
The Effect of Child Abuse and Neglect on Trajectories of Depressive Symptoms and Aggression in Korean Adolescents: Exploring Gender Differences


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data and Participants
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Descriptive Statistics
3.2. Gender Differences and Association between Abuse, Neglect, Depressive Symptoms, and Aggression
4. Discussion
Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Georgiou, S.N.; Symeou, M. Parenting practices and the development of internalizing/externalizing problems in adolescence. In Parenting—Empirical Advances and Intervention Resources; Benedetto, L., Ingrassia, M., Eds.; IntechOpen: London, UK, 2018; pp. 5–29. [Google Scholar]
- Ladouceur, C.D. Neural systems supporting cognitive-affective interactions in adolescence: The role of puberty and implications for affective disorders. Front. Integr. Neurosci. 2012, 6, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lynne, S.D.; Graber, J.A.; Nichols, T.R.; Brooks-Gunn, J.; Botvin, G.J. Links between pubertal timing, peer influences, and externalizing behaviors among urban students followed through middle school. J. Adolesc. Health 2007, 40, 181.e7–181.e13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, K.; Wong, C.H.; McIntyre, R.S.; Wang, J.; Zhang, Z.; Tran, B.X.; Tan, W.; Ho, C.S.; Ho, R.C. Global lifetime and 12-month prevalence of suicidal behavior, deliberate self-harm and non-suicidal self-injury in children and adolescents between 1989 and 2018: A meta-analysis. Int. J. Environ. Res. Public Health 2019, 16, 4581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steptoe, A.; Tsuda, A.; Tanaka, Y.; Wardle, J. Depressive symptoms, socio-economic background, sense of control, and cultural factors in university students from 23 countries. Int. J. Behav. Med. 2007, 14, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.M.; Kennard, B.D.; Lee, P.W.H.; Hughes, C.W.; Mayes, T.L.; Emslie, G.J.; Lewinsohn, P.M. A cross-cultural investigation of cognitions and depressive symptoms in adolescents. J. Abnorm. Psychol. 2004, 113, 248–257. [Google Scholar] [CrossRef]
- Bufferd, S.J.; Dougherty, L.R.; Carlson, G.A.; Rose, S.; Klein, D.N. Psychiatric disorders in preschoolers: Continuity from ages 3 to 6. Am. J. Psychiatry 2012, 169, 1157–1164. [Google Scholar] [CrossRef] [Green Version]
- Merikangas, K.R.; Nakamura, E.F.; Kessler, R.C. Epidemiology of mental disorders in children and adolescents. Dialogues Clin. Neurosci. 2009, 11, 7–20. [Google Scholar] [CrossRef]
- McGuinness, T.M.; Dyer, J.G.; Wade, E.H. Gender differences in adolescent depression. J. Psychosoc. Nurs. Ment. Health Serv. 2012, 50, 17–20. [Google Scholar]
- Ha, Y.H. Causal relationships of adolescent aggression: Empathy, prosocial behavior, self-esteem, and social support. Korean J. Child Stud. 2004, 25, 121–132. [Google Scholar]
- Moffitt, T.E. Adolescence-limited and life-course persistent antisocial behavior: A developmental taxonomy. Psychol. Rev. 1993, 100, 674–701. [Google Scholar] [CrossRef]
- Bukowski, W.M.; Sippola, L.K.; Newcomb, A.F. Variations in patterns of attraction to same- and other-sex peers during early adolescence. Dev. Psychol. 2000, 36, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Knox, M.; Carey, M.; Kim, W.J. Aggression in inpatient adolescents: The effects of gender and depression. Youth Soc. 2003, 35, 226–242. [Google Scholar] [CrossRef]
- Estévez, E.; Povedano, A.; Jiménez, T.I.; Musitu, G. Aggression in adolescence: A gender perspective. In Advances in Psychology Research; Columbus, A.M., Ed.; Nova Science Publishers: Hauppauge, NY, USA, 2014; pp. 71–91. [Google Scholar]
- Silverthorn, P.; Frick, P.J. Developmental pathways to antisocial behavior: The delayed-onset pathway in girls. Dev. Psychopathol. 1999, 11, 101–126. [Google Scholar] [CrossRef] [PubMed]
- Hammen, C. Adolescent depression: Stressful interpersonal contexts and risk for recurrence. Curr. Dir. Psychol. Sci. 2009, 18, 200–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thakur, S.; Grewal, K.K. A study of aggression among adolescents. Int. Res. J. Adv. Sci. Hub 2021, 3, 46–51. [Google Scholar] [CrossRef]
- Moretti, M.M.; Craig, S.G. Maternal versus paternal physical and emotional abuse, affect regulation and risk for depression from adolescence to early adulthood. Child Abus. Negl. 2013, 37, 4–13. [Google Scholar] [CrossRef]
- Keene, A.C.; Epps, J. Childhood physical abuse and aggression: Shame and narcissistic vulnerability. Child Abus. Negl. 2016, 51, 276–283. [Google Scholar] [CrossRef]
- Park, K. The effects of parents’ neglect and abuse on the school adjustment in adolescents: The mediating effects of social withdrawal. Korean J. Child Stud. 2014, 35, 1–15. [Google Scholar]
- Mennen, F.E.; Kim, K.; Sand, J.; Trickett, P.K. Child neglect: Definition and identification of youth’s experiences in official reports of maltreatment. Child Abus. Negl. 2010, 34, 647–658. [Google Scholar] [CrossRef] [Green Version]
- Stuewig, J.; McCloskey, L.A. The relation of child maltreatment to shame and guilt among adolescents: Psychological routes to depression and delinquency. Child Maltreatment 2005, 10, 324–336. [Google Scholar] [CrossRef]
- Kim, M.; Cicchetti, D. Longitudinal trajectories of self-system processes and depressive symptoms among maltreated and nonmaltreated children. Child Dev. 2006, 77, 624–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briere, J. Treating adult survivors of severe childhood abuse: Further development of an integrative model. In The APSAC Handbook on Child Maltreatment, 2nd ed.; Myers, J.E.B., Berliner, L., Briere, J., Hendrix, C.T., Reid, T., Jenny, C., Eds.; Sage Publications: Newbury Park, CA, USA, 2002; pp. 175–204. [Google Scholar]
- Teisl, M.; Cicchetti, D. Physical abuse, cognitive and emotional processes, and aggressive/disruptive behavior problems. Soc. Dev. 2008, 17, 1–23. [Google Scholar] [CrossRef]
- Maneta, E.K.; Cohen, S.; Schulz, M.S.; Waldinger, R.J. Links between childhood physical abuse and intimate partner aggression: The mediating role of anger expression. Violence Vict. 2012, 27, 315–328. [Google Scholar] [CrossRef] [Green Version]
- Trickett, P.K.; McBride-Chang, C. The development impact of different forms and child abuse and neglect. Dev. Rev. 1995, 15, 311–337. [Google Scholar] [CrossRef]
- National Child Protection Agency. Child Abuse & Neglect Korea 2016; Ministry of Health and Welfare: Sejong, Korea, 2017.
- Moylan, C.A.; Herrenkohl, T.I.; Sousa, C.; Tajima, E.A.; Herrenkohl, R.C.; Russo, M.J. The effects of child abuse and exposure to domestic violence on adolescent internalizing and externalizing behavior problems. J. Fam. Violence 2010, 25, 53–63. [Google Scholar] [CrossRef] [Green Version]
- Scarpa, A.; Haden, S.C.; Abercromby, J.M. Pathways linking child physical abuse, depression, and aggressiveness across genders. J. Aggress. Maltreatment Trauma 2010, 19, 757–776. [Google Scholar] [CrossRef]
- Evans, S.E.; Davies, C.; DiLillo, D. Exposure to domestic violence: A meta-analysis of child and adolescent outcomes. Aggress. Violent Behav. 2008, 13, 131–140. [Google Scholar] [CrossRef] [Green Version]
- Dodge, K.A.; Bates, J.E.; Pettit, G.S. Mechanisms in the cycle of violence. Science 1990, 250, 1678–1683. [Google Scholar] [CrossRef]
- Herrera, V.M.; McCloskey, L.A. Gender differences in the risk for delinquency among youth exposed to family violence. Child Abus. Negl. 2001, 25, 1037–1051. [Google Scholar] [CrossRef]
- Sternberg, K.J.; Lamb, M.E.; Greenbaum, C.; Cicchetti, D.; Dawud, S.; Cortes, R.M.; Krispin, O.; Lorey, F. Effects of domestic violence on children’s behavior problems and depression. Dev. Psychol. 1993, 29, 44–52. [Google Scholar] [CrossRef]
- National Youth Policy Institute. The Korean Children and Youth Panel Survey User Guide; National Youth Policy Institute: Sejong, Korea, 2017. [Google Scholar]
- Kim, K.; Kim, J.; Won, H. Guidelines for Conducting a Simple Psychological Examination; Central Aptitude Research Institute: Seoul, Korea, 1984. [Google Scholar]
- Jo, B.; Im, G. Development and Validation of Emotional or Behavioral Problems Scale. Korean J. Couns. Psychother. 2003, 15, 729–746. [Google Scholar]
- Huh, M. The Study for the Development and Validation of ‘Parenting Behavior Inventory’ Perceived by Adolescents. Ph.D. Thesis, Ewha Women’s University, Seoul, Korea, 2000. [Google Scholar]
- López, E.E.; Pérez, S.M.; Ochoa, G.M.; Ruiz, D.M. Adolescent aggression: Effects of gender and family and school environments. J. Adolesc. 2008, 31, 433–450. [Google Scholar] [CrossRef] [PubMed]
- Stevens, V.; De Bourdeaudhuij, I.; Van Oost, P. Relationship of the family environment to children’s involvement in bully/victim problems at school. J. Youth Adolesc. 2002, 31, 419–428. [Google Scholar] [CrossRef]
- Min, B. The Effects of School Life Adaptation and Self-Concept on Academic Achievement. Master’s Thesis, Hongik University, Seoul, Korea, 1991. [Google Scholar]
- Bollen, K.A.; Curran, P.J. Latent Curve Models: A Structural Equation Perspective; Wiley: Hoboken, NJ, USA, 2005. [Google Scholar]
- Curran, P.J.; West, S.G.; Finch, J. The robustness of test statistics to non-normality and specification error in confirmatory factor analysis. Psychol. Methods 1996, 1, 16–29. [Google Scholar] [CrossRef]
- Do, G.; Oh, J. Effects of a reality therapy group program for improving the self-esteem and coping behavior on problem of school violence-students who have been both victims and offenders of school violence. Korean J. Sch. Psychol. 2010, 7, 37–53. [Google Scholar]
- Girgus, J.S.; Yang, K. Gender and depression. Curr. Opin. Psychol. 2015, 4, 53–60. [Google Scholar] [CrossRef]
- Son, J.; Kim, H. The effects of perceived maternal parenting attitudes and peer relationships on children’s aggressive behaviors. J. Future Early Child. Educ. 2004, 11, 331–358. [Google Scholar]
- Jang, H. Understanding Developmental Psychopathology; Chanjisa: Seoul, Korea, 2005. [Google Scholar]
- Ryan, R.M.; La Guardia, J.G.; Solky-Butzel, J.; Chirkov, V.; Kim, Y. On the interpersonal regulation of emotions emotional reliance across gender, relationships and cultures. Pers. Relatsh. 2005, 12, 145–163. [Google Scholar] [CrossRef]
- Lee, J. The Relations between Peer Group Entry Process and Self-Perceived Competence Depending on Age, Sex, and Peer Status of Children. Ph.D. Thesis, Seoul National University, Seoul, Korea, 2003. [Google Scholar]
- Grant, K.E.; Compas, B.E.; Thurm, A.E.; McMahon, S.D.; Gipson, P.Y.; Campbell, A.J.; Krochock, K.; Westerholm, R.I. Stressors and child and adolescent psychopathology: Evidence of moderating and mediating effects. Clin. Psychol. Rev. 2006, 26, 257–283. [Google Scholar] [CrossRef]
- Yoo, J.A.; Huang, C.-C. Long term relationships among domestic violence, maternal mental health and parenting, and preschool children’s behavior problems. Fam. Soc. 2013, 94, 268–276. [Google Scholar] [CrossRef]
- Kolip, P.; Schmidt, B. Gender and health in adolescence. Health Policy Child. Adolesc. 1999, 1, 1–38. [Google Scholar]
- Jones, D.C. Social comparison and body image: Attractiveness comparisons to models and peers among adolescent girls and boys. Sex Roles 2001, 45, 645–664. [Google Scholar] [CrossRef]
- Crick, N.R.; Grotpeter, J.K. Relational aggression, gender, and social-psychological adjustment. Child Dev. 1995, 66, 710–722. [Google Scholar] [CrossRef] [PubMed]
- French, D.C.; Jansen, E.A.; Pidada, S. United States and Indonesian children’s and adolescents’ reports of relational aggression by dislike peers. Child Dev. 2002, 73, 1143–1150. [Google Scholar] [CrossRef]
- Leeb, R.T.; Lewis, T.; Zolotor, A.J. A review of physical and mental health consequences of child abuse and neglect and implications for practice. Am. J. Lifestyle Med. 2011, 5, 454–468. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Overall | Boys | Girls | t | ||||
|---|---|---|---|---|---|---|---|
| Construct | M | STD | M | STD | M | STD | |
| Depressive symptoms W5 | 1.77 | 0.57 | 1.70 | 0.55 | 1.84 | 0.58 | −4.99 *** |
| Depressive symptoms W6 | 1.77 | 0.55 | 1.70 | 0.53 | 1.85 | 0.55 | −5.92 *** |
| Depressive symptoms W7 | 1.79 | 0.55 | 1.69 | 0.54 | 1.89 | 0.55 | −7.58 *** |
| Aggression W5 | 1.94 | 0.56 | 1.93 | 0.56 | 1.96 | 0.56 | −1.00 |
| Aggression W6 | 1.92 | 0.54 | 1.90 | 0.54 | 1.95 | 0.54 | −2.03 * |
| Aggression W7 | 1.83 | 0.54 | 1.79 | 0.53 | 1.87 | 0.54 | −3.30 ** |
| Abuse W5 | 1.62 | 0.61 | 1.70 | 0.65 | 1.54 | 0.56 | 5.60 *** |
| Neglect W5 | 1.78 | 0.55 | 1.78 | 0.54 | 1.78 | 0.55 | −0.17 |
| Household income W5 | 4.79 | 2.05 | 4.74 | 2.00 | 4.85 | 2.10 | −1.09 |
| Health status W5 | 3.32 | 0.56 | 3.36 | 0.57 | 3.27 | 0.55 | 3.33 ** |
| Satisfaction with academic performance W5 | 2.56 | 0.78 | 2.59 | 0.80 | 2.52 | 0.75 | 1.99 * |
| Peer relationships W5 | 3.14 | 0.41 | 3.41 | 0.56 | 3.30 | 0.58 | −0.02 |
| Age W5 | 13.95 | 0.24 | 13.95 | 0.24 | 13.94 | 0.24 | 0.75 |
| Age W6 | 14.95 | 0.24 | 14.95 | 0.24 | 14.94 | 0.24 | 0.75 |
| Age W7 | 15.95 | 0.24 | 15.95 | 0.24 | 15.94 | 0.24 | 0.75 |
| N | 1797 | 942 | 855 | ||||
| Path | Boys (N = 942 for Each Wave) | Girls (N = 855 for Each Wave) | C.R | ||
|---|---|---|---|---|---|
| β | SE | β | SE | ||
| Step 1 | |||||
| Abuse→ICEPT | 0.215 *** | 0.025 | 0.283 *** | 0.033 | 1.649 |
| Abuse→SLOPE | −0.057 *** | 0.015 | −0.093 *** | 0.017 | −1.61 |
| Neglect→ICEPT | 0.207 *** | 0.03 | 0.219 *** | 0.034 | 0.275 |
| Neglect→SLOPE | −0.033 | 0.018 | −0.006 | 0.018 | 1.079 |
| Step 2 | |||||
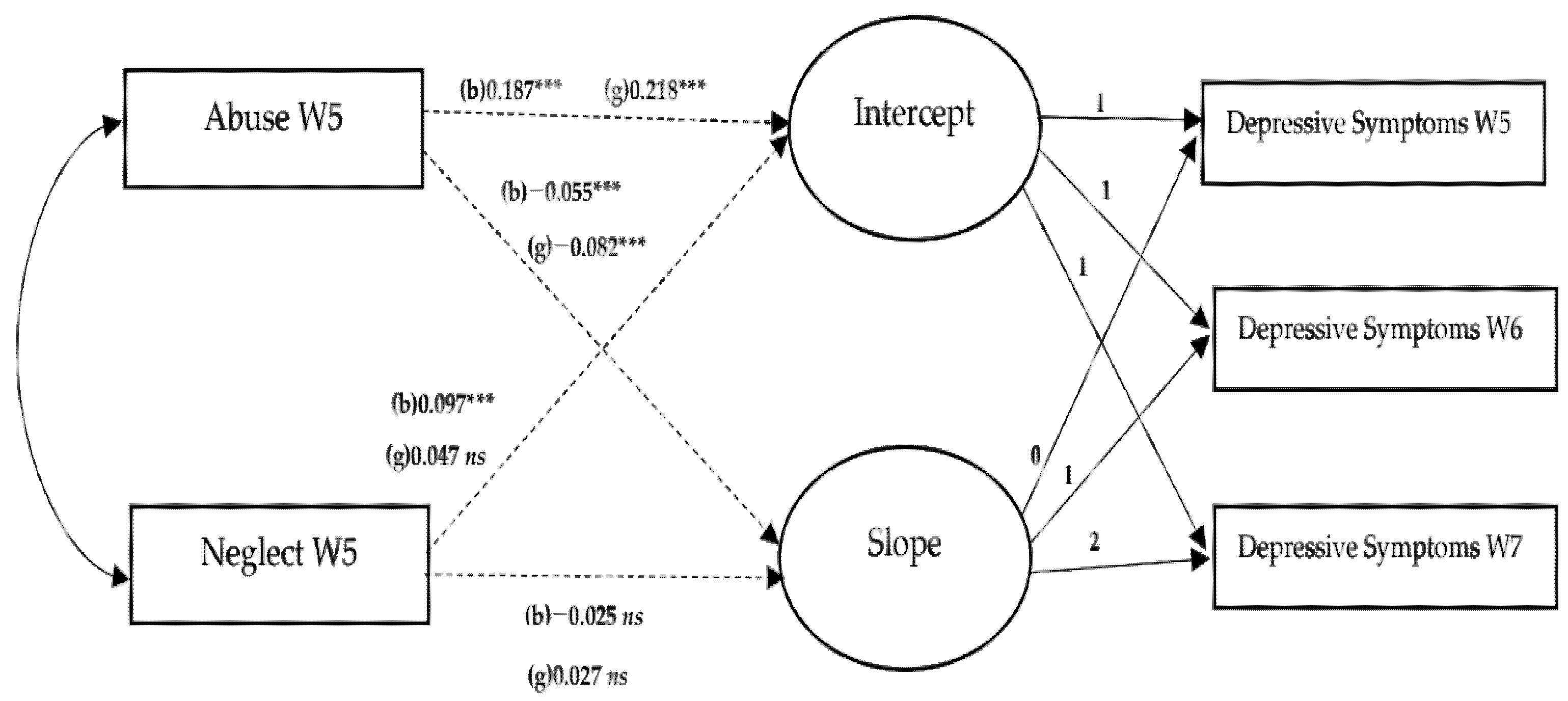
| Abuse→ICEPT | 0.187 *** | 0.023 | 0.218 *** | 0.029 | 0.843 |
| Abuse→SLOPE | −0.055 *** | 0.015 | −0.082 *** | 0.017 | −1.173 |
| Neglect→ICEPT | 0.097 *** | 0.03 | 0.047 | 0.032 | −1.148 |
| Neglect→SLOPE | −0.025 | 0.019 | 0.027 | 0.019 | 1.954 |
| Household income→ICEPT | 0.014 | 0.007 | −0.001 | 0.008 | −1.424 |
| Household income→SLOPE | −0.004 | 0.005 | −0.003 | 0.005 | 0.157 |
| Health status→ICEPT | −0.139 *** | 0.026 | −0.245 *** | 0.03 | −2.617 |
| Health status→SLOPE | 0.018 | 0.017 | 0.045 * | 0.018 | 1.14 |
| Satisfaction of academic performance→ICEPT | −0.092 *** | 0.019 | −0.107 *** | 0.022 | −0.509 |
| Satisfaction of academic performance→SLOPE | 0.012 | 0.012 | 0.004 | 0.013 | −0.488 |
| Peer relationships→ICEPT | −0.301 *** | 0.038 | −0.421 *** | 0.048 | −1.953 |
| Peer relationships→SLOPE | 0.019 | 0.024 | 0.1 *** | 0.028 | 2.195 |
| Path | Boys (N = 942 for Each Wave) | Girls (N = 855 for Each Wave) | C.R | ||
|---|---|---|---|---|---|
| β | SE | β | SE | ||
| Step 1 | |||||
| Abuse→ICEPT | 0.174 *** | 0.026 | 0.272 *** | 0.031 | 2.419 |
| Abuse→SLOPE | −0.006 | 0.015 | −0.063 *** | 0.017 | −2.529 |
| Neglect→ICEPT | 0.202 *** | 0.031 | 0.129 *** | 0.032 | −1.649 |
| Neglect→SLOPE | −0.045 * | 0.018 | −0.001 | 0.018 | 1.745 |
| Step 2 | |||||
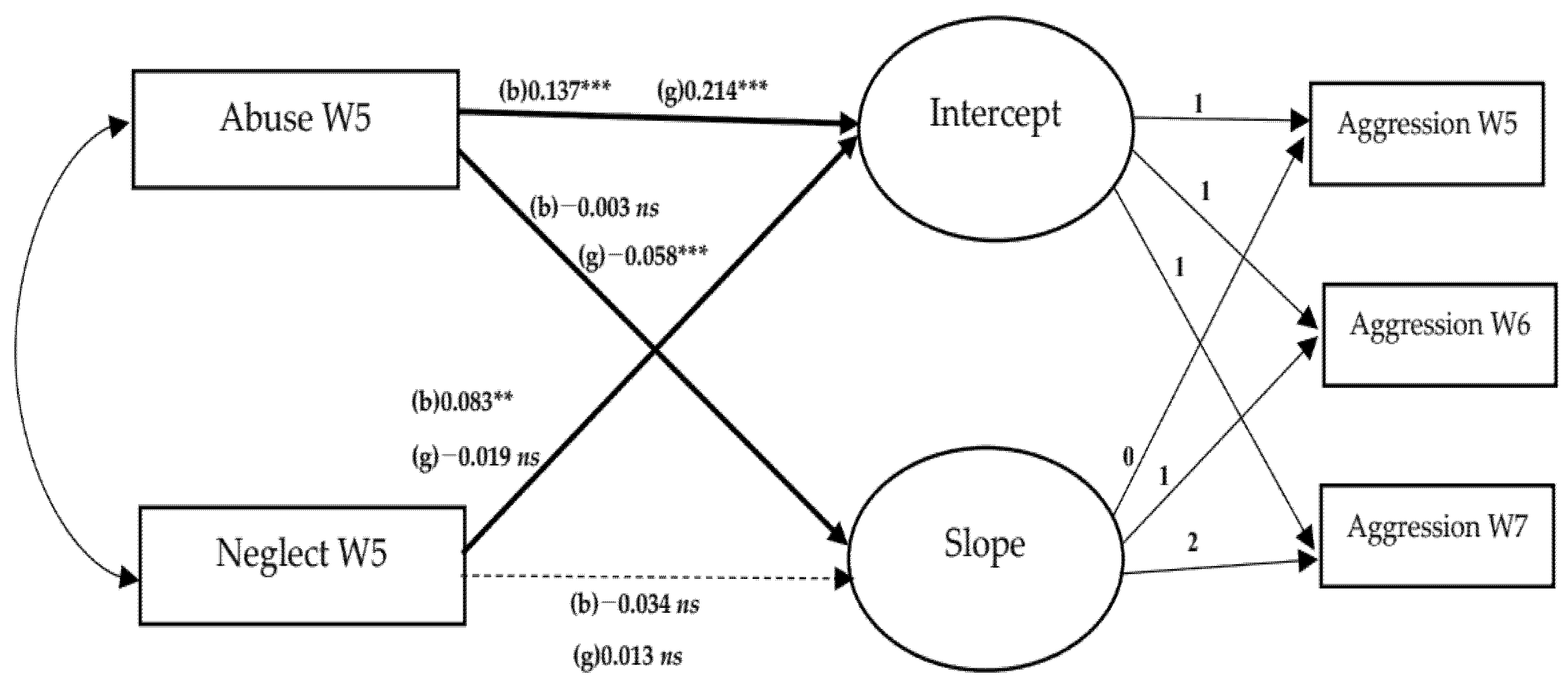
| Abuse→ICEPT | 0.137 *** | 0.025 | 0.214 *** | 0.029 | 2.001 |
| Abuse→SLOPE | −0.003 | 0.015 | −0.058 *** | 0.017 | −2.405 |
| Neglect→ICEPT | 0.083 ** | 0.031 | −0.019 | 0.032 | −2.286 |
| Neglect→SLOPE | −0.034 | 0.019 | 0.013 | 0.019 | 1.743 |
| Household income→ICEPT | 0.000 | 0.008 | −0.01 | 0.008 | −0.845 |
| Household income→SLOPE | −0.003 | 0.005 | −0.003 | 0.005 | −0.057 |
| Health status→ICEPT | −0.017 | 0.028 | −0.047 | 0.03 | −0.713 |
| Health status→SLOPE | 0.001 | 0.017 | −0.001 | 0.018 | −0.055 |
| Satisfaction of academic performance→ICEPT | −0.057 ** | 0.02 | −0.056 * | 0.022 | 0.055 |
| Satisfaction of academic performance→SLOPE | 0.002 | 0.012 | −0.001 | 0.013 | −0.19 |
| Peer relationships→ICEPT | −0.399 *** | 0.04 | −0.505 *** | 0.048 | −1.692 |
| Peer relationships→SLOPE | 0.042 | 0.025 | 0.063 * | 0.028 | 0.56 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choe, C.; Yu, S. The Effect of Child Abuse and Neglect on Trajectories of Depressive Symptoms and Aggression in Korean Adolescents: Exploring Gender Differences. Int. J. Environ. Res. Public Health 2022, 19, 6160. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106160
Choe C, Yu S. The Effect of Child Abuse and Neglect on Trajectories of Depressive Symptoms and Aggression in Korean Adolescents: Exploring Gender Differences. International Journal of Environmental Research and Public Health. 2022; 19(10):6160. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106160
Chicago/Turabian StyleChoe, Chung, and Seunghee Yu. 2022. "The Effect of Child Abuse and Neglect on Trajectories of Depressive Symptoms and Aggression in Korean Adolescents: Exploring Gender Differences" International Journal of Environmental Research and Public Health 19, no. 10: 6160. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106160