) | −33.1 ± −5.0 | 27 | 81.8 | ||
| Hyperlordosis (>−40°) | −44.3 ± 0.8 | 6 | 18.2 | ||
| SS | Hypokyphosis (<−15°) | − | − | − | |
| Normal (−15° to 15°) | 6.8 ± 5.3 | 29 | 87.9 | ||
| Hyperkyphosis (>15°) | 19.3 ± 1.5 | 4 | 12.1 | ||
| TFB | Hypokyphosis (<10°) | − | − | − | |
| Normal (10° to 30°) | 19.0 ± 5.1 | 31 | 93.9 | ||
| Hyperkyphosis (>30°) | 32.0 ± 0.0 | 2 | 6.1 |
| Thoracic SIM 1 | Position | N 2 | % 3 | |||
|---|---|---|---|---|---|---|
| Category | Subcategory | RS | SS | TFB | ||
| Normal Kyphosis | Normal (20° to 40°) | Normal (20° to 40°) | Normal (40° to 65°) | 17 | 51.5 | |
| Hypokyphosis or hypokyphosis attitude | Dynamic | Hypokyphosis (<20°) | Normal (20° to 40°) | Hypokyphosis (<40°) | 3 | 9.1 |
| Hypomobile kyphosis | Normal (20° to 40°) | Normal (20° to 40°) | Hypokyphosis (<40°) | 4 | 12.1 | |
| Functional hyperkyphosis | Static | Normal (20° to 40°) | Hyperkyphosis (>40°) | Normal (40° to 65°) | 6 | 18.2 |
| Dynamic | Normal (20° to 40°) | Normal (20° to 40°) | Hyperkyphosis (>65°) | 2 | 6.1 | |
| Total | Normal (20° to 40°) | Hyperkyphosis (>40°) | Hyperkyphosis (>65°) | 1 | 3 | |
| Lumbar SIM 1 | Position | N 2 | % 3 | |||
|---|---|---|---|---|---|---|
| Category | Subcategory | RS | SS | TFB | ||
| Normal lumbar curve | Normal (−20° to −40°) | Normal (−15° to 15°) | Normal (10° to 30°) | 23 | 69.7 | |
| Hyperlordotic attitude | Hyperlordosis (>−40° ) | Normal (−15° to −15° ) | Normal (10° to 30° ) | 6 | 18.2 | |
| Functional lumbar hyperkyphosis | Static | Normal (−20° to −40°) | Hyperkyphosis (>15°) | Normal (10° to 30°) | 2 | 6.1 |
| Total | Normal (−20° to −40°) | Hyperkyphosis (>15°) | Hyperkyphosis (>30°) | 2 | 6.1 | |
| Method Sample | Risk Factors | OR 1 | SE | 95% CI | p-Value | |
|---|---|---|---|---|---|---|
| Enter Regression | LC in SS | 1.420 Medium | 0.174 | 0.500 to 0.989 | 0.043 | |
| ≥8° 1 | <8° | |||||
| Asymptomatic (n = 17) | 52.9% | 47.1% | ||||
| Sciatica (n = 16) | 62.5% | 37.5% | ||||
| Enter Regression | LC in TFB | 1.623 Medium | 0.245 | 1.003 to 2.626 | 0.048 | |
| ≥24.5° 1 | <24.5° | |||||
| Asymptomatic (n = 17) | 5.9% | 94.1% | ||||
| Sciatica (n = 16) | 62.5% | 37.5% | ||||
| Stepwise Regression | Stature | |||||
| ≤161 cm 1 | >161 cm | 1.232 Small | 0.102 | 0.664 to 0.992 | 0.042 | |
| Asymptomatic (n = 17) | 64.7% | 35.3% | ||||
| Sciatica (n = 16) | 75.0% | 25.0% | ||||
| Stepwise Regression | Dance experience | 1.250 Medium | 0.038 | |||
| ≥14 y 1 | <14 y | 0.107 | 1.012 to 1.543 | |||
| Asymptomatic (n = 22) | 31.6% | 68.4% | ||||
| Low back pain (n = 11) | 72.7% | 27.3% | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cejudo, A.; Gómez-Lozano, S.; Sainz de Baranda, P.; Vargas-Macías, A.; Santonja-Medina, F. Sagittal Integral Morphotype of Female Classical Ballet Dancers and Predictors of Sciatica and Low Back Pain. Int. J. Environ. Res. Public Health 2021, 18, 5039. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18095039
Cejudo A, Gómez-Lozano S, Sainz de Baranda P, Vargas-Macías A, Santonja-Medina F. Sagittal Integral Morphotype of Female Classical Ballet Dancers and Predictors of Sciatica and Low Back Pain. International Journal of Environmental Research and Public Health. 2021; 18(9):5039. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18095039
Chicago/Turabian StyleCejudo, Antonio, Sebastián Gómez-Lozano, Pilar Sainz de Baranda, Alfonso Vargas-Macías, and Fernando Santonja-Medina. 2021. "Sagittal Integral Morphotype of Female Classical Ballet Dancers and Predictors of Sciatica and Low Back Pain" International Journal of Environmental Research and Public Health 18, no. 9: 5039. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18095039