
Birth Experience, Postpartum PTSD and Depression before and during the Pandemic of COVID-19 in Russia

Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedure and Participants
2.2. Ethical Considerations
2.3. Measures
2.3.1. The Demographic, Pregnancy and Childbirth Experience Questionnaire
- episiotomy
- amniotomy
- use of synthetic oxytocin
- epidural anesthesia
- medical interventions without patient’s consent and approval
- verbal aggression and bullying
- physical aggression (immobilization, forbiddance to drink)
- threats and accusations
- Kristeller maneuver
- pain relief denial
- ignoring the needs of the birthing woman
2.3.2. The City Birth Trauma Scale (CBTS)
2.3.3. Edinburgh Postnatal Depression Scale (EPDS)
2.3.4. Covariates
2.4. Statistical Analysis
3. Results
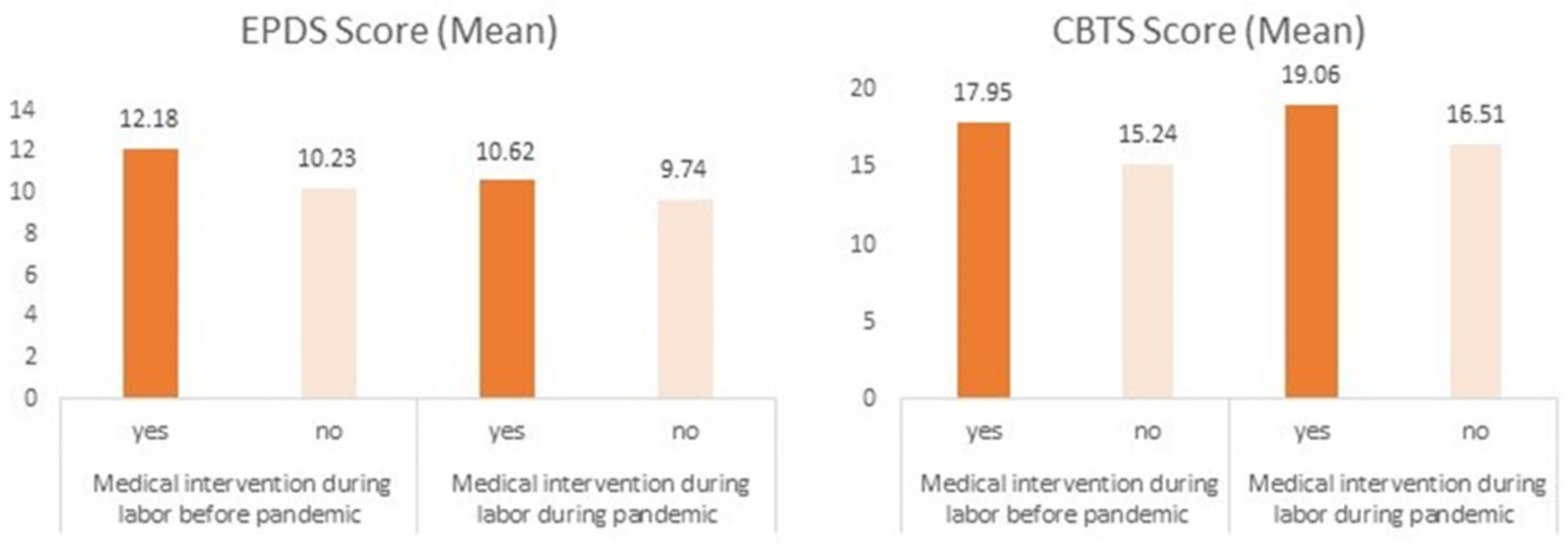
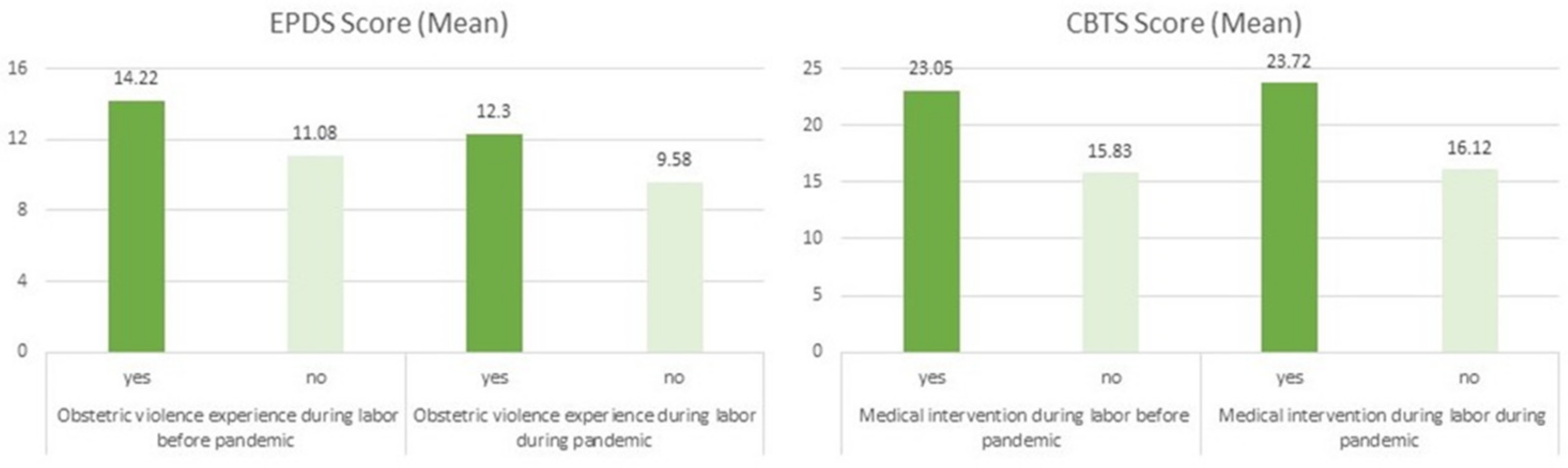
3.1. Medical Interventions and Obstetric Violence Experience
3.2. Postpartum Depressive and PTSD Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Пoстанoвления Главнoгo Гoсударственнoгo Санитарнoгo Врача Рoссийскoй Φедерации (Resolution of the Chief Sanitary Doctor of the Russian Federation). Available online: https://rospotrebnadzor.ru/ (accessed on 23 November 2021).
- Ozhiganova, A.A.; Molodczova, M.O. The childbirth in quarantine reality: The doula’s position. Med. Anthropol. Bioeth. 2020, 1, 158–173. [Google Scholar] [CrossRef]
- Mayopoulos, G.A.; Ein-Dor, T.; Dishy, G.A.; Nandru, R.; Chan, S.J.; Hanley, L.E.; Kaimal, A.J.; Dekel, S. COVID-19 is associated with traumatic childbirth and subsequent mother-infant bonding problems. J. Affect. Disord. 2021, 282, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Mariño-Narvaez, C.; Puertas-Gonzalez, J.A.; Romero-Gonzalez, B.; Peralta-Ramirez, M.I. Giving birth during the COVID-19 pandemic: The impact on birth satisfaction and postpartum depression. Int. J. Gynaecol. Obstet. 2021, 153, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Mollard, E.; Kupzyk, K.; Moore, T. Postpartum stress and protective factors in women who gave birth in the United States during the COVID-19 pandemic. Women’s Health 2021, 17, 17455065211042190. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.H.; Erdei, C.; Mittal, L. Risk factors for depression, anxiety, and PTSD symptoms in perinatal women during the COVID-19 Pandemic. Psychiatry Res. 2021, 295, 113552. [Google Scholar] [CrossRef] [PubMed]
- Stampini, V.; Monzani, A.; Caristia, S.; Ferrante, G.; Gerbino, M.; De Pedrini, A.; Amadori, R.; Rabbone, I.; Surico, D. The perception of Italian pregnant women and new mothers about their psychological wellbeing, lifestyle, delivery, and neonatal management experience during the COVID-19 pandemic lockdown: A web-based survey. BMC Pregnancy Childbirth 2021, 21, 473. [Google Scholar] [CrossRef]
- Rice, K.; Williams, S. Women’s postpartum experiences in Canada during the COVID-19 pandemic: A qualitative study. CMAJ Open 2021, 9, E556–E562. [Google Scholar] [CrossRef]
- Sweet, L.; Wilson, A.N.; Bradfield, Z.; Hauck, Y.; Kuliukas, L.; Homer, C.S.E.; Szabo, R.A.; Wynter, K.; Vasilevski, V. Childbearing women’s experiences of the maternity care system in Australia during the first wave of the COVID-19 pandemic. Women Birth, 2021; in press. [Google Scholar] [CrossRef]
- Janevic, T.; Maru, S.; Nowlin, S.; McCarthy, K.; Bergink, V.; Stone, J.; Dias, J.; Wu, S.; Howell, E.A. Pandemic Birthing: Childbirth Satisfaction, Perceived Health Care Bias, and Postpartum Health During the COVID-19 Pandemic. Matern. Child Health J. 2021, 25, 860–869. [Google Scholar] [CrossRef]
- Basu, A.; Kim, H.H.; Basaldua, R.; Choi, K.W.; Charron, L.; Kelsall, N.; Hernandez-Diaz, S.; Wyszynski, D.F.; Koenen, K.C. A cross-national study of factors associated with women’s perinatal mental health and wellbeing during the COVID-19 pandemic. PLoS ONE 2021, 16, e0249780. [Google Scholar] [CrossRef]
- Yakupova, V.A.; Suarez, А. Postpartum Depression and Birth Experience in Russia. Psychology in Russia. State Art 2021, 14, 28–38. [Google Scholar] [CrossRef]
- Simpson, M.; Catling, C. Understanding psychological traumatic birth experiences: A literature review. Women Birth 2016, 29, 203–207. [Google Scholar] [CrossRef] [PubMed]
- De Schepper, S.; Vercauteren, T.; Tersago, J.; Jacquemyn, Y.; Raes, F.; Franck, E. Post-Traumatic Stress Disorder after childbirth and the influence of maternity team care during labour and birth: A cohort study. Midwifery 2016, 32, 87–92. [Google Scholar] [CrossRef]
- Dikmen-Yildiz, P.; Ayers, S.; Phillips, L. Longitudinal trajectories of post-traumatic stress disorder (PTSD) after birth and associated risk factors. J. Affect. Disord. 2018, 229, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Barthel, D.; Göbel, A.; Barkmann, C.; Helle, N.; Bindt, C. Does Birth-Related Trauma Last? Prevalence and Risk Factors for Posttraumatic Stress in Mothers and Fathers of VLBW Preterm and Term Born Children 5 Years After Birth. Front. Psychiatry 2020, 11, 575429. [Google Scholar] [CrossRef]
- Molloy, E.; Biggerstaff, D.L.; Sidebotham, P. A phenomenological exploration of parenting after birth trauma: Mothers perceptions of the first year. Women Birth 2021, 34, 278–287. [Google Scholar] [CrossRef]
- Garthus-Niegel, S.; Ayers, S.; von Soest, T.; Torgersen, L.; Eberhard-Gran, M. Maintaining factors of posttraumatic stress symptoms following childbirth: A population-based, two-year follow-up study. J. Affect. Disord. 2015, 172, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Ayers, S.; Wright, D.B.; Thornton, A. Development of a Measure of Postpartum PTSD: The City Birth Trauma Scale. Front. Psychiatry 2018, 9, 409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yakupova, V.A. Diagnosis of PTSD after childbirth. Adaptation of the postpartum PTSD scale in the Russian sample. Вестн. Практ. Психoл. 2020, 2, 111–116. [Google Scholar]
- American Psychiatric Association, DSM-5 Task Force. Diagnostic and Statistical Manual of Mental Disorders: DSM-5™, 5th ed.; American Psychiatric Publishing Inc.: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Diagnostic and Statistical Manual of Mental Disorders: DSM-IV; American Psychiatric Association: Washington, DC, USA, 1994.
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression: Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [Green Version]
- Yakupova, V. The Impact of Psychological and Physiological Conditions of Motherhood on Post- natal Depression. Russ. J. Psychol. 2018, 15, 8–23. [Google Scholar] [CrossRef] [Green Version]
- Fiorillo, A.; Sampogna, G.; Giallonardo, V.; Del Vecchio, V.; Luciano, M.; Albert, U.; Carmassi, C.; Carrà, G.; Cirulli, F.; Dell’Osso, B.; et al. Effects of the lockdown on the mental health of the general population during the COVID-19 pandemic in Italy: Results from the COMET collaborative network. Eur. Psychiatry 2020, 63, e87. [Google Scholar] [CrossRef]
- Yildiz, P.D.; Ayers, S.; Phillips, L. The prevalence of posttraumatic stress disorder in pregnancy and after birth: A systematic review and meta-analysis. J. Affect. Disord. 2017, 208, 634–645. [Google Scholar] [CrossRef] [PubMed]
- Temkina, А. Medicalization of Reproduction and Childbirth: The Struggle for Control. J. Soc. Policy Res. 2014, 12, 321–336. [Google Scholar]
- Türkmen, H.; Yalniz Dilcen, H.; Akin, B. The Effect of Labor Comfort on Traumatic Childbirth Perception, Post-Traumatic Stress Disorder, and Breastfeeding. Breastfeed. Med. 2020, 15, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Wigert, H.; Nilsson, C.; Dencker, A.; Begley, C.; Jangsten, E.; Sparud-Lundin, C.; Mollberg, M.; Patel, H. Women’s experiences of fear of childbirth: A metasynthesis of qualitative studies. Int. J. Qual. Stud. Health Well-Being 2020, 15, 1704484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borozdina, E.; Novkunskaya, A. Patient-centered care in Russian maternity hospitals: Introducing a new approach through professionals’ agency. Health, 2020; in press. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Nurses’ burnout and associated risk factors during the COVID-19 pandemic: A systematic review and meta-analysis. J. Adv. Nurs. 2021, 77, 3286–3302. [Google Scholar] [CrossRef]
- Temkina, А.; Litvina, D.; Novkunskaya, А. Emotional styles in maternity hospitals in Russia: Juggling with rudeness and a smile. Emot. Soc. 2021, 3, 95–113. [Google Scholar] [CrossRef]
- Martinez-Vázquez, S.; Rodríguez-Almagro, J.; Hernández-Martínez, A.; Martínez-Galiano, J.M. Factors Associated with Postpartum Post-Traumatic Stress Disorder (PTSD) Following Obstetric Violence: A Cross-Sectional Study. J. Pers. Med. 2021, 11, 338. [Google Scholar] [CrossRef]
- Kountanis, J.A.; Kirk, R.; Handelzalts, J.E.; Jester, J.M.; Kirk, R.; Muzik, M. The associations of subjective appraisal of birth pain and provider-patient communication with postpartum-onset PTSD. Arch. Women’s Ment. Health 2021. [Google Scholar] [CrossRef]
- Liu, C.; Koire, A.; Erdei, C.; Mittal, L. Unexpected changes in birth experiences during the COVID-19 pandemic: Implications for maternal mental health. Arch. Gynecol. Obstet. 2021. [Google Scholar] [CrossRef]
- Thurston, L.A.F.; Abrams, D.; Dreher, A.; Ostrowski, S.R.; Wright, J.C. Improving birth and breastfeeding outcomes among low resource women in Alabama by including doulas in the interprofessional birth care team. J. Interprof. Educ. Pract. 2019, 17, 100278. [Google Scholar] [CrossRef]
- LeFevre, N.M.; Krumm, E.; Cobb, W.J. Labor Dystocia in Nulliparous Women. Am. Fam. Physician 2007, 75, 1671–1678. [Google Scholar]
- Cooijmans, K.H.M.; Beijers, R.; Rovers, A.C.; de Weerth, C. Effectiveness of skin-to-skin contact versus care-as-usual in mothers and their full-term infants: Study protocol for a parallel-group randomized controlled trial. BMC Pediatr. 2017, 17, 154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ionio, C.; Ciuffo, G.; Landoni, M. Parent–Infant Skin-to-Skin Contact and Stress Regulation: A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2021, 18, 4695. [Google Scholar] [CrossRef] [PubMed]
- Kirca, N.; Adibelli, D. Effects of mother-infant skin-to-skin contact on postpartum depression: A systematic review. Perspect. Psychiatr. Care 2021, 57, 2014–2023. [Google Scholar] [CrossRef] [PubMed]
- Sadler, M.; Leiva, G.; Olza, I. COVID-19 as a risk factor for obstetric violence. Sex. Reprod. Health Matters 2020, 28, 1785379. [Google Scholar] [CrossRef]
- Viero, A.; Barbara, G.; Montisci, M.; Kustermann, K.; Cattaneo, C. Violence against women in the Covid-19 pandemic: A review of the literature and a call for shared strategies to tackle health and social emergencies. Forensic Sci. Int. 2020, 319, 110650. [Google Scholar] [CrossRef]
- Levis, B.; Negeri, Z.; Sun, Y.; Benedetti, A.; Thombs, B.D. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for screening to detect major depression among pregnant and postpartum women: Systematic review and meta-analysis of individual participant data. BMJ 2020, 371, 4022. [Google Scholar] [CrossRef]
- Smith-Nielsen, J.; Matthey, S.; Lange, T.; Væver, M.S. Validation of the Edinburgh Postnatal Depression Scale against both DSM-5 and ICD-10 diagnostic criteria for depression. BMC Psychiatry 2018, 18, 393. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Women Gave Birth before Pandemic (n = 611) | Women Gave Birth during Pandemic (n = 1645) | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| Mean/N | SD/% | Range | Mean/N | SD/% | Range | |||
| Age at testing (years) | 31.17 | 4.54 | 18–45 | 30.98 | 4.42 | 19–50 | 0.39 | |
| Education | Upper Secondary/College | 57 | 9.3% | 135 | 8.2% | 0.40 | ||
| Tertiary/University | 554 | 90.7% | 1510 | 91.8% | ||||
| Family Status | Married | 559 | 91.5% | 1547 | 94.0% | 0.024 | ||
| Cohabiting with a Partner | 33 | 5.4% | 74 | 4.5% | ||||
| Single | 19 | 3.1% | 24 | 1.5% | ||||
| Time After the Childbirth (Months) | 6.37 | 3.42 | 0.2–12 | 6.93 | 3.30 | 0–14 | <0.001 | |
| Gestational Age | 39.47 | 1.67 | 28.0–43.0 | 39.40 | 2.04 | 0–43.0 | 0.45 | |
| Delivery Mode | Vaginal | 472 | 77.4% | 1183 | 71.9% | 0.010 | ||
| Cesarean | 138 | 22.6% | 462 | 28.1% | ||||
| Place of Birth | Moscow and Capital Region | 224 | 36.7% | 403 | 24.6% | NA | ||
| Other city in Russia with population > 1 million | 262 | 43% | 583 | 35.6% | ||||
| Other city in Russia with population < 1 million | 461 | 28.2% | ||||||
| CIS Countries | 42 | 6.9% | 98 | 6.0% | ||||
| Europe/USA/Other | 82 | 13.4% | 91 | 5.6% | ||||
| Parity | 1 | 359 | 58.8% | 971 | 59% | 0.022 | ||
| 2 | 173 | 28.3% | 522 | 31.8% | ||||
| 3+ | 79 | 12.9% | 152 | 9.2% | ||||
| Type of childbirth plan | Birth in a specialized birth hospital under state insurance | 344 | 56.3% | 1020 | 62.0% | 0.020 | ||
| Birth in a specialized birth hospital with a contract for a hospital or medical team of choice | 250 | 40.9% | 598 | 36.4% | ||||
| Home birth | 17 | 2.8% | 27 | 1.6% | ||||
| Had at least one medical intervention during labor (yes) | 517 | 84.6% | 1386 | 84.3% | 0.90 | |||
| Number of medical interventions | 1.62 | 1.19 | 0–5 | 1.57 | 1.19 | 0–7 | 0.40 | |
| Types of medical interventions | Amniotomy | 279 | 45.7% | 687 | 41.8% | 0.10 | ||
| Epidural anaesthesia | 244 | 39.9% | 655 | 39.8% | 0.96 | |||
| Use of synthetic oxytocin | 230 | 37.6% | 541 | 32.9% | 0.036 | |||
| Episiotomy | 116 | 19.0% | 332 | 20.2% | 0.55 | |||
| Experienced at least one instance of obstetric violence during labor (yes) | 138 | 22.6% | 456 | 27.7% | 0.015 | |||
| Number of obstetric violence instances | 0.32 | 0.68 | 0–4 | 0.42 | 0.82 | 0–4 | 0.007 | |
| Types of obstetric violence instances | Verbal aggression and bullying | 69 | 11.3% | 257 | 15.6% | 0.009 | ||
| Medical interventions without consent | 38 | 6.2% | 137 | 8.3% | 0.11 | |||
| Physical aggression (immobilization, forbiddance to drink) | NA | NA | 19 | 1.2% | NA | |||
| Threats and accusations | 27 | 4.4% | 104 | 6.3% | 0.10 | |||
| Pain relief denial | 19 | 3.1% | 82 | 5.0% | 0.066 | |||
| Use of Kristeller manoeuvre | 19 | 3.1% | 79 | 4.8% | 0.082 | |||
| Ignoring the needs of the birthing woman | 18 | 2.9% | 15 | 0.9% | <0.001 | |||
| Support person at labor (yes) | 354 | 57.9% | 443 | 27.0% | <0.001 | |||
| Mode of birth support | No support | 257 | 42.1% | 1200 | 73.0% | <0.001 | ||
| Partner | 217 | 35.5% | 199 | 12.1% | ||||
| Doula/Private midwife | 74 | 12.1% | 178 | 10.8% | ||||
| Partner + doula/private midwife | 63 | 10.3% | 66 | 4.0% | ||||
| EPDS | 9.88 | 6.07 | 0–26 | 9.46 | 6.13 | 0–30 | 0.15 | |
| CBTS | 17.16 | 11.35 | 0–56 | 15.83 | 11.40 | 0–60 | 0.014 | |
| Confirmed COVID-19 | During pregnancy | NA | NA | 111 | 4.9% | NA | ||
| During labor | NA | NA | 35 | 1.6% | NA | |||
| Postpartum | NA | NA | 121 | 5.4% | NA | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yakupova, V.; Suarez, A.; Kharchenko, A. Birth Experience, Postpartum PTSD and Depression before and during the Pandemic of COVID-19 in Russia. Int. J. Environ. Res. Public Health 2022, 19, 335. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010335
Yakupova V, Suarez A, Kharchenko A. Birth Experience, Postpartum PTSD and Depression before and during the Pandemic of COVID-19 in Russia. International Journal of Environmental Research and Public Health. 2022; 19(1):335. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010335
Chicago/Turabian StyleYakupova, Vera, Anna Suarez, and Anna Kharchenko. 2022. "Birth Experience, Postpartum PTSD and Depression before and during the Pandemic of COVID-19 in Russia" International Journal of Environmental Research and Public Health 19, no. 1: 335. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010335