
Is There Risk Compensation among HIV Infected Youth and Adults 15 Years and Older on Antiretroviral Treatment in South Africa? Findings from the 2017 National HIV Prevalence, Incidence, Behaviour and Communication Survey


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey Design and Population
2.2. Blood Specimen Collection and Processing
2.3. Measures
2.3.1. Primary Outcome and Control Variables
- Condom use at last sex (No = 1 and Yes = 0)
- Consistent condom use (No = 1 and Yes = 0)
- Number of sexual partners in the past 12 months (One partner = 0 and Two or more partners = 1).
- HIV positive, aware and not ART = 0
- HIV negative aware = 1
- HIV positive aware, and on ART = 2.
2.3.2. Explanatory Variables
2.4. Statistical Analysis
3. Results
3.1. Description of the Study Sample
3.2. Risky Sexual Behaviour by HIV Status and ART Exposure
3.3. Factors Associated with Risky Sexual Behaviour
3.3.1. Bivariate Logistic Regression Models
3.3.2. Multivariate Logistic Regression Models
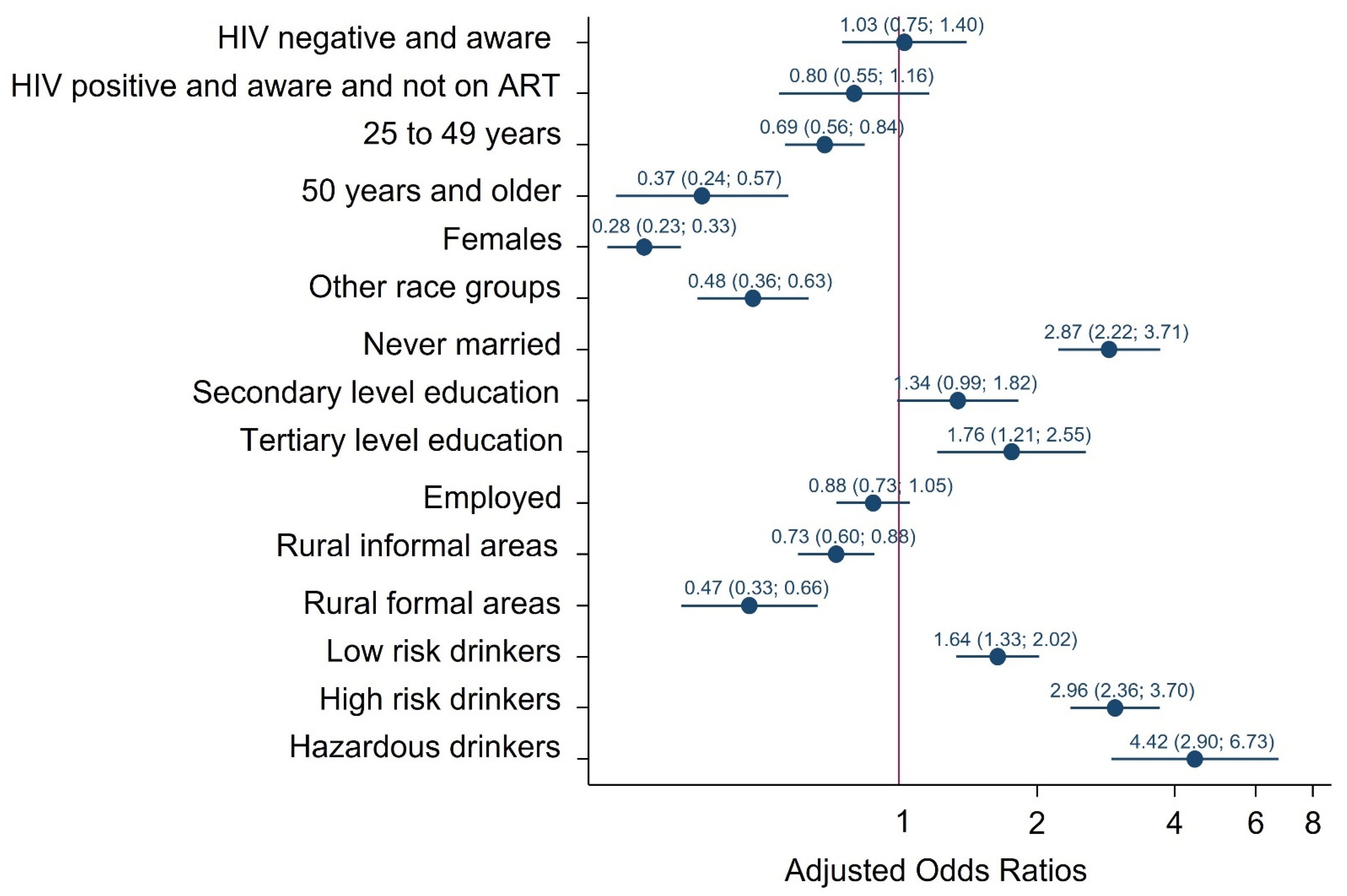
Multiple Sexual Partnerships
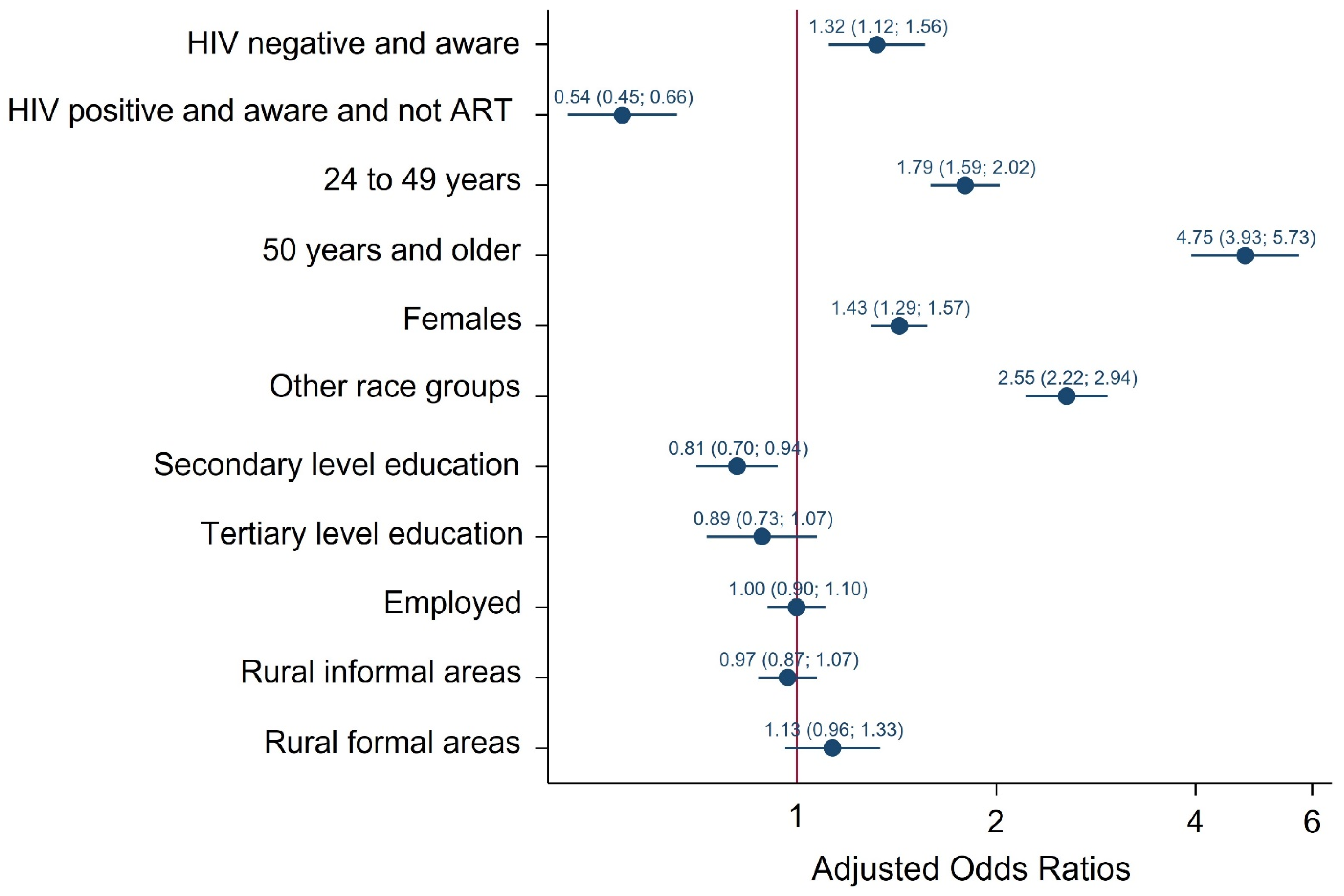
Condom Use at the Last Sexual Encounter
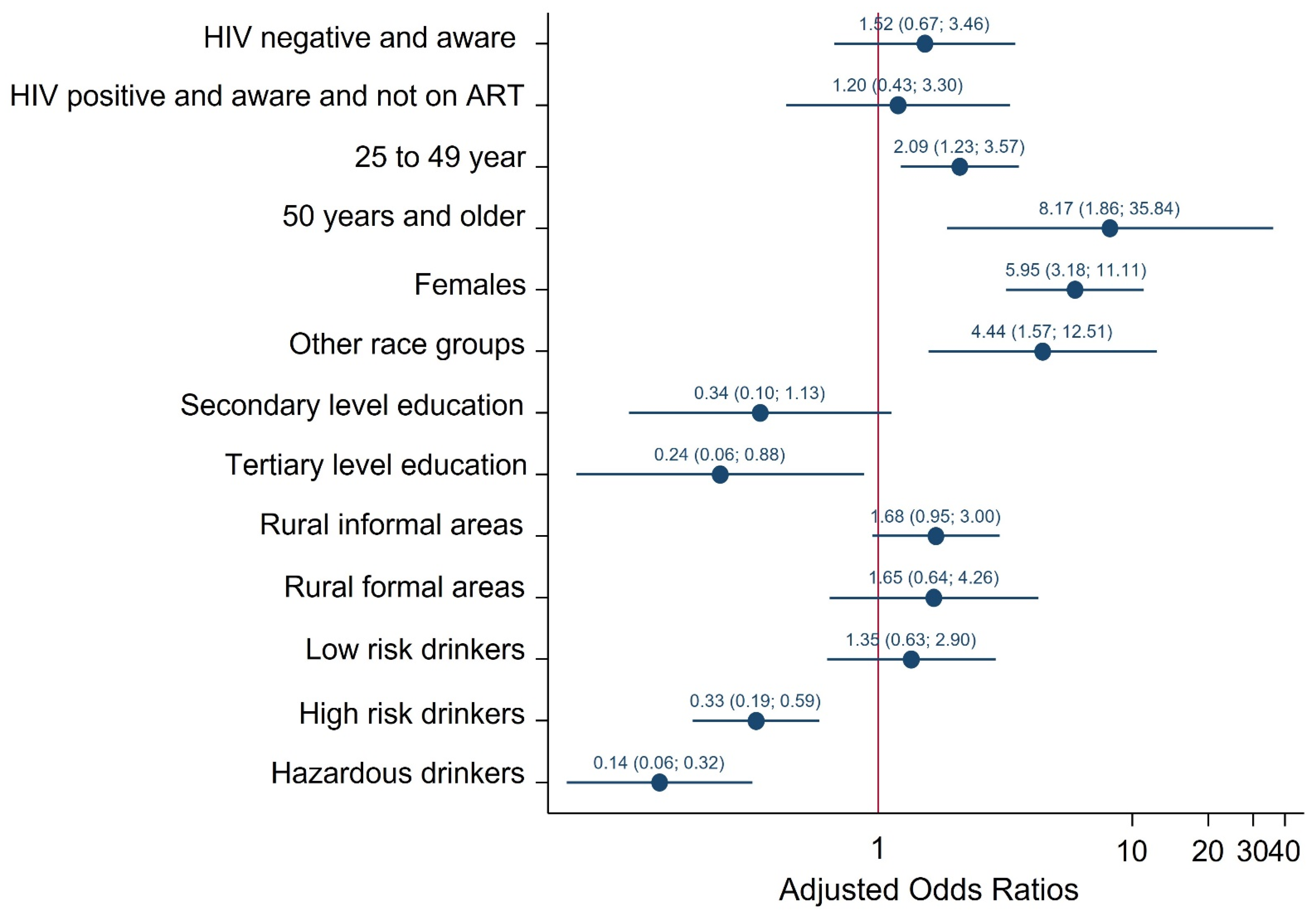
Consistent Condom Use
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Simbayi, L.; Zuma, K.; Zungu, N.; Moyo, S.; Marinda, E.; Jooste, S.; Mabaso, M.; Ramlagan, S.; North, A.; Zyl, J.V.; et al. South African National HIV Prevalence, Incidence, Behaviour and Communication Survey, 2017; HSRC Press: Cape Town, South Africa, 2019. [Google Scholar]
- Jean, K.; Gabillard, D.; Moh, R.; Danel, C.; Fassassi, R.; du Loû, A.D.; Eholié, S.; Lert, F.; Anglaret, X.; Dray-Spira, R. Effect of Early Antiretroviral Therapy on Sexual Behaviors and HIV-1 Transmission Risk Among Adults with Diverse Heterosexual Partnership Statuses in Cote d’Ivoire. J. Infect. Dis. 2014, 209, 431–440. [Google Scholar] [PubMed]
- Grinsztejn, B.; Hosseinipour, M.C.; Ribaudo, H.J.; Swindells, S.; Eron, J.; Chen, Y.Q.; Wang, L.; Ou, S.-S.; Anderson, M.; McCauley, M.; et al. Effects of early versus delayed initiation of antiretroviral treatment on clinical outcomes of HIV-1 infection: Results from the phase 3 HPTN 052 randomised controlled trial. Lancet Infect. Dis. 2014, 14, 281–290. [Google Scholar] [CrossRef] [Green Version]
- Cohen, M.S.; Chen, Y.Q.; McCauley, M.; Gamble, T.; Hosseinipour, M.C.; Kumarasamy, N.; Hakim, J.G.; Kumwenda, J.; Grinsztejn, B.; Pilotto, J.H.; et al. Prevention of HIV-1 infection with early antiretroviral therapy. N. Engl. J. Med. 2011, 365, 493–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goosby, E.; Von Zinkernagel, D.; Holmes, C.; Haroz, D.; Walsh, T. Raising the bar: PEPFAR and new paradigms for global health. J. Acquir. Immune Defic. Syndr. 2012, 60, S158–S162. [Google Scholar] [CrossRef]
- Goosby, E. The President’s Emergency Plan for AIDS Relief: Marshalling all tools at our disposal toward an AIDS-free generation. Health Aff. (Millwood) 2012, 31, 1593–1598. [Google Scholar] [CrossRef]
- Beyrer, C.; Birx, D.L.; Bekker, L.-G.; Barré-Sinoussi, F.; Cahn, P.; Dybul, M.R.; Eholié, S.P.; Kavanagh, M.M.; Katabira, E.T.; Lundgren, J.; et al. The Vancouver Consensus: Antiretroviral medicines, medical evidence, and political will. Lancet 2015, 386, 505–507. [Google Scholar] [CrossRef]
- Tanser, F.; Bärnighausen, T.; Grapsa, E.; Zaidi, J.; Newell, M.L. High Coverage of ART Associated with Decline in Risk of HIV Acquisition in Rural KwaZulu-Natal, South Africa. Science 2013, 339, 966–971. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, K.K.; Flanigan, T.P.; Mayer, K.H. Is expanded HIV treatment preventing new infections? Impact of antiretroviral therapy on sexual risk behaviors in the developing world. AIDS 2011, 25, 1939–1949. [Google Scholar] [CrossRef]
- UNAIDS. Country Factsheets, South Africa. 2019. Available online: https://www.unaids.org/en/regionscountries/countries/southafrica (accessed on 23 February 2021).
- National Department of Health. Annual Performance Plan 2018/19–2020/21; Department of Health: Pretoria, South Africa, 2018.
- Westercamp, N.; Agot, K.; Jaoko, W.; Bailey, R.C. Risk compensation following male circumcision: Results from a two-year prospective cohort study of recently circumcised and uncircumcised men in Nyanza Province, Kenya. AIDS Behav. 2014, 18, 1764–1775. [Google Scholar] [CrossRef]
- Macphail, C.L.; Sayles, J.N.; Cunningham, W.; Newman, P.A. Perceptions of sexual risk compensation following posttrial HIV vaccine uptake among young South Africans. Qual. Health Res. 2012, 22, 668–678. [Google Scholar] [CrossRef] [Green Version]
- Cassell, M.M.; Halperin, D.T.; Shelton, J.D.; Stanton, D. Risk compensation: The Achilles’ heel of innovations in HIV prevention? BMJ 2006, 332, 605–607. [Google Scholar] [CrossRef] [Green Version]
- Eaton, L.A.; Kalichman, S. Risk compensation in HIV prevention: Implications for vaccines, microbicides, and other biomedical HIV prevention technologies. Curr. HIV/AIDS Rep. 2007, 4, 165–172. [Google Scholar] [CrossRef]
- Sharma, M.; Romas, J.A. Theoretical Foundations of Health Education and Health Promotion; Jones & Bartlett Publishers: Boston, MA, USA, 2012. [Google Scholar]
- Berhan, A.; Berhan, Y. Is the Sexual Behaviour of HIV Patients on Antiretroviral therapy safe or risky in Sub-Saharan Africa? Meta-Analysis and Meta-Regression. AIDS Res. Ther. 2012, 9, 14. [Google Scholar] [CrossRef] [Green Version]
- Peltzer, K.; Ramlagan, S. Safer sexual behaviours after 1 year of antiretroviral treatment in KwaZulu-Natal, South Africa: A prospective cohort study. Sex Health 2010, 7, 135–141. [Google Scholar] [CrossRef]
- Risher, K.; Rehle, T.; Simbayi, L.; Shisana, O.; Celentano, D.D. Antiretroviral treatment is not associated with risk compensation among HIV infected South Africans. AIDS Behav. 2016, 20, 710–716. [Google Scholar] [CrossRef] [Green Version]
- Apondi, R.; Bunnell, R.; Ekwaru, J.P.; Moore, D.; Bechange, S.; Khana, K.; King, R.; Campbell, J.; Tappero, J.; Mermin, J. Sexual behavior and HIV transmission risk of Ugandan adults taking antiretroviral therapy: 3 year follow-up. AIDS 2011, 25, 1317–1327. [Google Scholar] [CrossRef]
- Shafer, L.A.; Nsubuga, R.N.; White, R.; Mayanja, B.N.; Chapman, R.; O’Brien, K.; Van der Paal, L.; Grosskurth, H.; Maher, D. Antiretroviral therapy and sexual behavior in Uganda: A cohort study. AIDS 2011, 25, 671–678. [Google Scholar] [CrossRef]
- Delva, W.; Helleringer, S. Beyond Risk Compensation: Clusters of Antiretroviral Treatment (ART) Users in Sexual Networks Can Modify the Impact of ART on HIV Incidence. PLoS ONE 2016, 11, e0163159. [Google Scholar]
- Hasse, B.; Ledergerber, B.; Hirschel, B.; Vernazza, P.; Glass, T.R.; Jeannin, A.; Evison, J.M.; Elzi, L.; Cavassini, M.; Bernasconi, E.; et al. Swiss HIV Cohort Study. Frequency and determinants of unprotected sex among HIV-infected persons: The Swiss HIV Cohort Study. Clin. Infect. Dis. 2010, 51, 1314–1322. [Google Scholar] [CrossRef]
- Doyle, J.S.; Degenhardt, L.; Pedrana, A.E.; McBryde, E.S.; Guy, R.J.; Stoové, M.A.; Weaver, E.R.; Grulich, A.E.; Lo, Y.-R.; Hellard, M.E. Effects of HIV antiretroviral therapy on sexual and injecting risk-taking behavior: A systematic review and meta-analysis. Clin. Infect. Dis. 2014, 59, 1483–1494. [Google Scholar]
- Nkhoma, K.; Ahmed, A.; Alli, Z.; Sherr, L.; Harding, R. Does sexual behaviour of people with HIV reflect antiretroviral therapy as a preventive strategy? A cross-sectional study among outpatients in Kenya. BMC Public Health 2019, 19, 1254. [Google Scholar] [CrossRef]
- Kaye, D.K.; Kakaire, O.; Osinde, M.O.; Lule, J.C.; Kakande, N. The impact of highly active antiretroviral therapy on high-risk behaviour of HIV-infected patients in sub-Saharan. Africa J. Infect. Dev. Ctries 2013, 7, 436–447. [Google Scholar] [CrossRef] [Green Version]
- Statistics South Africa. Mid-Year Population Estimates 2017; Statistics South Africa: Pretoria, South Africa, 2017.
- Saunders, J.B.; Aasland, O.G.; Babor, T.F.; de la Fuente, J.R.; Grant, M. Development of the Alcohol Use Disorders Screening Test (AUDIT). WHO collaborative project on early detection of persons with harmful alcohol consumption. II. Addiction 1993, 88, 791–804. [Google Scholar] [CrossRef]
- Morojele, N.K.; Nkosi, S.; Kekwaletswe, C.T.; Shuper, P.A.; Manda, S.O.; Myers, B.; Parry, C.D.H. Utility of Brief Versions of the Alcohol Use Disorders Identification Test (AUDIT) to Identify Excessive Drinking Among Patients in HIV Care in South Africa. J. Stud. Alcohol Drugs 2016, 78, 88–96. [Google Scholar] [CrossRef]
- Coates, T.J.; Richter, L.; Caceres, C. Behavioural strategies to reduce HIV transmission: How to make them work better. Lancet 2008, 372, 669–684. [Google Scholar]
- Suzan-Monti, M.; Lorente, N.; Demoulin, B.; Marcellin, F.; Préau, M.; Dray-Spira, R.; Lert, F.; Spire, B. Sexual risk behaviour among people living with HIV according to the biomedical risk of transmission: Results from the ANRS-VESPA2 survey. J. Int. AIDS Soc. 2016, 19, 20095. [Google Scholar] [CrossRef] [Green Version]
- Joint United Nations Programme on AIDS (UNAIDS). UNAIDS Global Report on the AIDS Epidemic Geneva, Switzerland, UNAIDS. 2010. Available online: http://search.unaids.org/search.asp?lg=en&search=2010%20report%20on%20the%20global%20aids%20epidemic (accessed on 7 November 2019).
- Yi, S.; Tuot, S.; Yung, K.; Kim, S.; Chhea, C.; Saphonn, V. Factors Associated with Risky Sexual Behavior among Unmarried Most-at-Risk Young People in Cambodia. Am. J. Public Health Res. 2014, 5, 211–220. [Google Scholar] [CrossRef] [Green Version]
- Mishra, V.; Bignami-Van Assche, S. Concurrent Sexual Partnership and HIV Infection: Evidence from National Population-Based Surveys, (UNAIDS 2009); Macro-International Inc.: Calverton, MD, USA, 2009. [Google Scholar]
- Exavery, A.; Kanté, A.M.; Tani, K.; Hingora, A.; Phillips, J.F. Socio-demographic drivers of multiple sexual partnerships among women in three rural districts of Tanzania. HIV/AIDS 2015, 7, 105. [Google Scholar]
- Nasrullah, M.; Oraka, E.; Chavez, P.R.; Johnson, C.H.; DiNenno, E. Factors Associated with Condom Use Among Sexually Active U.S. Adults, National Survey of Family Growth, 2006–2010 and 2011–2013. J. Sex Med. 2017, 14, 541–550. [Google Scholar] [CrossRef] [Green Version]
- Christopher, H.R.; Riley, S.J.; Richard, L.; Schell, H.; Patricia, D. Variability in Condom Use Trends by Sexual Risk Behaviors: Findings from the 2003–2015 National Youth Risk Behavior Surveys. Sex. Transm. Dis. 2018, 45, 400–405. [Google Scholar]
- Kordoutis, P.; Loumakou, M.; Sarafidou, J. Heterosexual relationship characteristics, condom use and safe sex practices. AIDS Care 2001, 12, 767–782. [Google Scholar] [CrossRef]
- Kathleen Ford KSohn, W.; Lepkowski, J. Characteristics of Adolescents’ Sexual Partners and Their association with use of Condoms and other contraceptive methods. Fam. Plan. Perspect. 2001, 33, 100–105. [Google Scholar]
- Prata, N.; Vahidnia, F.; Fraser, A. Gender and Relationship Differences in Condom Use Among 15–24-Year-Olds in Angola. Int. Perspect. Sex. Reprod. Health 2005, 31, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Woolf, S.E.; Maisto, S.A. Gender Differences in Condom Use Behavior? The Role of Power and Partner-Type. Sex Roles 2008, 58, 689–701. [Google Scholar]
- Qiao, J.; Guo, Y.; Zhu, Y.; Hong, Y.A.; Xu, Z.; Zeng, C.; Zhang, H.; Cai, W.; Li, L.; Liu, C.; et al. Gender differences in the relationship of sexual partnership characteristics and inconsistent condom use among people living with HIV in China. AIDS Care 2020, 32, 128–135. [Google Scholar] [CrossRef]
- Ernestine, A.; Duncan, W. Influence of Partner Type on Condom Use. J. Hum. Behav. Soc. Environ. 2011, 21, 784–802. [Google Scholar]
- Yamamoto, N.; Ejima, K.; Nishiura, H. Modelling the impact of correlations between condom use and sexual contact pattern on the dynamics of sexually transmitted infections. Theor. Biol. Med. Model. 2018, 15, 6. [Google Scholar] [CrossRef]
- Adetunji, J. Condom Use in Marital and Nonmarital Relationships in Zimbabwe. Int. Perspect. Sex. Reprod. Health 2000, 26, 196–200. [Google Scholar] [CrossRef]
- Eisele, T.; Mathews, C.; Chopra, M.; Lurie, M.N.; Brown, L.; Dewing, S.; Kendall, C. Changes in risk behaviour among HIV-positive patients during their first year of antiretroviral therapy in Cape Town South Africa. AIDS Behav. 2008, 13, 1097–1105. [Google Scholar] [CrossRef]
- Chimbindi, N.Z.; McGrth, N.; Herbst, K.; Tint, K.S.; Newell, M.L. Socio-Demographic Determinants of Condom Use among Sexually Active Young Adults in Rural KwaZulu-Natal, South Africa. Open AIDS J. 2010, 4, 88–95. [Google Scholar] [CrossRef]
- Eisele, T.P.; Mathews, C.; Chopra, M.; Brown, L.; Silvestre, E.; Daries, V.; Kendall, C. High levels of risk behavior among people living with HIV Initiating and waiting to start antiretroviral therapy in Cape Town South Africa. AIDS Behav. 2008, 12, 570–577. [Google Scholar] [CrossRef]
- Walusaga, H.A.; Kyohangirwe, R.; Wagner, G.J. Gender differences in determinants of condom use among HIV clients in Uganda. AIDS Patient Care STDS 2012, 26, 694–699. [Google Scholar] [CrossRef] [Green Version]
- Calsyn, D.A.; Peavy, M.; Wells, E.A.; Campbell, A.N.; Hatch-Maillette, M.A.; Greenfield, S.F.; Tross, S. Differences between men and women in condom use, attitudes, and skills in substance abuse treatment seekers. Am. J. Addict. 2013, 22, 150–1577. [Google Scholar] [CrossRef]
- Shai, N.J.; Jewkes, R.; Nduna, M.; Dunkle, K. Masculinities and condom use patterns among young rural South Africa men: A cross-sectional baseline survey. BMC Public Health 2012, 12, 462. [Google Scholar] [CrossRef] [Green Version]
- Lagarde, E.; Carael, M.; Glynn, J.R.; Kanhonou, L.; Abega, S.; Kahindo, M.; Musonda, R.; Auvert, B.; Buve, A. Education Level is Associated with Condom Use within Non-Spousal Partnerships in Four Cities of Sub-Saharan Africa. AIDS 2001, 15, 399–1408. [Google Scholar] [CrossRef]
- Beksinska, M.E.; Smit, J.A.; Mantell, J.E. Progress and challenges to male and female condom use in South Africa. Sex Health 2012, 9, 51–58. [Google Scholar] [CrossRef]
- Diabaté, S.; Alary, M.; Koffi, C.K. Short-term increase in unsafe sexual behaviour after initiation of HAART in Côte d’Ivoire. AIDS 2008, 22, 154–156. [Google Scholar] [CrossRef]
- Yaya, I.; Saka, B.; Landoh, D.E.; Patchali, P.M.; Makawa, M.-S.; Senanou, S. Sexual risk behaviour among people living with HIV and AIDS on antiretroviral therapy at the regional hospital of Sokodé, Togo. BMC Public Health 2014, 14, 636. [Google Scholar]
- Okoboi, S.; Castelnuovo, B.; Moore, D.M.; Musaazi, J.; Kambugu, A.; Birungi, J.; Kaleebu, P.; Nanfuka, M.; Kamya, M.R.; Van Rie, A. Risky sexual behavior among patients on long-term antiretroviral therapy: A prospective cohort study in urban and rural Uganda. AIDS Res. Ther. 2018, 15, 15. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | N | % |
|---|---|---|
| Age group in years | ||
| 15–24 | 2354 | 19.7 |
| 25–49 | 5764 | 60.4 |
| 50+ | 3023 | 19.9 |
| Sex | ||
| Male | 4046 | 45.1 |
| Female | 7095 | 54.9 |
| Race groups | ||
| Black African | 7856 | 83.1 |
| Other | 3285 | 16.9 |
| Marital status | ||
| Married | 3617 | 33.6 |
| Never married | 6332 | 66.4 |
| Education level | ||
| No education/primary | 1823 | 15.4 |
| Secondary | 5963 | 68.7 |
| Tertiary | 1078 | 15.9 |
| Employment status | ||
| Not employed | 7195 | 62.7 |
| Employed | 3800 | 37.3 |
| Locality type | ||
| Urban | 7211 | 72.2 |
| Rural informal (tribal areas) | 2843 | 24.2 |
| Rural (farms) | 1087 | 3.6 |
| AUDIT score * | ||
| Abstainers | 6944 | 65.9 |
| Low-risk drinkers (1–7) | 2100 | 22.2 |
| High-risk drinkers (8–19) | 928 | 10.3 |
| Hazardous drinkers (20+) | 148 | 1.6 |
| Numbers of sexual partners in the 12 months | ||
| One partner | 6047 | 88.6 |
| Two or more partners | 614 | 11.4 |
| Condom use at last sex | ||
| No | 2360 | 39.0 |
| Yes | 4262 | 61.0 |
| Consistent condom use | ||
| No | 69 | 1.0 |
| Yes | 11,072 | 99.0 |
| Variables | Multiple Sexual Partners | No Condom Use at Last Sex | No Consistent Condom Use | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | 95% CI | p-Value | n | % | 95% CI | p-Value | n | % | 95% CI | p-Value | |
| Age group years | ||||||||||||
| 15–24 | 1369 | 18.0 | 15.2–21.2 | <0.001 | 1357 | 43.7 | 40.1–47.4 | <0.001 | 1352 | 97.3 | 95.6–98.3 | 0.014 |
| 25–49 | 4174 | 11.1 | 9.7–12.8 | 4162 | 61.7 | 59.5–63.9 | 4117 | 98.5 | 97.7–99.0 | |||
| 50+ | 1117 | 3.4 | 2.2–5.2 | 1100 | 83.1 | 79.4–86.2 | 1090 | |||||
| Sex | ||||||||||||
| Male | 2636 | 17.7 | 15.6–20.0 | <0.001 | 2630 | 58.0 | 55.4–60.6 | <0.001 | 2601 | 97.1 | 95.9–97.9 | <0.001 |
| Female | 4024 | 5.5 | 4.4–6.8 | 3989 | 64.0 | 61.7–66.2 | 3958 | 99.8 | 99.6–99.9 | |||
| Race groups | ||||||||||||
| African | 4768 | 12.6 | 11.1–14.2 | <0.001 | 4759 | 56.8 | 54.8–58.7 | <0.001 | 4714 | 98.3 | 97.6–98.8 | 0.169 |
| Other | 1892 | 5.5 | 4.1–7.3 | 1860 | 83.8 | 80.9–86.3 | 1845 | 99.1 | 98.0–99.6 | |||
| Marital status | ||||||||||||
| Married | 2622 | 4.1 | 3.0–5.7 | <0.001 | 2602 | 82.1 | 79.3–84.6 | <0.001 | 2574 | 99.9 | 99.6–100.0 | <0.001 |
| Never married | 3767 | 16.1 | 14.4–18.0 | 3746 | 48.9 | 46.5–51.3 | 3718 | 97.5 | 96.6–98.3 | |||
| Education level | ||||||||||||
| No education/primary | 796 | 5.3 | 3.6–7.8 | 0.005 | 798 | 63.3 | 58.2–68.1 | <0.001 | 788 | 99.8 | 99.3–99.9 | 0.149 |
| Secondary | 4049 | 11.6 | 10.2–13.3 | 4024 | 61.0 | 58.7–63.3 | 3992 | 98.6 | 97.7–99.2 | |||
| Tertiary | 769 | 10.1 | 7.3–13.9 | 755 | 73.0 | 68.2–77.4 | 750 | 98.7 | 96.7-99.5 | |||
| Employment status | ||||||||||||
| Not employed | 3910 | 11.9 | 10.4–13.5 | 0.434 | 3890 | 56.7 | 54.4–59.0 | <0.001 | 3859 | 98.6 | 98.0–99.0 | 0.235 |
| Employed | 2681 | 10.9 | 9.1–13.1 | 2663 | 66.6 | 63.8–69.4 | 2634 | 98.3 | 96.9–99.0 | |||
| Locality type | ||||||||||||
| Urban | 4417 | 12.3 | 10.8–14.0 | <0.001 | 4371 | 62.6 | 60.3–64.8 | <0.001 | 4326 | 98.3 | 97.5–98.8 | 0.124 |
| Rural informal (tribal areas) | 1575 | 9.4 | 7.6–11.6 | 1581 | 54.5 | 51.0–58.0 | 1567 | 98.8 | 98.0–99.3 | |||
| Rural (farms areas) | 668 | 5.8 | 3.7–9.0 | 667 | 67.6 | 60.5–74.0 | 666 | 99.6 | 99.0–99.9 | |||
| AUDIT score * | ||||||||||||
| Abstainers | 3751 | 7.8 | 6.5–9.2 | <0.001 | 3728 | 59.8 | 57.4–62.1 | 0.251 | 3697 | 98.9 | 98.2–99.3 | 0.001 |
| Low-risk drinkers (1–7) | 1490 | 12.5 | 9.9–15.8 | 1473 | 63.9 | 60.2–67.5 | 1459 | 98.7 | 96.1–99.6 | |||
| High-risk drinkers (8–19) | 707 | 22.0 | 18.2–26.4 | 709 | 60.1 | 54.9–65.0 | 697 | 97.5 | 95.4-–98.6 | |||
| Hazardous drinkers (20+) | 112 | 39.9 | 26.9–54.5 | 113 | 55.0 | 40.1–69.0 | 112 | 90.4 | 80.4–95.6 | |||
| Variables | Multiple Sexual Partners | No Condom Use at Last Sex | No Consistent Condom Use | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Values | OR | 95% CI | p-Values | OR | 95% CI | p-Value | ||||
| HIV positive aware and not on ART | 1 | 1 | 1 | |||||||||
| HIV negative and aware | 1.0 | 0.8 | 1.3 | 0.890 | 1.4 | 1.2 | 1.7 | <0.001 | 1.1 | 0.5 | 2.2 | 0.837 |
| HIV positive aware and on ART | 0.6 | 0.4 | 0.8 | 0.001 | 0.6 | 0.5 | 0.7 | <0.001 | 1.8 | 0.7 | 4.4 | 0.224 |
| Multiple Sexual Partners | No Condom Use at Last Sex | No Consistent Condom Use | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Values | OR | 95% CI | p-Values | OR | 95% CI | p-Values | ||||
| Age groups | ||||||||||||
| 15–24 | 1 | 1 | 1 | |||||||||
| 25–49 | 0.6 | 0.5 | 0.7 | <0.001 | 2.4 | 2.2 | 2.6 | <0.001 | 2.2 | 1.5 | 3.3 | <0.001 |
| 50+ | 0.2 | 0.1 | 0.3 | <0.001 | 6.7 | 5.7 | 7.8 | <0.001 | 15.8 | 3.8 | 65.1 | <0.001 |
| Sex | ||||||||||||
| Male | 1 | 1 | 1 | |||||||||
| Female | 0.2 | 0.2 | 0.3 | <0.001 | 1.3 | 1.2 | 1.5 | <0.001 | 10.8 | 6.2 | 18.7 | <0.001 |
| Race | ||||||||||||
| Black African | 1 | 1 | 1 | |||||||||
| Other | 0.5 | 0.4 | 0.6 | <0.001 | 3.0 | 2.6 | 3.4 | <0.001 | 2.1 | 1.1 | 4.0 | 0.018 |
| Marital status | ||||||||||||
| Married | 1 | 1 | 1 | |||||||||
| Never married | 4.3 | 3.6 | 5.3 | <0.001 | 0.2 | 0.2 | 0.2 | <0.001 | 0.1 | 0.0 | 0.2 | <0.001 |
| Educational qualification | ||||||||||||
| None/primary | 1 | 1 | 1 | |||||||||
| Secondary | 1.8 | 1.4 | 2.3 | <0.001 | 0.6 | 0.6 | 0.7 | <0.001 | 0.2 | 0.1 | 0.8 | 0.017 |
| Tertiary | 1.8 | 1.3 | 2.5 | <0.001 | 0.8 | 0.7 | 1.0 | 0.013 | 0.2 | 0.1 | 0.7 | 0.016 |
| Employment status | ||||||||||||
| No | 1 | 1 | 1 | |||||||||
| Yes | 0.9 | 0.8 | 1.1 | 0.222 | 1.43 | 1.22 | 1.43 | <0.001 | 1.02 | 0.69 | 1.50 | 0.938 |
| Locality type | ||||||||||||
| Urban | 1 | 1 | 1 | |||||||||
| Rural informal (tribal areas) | 0.8 | 0.7 | 0.9 | <0.001 | 0.8 | 0.7 | 0.8 | <0.001 | 1.8 | 1.1 | 2.8 | 0.011 |
| Rural (farms) | 0.6 | 0.4 | 0.7 | <0.001 | 1.1 | 1.0 | 1.3 | 0.133 | 2.6 | 1.0 | 6.3 | 0.042 |
| AUDIT score * | ||||||||||||
| Abstainers | 1 | 1 | 1 | |||||||||
| Low risk drinkers (1–7) | 1.9 | 1.6 | 2.3 | <0.001 | 1.0 | 0.9 | 1.2 | 0.438 | 1.0 | 0.5 | 1.8 | 0.900 |
| High risk drinkers (8–19) | 4.6 | 3.9 | 5.5 | <0.001 | 1.0 | 0.8 | 1.1 | 0.516 | 0.2 | 0.1 | 0.3 | <0.001 |
| Hazardous drinkers (20+) | 7.0 | 4.9 | 10.0 | <0.001 | 1.2 | 0.9 | 1.7 | 0.279 | 0.1 | 0.0 | 0.2 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zungu, N.; Mabaso, M.; Ramlagan, S.; Simbayi, L.; Moyo, S.; Shisana, O.; Murangandi, P.; Igumbor, E.; Sigida, S.; Jooste, S.; et al. Is There Risk Compensation among HIV Infected Youth and Adults 15 Years and Older on Antiretroviral Treatment in South Africa? Findings from the 2017 National HIV Prevalence, Incidence, Behaviour and Communication Survey. Int. J. Environ. Res. Public Health 2022, 19, 6156. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106156
Zungu N, Mabaso M, Ramlagan S, Simbayi L, Moyo S, Shisana O, Murangandi P, Igumbor E, Sigida S, Jooste S, et al. Is There Risk Compensation among HIV Infected Youth and Adults 15 Years and Older on Antiretroviral Treatment in South Africa? Findings from the 2017 National HIV Prevalence, Incidence, Behaviour and Communication Survey. International Journal of Environmental Research and Public Health. 2022; 19(10):6156. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106156
Chicago/Turabian StyleZungu, Nompumelelo, Musawenkosi Mabaso, Shandir Ramlagan, Leickness Simbayi, Sizulu Moyo, Olive Shisana, Pelagia Murangandi, Ehimario Igumbor, Salome Sigida, Sean Jooste, and et al. 2022. "Is There Risk Compensation among HIV Infected Youth and Adults 15 Years and Older on Antiretroviral Treatment in South Africa? Findings from the 2017 National HIV Prevalence, Incidence, Behaviour and Communication Survey" International Journal of Environmental Research and Public Health 19, no. 10: 6156. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106156