4. Suggestions
Some suggestions are put forward by this article for reference, based on the above research results:
The research results of this study showed that emotional labor had a significant impact on workplace spirituality. Therefore, it is suggested that medical staffs should face their emotions, as both positive and negative emotions are feelings produced by staying in the workplace for a long time. In particular, when nursing staffs are providing care in the medical process, they face not only patients and visitors but also family members; thus, if the management system of the service unit is not perfect, it is important to improve the emotional labor of medical staffs who are providing services under the pressure of multiple aspects. Therefore, proper guidance and learning can help medical staffs to release their emotions. For example, before caring for patients with COVID-19, if medical staffs could understand in advance that the pressure and emotional responses of these patients would be different from those of general patients and consult colleagues or seniors regarding strategies for regulating emotions in the front line, it would have helped medical staffs to face this high-stress situation. In addition to their own emotions, medical staffs need to accept the negative emotions of patients and especially the isolation of patients with COVID-19, which makes them socially separated from others, and they tend to have feelings of abandonment. Therefore, if medical staffs can properly use empathy to care for and listen to the negative emotions of patients and provide medical expertise and medical resources support, it will help patients to relieve their anxiety. This interactive process will not only reduce the impact of emotional labor for nursing staffs, but such dedication to patients will also maintain good interpersonal relationships and establish a stronger support system, which will allow medical staffs to have a high sense of identity in their work, understand the value of life due to their efforts and the meaning of their work, and improve their workplace spirituality. The results of this study showed that emotional labor had a significant impact on leisure coping strategies. Therefore, it is recommended that medical staffs should seek to establish a channel to express stress, reduce work stress, and manage emotions through participation in leisure activities. For example, engaging in socially supported leisure companionship is an approach in which a leisure sports community is established; then, the place engaged in leisure sports can usually become a social place. Such community initiatives can promote social connections and psychological support for medical staffs and help transfer the pressure brought about by negative emotions through investment in leisure sports, so that medical staffs can further obtain the benefits brought about by experiencing leisure sports. These methods all help to stabilize emotions. For example, the New Start Sports Center, which is located on the seventh floor of the Health Management Building of Tai’ an Hospital, includes large aerobics classrooms, small aerobics classrooms, cardio and weight training areas, and flywheel areas, and various courses are provided. If medical staffs have the opportunity to develop the habit of continuous and regular exercise, it will play a role in buffering and regulating negative pressure, thereby helping medical staffs to maintain their physical and psychological health.
- (2)
For Medical Institutions and Organizations
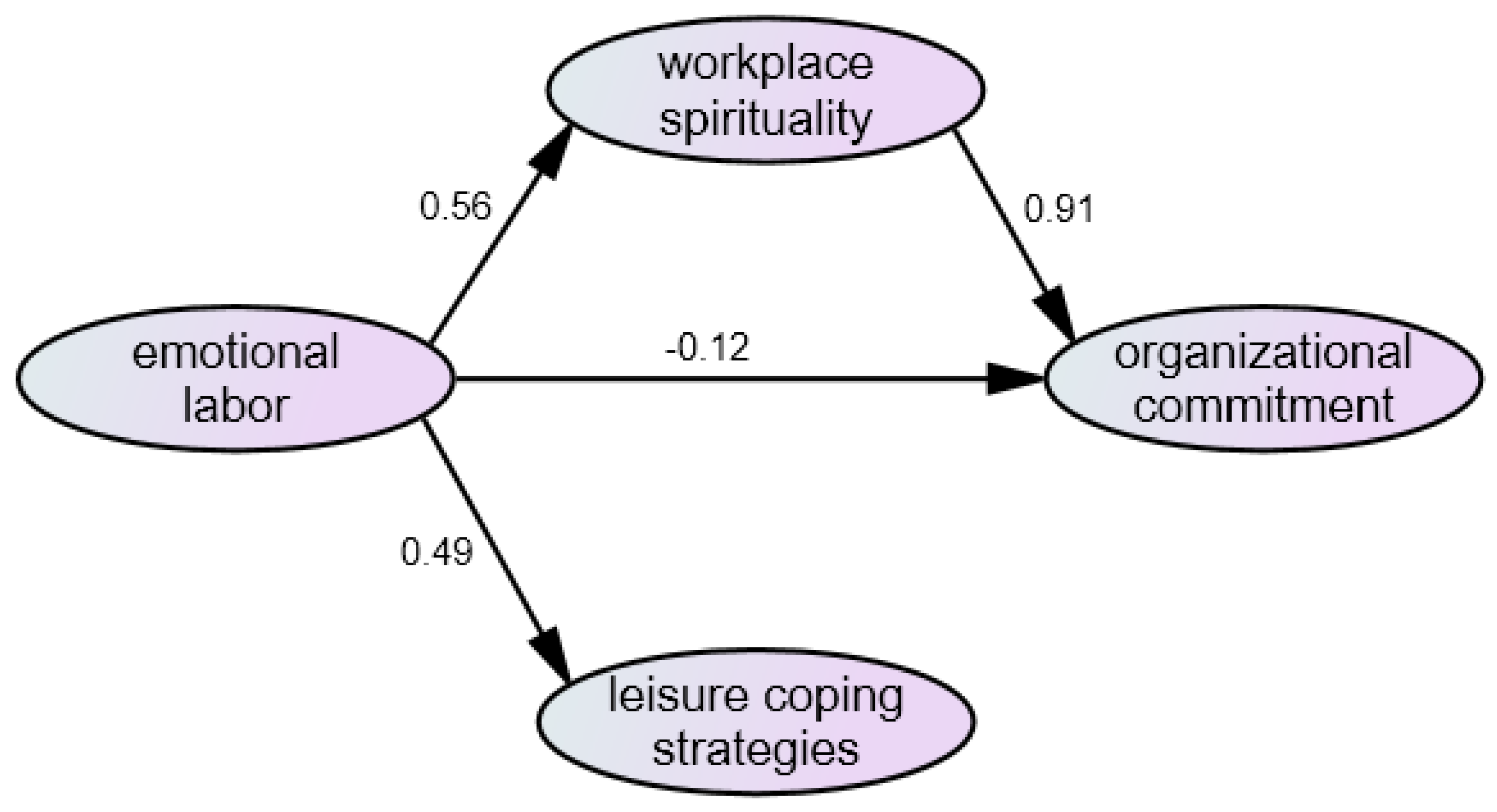
The results of this study show that emotional labor had a negative impact on organizational commitment, and it reached a significant level. Therefore, it is suggested that medical institutions and organizations should establish an in-hospital care mechanism. Especially, it is inevitable that emotional labor issues will be involved in the process when the first-line medical staffs who bear the brunt use empathy to accompany, care for, and offer consolation to patients and their family members; thus, medical staffs can build trust and harmony between doctors and patients; therefore, it is urgent to establish a care mechanism in hospitals. The COVID-19 Mental Health Guidelines for Employees of Medical Institutions, as released in 2021 by the Centers for Disease Control, Ministry of Health and Welfare, can be regarded as information worthy of reference by medical institutions and organizations, such as establishing a task force of general mental health services or setting up employee mental health services using the institution’s original employee care mechanism or one established under the structure of the pandemic prevention command center in response to the pandemic, thus providing employee consultations through more than one channel. In other words, medical institutions and organizations can help strengthen the mental health of medical staffs and reduce their emotional pressure through such measures. Once medical staffs feel that the medical institutions and organizations are attentive to assisting them in seeking out an appropriate outlet for pressure to reduce emotional labor, medical staffs can increase their emotional attachment to medical institutions and organizations, identify with the organizations, and share their goals and values. The results of this study showed that workplace spirituality had a significant impact on organizational commitment. Therefore, it is recommended that medical institutions and organizations should establish harmonious relationships that cover medical staffs and patients, colleagues, supervisors, and family members. In particular, medical staffs have different psychological needs and emotional issues. For example, the psychological pressure of medical staffs who care for confirmed patients and who are confirmed patients themselves is different. Therefore, medical institutions and organizations should develop psychological support service plans to provide assistance to medical staffs through appropriate professional manpower and prepare graded service contents based on expert advice and relevant experience. Through such measures, medical staffs will feel that medical institutions and organizations can provide strong backing, which allows them to fully devote themselves to medical care work, achieve the identification of themselves and their lives in their own hearts, and ultimately, continue to identify with the medical institutions and organizations they serve.
- (3)
Recommendations for Future Research
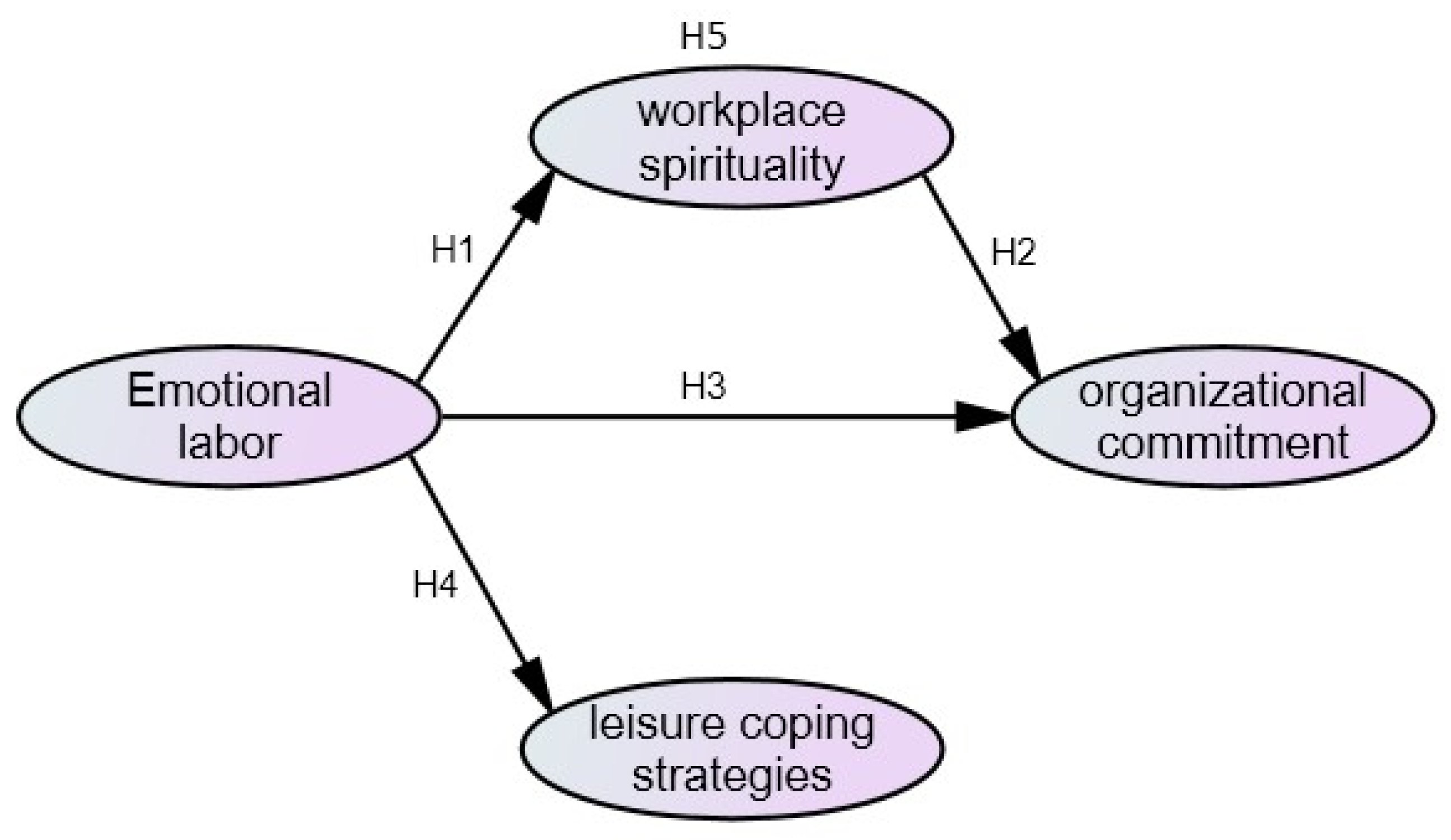
The results of this study indicated that workplace spirituality did not have a significant mediating effect between emotional labor and organizational commitment. However, in general, when the emotional labor of medical staffs is increased, they should be able to improve their own workplace spirituality to achieve positive improvements in organizational commitment. While this article only discussed workplace spirituality related to “workplace work”, there are also more and more related research on “spiritual health” as related to well-being and happiness. For example, Li et al. [
53] conducted research on the spiritual health and job satisfaction of nursing staffs, and the results of their research showed the relationship between the themes of different spiritual research and the personal and career lives of medical staffs. In addition, the research direction related to learning and growth, as well as one’s own attitude toward life, is another topic of spirituality-related research. For example, Lo and Shiau [
54] emphasized the importance of nurturing spiritual life for nursing staffs and explored building up the value of humanity, promoting spiritual growth, driving life renewal, implementing whole-person care, and other topics with nursing staffs as the research subjects, which indicates that there is diverse spiritual-related research. Thus, future related research can include broader spiritual issues beyond the “workplace work” when discussing mediation effects, and semi-structured interviews can be used to obtain more nursing staff’s inner processes. The integration of such materials will help to understand the practical significance of spirituality-related issues for enterprise organization management.
On the other hand, the theoretical framework of emotional labor, leisure coping strategies, workplace spirituality, and organizational commitment constructed in this study has been verified through empirical research. In the application of the theoretical framework in the future, it is suggested that this theoretical framework can be applied to other working groups of high emotional labor services, such as flight attendants, caregivers, department store counter staffs, and first-line customer service staffs, to understand whether different degrees of physical and psychological impacts of the same high emotional labor work groups in the face of the COVID-19 pandemic have an impact on leisure coping strategies, workplace spirituality, and organizational commitment.
Finally, the focus of the public’s attention is often on the footprints of confirmed cases, the transmission chain, vaccine administration, community transmission, and pandemic prevention policies, though the burden of maintaining the normal operation of the entire medical system and implementing pandemic prevention policies often falls on medical staffs. However, the pressure on medical staffs and the issues of emotional adjustment are often easily ignored by the public, which, in turn, leads to more medical staffs quitting their jobs. Therefore, this study takes medical staffs as an example to describe the emotional labor faced by medical staffs currently in the COVID-19 pandemic through empirical research. The article also proposes appropriate leisure coping strategies to enhance medical staffs’ sense of work purpose and meaning, as well as group identity, through leisure coping to improve the organizational commitment of medical staffs in order for them to continue to make good use of their professionalism in the medical system. Thus, this study has a certain degree of practical contribution.






{kind=link}
{kind=link}