
Do Adults Who Practice Aerobic Physical Activities Have Different Influencing Factors for Depression: A Secondary Data Analysis


Abstract
:1. Introduction
2. Materials and Methods
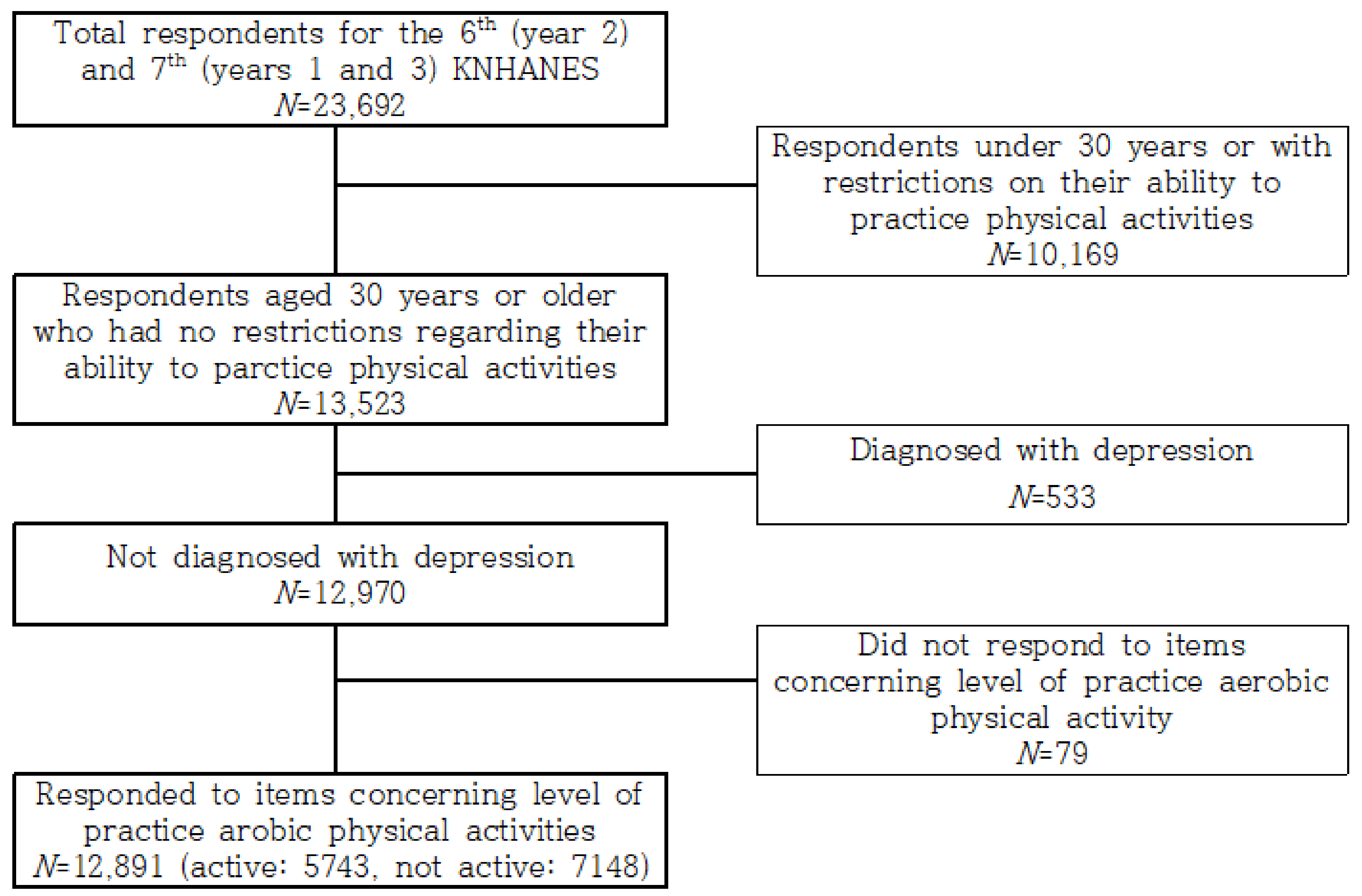
2.1. Participants and Procedure
2.2. Measures
2.2.1. Sociodemographic Factors
2.2.2. Physical Factors
2.2.3. Psychological Factors
2.3. Statistical Analysis
3. Results
3.1. Participants’ Sociodemographic Characteristics
3.2. Participants’ Health-Related Characteristics
3.3. Influencing Factors for Depression Depending on Aerobic Physical Activity Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Depression. Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 31 March 2022).
- Bąk, E.; Marcisz-Dyla, E.; Młynarska, A.; Sternal, D.; Kadłubowska, M.; Marcisz, C. Prevalence of depressive symptoms in patients with type 1 and 2 diabetes mellitus. Patient Prefer. Adherence 2020, 14, 443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, H.O.; Taylor, R.J.; Nguyen, A.W.; Chatters, L. Social isolation, depression, and psychological distress among older adults. J. Aging Health 2018, 30, 229–246. [Google Scholar] [CrossRef] [PubMed]
- Kwag, B.G.; Park, J.C.; Lee, W.; Chang, S.H.; Chun, D.H. The relationship between depression and health-related quality of life in Korean adult: Using 2014 Korea national health and nutrition examination survey data. Korean J. Fam. Pract. 2018, 8, 236–243. [Google Scholar] [CrossRef]
- Gilman, S.E.; Sucha, E.; Kingsbury, M.; Horton, N.J.; Murphy, J.M.; Colman, I. Depression and mortality in a longitudinal study: 1952–2011. Can. Med. Assoc. J. 2017, 189, E1304–E1310. [Google Scholar] [CrossRef] [Green Version]
- Bica, T.; Castelló, R.; Toussaint, L.L.; Montesó-Curto, P. Depression as a risk factor of organic diseases: An international integrative review. J. Nurs. Scholarsh. 2017, 49, 389–399. [Google Scholar] [CrossRef]
- Lee, S.U.; Park, J.K.; Lee, S.; Oh, I.H.; Choi, J.M.; Oh, C.M. Changing trends in suicide rates in South Korea from 1993 to 2016: A descriptive study. BMJ Open 2018, 8, e023144. [Google Scholar] [CrossRef] [Green Version]
- Magaard, J.L.; Seeralan, T.; Schulz, H.; Brütt, A.L. Factors associated with help-seeking behaviour among individuals with major depression: A systematic review. PLoS ONE 2017, 12, e0176730. [Google Scholar] [CrossRef]
- Ziser, K.; Finklenburg, C.; Behrens, S.C.; Giel, K.E.; Becker, S.; Skoda, E.M.; Teufel, M.; Mack, I.; Zipfel, S.; Junne, F. Perceived stress mediates the relationship of body image and depressive symptoms in individuals with obesity. Front. Psychiatry 2019, 10, 852. [Google Scholar] [CrossRef]
- Djernes, J.K. Prevalence and predictors of depression in populations of elderly: A review. Acta Psychiatr. Scand. 2006, 113, 372–387. [Google Scholar] [CrossRef]
- Schuch, F.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.; Reichert, T.; Bagatini, N.C.; Bgeginski, R.; Stubbs, B. Physical activity and sedentary behavior in people with major depressive disorder: A systematic review and meta-analysis. J. Affect. Disord. 2017, 210, 139–150. [Google Scholar] [CrossRef] [Green Version]
- Schuch, F.B.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.B.; Silva, E.S.; Hallgren, M.; Ponce De Leon, A.; Dunn, A.L.; Deslandes, A.C.; et al. Physical activity and incident depression: A meta-analysis of prospective cohort studies. Am. J. Psychiatry 2018, 7, 631–648. [Google Scholar] [CrossRef]
- Song, J.; Liu, Z.Z.; Huang, J.; Wu, J.S.; Tao, J. Effects of aerobic exercise, traditional Chinese exercises, and meditation on depressive symptoms of college student: A meta-analysis of randomized controlled trials. Medicine 2021, 100, e23819. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health. Available online: https://www.who.int/publications/i/item/9789241599979 (accessed on 10 May 2022).
- Bennie, J.A.; Teychenne, M.J.; De Cocker, K.; Biddle, S.J. Associations between aerobic and muscle-strengthening exercise with depressive symptom severity among 17,839 US adults. Prev. Med. 2019, 121, 121–127. [Google Scholar] [CrossRef]
- Clemente-Suárez, V.J. Multidisciplinary intervention in the treatment of mixed anxiety and depression. Physiol. Behav. 2020, 219, 112858. [Google Scholar] [CrossRef]
- Cangin, C.; Harris, R.; Binkley, P.; Schwartzbaum, J.; Focht, B. Anaerobic muscle strengthening physical activity and depression severity among USA adults. Prev. Med. Rep. 2018, 10, 299–303. [Google Scholar] [CrossRef]
- Byeon, H. Relationship between physical activity level and depression of elderly people living alone. Int. J. Environ. Res. Public Health 2019, 16, 4051. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.; Kwak, S.G.; Ko, E.J.; Chang, M.C. The mental health burden of the COVID-19 pandemic on physical therapists. Int. J. Environ. Res. Public Health 2020, 17, 3723. [Google Scholar] [CrossRef]
- Lee, J. Trajectories of depression between 30s and 50s: Latent growth modeling. Issues Ment. Health Nurs. 2020, 41, 624–636. [Google Scholar] [CrossRef]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea national health and nutrition examination survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Patient Health Questionnaire Primary Care Study Group. Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C. Epidemiology of women and depression. J. Affect. Disord. 2003, 74, 5–13. [Google Scholar] [CrossRef]
- Health Insurance Review & Assessment Service. Healthcare Bigdata Hub. Available online: http://opendata.hira.or.kr/op/opc/olapMfrnIntrsIlnsInfo.do (accessed on 31 March 2022).
- Kennedy, T.; Rae, M.; Sheridan, A.; Valadkhani, A. Reducing gender wage inequality increases economic prosperity for all: Insights from Australia. Econ. Anal. Policy 2017, 55, 14–24. [Google Scholar] [CrossRef]
- Organisation for Economic Co-operation and Development. The Pursuit of Gender Equality: An Uphill Battle; OECD Publishing: Paris, France, 2017. [Google Scholar]
- Debowska, A.; Horeczy, B.; Boduszek, D.; Dolinski, D. A repeated cross-sectional survey assessing university students’ stress, depression, anxiety, and suicidality in the early stages of the COVID-19 pandemic in Poland. Psychol. Med. 2020, 1–4. [Google Scholar] [CrossRef]
- Xue, Y.; Lu, J.; Zheng, X.; Zhang, J.; Lin, H.; Qin, Z.; Zhang, C. The relationship between socioeconomic status and depression among the older adults: The mediating role of health promoting lifestyle. J. Affect. Disord. 2021, 285, 22–28. [Google Scholar] [CrossRef]
- Tracy, M.; Zimmerman, F.J.; Galea, S.; McCauley, E.; Vander Stoep, A. What explains the relation between family poverty and childhood depressive symptoms? J. Psychiatr. Res. 2008, 42, 1163–1175. [Google Scholar] [CrossRef]
- Jadhav, A.; Weir, D. Widowhood and depression in a cross-national perspective: Evidence from the United States, Europe, Korea, and China. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2018, 73, e143–e153. [Google Scholar] [CrossRef]
- Ruggles, K.V.; Fang, Y.; Tate, J.; Mentor, S.M.; Bryant, K.J.; Fiellin, D.A.; Braithwaite, R.S. What are the patterns between depression, smoking, unhealthy alcohol use, and other substance use among individuals receiving medical care? A longitudinal study of 5479 participants. AIDS Behav. 2017, 21, 2014–2022. [Google Scholar] [CrossRef]
- Chang-Quan, H.; Xue-Mei, Z.; Bi-Rong, D.; Zhen-Chan, L.; Ji-Rong, Y.; Qing-Xiu, L. Health status and risk for depression among the elderly: A meta-analysis of published literature. Age Ageing 2010, 39, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Padayachey, U.; Ramlall, S.; Chipps, J. Depression in older adults: Prevalence and risk factors in a primary health care sample. S. Afr. Fam. Pract. 2017, 59, 61–66. [Google Scholar] [CrossRef] [Green Version]
- Eli, B.; Cheng, J.; Liang, Y.M. Posttraumatic stress disorder and depression prevalence among enterprise employees after an accident disaster. China J. Public Health 2018, 34, 1355–1359. [Google Scholar]
- Seo, E.H.; Kim, S.G.; Kim, S.H.; Kim, J.H.; Park, J.H.; Yoon, H.J. Life satisfaction and happiness associated with depressive symptoms among university students: A cross-sectional study in Korea. Ann. Gen. Psychiatry 2018, 17, 52. [Google Scholar] [CrossRef] [PubMed]
- Han, J.W.; Kim, D.J. Longitudinal relationship study of depression and self-esteem in postnatal Korean women using autoregressive cross-lagged modeling. Int. J. Environ. Res. Public Health 2020, 17, 3743. [Google Scholar] [CrossRef] [PubMed]
- Paquette, M.C.; Raine, K. Sociocultural context of women’s body image. Soc. Sci. Med. 2004, 59, 1047–1058. [Google Scholar] [CrossRef] [PubMed]
- Lavretsky, H.; Kumar, A. Practical geriatrics: Clinically significant nonmajor geriatric depression. Psychiatr. Serv. 2003, 54, 297–299. [Google Scholar] [CrossRef] [PubMed]
- Beautrais, A.L. Suicide and serious suicide attempts in youth: A multiple-group comparison study. Am. J. Psychiatry 2003, 160, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Primack, B.A.; Shensa, A.; Escobar-Viera, C.G.; Barrett, E.L.; Sidani, J.E.; Colditz, J.B.; James, A.E. Use of multiple social media platforms and symptoms of depression and anxiety: A nationally-representative study among U.S. young adults. Comput. Hum. Behav. 2017, 69, 1–9. [Google Scholar] [CrossRef]
- Yeung, W.J.J.; Yang, Y. Labor Market Uncertainties for Youth and Young Adults: An International Perspective. Ann. Am. Acad. Political Soc. Sci. 2020, 688, 7–19. [Google Scholar] [CrossRef]
- Strandh, M.; Winefield, A.; Nilsson, K.; Hammarström, A. Unemployment and mental health scarring during the life course. Eur. J. Public Health 2014, 24, 440–445. [Google Scholar] [CrossRef]
- Paul, K.I.; Moser, K. Unemployment impairs mental health: Meta-analyses. J. Vocat. Behav. 2009, 74, 264–282. [Google Scholar] [CrossRef]
- Lee, J. Pathways from education to depression. J. Cross Cult. Gerontol. 2011, 26, 121–135. [Google Scholar] [CrossRef]
- Dave, D.; Rashad, I.; Spasojevic, J. The Effects of Retirement on Physical and Mental Health Outcomes; NBER Working Paper Series, Working Paper 12123; National Bureau of Economic Research: Cambridge, MA, USA, 2006. [Google Scholar]


{kind=link}
| Characteristics | Total n (Weight %) | No Aerobic Physical Activity n (Weighted %) | Aerobic Physical Activity n (Weighted %) | χ2 (p) | |
|---|---|---|---|---|---|
| Gender | Men | 5702 (50.2) | 2986 (47.6) | 2716 (53.2) | 40.513 (<0.001) |
| Women | 7189 (49.8) | 4162 (52.4) | 3027 (46.8) | ||
| Age (years) | 30–49 | 5443 (50.0) | 2731 (45.8) | 2712 (54.7) | 170.662 (<0.001) |
| 50–64 | 4098 (32.7) | 2265 (33.2) | 1833 (32.2) | ||
| ≥65 | 3350 (17.3) | 2152 (21.0) | 1198 (13.1) | ||
| Family income | Upper | 3771 (31.5) | 1844 (27.8) | 1927 (35.7) | 150.693 (<0.001) |
| Middle | 6896 (55.1) | 3852 (56.1) | 3044 (54.1) | ||
| Lower | 2188 (13.4) | 1426 (16.1) | 762 (10.2) | ||
| Education level | ≤Middle school | 4156 (26.1) | 2744 (32.1) | 1412 (19.2) | 293.818 (<0.001) |
| High school | 3920 (32.6) | 2064 (31.2) | 1856 (34.2) | ||
| ≥College | 4784 (41.3) | 2319 (36.7) | 2465 (46.6) | ||
| Number of household members | 1 | 1346 (8.6) | 819 (9.2) | 527 (7.9) | 33.348 (<0.001) |
| 2 | 3908 (25.8) | 2281 (27.5) | 1627 (23.9) | ||
| ≥3 | 7637 (65.6) | 4048 (63.3) | 3589 (68.2) | ||
| Housing type | Detached house | 4248 (31.3) | 2552 (33.4) | 1696 (29.0) | 32.649 (<0.001) |
| Apartment | 7122 (55.7) | 3744 (53.5) | 3378 (58.1) | ||
| Other | 1521 (13.0) | 852 (13.1) | 669 (12.9) | ||
| Marital status | Living with spouse | 10,303 (87.7) | 5626 (85.4) | 4677 (90.4) | 68.653 (<0.001) |
| Other | 1740 (12.3) | 1135 (14.6) | 605 (9.6) | ||
| Characteristics | Total n (Weight %)/M (SE) | No Aerobic Physical Activity n (Weight %)/M (SE) | Aerobic Physical Activity n (Weight %)/M (SE) | χ2/t (p) | |
|---|---|---|---|---|---|
| Blood pressure | Normal | 5346 (43.7) | 2800 (41.4) | 2546 (46.3) | 59.253 (<0.001) |
| Prehypertension | 3145 (25.8) | 1677 (25.2) | 1468 (26.4) | ||
| Hypertension | 4364 (30.5) | 2656 (33.4) | 1708 (27.3) | ||
| Body weight | Underweight | 381 (3.4) | 231 (4.0) | 150 (2.7) | 13.852 (0.001) |
| Normal | 6844 (61.2) | 3678 (60.4) | 3166 (62.1) | ||
| Obese | 3922 (35.4) | 2168 (35.6) | 1754 (35.2) | ||
| Diabetes status | Normal | 7301 (61.9) | 3881 (59.9) | 3420 (64.2) | 27.945 (<0.001) |
| Impaired fasting glucose | 3148 (26.7) | 1773 (27.5) | 1375 (25.6) | ||
| Diabetes | 1565 (11.4) | 961 (12.6) | 604 (10.2) | ||
| Hypercholesterolemia status | No hypercholesterolemia | 9423 (80.0) | 5119 (79.0) | 4304 (81.1) | 8.583 (0.004) |
| Hypercholesterolemia | 2604 (20.0) | 1505 (21.0) | 1099 (18.9) | ||
| Weight change | Increased | 2716 (22.1) | 1494 (22.2) | 1222 (22.0) | 0.045 (0.975) |
| Decreased | 1519 (12.1) | 841 (12.1) | 678 (12.2) | ||
| No change | 8573 (65.8) | 4752 (65.7) | 3821 (65.8) | ||
| Weight control | Made efforts to reduce | 5108 (41.0) | 2550 (36.7) | 2558 (45.9) | 292.777 (<0.001) |
| Made efforts to Maintain | 2412 (18.8) | 1165 (16.4) | 1247 (21.6) | ||
| Made efforts to increase | 605 (4.7) | 344 (4.8) | 261 (4.4) | ||
| Made no efforts | 4700 (35.5) | 3041 (42.1) | 1659 (28.1) | ||
| Drinking | No | 1463 (9.1) | 908 (10.3) | 555 (7.7) | 26.454 (<0.001) |
| Yes | 11,360 (90.9) | 6190 (89.7) | 5170 (92.3) | ||
| Frequency of drinking | ≤1/month | 5618 (46.0) | 3185 (47.7) | 2433 (44.2) | 19.342 (<0.001) |
| 2–4/month | 2723 (25.5) | 1386 (24.0) | 1337 (27.2) | ||
| ≥2/week | 3018 (28.5) | 1618 (28.3) | 1400 (28.6) | ||
| Alcohol consumption per session (glasses) | 1–2 | 3653 (35.1) | 1956 (35.4) | 1697 (34.8) | 0.633 (0.719) |
| 3–6 | 3350 (36.7) | 1780 (36.8) | 1570 (36.6) | ||
| ≥7 | 2213 (28.2) | 1140 (27.8) | 1073 (28.6) | ||
| Smoking | No | 1561 (54.7) | 4230 (55.2) | 3331 (54.2) | 1.306 (0.232) |
| Yes | 5254 (45.3) | 2862 (44.8) | 2392 (45.8) | ||
| Subjective health | Good | 3865 (30.9) | 1849 (26.3) | 2016 (36.2) | 178.686 (<0.001) |
| Normal | 7021 (54.7) | 4005 (56.9) | 3016 (52.3) | ||
| Bad | 2004 (14.4) | 1293 (16.8) | 711 (11.5) | ||
| Subjective body weight | Thin | 1897 (14.6) | 1122 (15.9) | 775 (13.1) | 20.499 (<0.001) |
| Normal | 5288 (40.4) | 2921 (40.1) | 2367 (40.8) | ||
| Obese | 5636 (45.0) | 3054 (44.0) | 2582 (46.1) | ||
| Perceived stress | Low | 9933 (76.3) | 5448 (75.6) | 4485 (77.1) | 3.938 (0.040) |
| High | 2878 (23.7) | 1641 (24.4) | 1237 (22.9) | ||
| Depression | 2.06 (0.031) | 2.11 (0.042) | 2.0 (0.035) | 2.309 (0.022) | |
| Characteristics | No Aerobic Physical Activity | Aerobic Physical Activity | |||||
|---|---|---|---|---|---|---|---|
| β | t | p | β | t | p | ||
| Gender | Men | −0.629 | −7.390 | <0.001 | −0.530 | −7.020 | <0.001 |
| Women | 1.0 | 1.0 | |||||
| Age (years) | 30–49 | −0.170 | −1.264 | 0.207 | 0.360 | 2.964 | 0.003 |
| 50–64 | −0.217 | −1.986 | 0.048 | 0.060 | 0.550 | 0.582 | |
| ≥65 | 1.0 | 1.0 | |||||
| Family income | Upper | −0.362 | −2.631 | 0.009 | −0.418 | −2.697 | 0.007 |
| Middle | −0.141 | −1.076 | 0.283 | −0.293 | −2.045 | 0.042 | |
| Lower | 1.0 | 1.0 | |||||
| Education level | ≤Middle school | −0.076 | −0.714 | 0.476 | 0.269 | 2.516 | 0.012 |
| High school | 0.035 | 0.447 | 0.655 | 0.260 | 3.434 | 0.001 | |
| ≥College | 1.0 | 1.0 | |||||
| Housing type | Detached house | 0.167 | 1.339 | 0.182 | 0.257 | 2.560 | 0.011 |
| Apartment | 0.095 | 0.787 | 0.432 | 0.183 | 1.917 | 0.056 | |
| Other | 1.0 | 1.0 | |||||
| Marital status | Living with spouse | −0.369 | −2.215 | 0.027 | −0.745 | −3.307 | 0.001 |
| Other | 1.0 | 1.0 | |||||
| Blood pressure | Normal | 0.209 | 2.012 | 0.045 | 0.347 | 3.430 | 0.001 |
| Prehypertension | 0.198 | 1.966 | 0.050 | 0.165 | 1.721 | 0.086 | |
| Hypertension | 1.0 | 1.0 | |||||
| Body weight | Underweight | 1.166 | 4.498 | <0.001 | 0.408 | 1.809 | 0.071 |
| Normal | 0.409 | 4.815 | <0.001 | 0.289 | 3.182 | 0.002 | |
| Obese | 1.0 | 1.0 | |||||
| Hypercholesterolemia status | No hypercholesterolemia | −0.078 | −0.788 | 0.432 | 0.209 | 2.202 | 0.028 |
| Hypercholesterolemia | 1.0 | 1.0 | |||||
| Frequency of drinking | ≤1/month | −0.443 | −4.703 | <0.001 | −0.300 | −3.701 | <0.001 |
| 2–4/month | −0.402 | −4.107 | <0.001 | −0.297 | −3.127 | 0.002 | |
| ≥2/week | 1.0 | ||||||
| Subjective health | Good | −2.001 | −15.253 | <0.001 | −2.341 | −13.627 | <0.001 |
| Normal | −1.286 | −10.458 | <0.001 | −1.774 | −10.222 | <0.001 | |
| Bad | 1.0 | 1.0 | |||||
| Subjective body weight | Thin | −0.320 | −2.328 | 0.021 | −0.134 | −1.010 | 0.313 |
| Normal | −0.340 | −3.909 | <0.001 | −0.323 | −3.871 | <0.001 | |
| Obese | 1.0 | 1.0 | |||||
| Stress | Low | −2.213 | −20.730 | <0.001 | −2.210 | −20.964 | <0.001 |
| High | 1.0 | 1.0 | |||||
| R2/F/p | R2 = 0.213, F = 41.475, p < 0.001 | R2 = 0.246, F = 40.190, p < 0.001 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.A.; Song, Y.; Kwon, M. Do Adults Who Practice Aerobic Physical Activities Have Different Influencing Factors for Depression: A Secondary Data Analysis. Int. J. Environ. Res. Public Health 2022, 19, 6142. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106142
Kim SA, Song Y, Kwon M. Do Adults Who Practice Aerobic Physical Activities Have Different Influencing Factors for Depression: A Secondary Data Analysis. International Journal of Environmental Research and Public Health. 2022; 19(10):6142. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106142
Chicago/Turabian StyleKim, Sun Ae, Youngshin Song, and Myoungjin Kwon. 2022. "Do Adults Who Practice Aerobic Physical Activities Have Different Influencing Factors for Depression: A Secondary Data Analysis" International Journal of Environmental Research and Public Health 19, no. 10: 6142. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106142