
The Effect of Professional Oral Care on the Oral Health Status of Critical Trauma Patients Using Ventilators

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Examination of Oral Health Condition and Performance of Professional Oral Hygiene Care
2.3.1. Examination of Oral Health Condition
2.3.2. Performance of Professional Oral Hygiene Care
2.3.3. Training for General Oral Hygiene Care
2.3.4. Intervention Performed for Each Group
2.3.5. Study Variables
2.3.6. Modified Bedside Oral Exam (MBOE)
2.4. Analysis Method
3. Results
3.1. General Patient Characteristics and Oral Health Status
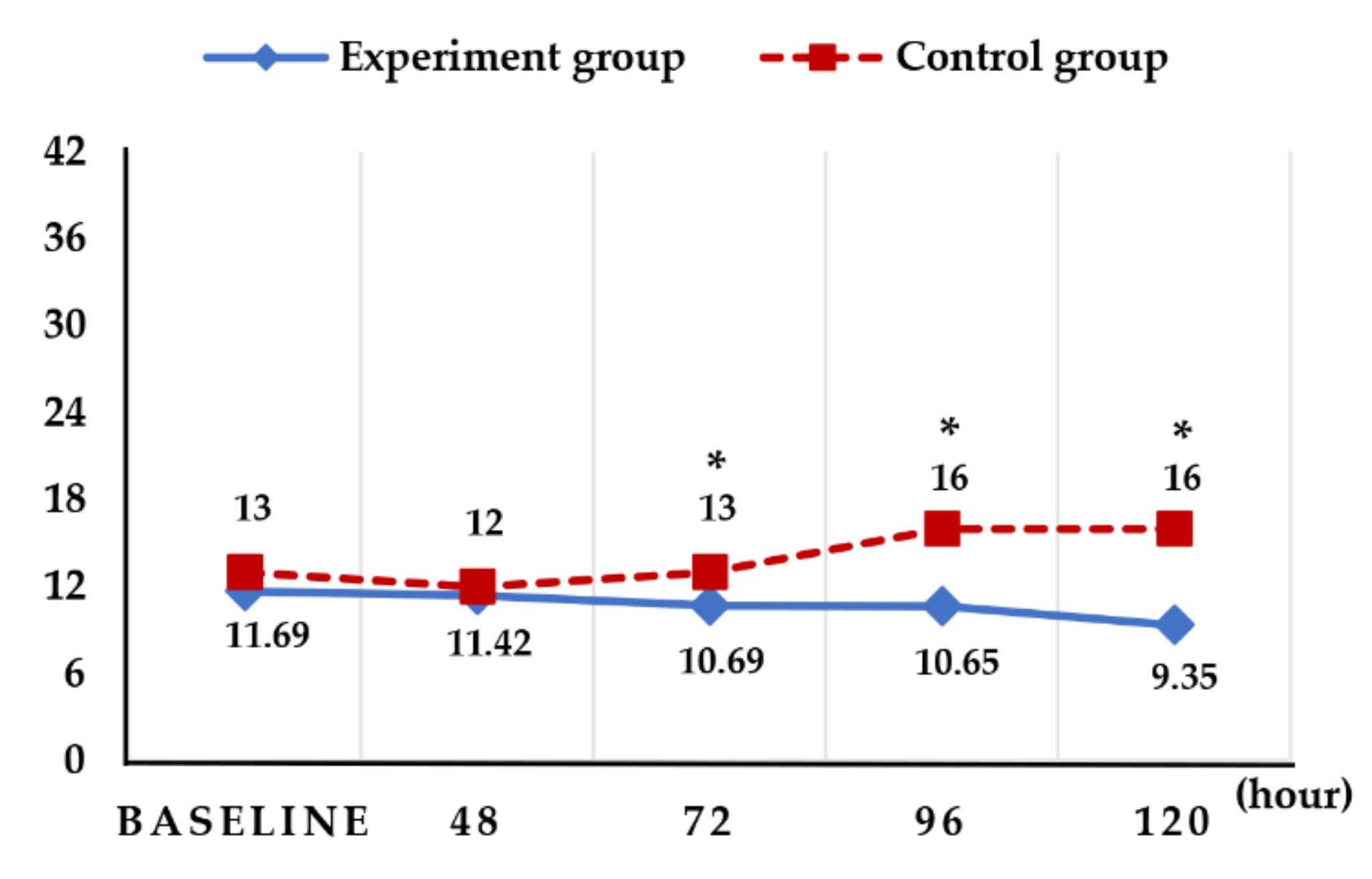
3.2. Changes in the Oral Health Status of the Patients According to Professional Oral Hygiene Care
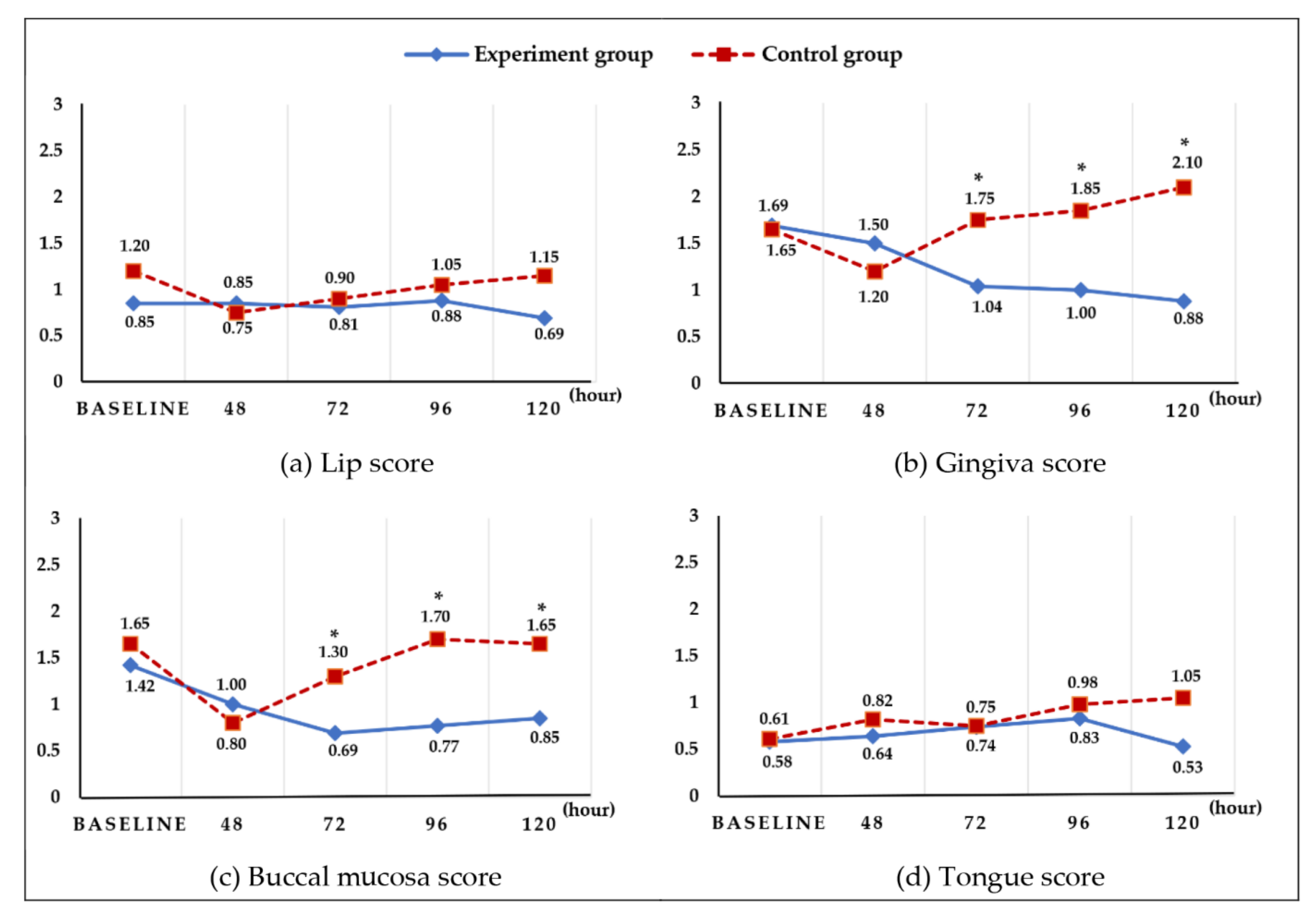
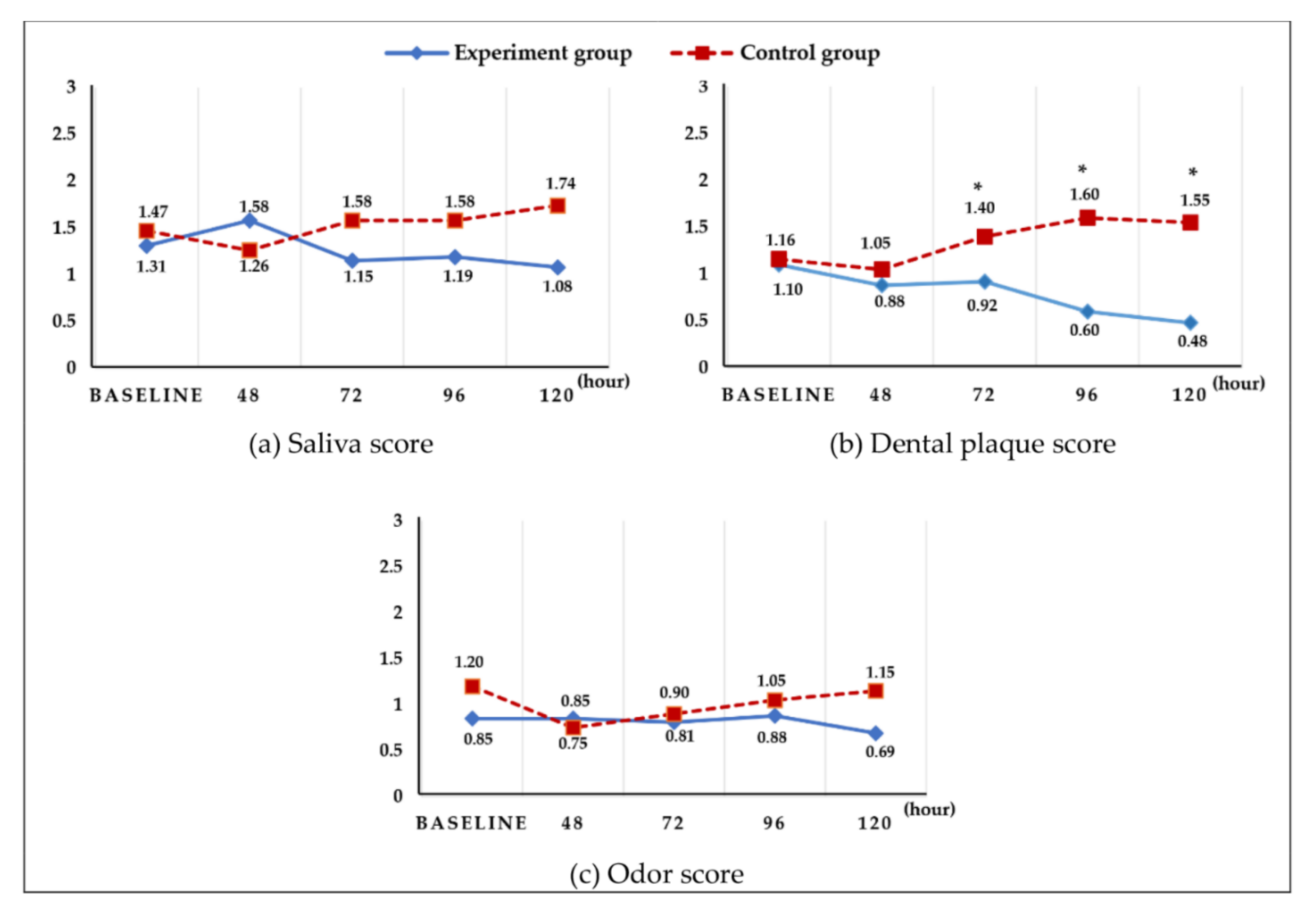
3.3. Changes in the Oral Health Status by Items According to Professional Oral Hygiene Care
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Mori, H.; Hirasawa, H.; Oda, S.; Shiga, H.; Matsuda, K.; Nakamura, M. Oral care reduces incidence of ventilator-associated pneumonia in ICU populations. Intensive Care Med. 2006, 32, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Papazian, L.; Klompas, M.; Luyt, C.E. Ventilator-associated pneumonia in adults: A narrative review. Intensive Care Med. 2020, 46, 888–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Institute for Healthcare Improvement. How-to Guide: Prevent Ventilator-Associated Pneumonia; Institute for Healthcare Improvement: Cambridge, MA, USA, 2012. [Google Scholar]
- Institute for Healthcare Improvement. What is a Bundle? Institute for Healthcare Improvement: Cambridge, MA, USA, 2012. [Google Scholar]
- Zhao, T.; Wu, X.; Zhang, Q.; Li, C.; Worthington, H.V.; Hua, F. Oral hygiene care for critically ill patients to prevent ventilator-associated pneumonia. Cochrane Database Syst. Rev. 2020, 12, CD008367. [Google Scholar] [CrossRef] [PubMed]
- Munro, C.L.; Grap, M.J. Oral health and care in the intensive care unit: State of the science. Am. J. Crit. Care 2004, 13, 25–33. [Google Scholar] [CrossRef]
- McNeill, H.E. Biting back at poor oral hygiene. Intensive Crit. Care Nurs. 2000, 16, 367–372. [Google Scholar] [CrossRef]
- Bailey, R.L.; Ledikwe, J.H.; Smiciklas-Wright, H.; Mitchell, D.C.; Jensen, G.L. Persistent oral health problems associated with comorbidity and impaired diet quality in older adults. J. Am. Diet Assoc. 2004, 104, 1273–1276. [Google Scholar] [CrossRef]
- Özden, D.; Türk, G.; Düger, C.; Güler, E.K.; Tok, F.; Gülsoy, Z. Effects of oral care solutions on mucous membrane integrity and bacterial colonization. Nurs. Crit. Care 2014, 19, 78–86. [Google Scholar] [CrossRef]
- Shiraishi, A.; Yoshimura, Y.; Wakabayashi, H.; Tsuji, Y.; Yamaga, M.; Koga, H. Hospital dental hygienist intervention improves activities of daily living, home discharge and mortality in post-acute rehabilitation. Geriatr. Gerontol. Int. 2019, 19, 189–196. [Google Scholar] [CrossRef]
- Lupi, S.M.; Pascadopoli, M.; Maiorani, C.; Preda, C.; Trapani, B.; Chiesa, A.; Esposito, F.; Scribante, A.; Butera, A. Oral Hygiene Practice among Hospitalized Patients: An Assessment by Dental Hygiene Students. Healthcare 2022, 10, 115. [Google Scholar] [CrossRef]
- Mangram, A.J.; Sohn, J.; Zhou, N.; Hollingworth, A.K.; Ali-Osman, F.R.; Sucher, J.F.; Moyer, M.; Dzandu, J.K. Trauma-associated pneumonia: Time to redefine ventilator-associated pneumonia in trauma patients. Am. J. Surg. 2015, 210, 1056–1061. [Google Scholar] [CrossRef] [Green Version]
- Prendergast, V.; Hallberg, I.R.; Jahnke, H.; Kleiman, C.; Hagell, P. Oral health, ventilator-associated pneumonia, and intracranial pressure in intubated patients in a neuroscience intensive care unit. Am. J. Crit. Care 2009, 18, 368–376. [Google Scholar] [CrossRef] [Green Version]
- Beck, S. Impact of a systematic oral care protocol on stomatitis after chemotherapy. Cancer Nurs. 1979, 2, 185–199. [Google Scholar] [CrossRef] [PubMed]
- Wallace, W.C.; Cinat, M.; Gornick, W.B.; Lekawa, M.E.; Wilson, S.E. Nosocomial infections in the surgical intensive care unit: A difference between trauma and surgical patients. Am. Surg. 1999, 65, 987–990. [Google Scholar]
- Baruah, K.; Thumpala, V.K.; Khetani, P.; Barua, Q.; Tiwari, R.V.; Dixit, H. A review on toothbrushes and tooth brushing methods. Int. J. Pharm. Sci. Invent. 2017, 6, 29–38. [Google Scholar]
- Nakahodo, N.; Nomura, Y.; Oshiro, T.; Otsuka, R.; Kakuta, E.; Okada, A.; Inai, Y.; Takei, N.; Hanada, N. Effect of Mucosal Brushing on the Serum Levels of C-Reactive Protein for Patients Hospitalized with Acute Symptoms. Medicina 2020, 56, 549. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.H.; Kim, G.M.; Lee, J.Y.; Kwon, H.K.; Kim, B.I. A comparison of tooth brushing methods recommended in different countries. J. Korean Acad. Oral Health 2015, 39, 195–200. [Google Scholar] [CrossRef] [Green Version]
- Terezakis, E.; Needleman, I.; Kumar, N.; Moles, D.; Agudo, E. The impact of hospitalization on oral health: A systematic review. J. Clin. Periodontol. 2011, 38, 628–636. [Google Scholar] [CrossRef]
- Grap, M.J.; Munro, C.L. Preventing ventilator-associated pneumonia: Evidence-based care. Crit. Care Nurs. Clin. 2004, 16, 349–358. [Google Scholar] [CrossRef]
- Diaz, E.; Rodríguez, A.H.; Rello, J. Ventilator-associated pneumonia: Issues related to the artificial airway. Respir. Care 2005, 50, 900–909. [Google Scholar]
- Murray, J.; Scholten, I. An oral hygiene protocol improves oral health for patients in inpatient stroke rehabilitation. Gerodontology 2018, 35, 18–24. [Google Scholar] [CrossRef]
- Dallanora, L.M.F.; Menegazzo, K.; Durigon, A.S. Evaluation of oral hygiene techniques in intensive care units (icus) of macroregional health in the midwest of the state of santa catarina and protocol suggestion. Int. J. Dev. Res. 2021, 11, 46978–46983. [Google Scholar]
- Jang, Y.S. Development of admission and discharge criteria in intensive care unit. Korean J. Adult Nurs. 2001, 13, 291–300. [Google Scholar]
- Bellissimo-Rodrigues, W.T.; Menegueti, M.G.; Gaspar, G.G.; de Souza, H.C.C.; Auxiliadora-Martins, M.; Basile-Filho, A.; Martinez, R.; Bellissimo-Rodrigues, F. Is it necessary to have a dentist within an intensive care unit team? Report of a randomised clinical trial. Int. Dent. J. 2018, 68, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Wennerholm, L.; Perez, N.R.; Abt, S.; Fon, K.; Elsabrout, K. Development of an Oral Care Multidisciplinary Initiative in an Acute Care Community Hospital: Framework, Timeline, and Outcomes. Am. J. Speech Lang. Pathol. 2021, 30, 517–531. [Google Scholar] [CrossRef]
- Shirabon Net. Heisei 30-Year Medical Fee Schedule Table. Available online: https://shirobon.net/medicalfee/latest/ (accessed on 14 February 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Categories | Exp. Group (n:29) | Cont. Group (n:28) | x2 † or t ‡ | p | ||
|---|---|---|---|---|---|---|---|
| n (%) | Mean ± SD | n (%) | Mean ± SD | ||||
| Age (yr) | 60.62 ± 15.67 | 57.43 ± 16.94 | 0.464 | ||||
| Sex | Male | 20 (69) | 19 (67.9) | 0.008 | 0.928 | ||
| Female | 9 (31) | 9 (32.1) | |||||
| Antibiotics | Yes | 25 (86.2) | 27 (96.4) | 1.860 | 0.352 | ||
| No | 4 (13.8) | 1 (3.6) | |||||
| Oral status | |||||||
| Lips | 0.85 ± 0.78 | 1.20 ± 0.95 | 0.161 | 0.767 | |||
| Gingiva | 1.69 ± 1.44 | 1.65 ± 1.23 | 0.281 | 0.598 | |||
| Buccal mucosa | 1.42 ± 1.50 | 1.65 ± 1.90 | 1.411 | 0.240 | |||
| Tongue | 1.73 ± 1.37 | 1.84 ± 1.36 | 1.844 | 0.176 | |||
| Saliva | 1.31 ± 0.79 | 1.47 ± 0.96 | 2.959 | 0.091 | |||
| Teeth (plaque) | 1.16 ± 0.69 | 1.10 ± 0.79 | 0.017 | 0.895 | |||
| Odor | 0.65 ± 0.80 | 0.80 ± 0.83 | 0.942 | 0.336 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, M.-I.; Han, S.-Y.; Jeon, H.-S.; Choi, E.-S.; Won, S.-E.; Lee, Y.-J.; Baek, C.-Y.; Mun, S.-J. The Effect of Professional Oral Care on the Oral Health Status of Critical Trauma Patients Using Ventilators. Int. J. Environ. Res. Public Health 2022, 19, 6197. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106197
Choi M-I, Han S-Y, Jeon H-S, Choi E-S, Won S-E, Lee Y-J, Baek C-Y, Mun S-J. The Effect of Professional Oral Care on the Oral Health Status of Critical Trauma Patients Using Ventilators. International Journal of Environmental Research and Public Health. 2022; 19(10):6197. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106197
Chicago/Turabian StyleChoi, Ma-I, Sun-Young Han, Hyun-Sun Jeon, Eun-Sil Choi, Seung-Eun Won, Ye-Ji Lee, Chi-Yun Baek, and So-Jung Mun. 2022. "The Effect of Professional Oral Care on the Oral Health Status of Critical Trauma Patients Using Ventilators" International Journal of Environmental Research and Public Health 19, no. 10: 6197. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106197